
Abstract
Descriptive research of inpatient populations provides necessary information on the causes and treatments of psychiatric illness [1], population-based changes in mental health, the accountability of mental health services in relation to service objectives [2], the type and quantity of resources required and the cost-effectiveness of treatment [3].
Relatively few high-quality international studies of child and adolescent inpatients have been published [3]. A summary of studies published between 1983 and 2000 reported highly heterogeneous sample characteristics, with mean admission age ranging from 9.5 to 14.8 years [4]. All studies except one reported a predominance of male subjects, with rates varying from 52% to 81%. The exceptional study found that of 276 consecutive admissions to British adolescent units (1986–1989), 57% were female [5]. The high heterogeneity in child and adolescent inpatient populations partly reflects different admission criteria, diagnostic systems and research methodologies [1].
Despite heterogeneity in child and adolescent inpatient samples, some themes have emerged. Conduct disorders are often the main diagnosis, with prevalence ranging from 21% to 51% [1], [5], [6]. Studies also concur that adolescent inpatients are diagnostically complex, reflecting a range of biological, familial, social and economic vulnerabilities [1].
An Australian study provided a comprehensive description of 58 consecutive admissions to a Western Australian public child and adolescent unit (mean age = 11.3 years, 79% male) which provided the most intensive treatment in the state [3]. The most common principal diagnosis was disruptive behaviour disorder, perhaps reflecting the intensive nature of the unit. Almost 40% had multiple Axis I diagnoses, 40% had a language disorder and impairments in social, daily living, motor skills and self-esteem were common.
In consecutive referrals to a Western Australian public child and adolescent psychiatric facility, most of the 126 participants were female (mean age = 12.18 years) and they experienced more severe internalizing and externalizing problems than patients in less restrictive treatment settings [7]. Conversely, 51 adolescents (mean age = 15 years, 41% female) consecutively admitted to a Brisbane public inpatient unit did not differ from a comparative outpatient sample on internalizing and externalizing problems but were more likely to have problems with overactivity, inattention, substance abuse, peer and family relationships and school attendance [8]. An outcome study of 137 adolescents (mean age = 15.1 years; 60% female) admitted to a Sydney public inpatient unit (85% participation rate) found that the most common principal diagnoses were unipolar mood disorders (52%), followed by psychotic disorders and anxiety disorders [9]. More than three-quarters of adolescents with mood disorder or psychosis had a comorbid diagnosis.
Australian studies of child and adolescent inpatients have differed on demographic and psychiatric characteristics of inpatients relative to community clinical and non-clinical groups [3], [8–10]. Between-study variation probably reflects variation in unit admission criteria and the demography of catchment areas [7], [8].
Information on family functioning associated with Australian child and adolescent inpatients is beginning to emerge [7]. Consistent with international findings [1], studies have reported that families are more likely to be socioeconomically disadvantaged, sole-parent families and experience high dysfunction [3], [7]. Parents of inpatients are reported to experience more psychiatric and alcohol problems than parents from community clinical groups [7].
Given the important association between family and parent factors and adolescent mental illness [11] and the complexity and severity of disturbance among adolescent inpatients, the aim of the present study was to provide a comprehensive description of adolescents admitted to a public psychiatric inpatient unit and examine the functioning of parents and families.
Method
Ethical approval was obtained from Monash University and from the relevant health service.
Participants
Participants were recruited from a regional public child and adolescent mental health service (CAMHS) inpatient unit in Melbourne. The unit is gazetted under the State of Victoria's Mental Health Legislation. It operates 24 h, 7 days a week and accepts referrals of 12–18-year-olds. There are no absolute exclusion criteria but to be admitted the significant problem needs to be psychiatric and not manageable in a less restrictive environment. Patients with disruptive behaviour disorders are not excluded.
A referral process was established with three main case clinicians from the unit. Clinicians referred consecutive cases to the project between November 2001 and October 2005. Eligibility criteria were that the adolescent's admission was not a crisis admission; that is, the admission was for more than a few days, and the patient was well enough to provide consent and be interviewed. When possible, the assessment of patients who were too unwell was postponed until they were well enough to participate.
