
Abstract
Objective:
Child abuse is associated with poor mental health outcomes in adulthood. However, little is known about how a history of child abuse may be related to perceived need for care (PNC) and mental health service use (MHSU) among Canadian military personnel. The objectives of this study were to determine 1) the relationship between child abuse history and PNC and 2) the relationship between child abuse history and MHSU in the Canadian military.
Method:
Data were drawn from the 2013 Canadian Forces Mental Health Survey (n = 6692 Regular Force personnel between the ages of 18 and 60 years). Logistic regression was used to examine the relationships between individual child abuse types and PNC and MHSU while adjusting for sociodemographic variables, the presence of mental disorders, deployment-related variables, and other types of child abuse. Population attributable fractions (PAFs) were calculated to estimate the proportion of PNC and MHSU that may be attributable to child abuse.
Results:
Each individual child abuse type was associated with increased odds of PNC and MHSU after adjusting for all covariates (adjusted odds ratio ranging from 1.26 to 1.80). PAFs showed that if any child abuse did not occur, PNC and MHSU among Regular Force personnel may be reduced by approximately 14.3% and 11.3%, respectively.
Conclusions:
This study highlights that preenlistment factors, such as a history of child abuse, have an independent association with PNC and MHSU and hence need to be considered when assessing the mental health service needs of the Canadian Regular Force personnel.
Child abuse is associated with a significant burden of suffering, including increased risk of mental health problems and suicidal ideation and attempts. 1 –7 Recent estimates from a representative Canadian population indicate that 47.7% of Regular Force personnel experienced physical abuse, sexual abuse, and/or exposure to intimate partner violence (IPV) before the age of 16. 8 This estimate is higher than the most recent estimates of the Canadian general population, which indicates that 33.1% experienced physical abuse, sexual abuse, and/or exposure to IPV. 1 While the reason for this difference cannot be determined from the available data, it is possible that those entering the military have a higher prevalence of child abuse because they are trying to escape harmful home environments 9 or are attracted to the career and educational opportunities that may improve their life circumstances.
In military populations, deployment-related trauma is an important factor associated with mental disorders, suicidal ideation, perceived need for care (PNC), and mental health service use (MHSU). 10 –12 However, recent findings showed that the association between child abuse and suicide in the military population was often stronger than the association between deployment-related traumas and suicidal outcomes. 8 Additionally, other studies have shown that a minority of mental health problems are directly attributable to factors associated with deployment-related trauma. 10,13 It is important to acknowledge preenlistment traumas, such as child abuse, as factors associated with mental health problems, PNC, and MHSU in the military population. This is especially important considering the greater prevalence of child abuse in the military population compared to the general population. 8
Determining the accurate mental health service needs in military samples can be difficult due to the multitude of factors that drive MHSU aside from being diagnosed with a mental disorder. 14 –16 Previous studies have shown that PNC is a strong predictor of MHSU, 15 and while mental disorders strongly predict PNC and MHSU, the presence of a mental disorder alone is not the only predictor of PNC or MHSU. 17 –20 Despite the availability of mental health services to the military population, the literature has identified that many who are diagnosed with a mental disorder do not receive treatment. 11,12,21 This may be due to numerous barriers to care, including stigma associated with seeking care or negative attitudes towards receiving treatment, among others. 12,15,22 Furthermore, the presence of a mental disorder does not always precede PNC, and many individuals with subclinical mental health problems may perceive a need for care. 11,17,20,23 A theoretical perspective of help seeking created by Goldberg and Huxley 24 illustrates how the decision to seek help occurs in a series of stages, including 1) experiencing symptoms, 2) evaluating severity and consequences of the symptoms, 3) assessing whether treatment is required, 4) assessing the feasibility of and options for treatment, and 5) deciding to seek treatment. It is important to consider that the need for mental health services may occur outside of mental health diagnoses and, therefore, the presence of a mental disorder may not accurately depict the true mental health service needs of the population. 25 Other factors, such as preenlistment trauma, may play a role in increasing PNC and MHSU in the military population.
