
Abstract
Objective:
The objective of this study is to examine suicide attempts and completions among mothers who had a child taken into care by child protection services (CPS). These mothers were compared with their biological sisters who did not have a child taken into care and with mothers who received services from CPS but did not have a child taken into care.
Methods:
A retrospective cohort of mothers whose first child was born in Manitoba, Canada, between April 1, 1992, and March 31, 2015, is used. Rates among discordant biological sisters (1872 families) were compared using fixed-effects Poisson regression models, and mothers involved with CPS (children in care [n = 1872] and received services [n = 9590]) were compared using a Poisson regression model.
Results:
Compared with their biological sisters and mothers who received services, the adjusted incidence rate ratio (aIRR) of death by suicide was greater among mothers whose child was taken into care by CPS (aIRR = 4.46 [95% confidence interval (CI), 1.39-14.33] and ARR = 3.45 [95% CI, 1.61-7.40], respectively). Incidence rates of suicide attempts were higher among mothers with a child taken into care compared with their sisters (aIRR = 2.15; 95% CI, 1.40-3.30) and mothers receiving services (aIRR = 2.82; 95% CI, 2.03-3.92).
Conclusions:
Mothers who had a child taken into care had significantly higher rates of suicide attempts and completions. When children are taken into care, physician and social workers should inquire about maternal suicidal behaviour and provide appropriate mental health.
The impact of being placed in care of child protection services (CPS) on children has been examined extensively. These children have worse health and social outcomes than those of children in the general population. 1 –5 Several population-based studies have also identified these children as being at higher risk for suicide and suicide attempts. 5 –7 Less known are the outcomes of mothers whose children are placed in care by CPS. While mothers with mental illness have significantly greater involvement with CPS, women have reported that they developed mental health conditions, or their existing mental health conditions worsened, after custody loss. 8,9 Being a mother has been identified as being protective against suicide; however, experiencing the death of a child increases this risk, particularly if the child is young. 10 Parents who lose custody of their children have been shown to experience this situation as a ‘living death’. 11 The purpose of this study is to examine whether mothers who lost custody of their children due to involvement with CPS have higher rates of suicide attempts and completions than mothers not separated from their children.
Previous observational studies investigating rates of suicide in at-risk populations have controlled for individual mental health, socioeconomic status, and various demographic variables, as these factors have been linked to suicide and suicide attempts. 12,13 Mothers whose children are taken into care often have very different life circumstances than mothers in the general population. To account for some of these differences, we used to comparison groups. The first comparison is between mothers who had a child taken into care and their biological sisters who did not have a child taken into care. This was done because suicide attempts and completions often cluster within families due to shared genetic and environmental factors, and family fixed-effects models of discordant siblings account for stable family characteristics. 14 –16 The second comparison was between mothers who had a child taken into care and mothers who received services from CPS but were not separated from their child or children. This comparison was made as the instability that resulted in involvement with CPS may also contribute to differences in suicide attempts and completions. While the comparison groups are imperfect, both capture important similarities. 17