Adolescent measures
Adolescents completed the Youth Self Report (YSR) [12] as a measure of internalizing and externalizing problems and competence in social, educational and general domains. Parents completed the equivalent Child Behaviour Checklist (CBCL) [12]. Normative data are available for these reliable and valid measures [12].
Specific psychopathology was measured with the Revised Children's Manifest Anxiety Scale (RCMAS) [13], a measure of generalized trait anxiety for 6–19-year-olds with good reliability and validity [14] and the Reynolds Adolescent Depression Scale (RADS) [15], consisting of 30 items reflecting DSM-III depressive symptoms. High reliability and validity are reported [16]. Adolescents also completed the Adolescent Dissociative Experiences Scale (ADES) [17], a reliable and valid 30-item measure of pathological dissociative symptomatology [18], [19].
Parent and family self-report measures
Parents and adolescents each completed the 12-item General Functioning Scale of the Family Assessment Device (FAD) [20], which measures global family functioning [20], [21].
Parents completed the Personality Diagnostic Questionnaire–4+ (PDQ-4) [22], which provides an overall personality disturbance score. Parents also completed the Brief Symptom Inventory (BSI) [23], a 53-item measure that provides a general severity index of current, global psychological distress.
Clinician information
CAMHS case clinicians provided patients’ DSM-IV diagnosis. The diagnosis was made collectively by the patient's multi-disciplinary treatment team, consisting of a teacher, a psychiatric nurse and a case clinician trained in nursing or allied health with a specialization in mental health. The diagnosis was overseen and reviewed by the unit's consultant psychiatrist, who assessed the patient individually and provided supervision to the treatment team.
Case clinicians completed the Global Assessment of Functioning (GAF), a 100-point hypothetical continuum of mental health and functioning, and the Global Assessment of Relational Functioning (GARF), an equivalent continuum for overall family functioning [24], [25].
Results
Response rate
Ninety-five of 111 referrals were accepted. Those not accepted were outside the age range, were not a patient of CAMHS, or were discharged before eligibility could be determined. Of 95 accepted referrals, 88 (93%) completed an assessment, four were discharged before the assessment could occur, two withdrew consent and one patient was too unwell to participate.
Participants were 37 male and 51 female subjects aged 12–18 years (mean = 15.36 years; SD = 1.48). There was no association between age and sex. At the time of recruitment 76 participants were inpatients and 12 were attending a day programme, but had been inpatients and were still unwell.
Parent participation rate
In 65 cases (74%) at least one parent participated. Fifty-four female carers/mothers (66%) and 37 male carers/fathers (61%) participated.
Demographics
Forty-seven adolescents (53%) lived in a two-parent/carer home and 31 (35%) lived in single-parent home (87% single mothers). In comparison, recent statewide census data show that 81% of children living with family live in a two-parent/carer home while 18% live in a single-parent home [26]. Six adolescents lived in foster care, and four with extended family or friends.
Fifteen adolescents (17%) were born outside Australia, most (n = 13) in non-English-speaking nations. Twenty-eight female carers (32%) and 27 male carers (31%) were born outside Australia, all but three in non-English-speaking nations. Figures were marginally higher than census data, which show that 24% of the Australian population were born overseas and, of Australian-born people, 26% have at least one parent born overseas [27].
Familial socioeconomic status
Familial socioeconomic status (SES) was estimated by parental occupation using the second edition of the Australian standard classification of occupations (ASCO-2) [28]. Occupational categories were collapsed into three groups approximating higher, mid- and lower status occupations. The proportion of parents in each group approximated the Australian workforce [29] (Table 1).
