
Abstract
Objective:
The objective was to compare mental illness diagnoses and treatment use among mothers who lost custody of their child through involvement with child protection services and those seen in mothers dealing with the death of a child.
Methods:
We studied mental health outcomes of a cohort of women whose first child was born in Manitoba, Canada between 1 April 1997 and 31 March 2015. Of these women, 5,792 had a child taken into care, and 1,143 mothers experienced the death of a child (<18 y old) before 31 March 2015. Adjusted relative rates (ARR) of 3 mental health diagnoses and 3 mental health treatment use outcomes between these 2 groups were examined.
Results:
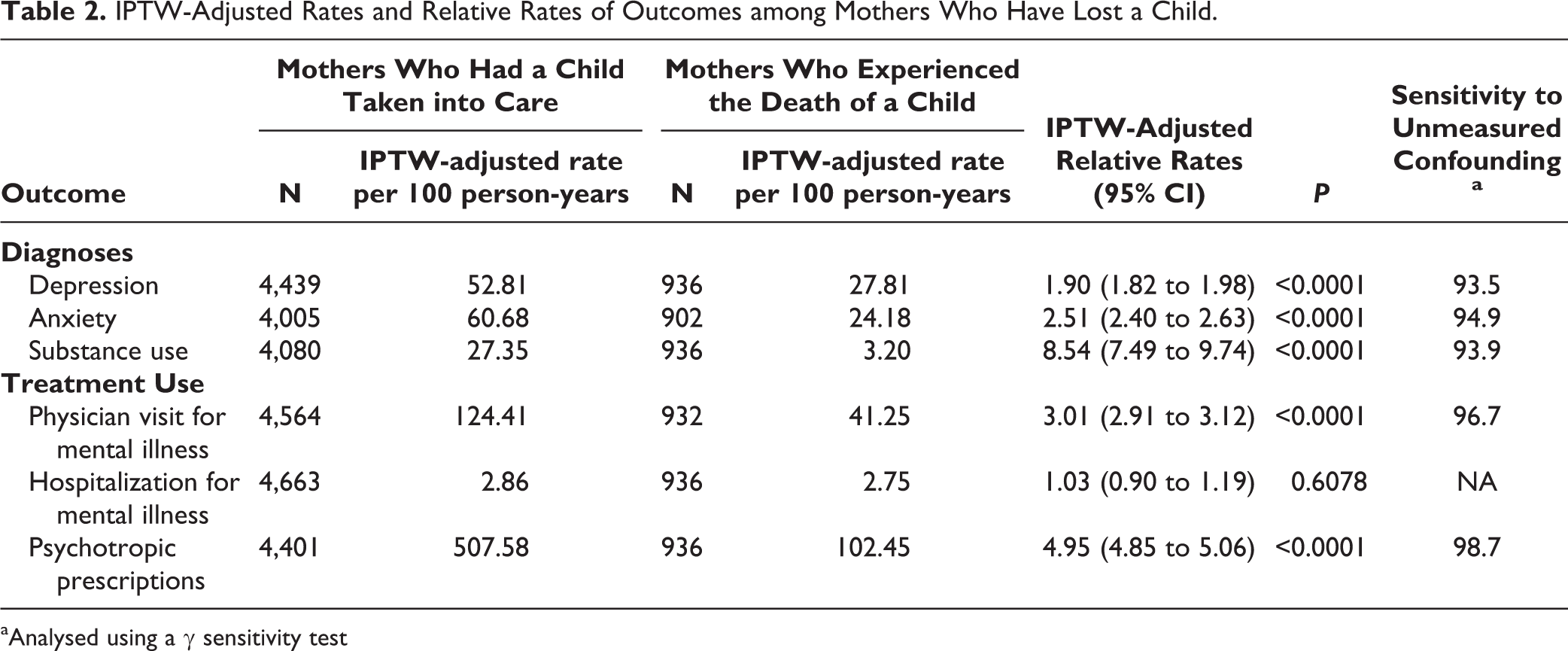
Mothers with a child taken into care had significantly greater ARR of depression (ARR = 1.90; 95% CI, 1.82 to 1.98), anxiety (ARR = 2.51; 95% CI, 2.40 to 2.63), substance use (ARR = 8.54; 95% CI, 7.49 to 9.74), physician visits for mental illness (ARR = 3.01; 95% CI, 2.91 to 3.12), and psychotropic medication use (ARR = 4.95; 95% CI, 4.85 to 5.06) in the years after custody loss compared with mothers who experienced the death of a child.