In a general population sample, different types of childhood adversity, including parental separation, emotional neglect, physical abuse, sexual abuse, contact with child protection services, and parental psychopathology, were independently linked to increased PNC and MHSU. 26 To date, no studies using military samples have considered the relationship between child abuse history and PNC and MHSU. To extend this area of inquiry, we analysed data from the 2013 Canadian Forces Mental Health Survey. The objectives of this study were to 1) determine the relationship between child abuse history and PNC and MHSU among the Regular Force personnel in Canada; 2) determine whether the associations between child abuse history and PNC and MHSU remain after adjusting for the effects of sociodemographic variables, mental disorders, deployment-related variables, and other types of child abuse; and 3) calculate the population attributable fractions (PAFs) for PNC and MHSU attributable to child abuse experiences.
Methods
Data and Sample
Data were drawn from the 2013 Canadian Forces Mental Health Survey (CFMHS; N = 8161, response rate = 79.8%) collected by Statistics Canada. The sample was limited to a representative sample of Regular Force personnel (n = 6692) and restricted to respondents aged 18 years and older. The upper age bound of survey participants was 60 years. Participation in the survey was voluntary, and confidentiality and anonymity were maintained under the Statistics Act. 27 Respondents provided informed consent prior to participating.
Primary Measurements
Child abuse
Three types of child abuse were assessed in the CFMHS 2013, including physical abuse, exposure to IPV, and sexual abuse. Physical abuse and exposure to IPV were measured using items from the Childhood Experiences of Violence Questionnaire (CEVQ), which has been shown to be a valid and reliable instrument used in previous research on child abuse. 28 Respondents aged 18 years or older were asked questions about abuse occurring before the age of 16 years. Response options were classified using threshold criteria according to the CEVQ. Physical abuse was present if the respondent was 1) slapped on the face, head, or ears or hit or spanked with something hard 3 times or more; 2) pushed, grabbed, shoved, or having something thrown at the respondent to hurt them 3 times or more; or 3) kicked, bit, punched, choked, burned, or physically attacked 1 time or more. Exposure to IPV was present if the respondent saw or heard parents, stepparents, or guardians hitting each other or another adult in the home 3 times or more. Sexual abuse was present if either of the following occurred 1 time or more: 1) attempted or being forced into unwanted sexual activity by being threatened, held down, or hurt in some way and/or 2) sexually touched, meaning unwanted touching or grabbing, kissing, or fondling against their will. An additional variable was computed from combing all 3 types of abuse together to create a measure of any child abuse. Finally, the number of types of child abuse a respondent experienced was categorised into none, 1 type, or 2 or more types.
Perceived need
Perceived need for care was assessed with the Perceived Need for Care Questionnaire (PNCQ), developed for the Australia National Survey of Mental Health and Well-being. 11,29 Respondents were asked about 4 different kinds of help (i.e., information, medication, counselling, and/or other) they received or thought they needed for problems with emotions, mental health, or use of alcohol or drugs in the past 12 months. A dichotomous variable was created to classify respondents who thought they needed help and either received help or did not into the yes PNC category and respondents who did not receive help and did not think they needed it into the no PNC category.
Mental health service use
Respondents were asked if they sought professional help about a problem with their emotions, mental health, or use of alcohol or drugs from a psychiatrist, psychologist, family doctor or general practitioner, nurse, or social worker, counsellor, or psychotherapist in the past 12 months. Mental health service use was dichotomised into using 1 or more types of services and using no services in the past 12 months.
Sociodemographic variables
Seven sociodemographic variables were included in this study. Age was included as a continuous variable measured in years. Sex was measured as male or female. Similar to another paper using these data, household income was assessed in the following categories: ≤$29,999, $30,000 to $49,999, $50,000 to $79,999, and ≥$80,000. 8 Marital status was measured in 3 categories: married or common law, separated/widowed/divorced, and never married. Visible minority status was measured as yes or no. Education was measured as high school or less, some postsecondary education, trade or college certificate/ diploma, and university degree. Military rank included junior noncommissioned member, senior noncommissioned member, and officer.
Mental disorders
Six lifetime mental disorders were measured using the World Health Organization Composite International Diagnostic Interview (CIDI) criteria, including depression, general anxiety disorder, alcohol abuse or dependence, panic attacks, panic disorder, and posttraumatic stress disorder. We used lifetime rather than past-year mental disorders because there is a high percentage of people with a history of mental disorders who do not meet criteria for a past-year mental disorder but still have PNC or MHSU. 25 Obsessive-compulsive disorder, bipolar disorder, and phobia were individually measured through self-report by asking participants whether they had been diagnosed with a health condition by a health professional that was expected to last or had already lasted 6 months or more. Two dichotomous yes or no variables were computed: one for the CIDI diagnosed mental disorders and one for self-reported mental disorders that classified respondents as having 1 or more mental disorders.