Parental occupation
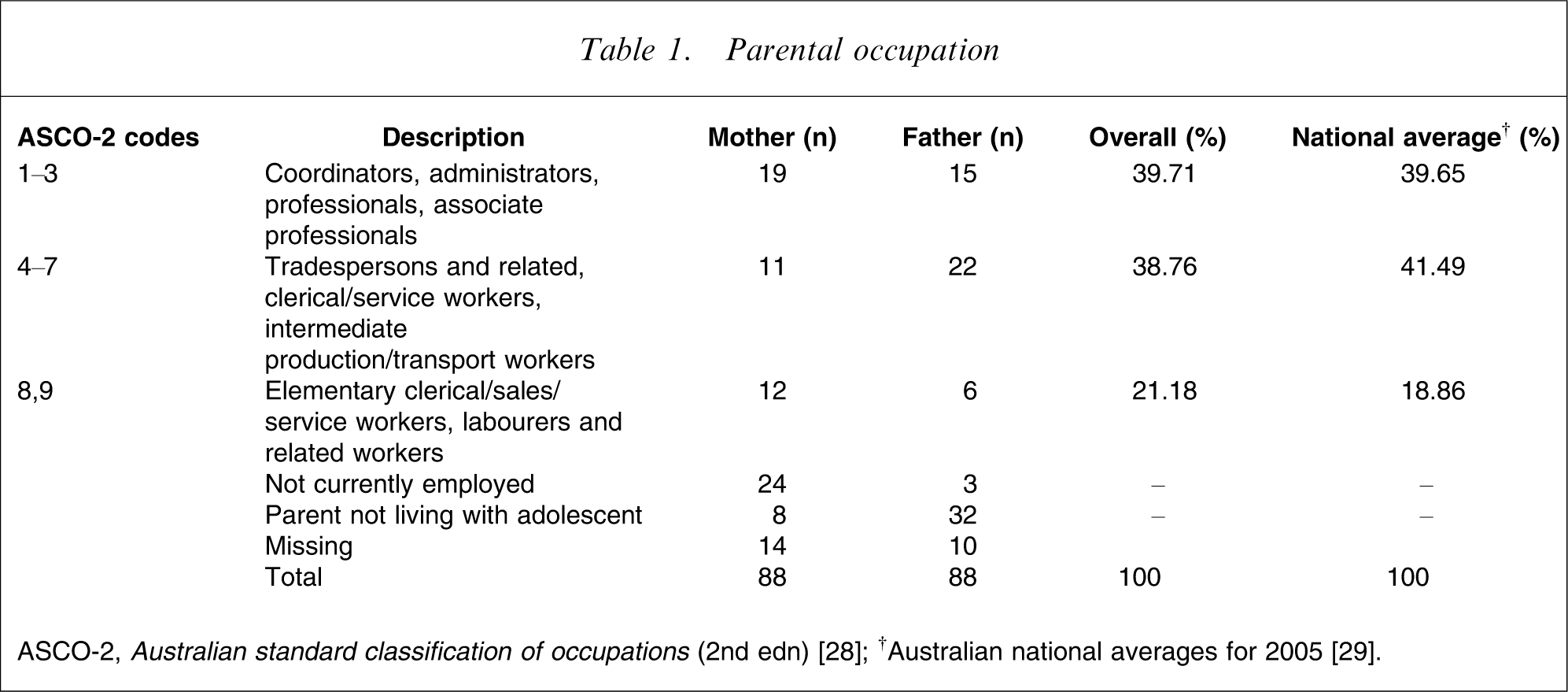
At least one parent was employed in 93% of two-parent families, and 64% of single parents were employed. Figures were comparable to national census figures of 94.7% and 49.3%, respectively [26].
ASCO-2 occupational codes were converted into values of SES using the ANU-4 index [30]. The ANU-4 index assigns values of SES to occupational codes based on linkages between education, occupation and market income [28]. Scores range from 0 (unemployed; lowest) to 100 (highest) and approach normal distribution [30]. SES values were used in subsequent analyses of associations with SES.
Adolescent psychiatric measures
The principal DSM-IV Axis I diagnoses are presented in Table 2, sorted into Internalizing, Externalizing and Psychotic-type disorders. Most adolescents (56%) had multiple Axis I diagnoses. The most common second Axis I diagnoses were parent–child relational problems (n = 17), behaviour disorders (n = 7), and substance abuse (n = 5).