Conclusion:
Losing custody of a child to child protection services is associated with significantly worse maternal mental health than experiencing the death of a child. Greater acknowledgement and supportive services should be provided to mothers experiencing the loss of a child through the involvement of child protection services.
The loss of a child is traumatic for mothers. 1 The grief associated with the death of a child, and the health and social implications of this grief, are well documented. Mothers experiencing the death of a child have worse mental health than mothers who did not lose a child. 2 –4 Another type of loss parents can experience is the loss of custody of a child due to involvement with child protection services. This is often experienced as a “living death,” characterized by ambiguous loss, as parents no longer have control over how and when they can interact with their children and parents may go for long periods without being able to see their children. 5 Distress experienced by mothers losing custody of their children is often overlooked, because they have failed society’s ideal of “good parenting.” 6
Maternal mental health after experiencing the death of a child has been frequently examined but research into the health of mothers who have lost custody of a child due to involvement with child protection services is limited to a few qualitative studies. 6 Women who lose custody of their child due to involvement with child protection services have been shown to have many of the same feelings as mothers following the death of a child 7 ; however, outcomes seen in these 2 groups of mothers have never been compared. This study addresses this gap in knowledge by comparing the adjusted relative rates of mental illness diagnoses and treatment use for mothers having a child taken into care with those of mothers experiencing the death of a child. This study provides the first population comparison of mental health between these 2 groups of mothers.
Methods
Setting
Manitoba is a central Canadian province; at the time of the 2011 census, there were approximately 1.2 million residents. Residents of Manitoba receive universal healthcare coverage. Although Manitoba is representative of Canada in many aspects—ranking in the middle for several health indicators and slightly below average on education indicators—rates of children placed in out-of-home care and infant mortality are among the highest in the country. 8 –10 With approximately 3% of children in care, Manitoba has one of the highest rates of children in care in the world. 11 Although Manitoba does have the highest rates of children in care among the provinces, several provinces and territories also have similarly high rates; Canadian provinces with relatively low rates have higher rates than many other countries around the world. 12
At over 16% of the population, Manitoba has the highest proportion of residents of indigenous descent among the Canadian provinces. 13 In Canada, indigenous children are over-represented both in the child welfare system and in child mortality. In 2014, 90% of Manitoba children in care were indigenous; in the population, only 26% of children are indigenous. 9 Infant mortality rates in indigenous communities range from 1.7 to over 4 times the overall Canadian and/or non-indigenous rates. 14 This over-representation is often attributed to historical social and health inequalities and injustices, including the legacy of residential schools. 15
Data
This study used the linkable administrative data found in the Population Research Data Repository housed at the Manitoba Centre for Health Policy, which contains province-wide, routinely collected, individual data over time and across geographic space for each Manitoba resident. 16 Births, deaths, arrival, and departure dates are identified for each resident. 17 This study included data from the population registry, linked at the individual-level with physician claims, hospital discharge abstracts, pharmaceutical claims, Child and Family Services (CFS) case reports, vital statistics, and the Canadian Census. An encrypted personal health number was used to link these de-identified datasets. Information on linkage methods, confidentiality/privacy, and validity can be found elsewhere. 18 Children are linked to biological mothers using hospital birth record information. 19
Cohort Formation
Individuals included in this research were drawn from the whole Manitoba population of women whose first child was born in Manitoba between 1 April 1997 and 31 March 2015. The cohort was divided into 2 groups. Group 1 included all women who had a child taken into care before the age of 18 y. For these mothers, the index child is the date their first child was taken into care; when more than one child was taken into care during this first incident, the oldest child was selected as the index child. Mothers in Group 1 were followed for a total of 35,228 person-years after the index date. Group 2 included all mothers with a child who died before the age of 18 y. For mothers experiencing more than one death before age 18 y, the index child was the first child who died before 31 March 2015. The index date for these mothers is the date their index child died; mothers in Group 2 were followed for a total of 8,290 person-years after this date. All mothers lived in the province for at least 2 y before the index date. Figure 1 diagrams the cohort formation.