Methods
Setting
Manitoba is a central Canadian province with approximately 1.2 million residents at the time of the 2011 census. 18 Manitoba residents receive universal health care coverage. While Manitoba is representative of Canada in many aspects, ranking in the middle for several health indicators and slightly below average on education indicators, rates of children placed in out-of-home care are among the highest in the country. 19,20 With approximately 3% of children in care, Manitoba has the highest rates of children in care among Canadian provinces and one of the highest rates in the world. 21 Several Canadian provinces and territories have similarly high rates, but provinces with rates lower than those seen in Manitoba still have higher rates than many other countries. 22 Suicide is a leading cause of death among young Canadians, with a rate of 4.8 per 100,000 in the female population in 2012. 23,24 This is above the rate of 2.6 in the United Kingdom and below the rate of 5.6 seen in the United States. 24 Manitoba ranks in the middle of suicide rates among Canadian provinces and territories. 25
Data
This study uses linkable administrative data found in the Population Research Data Repository housed at the Manitoba Centre for Health Policy. This Repository contains province-wide, routinely collected individual data over time and across geographic space for each provincial resident. 26 Births, deaths, arrival, and departure dates are identified for each resident, with follow-up comparable to that of the largest cohort studies based on primary data. 27 This research links data from the population registry with individual-level information from physician claims, hospital discharge abstracts, vital statistics, Child and Family Services (CFS) case reports, and the Canadian Census. An encrypted personal health number linked these de-identified data sets. Information on linkage methods, confidentiality/ privacy, and validity can be found elsewhere. 28,29 Children are linked to mothers using hospital birth record information; mothers are noted in essentially all cases. 30
Cohort Formation
Individuals included in this study were drawn from the whole Manitoba population of women whose first child was born in Manitoba between April 1, 1992, and March 31, 2015. The cohort was divided into 3 groups. Group 1 included all women having at least 1 child taken into care before March 31, 2015. For mothers having multiple children removed from their home, the oldest child was selected as the index child; the index date is the date the index child was first taken into care. Mothers in group 1 may have sisters who also had a child taken into care; to ensure independence, 1 sister is randomly selected in group 1. Group 2 included biological sisters of mothers in group 1 who did not have a child taken into care. The index date for these mothers is the date that their oldest child turns the age their sister's child was when taken into care. Again, 1 sister per family was randomly selected when families had more than 1 sister in group 2. Group 3 is a group of mothers without a sister in the cohort; these women received other protection or support services from CPS but did not have a child taken into care. Other protection or support services are provided to resolve family matters, with the children not removed from the home; these services include counselling, guidance, support, education, and emergency shelter services. 31,32 The index date for mothers in group 3 is the date they first began receiving services from CPS. Mothers not living in Manitoba for at least 2 years before the index date, or those for whom the index date was after March 31, 2015, were excluded. Figure 1 diagrams the cohort formation.
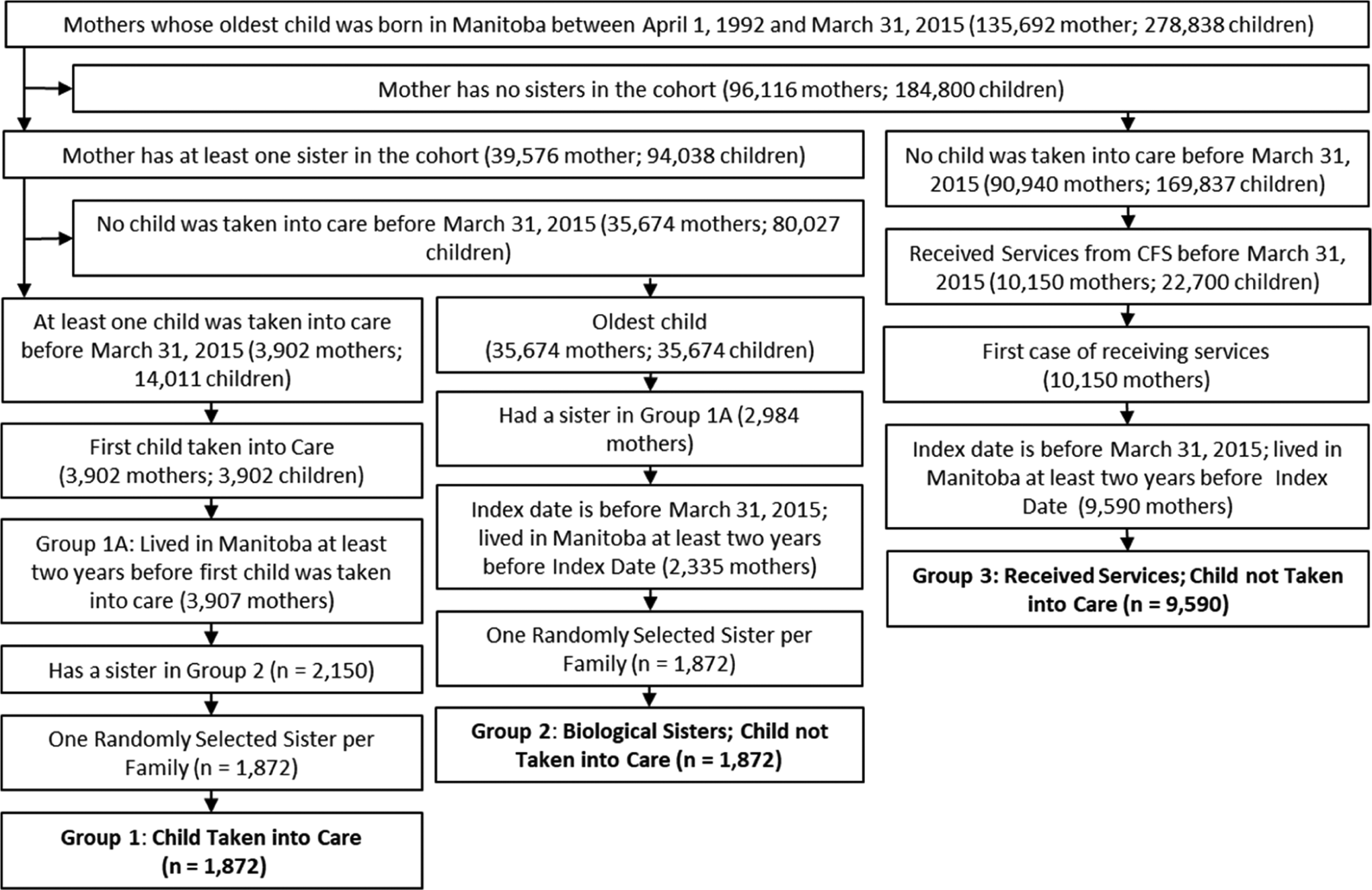
Cohort selection.