DSM-IV Axis I principal diagnosis (n = 88)
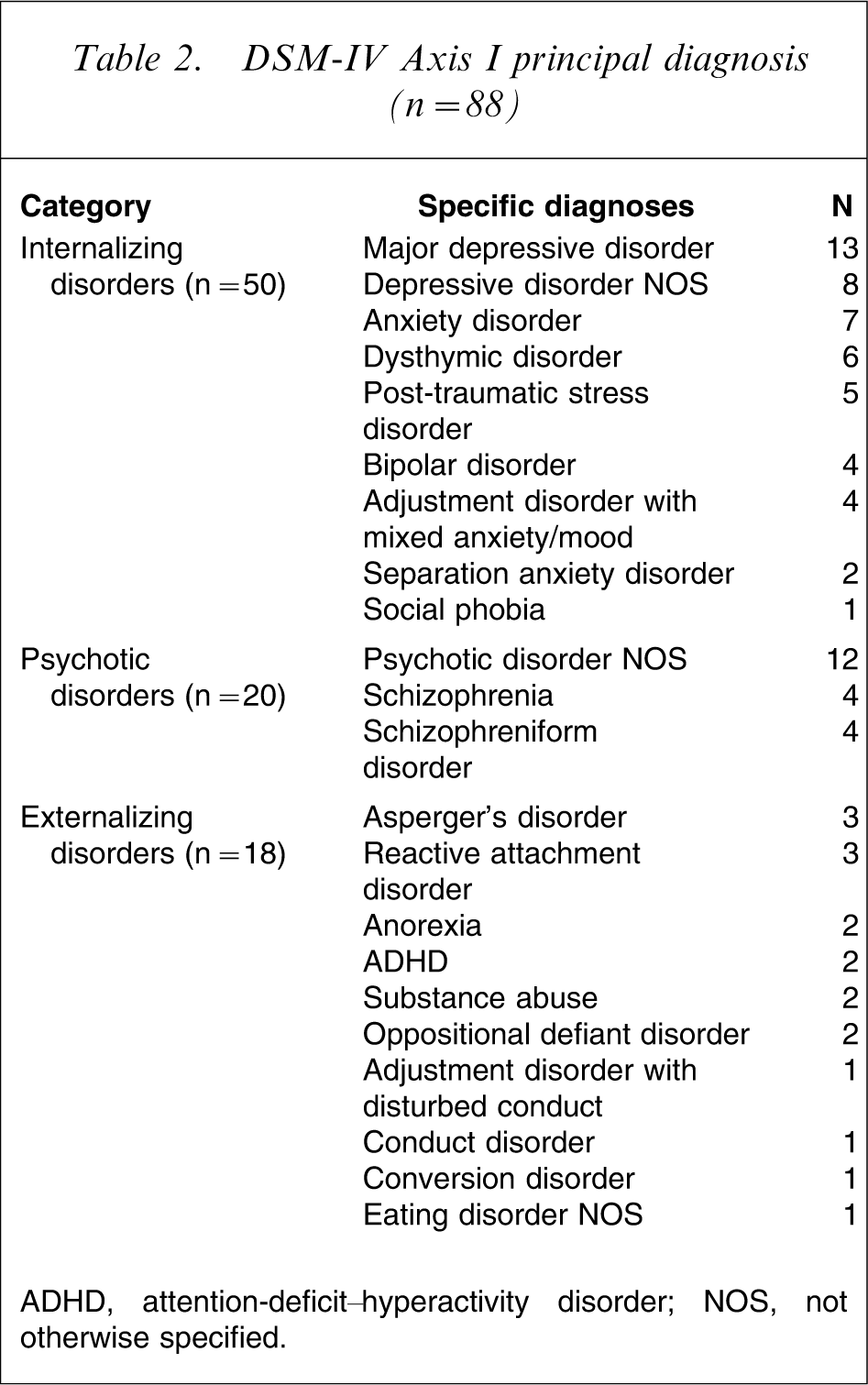
ADHD, attention-deficit–hyperactivity disorder; NOS, not otherwise specified.
On DSM-IV Axis IV, 82% of participants were diagnosed with ‘problems with primary support group’, 63% with educational/occupational problems and 27% with problems related to the social environment.