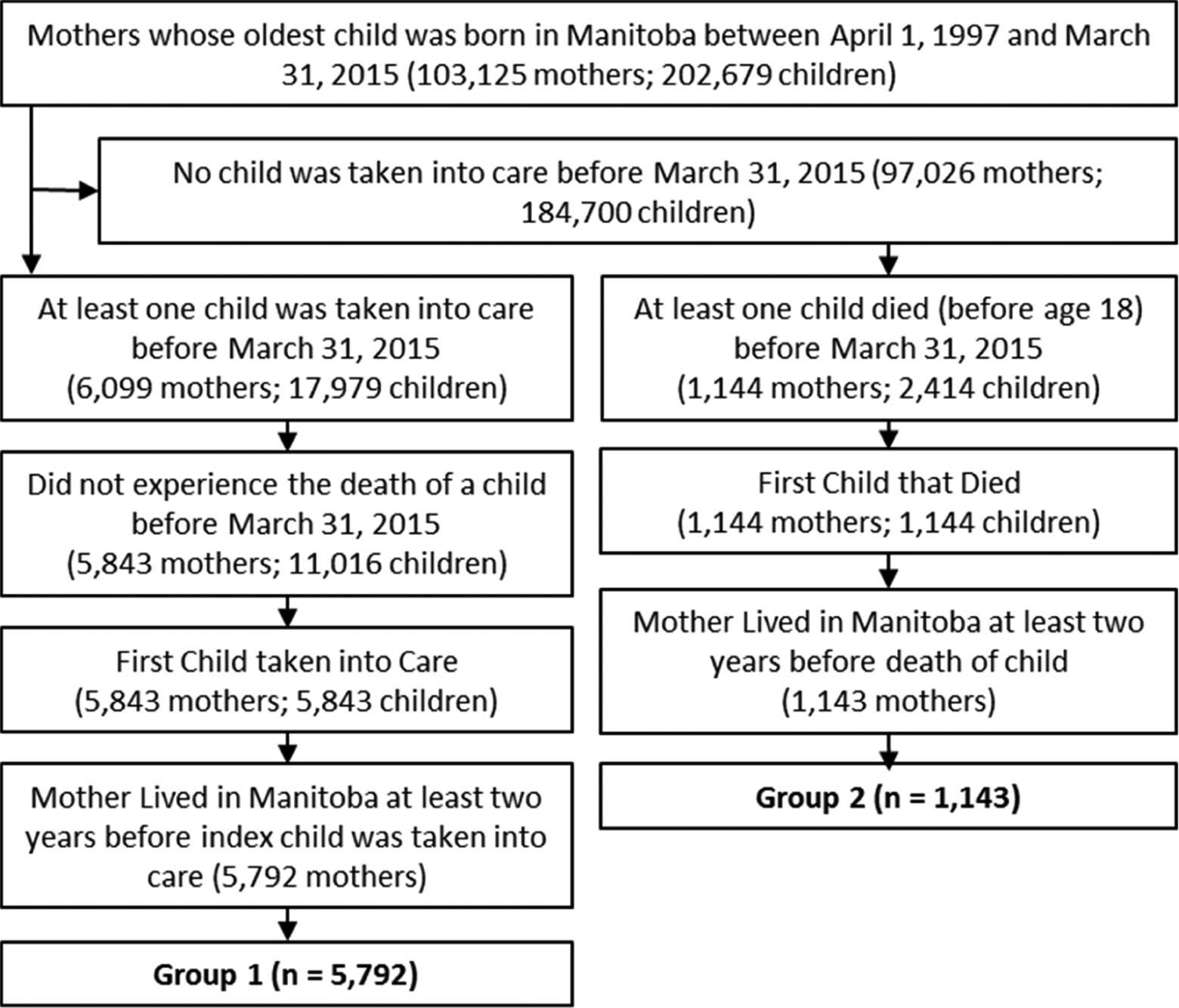
Cohort formation of mothers who experienced the loss of a child.