Deployment-related variables
Eight deployment-related traumatic events (DRTEs) were assessed, including the following: 1) known someone who was seriously injured or killed; 2) found yourself in a life-threatening situation where you were unable to respond because of rules of engagement; 3) ever been injured; 4) ever seen ill or injured women or children who you were unable to help; 5) ever received incoming artillery, rocket, or mortar fire; 6) ever felt responsible for the death of Canadian or ally personnel; 7) ever had a close call (e.g., shot or hit but protective gear saved you); and 8) ever had difficulties distinguishing combatants from noncombatants. A dichotomous variable was created that classified respondents into 1) those who experienced 1 or more DRTEs and 2) those with none or were never deployed. Deployment in support of the mission in Afghanistan and any other international deployment were combined to classify respondents as having a past deployment or none.
Statistical Analysis
Data were analysed using Stata for Windows, release 13 (StataCorp LP, College Station, TX, USA). Bootstrapping was used as a variance estimation technique to account for the complex survey design; survey weights were applied to ensure the data were representative of the Canadian Regular Forces personnel. First, prevalence rates were computed for all variables included in the study. Second, logistic regression models were computed to determine the strength of the relationship between different types of child abuse and PNC and MHSU in 4 nested models. The first model adjusted for sociodemographic variables, including age, sex, education, visible minority status, income, marital status, and military rank (adjusted odds ratio [AOR]–1); the second model adjusted for sociodemographic variables as well as any CIDI indicated mental disorders and any self-reported mental condition (AOR-2); the third model adjusted for all the previously mentioned variables as well as deployment-related variables (AOR-3); and the fourth model adjusted for all other variables as well as other types of child abuse (AOR-4). Third, PAFs and 95% confidence intervals (CIs) were calculated using the Stata punaf module that has been described in detail elsewhere. 30 The PAFs estimate the proportion of PNC and MHSU that may be reduced if child abuse experiences were eliminated. Missing data were excluded using complete case analysis for regression models.
Results
The prevalence of sociodemographic, mental health, deployment-related, and child abuse variables, as well as the prevalence of PNC and MHSU among the Regular Force personnel, is presented the Table 1. The associations between child abuse and PNC among Regular Force personnel are presented in Table 2. The prevalence of PNC among those who experienced physical abuse, sexual abuse, exposure to IPV, or any child abuse was 37.0%, 52.3%, 45.8%, and 37.1%, respectively. Among those who did not experience any child abuse, the prevalence of PNC was 23.0%. Experiencing physical abuse, sexual abuse, exposure to IPV, or any child abuse was associated with increased odds of PNC in the past 12 months, even after adjusting for sociodemographic variables, mental disorders, deployment-related variables, and other types of abuse (AOR-4 range from 1.40 [95% CI, 1.2-1.7] to 1.80 [95% CI, 1.4-2.3]). A dose-response trend was noted with increasing number of child abuse types corresponding to increased odds of PNC in all adjusted models (AOR-3: 1 type of child abuse = 1.39 [95% CI, 1.2-1.6]; 2 or more types = 2.36 [95% CI, 2.0-2.8]). The PAFs estimate that 9.9%, 3.1%, 2.4%, and 14.3% of PNC could be reduced if physical abuse, sexual abuse, and exposure to IPV and all types of child abuse, respectively, were eliminated. If experiencing multiple abuse types were eliminated, it is estimated that PNC could be reduced by 7.3%, while eliminating the experience of all single types of abuse could reduce PNC by an estimated 7.3% as well.
Prevalence of Sociodemographic Variables among the Canadian Regular Armed Forces Ages 18 to 60 Years.