Variables
Outcomes
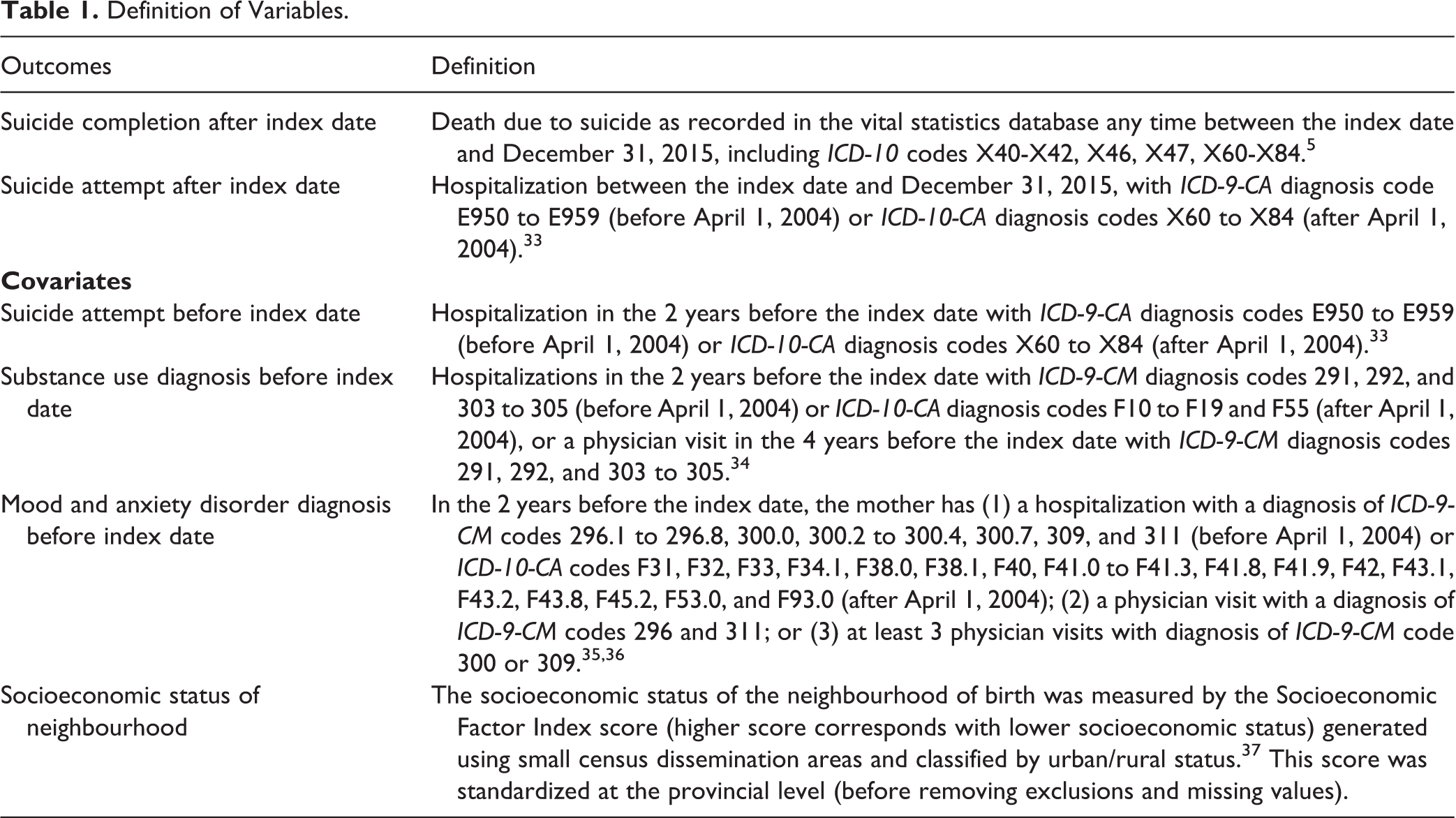
For each mother, we examined suicide attempts and completions from the index date up to December 31, 2015 (see Table 1 for definitions). Both variables were defined using administrative data, with definitions based on previous work using these data.