Outcomes of Interest
A series of mental illness diagnoses and treatment use outcomes were measured between the index date and the study end date (31 March 2015). The mental illness diagnoses examined were depression, anxiety, and substance use. Treatment use for mental illness included physician visits for any mental illness, hospitalizations for any mental illness, and psychotropic prescriptions. Each outcome was measured as a count to examine the number of diagnoses or events experienced. Definitions were based on pre-existing work using the same data sets. Supplemental Table S1 in Appendix A presents the definitions of all variables.
Statistical Analyses
Mothers who experienced the death of a child and mothers who lost custody of a child may be quite different in the years leading up to their loss; these differences may contribute to the mental health outcomes of the mothers following their loss. To make these 2 groups of mothers more comparable, we used statistical methods to balance baseline characteristics.
For each of the 6 outcomes, a multistep algorithm applied high-dimensional propensity score (hdPS) adjustments to balance the differences between the 2 groups of mothers. 20 We used hdPS adjustments, as this method is better at adjusting for confounding by indication, resulting in effect estimates closer to randomized control trial findings than standard covariate adjustments. 20,21 Unlike traditional propensity score methods, which are limited to investigator-specified covariates, the multistep algorithm used to derive hdPSs identifies potential confounders from a database by selecting variables correlated to both the exposure and each of the outcomes, prioritizing covariates by prevalence and potential for bias. 22
Covariates were drawn from data collected during the 2 y before the loss of a child, which included: (1) medical service tariff codes, (2) physician diagnostic codes, (3) hospital procedure codes, (4) hospital diagnostic codes, and (5) prescription medication claims. These data are a set of proxies describing the health status of the women in our study. 22 Examining health care use, physician diagnoses, and medications dispensed within these 5 data dimensions before the index date makes use of many proxy covariates to control for co-morbid conditions, concurrent medication use, and disease severity. In addition to the health variables obtained from these data, a series of sociodemographic variables were included in the models. In the 2 y before the loss of the child, we included whether the mother had moved and whether the mother had received Employment and Income Assistance (EIA; analogous to welfare). We also included the mother’s age and the child’s age at the loss of the child, as well as the child’s birth order, neighbourhood income (low/high) and the neighbourhood location (urban/rural). See Appendix A for definitions of low neighbourhood socioeconomic status, residential mobility, and welfare receipt.
The 5 datasets used to assess the health status in the 2 y before a mother’s loss are extremely large. For example, the physician diagnoses are claimed as ICD-9-CM codes; these include approximately 17,000 different diagnostic codes. For each outcome, hdPSs were constructed including all sociodemographic variables and the top 500 health covariates. The algorithms used to create the hdPSs select variables correlating to both exposure and outcomes; given the 6 different outcomes, the variables selected could differ for each outcome model. We excluded mothers with extreme weights; weights were trimmed at the value corresponding to the 2.5th and 97.5th percentile. Balance was assessed using standardized differences (see Appendix B).
We adjusted for the confounders included in the HDPS models using Inverse Probability of Treatment Weights (IPTWs). Each outcome model used a summarized data set for the total number of events produced for the 2 groups of mothers. IPTW-adjusted relative rates for each of the outcomes of interest were obtained from Poisson regression models. The log of the total number of person-years at risk was included as an offset to ensure the modelling of relative rate as opposed to a relative count of events.
Using IPTWs can reduce confounding but does not account for unobserved confounders that may impact our findings. The most important issue is whether bias from an unobserved confounder would make our relationships seem significant when they in fact are not. To estimate how large any remaining bias would have to be to change our study’s findings, we used a gamma sensitivity analysis. The gamma sensitivity analysis uses both the magnitude of the estimated effect as well as its precision to determine how large the effect of an unobserved confounder would need to be—over and above the balancing of all the observed characteristics in the HDPS —to make our significant relationships non-significant. 23 All data management, programming, and analyses were performed using SAS® version 9.4.