Researchers estimated GAF and GARF scores based on information from all informants. GAF scores ranged from 10 to 70 (mean = 49.89, SD = 9.54). Most adolescents (55%) obtained scores of ≤50, indicating serious symptoms and/or serious impairment in basic functioning. GARF scores ranged from 20 to 85 (mean = 58.08, SD = 12.52) with 56% of participants scoring ≤60, indicating clear family dysfunction with, at best, occasional times of satisfying and competent functioning. Researcher-rated scores correlated with clinician-rated scores (GAF: r = 0.72, p < 0.01 and GARF: r = 0.64, p = 0.01), supporting the validity of researcher ratings.
Psychometric measures
Most adolescents were in the clinical range for internalizing problems according to YSR and CBCL results (Table 3). Parents reported higher externalizing behaviour problems, social problems and thought problems than adolescents, with the largest discrepancy regarding thought problems. Competency scale results showed that 41% of parents and 33% of adolescents reported clinical-range problems.
NESB status and SES by type of prinicipal diagnosis
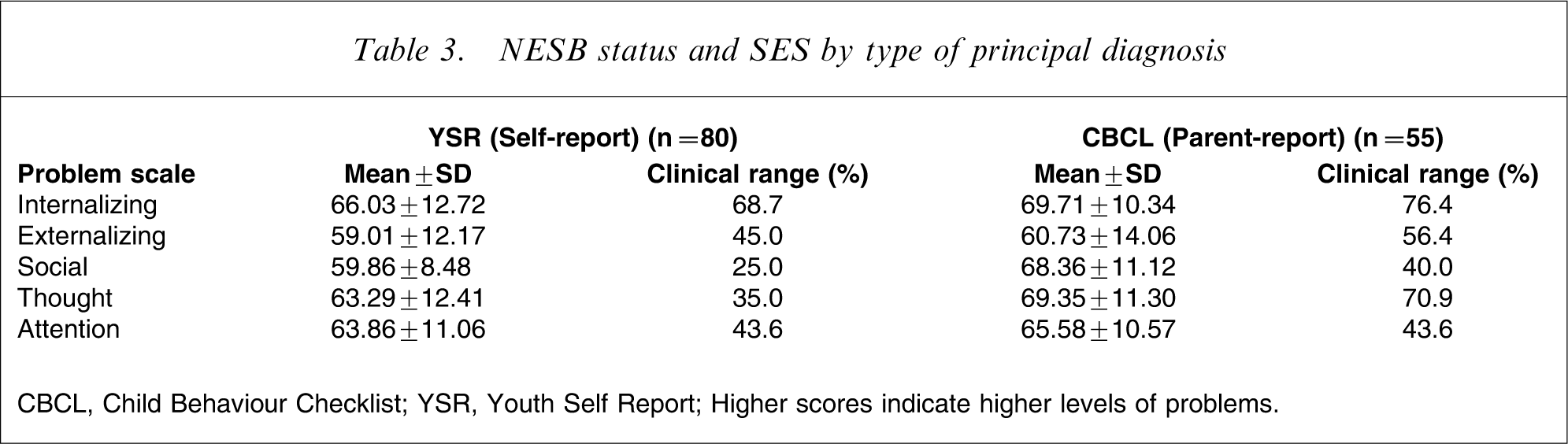
CBCL, Child Behaviour Checklist; YSR, Youth Self Report; Higher scores indicate higher levels of problems.
Most adolescents (56%) reported clinical levels of depressive symptoms on the RADS (mean = 79.51, SD = 18.16) and 64% reported clinical levels of anxiety on the RCMAS (mean = 63.44, SD = 11.60). One-third of adolescents reported clinical levels of dissociative symptoms on the ADES (mean = 3.40, SD = 2.14).
Most adolescents (52%) were not attending school at the time of admission and 33% had not attended school for ≥8 weeks. The mean length of absence was 14 weeks.
Parent functioning
Three female carers (6.4%) and one male carer (8.3%) reported clinical levels of personality disturbance on the PDQ-4 (female mean = 18.32, SD = 15.83; male mean = 16.47, SD = 14.99). Seven female carers (14.6%) and seven male carers (21.8%) scored in the clinical range for current global psychological distress on the BSI (female mean = 32.20; SD = 29.04; male mean = 54.91; SD = 11.61).