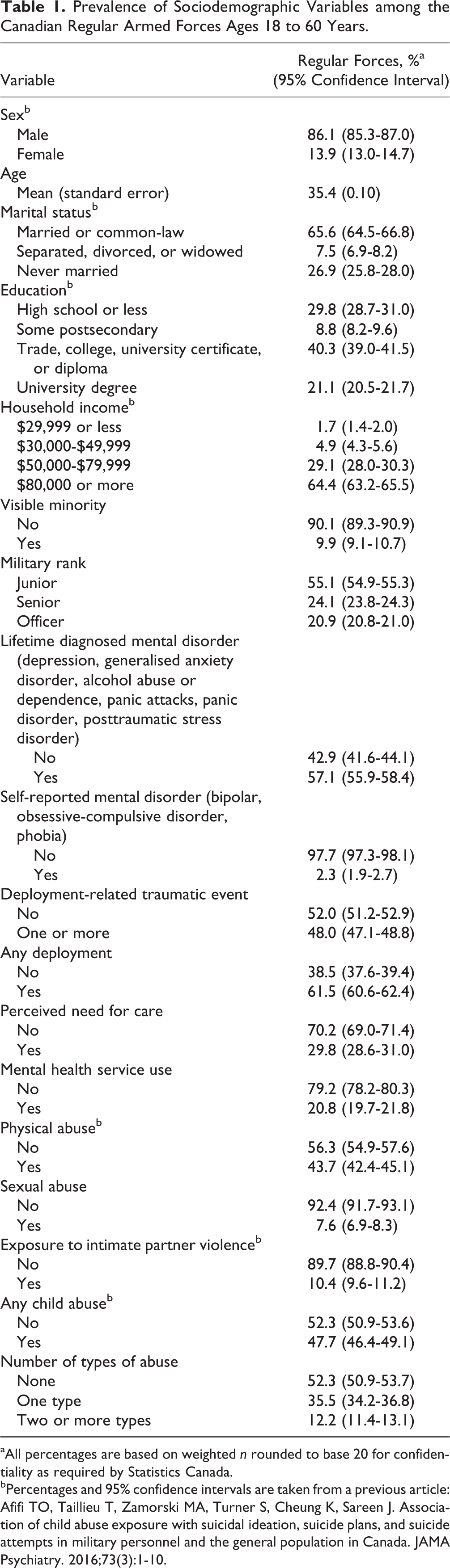
aAll percentages are based on weighted n rounded to base 20 for confidentiality as required by Statistics Canada.
bPercentages and 95% confidence intervals are taken from a previous article: Afifi TO, Taillieu T, Zamorski MA, Turner S, Cheung K, Sareen J. Association of child abuse exposure with suicidal ideation, suicide plans, and suicide attempts in military personnel and the general population in Canada. JAMA Psychiatry. 2016;73(3):1-10.
Associations between Past 12-Month Perceived Need for Care and Child Abuse among Regular Force Personnel.
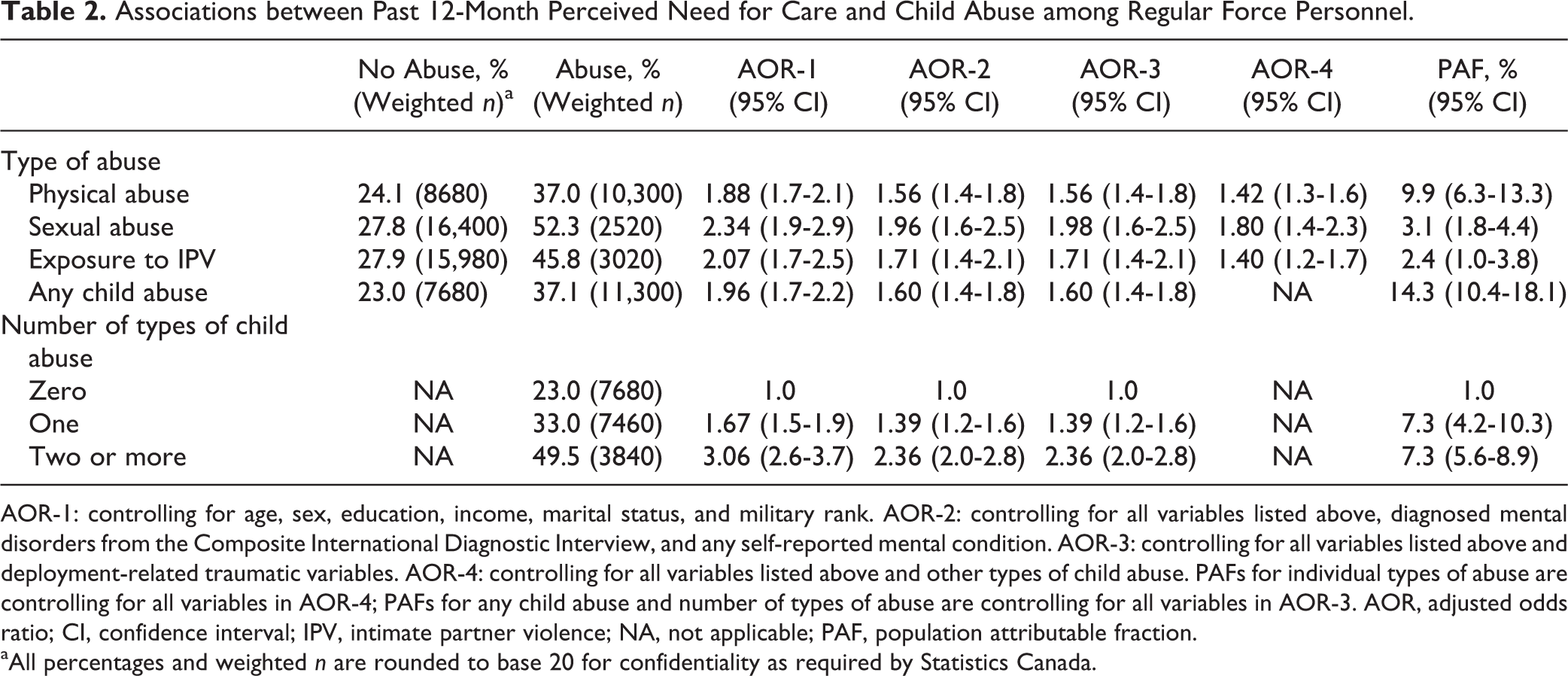
AOR-1: controlling for age, sex, education, income, marital status, and military rank. AOR-2: controlling for all variables listed above, diagnosed mental disorders from the Composite International Diagnostic Interview, and any self-reported mental condition. AOR-3: controlling for all variables listed above and deployment-related traumatic variables. AOR-4: controlling for all variables listed above and other types of child abuse. PAFs for individual types of abuse are controlling for all variables in AOR-4; PAFs for any child abuse and number of types of abuse are controlling for all variables in AOR-3. AOR, adjusted odds ratio; CI, confidence interval; IPV, intimate partner violence; NA, not applicable; PAF, population attributable fraction.