Results
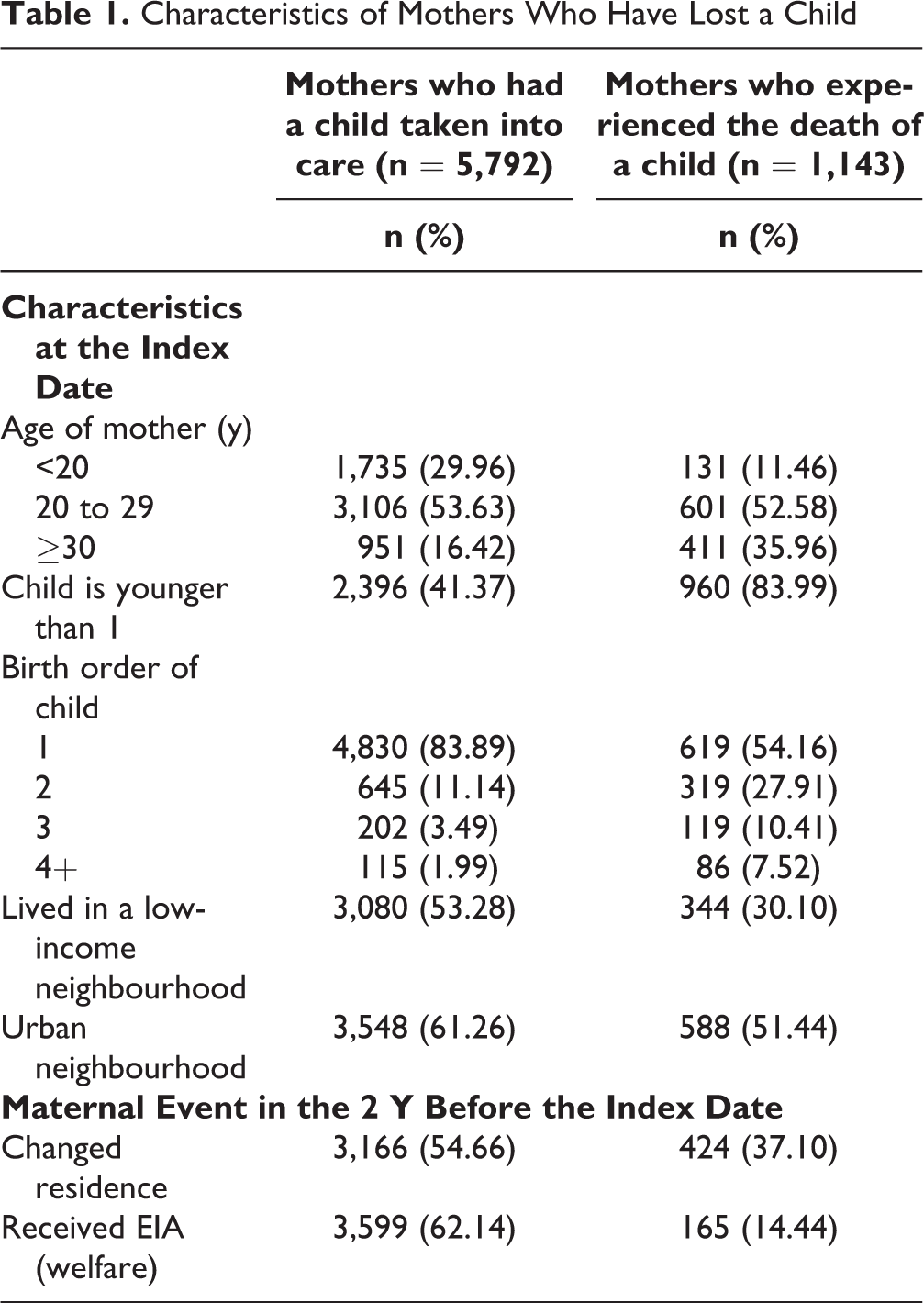
Our cohort included 6,935 women suffering the loss of a child between 1997 and 2015; 5,792 had a child taken into care, and 1,143 experienced the death of a child. Table 1 displays the frequencies of the sociodemographic covariates of mothers in each group; sociodemographic characteristics were different between the 2 groups of mothers.