Family functioning
Most adolescents (52.3%) reported clinical-level family dysfunction on the FAD (mean = 2.31, SD = 0.61). Parent-rated mean scores were not in the clinical range, but 40% of mothers and 33.3% of fathers reported clinical levels of family dysfunction. Family demographic characteristics and family functioning were further examined in relation to three categories of adolescent principal diagnosis.
Descriptive results for non-English-speaking background (NESB) and SES are presented in Table 4. NESB status was assigned if the individual was born in a non-English-speaking country. Significant associations were found between adolescent NESB status and diagnostic group (χ2(2) = 9.44, p = 0.01) and between maternal and paternal NESB status and diagnostic group (χ2(2) = 15.77, p = 0.00 and χ2(2) = 12.49, p = 0.00, respectively). NESB status was associated with the diagnostic category of psychotic disorders (Table 4).
NESB and SES status
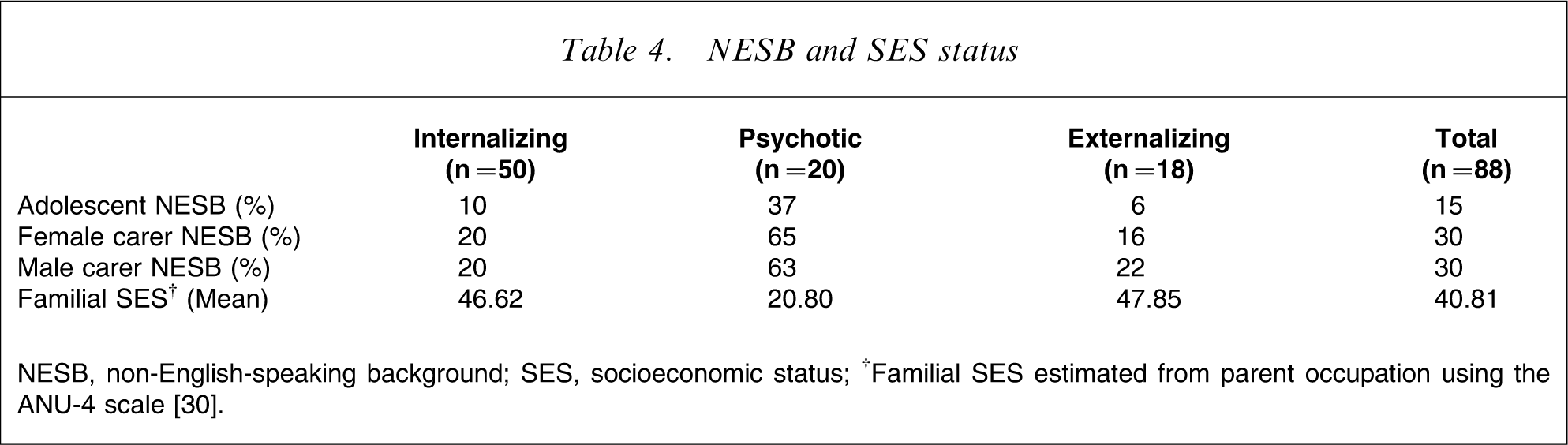
NESB, non-English-speaking background; SES, socioeconomic status; †Familial SES estimated from parent occupation using the ANU-4 scale [30].
Familial SES was also associated with diagnostic group (F(2,69) = 4.90, p = 0.01). Pairwise analyses showed that the SES of the psychotic group was significantly lower than the other groups. There was a significant association between maternal NESB status and SES (F(1,70) = 4.11, p = 0.05) and an association approaching significance between paternal NESB status and SES (F(1,67) = 3.29, p = 0.07).
There was no association between diagnostic group and family functioning as indicated by adolescent-reported FAD scores or researcher-rated GARF scores (F(2 83) = 1.59, p = 0.21 and F(2,85) = 0.94, p = 0.39, respectively).