Definition of Variables.
Covariates
Potential confounders were selected based on clinical relevance; among the best predictors of suicide or suicide attempts are previous suicide attempts and mental illness. 38 Each model adjusted for a series of maternal mental health conditions in the 2 years before the index date: suicide attempts (yes/no), number of substance use diagnoses (0, 1, 2+), and number of mood and anxiety disorder diagnoses (0, 1, 2+) (see Table 1 for definitions). We included the number of diagnoses in the 2 years before the index date to estimate the severity of the diagnosis. Socioeconomic status, mother’s age, and child’s age have also been identified as predictors of suicide attempts and completions. 39,40 Each model adjusted for socioeconomic status (see Table 1 for definition) and location of neighbourhood (urban, rural south, rural mid, rural north), age of mother, and age of child at the index date.
Ethics
This study was reviewed and approved by the Health Research Ethics Board at the University of Manitoba (#H2016:182) and the Health Information Privacy Commission at Manitoba Health, Seniors and Active Living (#2016/2017-09). This study used de-identified administrative data files, which did not require informed consent from participants.
Statistical Analysis
Two analyses were conducted. First, mothers having a child taken into care (group 1) were compared with their biological sisters who did not have a child taken into care (group 2). Adjusted incidence rate ratios (aIRRs) for each outcome were obtained from family fixed-effects Poisson regression models. This reduced the potential for confounding, as this approach helps account for shared familial characteristics, environment, and genetic predisposition. 41 The second analysis compared mothers with a child taken into care with mothers who received other protection or support services from CPS (but did not have a child taken into care). Adjusted IRRs for each of the outcomes were obtained using Poisson regression models. For each analysis, the log of the total number of person-years at risk was included as an offset to ensure modeling of a rates as opposed to a count of events. Data management, programming, and analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC).
Results
Overall, 13,334 mothers were included in this study. Of these mothers, 1872 had a child taken into care, 1872 were biological sisters not having a child taken into care, and 9590 mothers received services from CPS but did not have a child taken into care. Mothers were followed from the index date until their coverage ended or December 31, 2015 (whichever came first), resulting in a total of 131,582 person-years of follow-up. Those in group 1 were followed for an average of 8.96 years, their sisters (group 2) were followed for an average of 8.38 years, and the mothers (group 3) receiving services were followed for an average of 10.34 years. Mothers whose children were taken into care were younger and lived in neighbourhoods of lower socioeconomic status at the index date. These mothers were also more likely to have had a suicide attempt and had more substance use diagnoses in the 2 years before the index date (Table 2). Almost all mothers (99%) had contact with a physician after the index date.
Characteristics of Mothers, Manitoba, Canada, 1992-2015.