Characteristics of Mothers Who Have Lost a Child
The health variables included in the high-dimensional propensity scores differed as they were selected based on correlations to the exposure and the outcome; this resulted in mothers receiving different weights for each outcome. For each outcome, mothers with extreme weights were excluded; therefore, each outcome had a slightly different sample size. The resulting trimmed samples did not differ significantly on observed sociodemographic and health covariates (see Appendix B for the weighted and unweighted standardized differences of the top covariates in each model). Applying the weights obtained from the IPTWs meant that, based on their observed characteristics, these 2 groups of mothers were equally likely to experience either type of loss.
Mothers whose children were taken into care have much higher rates of mental illness diagnosis and mental illness treatment use than mothers whose children were not taken (see Appendix D), and mothers who experienced the death of a child (Table 2). Compared with mothers whose children died, there were 25 additional depression diagnoses, 36 additional anxiety diagnoses, 24 additional substance use diagnoses, 83 additional physician visits for mental illness, and 405 additional psychotropic prescriptions per 100-person years among mothers having children taken into care.
IPTW-Adjusted Rates and Relative Rates of Outcomes among Mothers Who Have Lost a Child.
aAnalysed using a γ sensitivity test
Table 2 shows IPTW-adjusted rates and IPTW-adjusted relative rates (ARRs) for each of the outcomes for both groups of mothers. Mothers with a child taken into care had significantly greater ARRs (at P < 0.001) of depression, anxiety, and substance use diagnoses, as well physician visits for mental illness and psychotropic prescriptions compared with mothers who experienced the death of a child. The biggest differences were seen for substance use (ARR = 8.54) and number of psychotropic prescriptions (ARR = 4.95).
The associations of type of loss with all significant outcomes were robust to unmeasured confounding based on γ sensitivity test values greater than 90 (Table 2). After adjusting for the variables included in the high-dimensional propensity score, there would need to be an unmeasured confounder that both perfectly predicted the type of loss (death or custody loss) and accounted for more than 90 percent of the relationship between type of loss and each outcome. The likelihood of such a confounder existing, after adjusting for variables included in the high dimensional propensity score, is very small.
Discussion
The outcomes of mothers who lost custody of a child due to involvement with child protection services have not previously been examined at a population-level, and have never been compared with outcomes of mothers who suffered the death of a child. When comparing outcomes for mothers experiencing these 2 types of loss, we reduced differences in baseline characteristics using inverse probability of treatment weights. Mothers whose children were taken into care were shown to have significantly more mental illness diagnoses and greater mental health treatment use than mothers experiencing the death of a child.
Losing custody of a child was associated with worse mental health outcomes for the biological mother than was the death of a child. This could be due to several factors. Both groups of mothers may experience a spiralling decline after the loss of their child that can result in worse mental health. For instance, experiencing the death of a child can result in loss of income or marital breakdown, and mothers who have a child taken into care are more likely to have subsequent children taken into care. 24,25 These additional outcomes could lead to worse outcomes for mothers whose children were taken into care. Differing levels of social support and public acknowledgement of these 2 types of loss may be contributing to these differences in outcomes. Mothers who experience the death of a child are able to publicly mourn this event and are likely to receive a wide range of social support. 26 Mothers’ grief on losing custody of their child is considered disenfranchised as it is not acknowledged, publicly mourned, or socially supported. 27 Individuals repressing their grief—such as those whose grief is disenfranchised—are more likely to express suicidal ideation, loneliness, insomnia, depression, anxiety, distress, somatic symptoms, social dysfunction, impaired memory function, nutritional problems, work and relational difficulties, and difficulties concentrating. 28,29 Finally, mothers who lost a child to death were generally older, lived in neighbourhoods of higher socioeconomic status, and were less likely to have received welfare before the loss of their child (see Table 1); these mothers may be better resourced to access support outside of the public health system following their loss. 30,31