Discussion
Adolescent results
Adolescent inpatients were equally distributed by sex and most commonly had a principal diagnosis of a depressive disorder (major depressive disorder, dysthymic disorder, depressive disorder not otherwise specified), followed by psychotic disorders. These findings contrast with previous studies that have reported more male subjects and a predominance of externalizing disorders among child and adolescent inpatients [3], [4], [8], but might reflect a difference in sample age. Studies of child and adolescent inpatients necessarily include a younger age range; and younger children, particularly boys, are referred for the treatment of externalizing problems more than internalizing problems [11]. Some studies indicate that by adolescence, behaviour disorders are surpassed by mood disorders as the most common diagnosis and consequently the inpatient sex ratio becomes more balanced [9].
The rate of substance abuse diagnosis may appear low given its association with the two most common diagnoses of mood and psychotic disorders. Yet results were consistent with other studies of Australian child and adolescent inpatients that identified substance abuse as a comparatively minor problem [8] or did not mention substance abuse at all, an omission that identified substance abuse as an uncommon diagnosis [7], [9]. International studies have also not mentioned substance abuse [1], [4] or have not listed it as a main diagnosis [5].
The unit's admission criterion that patients’ significant problem must be psychiatric might have the effect of restricting the admission of patients with primarily substance abuse problems. But it seems unlikely that this criterion has caused substance abuse to be underrepresented in the present study compared to other inpatient units, because the criterion is standard and unremarkable for an inpatient facility. Rather, current results appear to indicate that the level of diagnosable substance abuse among adolescent inpatients is low. The full extent of drug and alcohol use is not indicated by diagnostic information, however, because inpatients may use these substances without fulfilling diagnostic criteria.
The finding might also suggest that the common association between mental illness and substance abuse described in young adults [31] is not as frequent in adolescents and may be a developmental phenomenon. For some adolescents a mental illness may predicate the development of later associated substance abuse. For others, substance abuse in adolescence might increase their risk of mental illness in early adult life.
Most adolescents had multiple Axis I diagnoses, indicating the protean nature of their symptoms and the challenges involved in diagnosis and treatment. The result was consistent with previous findings [4] and supports the Cornsweet (1990) conclusion that adolescent inpatients are diagnostically complex [1].
The results of self- and other-reported symptomatology measures indicated the high level of mood disturbance. Most adolescents reported a clinical level of internalizing problems, fewer reported clinical levels of externalizing problems and fewer again reported thought disturbance, although levels were still high compared to normative figures. Parents rated adolescent symptomatology more severely: 70% of parents rated their adolescent as having clinical-level thought problems, compared to 35% of adolescents. Case clinicians concurred with parents in reporting high symptomatology, suggesting that these seriously unwell adolescents underreported symptoms.
Most adolescents had not been attending school at the time of admission. The mean length of absence (14 weeks) and the common diagnosis of Axis IV educational/occupational problems indicated significant and widespread impairment in this critical area. Social functioning was also an area of impairment, with 40% of parents reporting clinical levels of social problems and 41% reporting clinical-level problems in overall competence. Researcher-rated GAF scores were consistent with parent report and indicated that moderate to serious impairment of functioning in key domains was typical. Adolescents reported comparatively less impairment, again suggesting that they underreported problems.
Family demographics
Results did not fully support previous findings of socioeconomic disadvantage among adolescent inpatients [1], [3]. The range of parental occupation and the rate of employment suggested that families came from a cross-section of socioeconomic backgrounds. Other inexact markers of SES were familial NESB status and single parent status. The rate of NESB status somewhat approximated national rates, while the rate of single-parent families was elevated. The association between single-parent families and child and adolescent health issues is widely reported [3], but the exact reasons for the association are unclear.
An unexpected finding was that NESB status was associated with a principal diagnosis of a psychosis-related disorder. A possible explanation for the association is that some NESB families were refugees, and associated trauma contributed to the manifestation of psychotic symptoms [32]. Contrary to this explanation, only two families had been refugees. It remains possible that non-refugee families also experienced problems and stressors in their country of origin, including a family history of psychosis, which compelled them to migrate.
The process of acculturation is another possibly relevant factor [33]. Most adolescents from NESB families were born in Australia but their parents may have faced challenges of acculturation and experienced inadequate social support, which directly affected their child. Also the adolescent's experience of discord between the family's culture and the culture of the wider community may have negatively impacted upon their mental health [34].