aAll percentages and weighted n are rounded to base 20 for confidentiality as required by Statistics Canada.
The associations between child abuse and MHSU among Regular Force personnel are presented in Table 3. The prevalence of MHSU among those who experienced physical abuse, sexual abuse, exposure to IPV, or any child abuse was 25.5%, 39.1%, 31.0%, and 25.6%, respectively. The prevalence of MHSU among those who did not experience any child abuse was 16.3%. Physical abuse (AOR-4, 1.26; 95% CI, 1.1-1.4) and sexual abuse (AOR-4, 1.63; 95% CI 1.3-2.1) were associated with increased odds of MHSU in all models. Exposure to IPV was significant in AOR-1 to AOR-3 but was no longer significant in the most adjusted model (AOR-4, 1.20; 95% CI, 0.96-1.5). Increasing number of types of child abuse was associated with increased odds of MHSU even in the most adjusted model (AOR-3: 1 type of child abuse = 1.24 [95% CI, 1.1-1.4]; 2 or more types = 1.77 [95% CI, 1.4-2.2]). The PAFs estimate that 7.6%, 3.5%, and 11.3% of MHSU could be reduced if physical abuse, sexual abuse, and any type of child abuse, respectively, were eliminated. If experiencing multiple abuse types were eliminated, it is estimated that MHSU could be reduced by 6.1%, while eliminating the experience of all single types of abuse could reduce MHSU by an estimated 5.4%.
Associations between Past 12-Month Mental Health Service Use and Child Abuse among Regular Force Personnel.