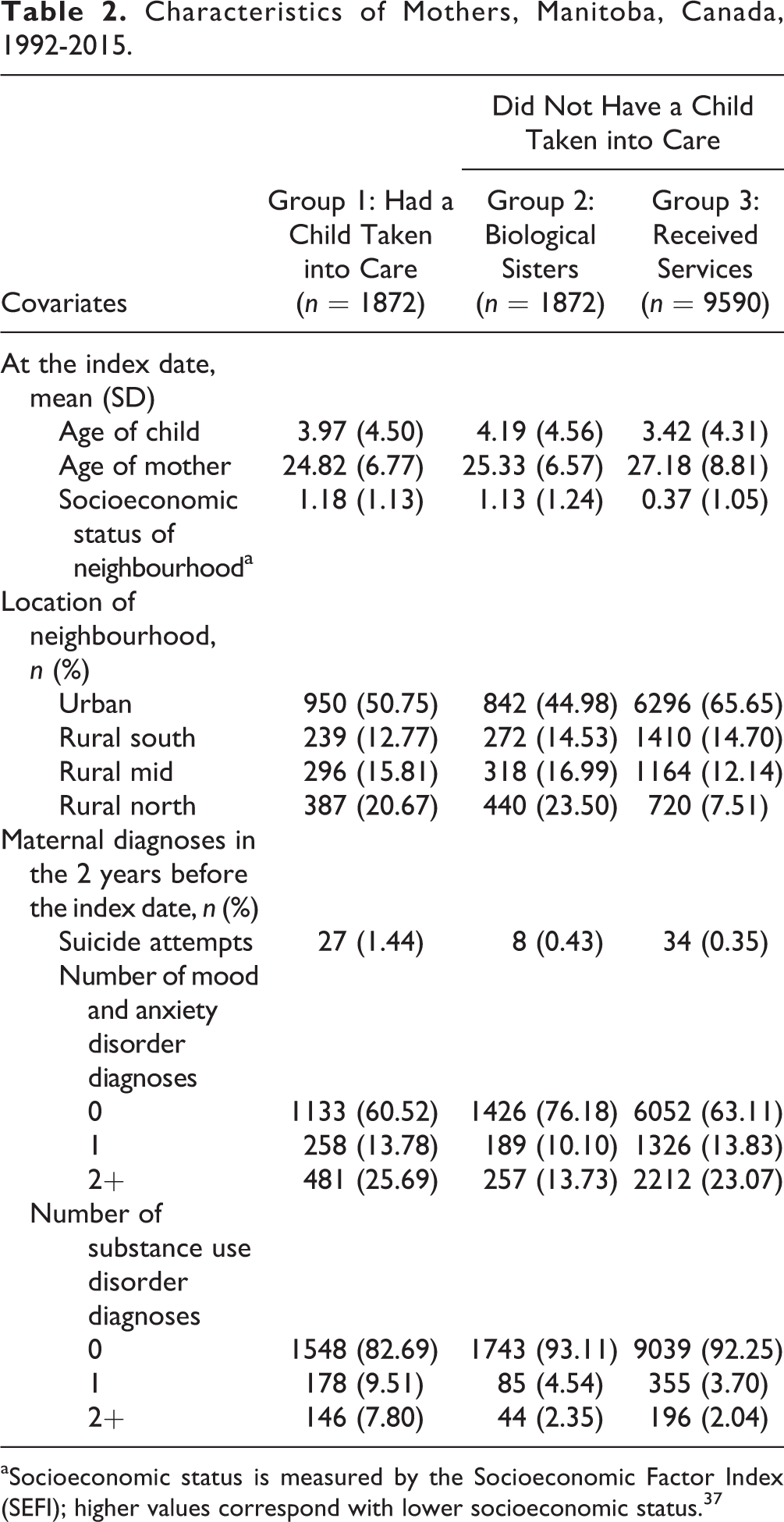
aSocioeconomic status is measured by the Socioeconomic Factor Index (SEFI); higher values correspond with lower socioeconomic status. 37
Mothers whose children were taken into care had 286 additional suicide attempts and 76 suicide completions per 100,000 person-years compared with their sisters who did not have a child taken into care (Table 3). Compared with mothers who received services, mothers whose children were taken into care had 352 additional suicide attempts and 77 suicide completions per 100,000 person-years.
Rates (per 100,000 Person-Years) of Suicide Attempts and Completions, Manitoba, Canada, 1992-2015.