A weak association was found between NESB and low SES. The weakness of the association may reflect the small sample size. Mental illness generally is associated with lower SES [35], but the association is particularly strong for psychotic illness [36]. Socioeconomic disadvantage may be an important contributing factor to the elevated rate of psychosis found among NESB patients [37].
Family and parent functioning
Adolescents reported greater problems in family functioning than did their parents, in a reversal of the pattern of reporting for adolescent symptoms. GARF results supported adolescent report, indicating that the average family unit was dysfunctional, with ‘unsatisfying relationships tending to predominate’ [24]. The result is consistent with other studies of child and adolescent inpatients [7] and emphasizes the family unit as a necessary focus for clinical attention.
The results of parent self-report mental health measures were less clear. Approximately one in 15 parents reported clinical-level personality disturbance on the PDQ-4 while one in six parents experienced clinical levels of psychological distress according to BSI results. The results are somewhat paradoxical when it is considered that the PDQ-4 tends to over-identify disturbance [38], while the BSI is reportedly more conservative. Results might reflect that the PDQ-4 taps symptoms experienced over the past several years while the BSI records symptoms experienced in the past week. Parents may have experienced psychological distress in response to their adolescent's inpatient admission but in general their levels of psychological disturbance were comparable to levels in the general population.
Parent results may have been influenced by response bias. Participation was moderate, with 60% of fathers and 65% of mothers participating. High-functioning parents were possibly more likely to agree to participate and complete the assessment than dysfunctional parents. A post-hoc analysis indicated that the average familial SES of participating parents was higher than non-participating parents, but not significantly so. It remains possible that participating parents were unrepresentative of the parent group as a whole. Also, parental mental health was assessed through self-report, and parents may have underreported problems.
The findings suggest that some parents maintained their own mental health and that these parents might be able to play a positive role in the treatment and recovery of their adolescent. But the positive results contradicted other studies [7] and were inconsistent with the high level of family dysfunction, suggesting that results were affected by response bias and self-report bias.
Limitations
It is possible that the sample was unrepresentative of adolescent inpatients generally. Adolescents with defiant behaviours might have declined to participate and adolescents with severe psychosis may have been unable to participate. But few adolescents declined or were unable to participate, suggesting that these were not major causes for sample bias. A bias may have also occurred because participants were not recruited consecutively from the unit. The use of a small number of case clinicians to refer consecutive cases, however, provided randomness to the selection process, because clinicians were allocated patients primarily according to caseload capacity.
Although clinicians were asked to refer consecutive patients, it is possible that they did not ask patients they believed would refuse involvement, perhaps due to defiant or oppositional traits. Also, patients with short-term, crisis-driven admissions were excluded from the study. These patients may have had acting-out behaviour problems that resolved quickly with containment. Short-term admissions were excluded because the brief admission period indicated that the patient did not require standard inpatient treatment and that their problems may not have been primarily mental illness. A considerable proportion of participants had externalizing behaviour problems, indicating that inpatients with defiant or oppositional behaviour were not entirely excluded.
Conclusions
Adolescent inpatients typically experienced moderate to extreme levels of difficulty in emotional, behavioural, social and educational domains beyond that which can be conveyed by Axis I diagnostic information alone. Family functioning was an area of particular difficulty. These results indicate that the treatment of psychiatric symptoms is only part of the required intervention [3].
The predominance and severity of mood disorders likely reflects the emergence of these problems in adolescence [39], growing community recognition of mood disorders including depression [40], and indicate the increasing demand on treatment.
Some preliminary findings arose that are worthy of further investigation. Parental mental health appeared somewhat robust, but the finding contradicts other studies [7] and may reflect self-report bias and response bias. Further investigation is indicated to explore the possible association between psychotic disorders, familial NESB and low SES.
Footnotes
Acknowledgements
The authors thank Nicola Williams for her contribution to data collection and clinical interviews and Dr David Scholl and the Stepping Stones inpatient unit staff for their contribution. This research was funded by the Pratt Foundation.