The population-based repository at the Manitoba Centre for Health Policy has some significant strengths, such as a large sample size, minimal attrition, and numerous predictors over many years. The use of linkable administrative data also minimised the risk of surveillance bias, as the data were collected independently of the research hypothesis. The modelling used to create the IPTWs generated excellent discrimination between outcomes. The study limitations concern the potential confounders and the measurement of variables. Mental illness before and after the loss of a child were measured using claims data; these data may not be adequately capturing mental illness, as we are only capturing those who seek treatment and may be missing undiagnosed mental illnesses. 32 However, over 98% of women in this sample visited a primary care physician in the follow-up period, increasing the likelihood of a diagnosis of mental illness. Although unobserved confounding is a threat to all observational studies, the use of IPTWs minimizes this bias. A possibly important confounder not included in the primary analysis is indigenous status; access to this identifier requires permissions from federal agencies, is not guaranteed, and is likely to take 1 to 2 years to obtain. To examine the possible impact of this confounder on our results, a discordant sibling analysis was performed (see Appendix C). When comparing the mental health outcomes of sibling mothers—one who had a child taken into care and the other who experienced the death of a child (controlling for many baseline covariates and stable family characteristics)—we saw that mothers who lose a child into care still had significantly higher rates of substance use diagnoses and psychotropic prescriptions. For anxiety diagnoses and hospitalizations for mental illness, the estimates were like those seen in the original analysis but with larger confidence intervals, making the results non-significant. This could be due in part to the much smaller sample size of the cohort. The results depression diagnoses and physician visits for mental illness were no longer significant, with estimates very different to those seen in the original analysis. Other unmeasured confounders that could affect our conclusions include stressful events in the mother’s life, such as divorce/separation, intimate partner violence, and financial instability. Finally, these findings need to be replicated in other settings to ensure generalizability.
Conclusion
The outcomes seen in mothers who lost custody of a child have been shown to be worse than those found among mothers suffering the death of a child. This is likely in part due to the differing levels of support and acknowledgement available to these 2 groups of mothers. While the death of a child may be unavoidable, having a child taken into care often is. Recent studies have found better outcomes to be achieved by strengthening resources and capabilities of parents rather than focusing solely on the child. 33 –35 Supporting mothers at risk of having a child taken into care would result in better outcomes for her child(ren), and modify the health and social outcomes associated with having a child taken into care. Where children do need to be taken into the care of child protection services, the grief their mothers experience needs to be acknowledged, and more supportive services should be provided. Mothers whose children are taken into care face significant issues before their children are removed; the stress of losing custody can add to these challenges. Providing adequate support for mothers to address mental illness can prevent these additional challenges from becoming another barrier to being reunited with their children. In situations where mothers are not reunified with their children, receiving support to stabilize mental illness could benefit the maternal–child relationship in adulthood.
Supplemental Material
Supplemental Material, Sept_13.17_-_CJP_Maternal_Loss_Appendix - Maternal Mental Health after Custody Loss and Death of a Child: A Retrospective Cohort Study Using Linkable Administrative Data
Supplemental Material, Sept_13.17_-_CJP_Maternal_Loss_Appendix for Maternal Mental Health after Custody Loss and Death of a Child: A Retrospective Cohort Study Using Linkable Administrative Data by Elizabeth Wall-Wieler, Leslie L. Roos, James Bolton, Marni Brownell, Nathan Nickel, and Dan Chateau in The Canadian Journal of Psychiatry
Footnotes
Acknowledgement
Data used in this study are from the Population Research Data Repository housed at the Manitoba Centre for Health Policy, University of Manitoba and were derived from data provided by Manitoba Health, Seniors and Active Living, Manitoba Families, and Vital Statistics under project #2016/2017-09. The results and conclusions are those of the authors and no official endorsement by the Manitoba Centre for Health Policy, Manitoba Health, Seniors and Active Living or other data providers is intended or should be inferred. All data management, programming and analyses were performed using SAS® version 9.4.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Preparation of this manuscript was supported by a Social Sciences and Humanities Research Council of Canada Joseph-Armand Bombardier Canada Doctoral Scholarship, a Graduate Enhancement of Tri-Council Stipend, and a Women’s Health Research Foundation of Canada Full Time Scholarship.
Supplemental Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.