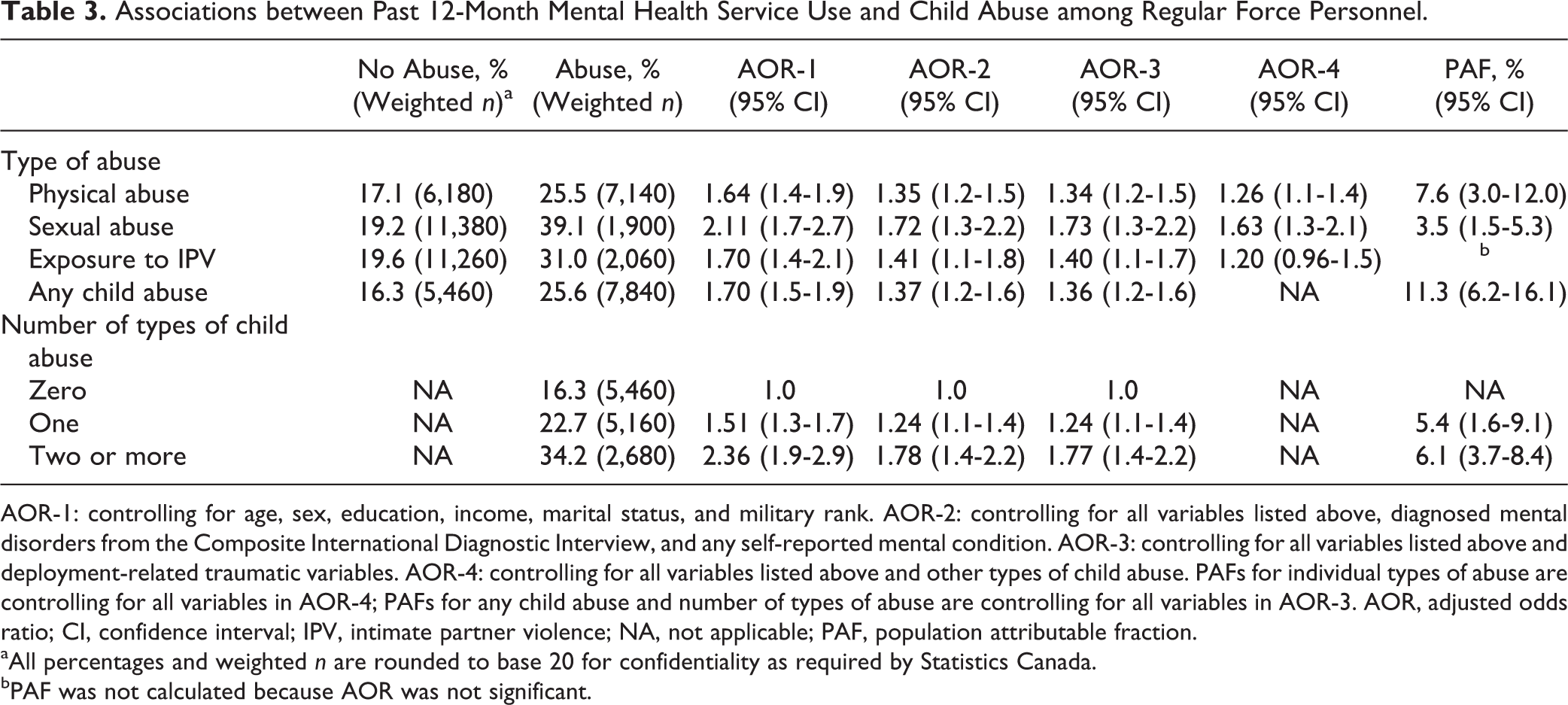
AOR-1: controlling for age, sex, education, income, marital status, and military rank. AOR-2: controlling for all variables listed above, diagnosed mental disorders from the Composite International Diagnostic Interview, and any self-reported mental condition. AOR-3: controlling for all variables listed above and deployment-related traumatic variables. AOR-4: controlling for all variables listed above and other types of child abuse. PAFs for individual types of abuse are controlling for all variables in AOR-4; PAFs for any child abuse and number of types of abuse are controlling for all variables in AOR-3. AOR, adjusted odds ratio; CI, confidence interval; IPV, intimate partner violence; NA, not applicable; PAF, population attributable fraction.
aAll percentages and weighted n are rounded to base 20 for confidentiality as required by Statistics Canada.
bPAF was not calculated because AOR was not significant.