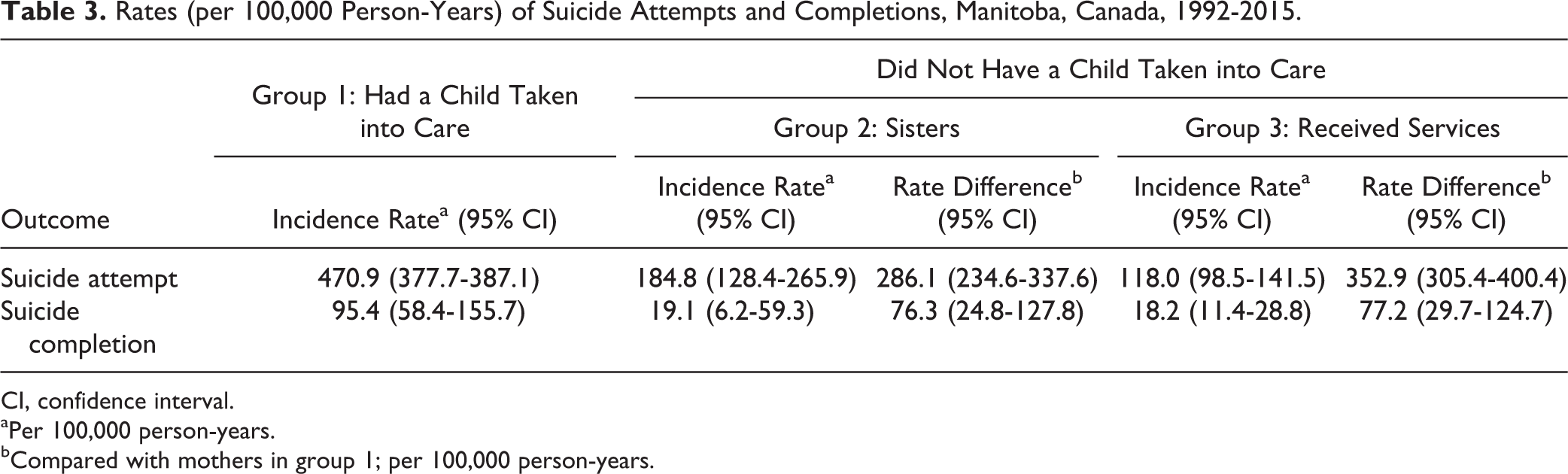
CI, confidence interval.
aPer 100,000 person-years.
bCompared with mothers in group 1; per 100,000 person-years.
Compared with sisters and mothers who received services, the incidence rate of suicide attempts and completions was significantly higher among mothers having a child taken into care by CPS (Table 4). The sister comparison helps control for shared familial and genetic confounding, whereas the comparison with mothers who received services controls for maternal instability requiring CPS involvement.
Unadjusted and Adjusted Incidence Rate Ratios of Suicide Attempts and Completions, Manitoba, Canada, 1992-2015.
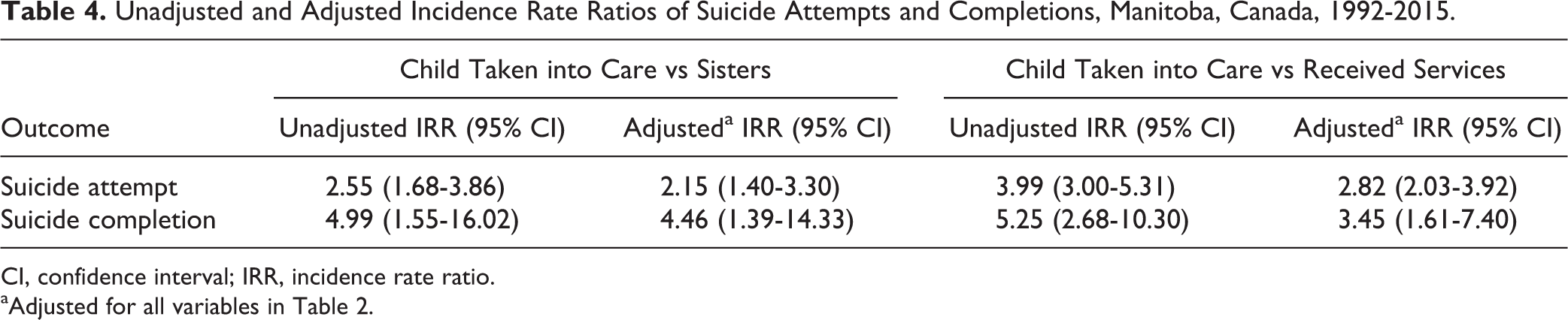
CI, confidence interval; IRR, incidence rate ratio.
aAdjusted for all variables in Table 2.
Discussion
To our knowledge, this study is the first to examine suicide attempts and completions among mothers who had a child taken into care by CPS. Mothers who have a child placed in care have much higher rates of suicide attempts and completions than their biological sisters and mothers who received services, even when adjusting for many risk factors.
These results of our study are concordant with, and may be explained by, earlier findings indicating that mothers losing custody of their child to CPS have increased distress and psychiatric problems. 9 Most mothers experience a great deal of pain when they lose custody of a child, which often leads to a loss of self-worth and confidence. 42,43 Regardless of their situation, mothers want to be seen as ‘good mothers’, and when a woman associates being a ‘good mother’ with being a ‘good person’, the involvement with child protective services will place in question her mothering and her identity. 44 Feelings of guilt, responsibility, shame, stigmatization, and loss of self-worth often associated with this type of custody loss may also contribute to the increased rates of suicide attempts and completions. 42,43,45
Mothers whose children are taken into care often have existing mental health conditions that contributed to the loss of custody of their children. 46 Mothers have reported the development and worsening of mental health conditions after separation from their child. 8,9 Strengthening resources and capabilities of mothers who are at risk of having a child taken into care may result in better outcomes for both mother and child. 47 –49 In situations where a child does need to be removed from the home, service providers ensure that the biological mothers are receiving adequate mental health supports. This could both prevent the deterioration of mental health in these mothers and ensure that the stresses associated with the separation do not become another barrier to reunification.
The use of the population-based repository at the Manitoba Centre for Health Policy offers significant strengths, including a large sample size, minimal attrition, and a large number of predictors over many years. 50 Study limitations concern unmeasured confounders and the measurement of variables. This study only captures physician-treated mental illness. Therefore, we may be missing women who experience mental illness but do not seek treatment or treatment from physicians, resulting in an underestimation of history of mental illness in our cohort. 51 In addition, for both mood and anxiety disorders and substance use disorders before the index date, we do not know the severity of the disease, its duration, or resulting disability. Suicide is often undercoded in administrative data, as physicians may list underlying mental illness as the diagnosis or not accurately chart the occurrence of suicidal behaviour. 52 These data have low sensitivity in tracking the prevalence of suicide outcomes; using hospital and physician claims data to identify suicidal outcomes in patients may undercount one-half to two-thirds of these outcomes. 52 Only women who received physician treatment owing to a suicide attempt or whose death has been classified as a suicide were included. Our definition of suicide using vital statistics files excludes deaths related to motor or other vehicle collisions, which could potentially be suicide-related deaths (particularly in rural areas). These limitations may result in the underestimation of the burden of suicide among our study population. As in many observational studies, the results of this study may be biased by unmeasured confounders. Variables that have been linked with suicide attempts and completion and were not accounted for in this study include maternal education, domestic violence, maternal history of abuse and neglect, and Indigenous status. 7,53,54 In Manitoba, Indigenous individuals are more likely to be involved with CPS and also have higher rates of suicide and suicide attempts. 20,55 While this confounder was not adjusted for in the analysis comparing mothers whose children were taken with mothers who received services, the discordant sibling analysis takes Indigenous status into account (because it is a stable family characteristic). Methodologically, this work builds on efforts to incorporate family variables into cohort studies. 56 The setting of this research—Manitoba, Canada—has a very high rate of children in care. 21 To ensure generalizability, this study needs to be replicated in other settings with different policies around child welfare.
Conclusion
Women who have children taken into care have increased psychological distress and are at greater risk for suicide and suicide attempts. For mothers whose children are taken into care, greater mental health supports should be provided to minimize the impact of this event and to address any underlying mental health issues contributing to the child being taken into care.
Footnotes
Acknowledgement
Data used in this study are from the Population Research Data Repository housed at the Manitoba Centre for Health Policy, University of Manitoba and were derived from data provided by Manitoba Health, Seniors and Active Living, Manitoba Families, and Vital Statistics under project 2016/2017-09. The results and conclusions are those of the authors and no official endorsement by the Manitoba Centre for Health Policy, Manitoba Health, Seniors and Active Living, or other data providers is intended or should be inferred.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Preparation of this manuscript was supported by a Social Sciences and Humanities Research Council of Canada Joseph-Armand Bombardier Canada Doctoral Scholarship, a Graduate Enhancement of Tri-council Stipend, and a Women’s Health Research Foundation of Canada Full Time Scholarship.