Discussion
This study adds to the literature in 3 important ways. First, physical abuse, sexual abuse, and exposure to IPV are associated with both PNC and MHSU in Regular Force personnel, independent of mental health conditions and deployment-related variables. Second, a dose-response trend exists with increasing number of types of child abuse experienced relating to increased PNC and MHSU. Third, PAFs showed that child abuse is an important, independent contributor to PNC and MHSU. After controlling for sociodemographic variables, mental disorders, and deployment-related variables, if any experience of child abuse did not occur, PNC and MHSU could be reduced by 14.3% and 11.3%, respectively.
The results of this study are consistent with the findings from a Canadian general population sample showing that childhood adversity is independently related to both PNC and MHSU. 26 To our knowledge, the relationship between child abuse and PNC and MHSU has not been similarly studied in comparable international populations, precluding such comparisons with our findings. Results from recent comparison studies show that military and general population samples differ in important ways. For example, there are higher rates of child abuse and PNC in the military population, the system for seeking mental health treatment is different between the two populations, and there are barriers to seeking care such as stigma and negative perceptions of mental health treatment that may affect PNC and MHSU differently for military compared to general population samples. 8,22,31 Over the past decade, significant investments have been made to the Canadian military’s mental health system that attempt to address barriers to care, facilitate access, and increase the capacity for care provision. Details about these changes can be found elsewhere. 32,33 Unfortunately, comparable investments have not been implemented in the Canadian public mental health care system, and at a minimum, these potentially influenced mental health awareness, PNC, and MHSU. Therefore, these results add to the literature by examining and verifying the relationship between child abuse and PNC and MHSU using a recent Canadian military sample.
Both the presence of a mental health problem and exposure to deployment-related variables are factors that may increase the PNC and MHSU in the military population. 10 –12 However, this study showed that even after taking these variables into account, experiencing child abuse was still significantly related to both PNC and MHSU. More specifically, adding DRTEs and any deployment as control variables in AOR-3 did not change the magnitude of the odds ratios for both PNC and MHSU, showing that broad-level deployment-related variables do not account for much of the measured association between child abuse and PNC or MHSU. Other researchers have noted a strong association between witnessing atrocities during deployment and both mental disorders and PNC, 11 but this study did not adjust for experiences of child abuse. It is possible that these associations would have been largely attenuated if child abuse was adjusted for in the analysis. Child abuse may increase subdiagnostic psychiatric symptoms related to mental disorders, therefore causing an increased need for mental health care even in the absence of a mental disorder diagnosis. These findings are also important in clinical settings so that preenlistment trauma, including child abuse, is assessed and included in postdeployment screening and treatment programs. It is important to note that even among those who do not have a history of child abuse, the prevalence of PNC and MHSU ranges from 16.3% to 27.9%, showing that there are important mental health treatment needs among Regular Force personnel who did not experience child abuse as well.
The dose-response trend of increasing child abuse types relating to increased odds of PNC and MHSU is consistent with other literature that has looked at the relationship between experiencing multiple types of abuse and long-term health outcomes in general population samples. 1 It is important to consider co-occurring types of child abuse because individuals who report experiences of child abuse commonly experience more than 1 type of abuse, and the needs of those who experience more than 1 type of abuse may be higher compared to those who experience 1 type. 34,35
To our knowledge, this is also the first study to calculate PAF estimates for the association between child abuse types and PNC and MHSU. A previous study using a general population sample used PAFs for estimating the reduction in mental disorders, suicide ideation, and suicide attempts associated with adverse childhood experiences (PAFs ranged from 16% to 50% among women and 20% to 33% among men for experiencing any adverse childhood event). 36 Other studies using military samples have used PAFs for estimating the reduction in mental disorders associated with combat exposure and peacekeeping operations. 10,37 PAFs are useful because they provide an estimate of the proportion of the outcome that may be reduced if the exposure were eliminated; however, PAF estimates are influenced by the prevalence of the exposure in the study population. As a consequence, we note that physical abuse has the smallest adjusted odds ratios for PNC and MHSU, yet it has the largest PAF. This is a result of the higher proportion of reported physical abuse compared to sexual abuse or exposure to IPV in our study population. Similarly, this pattern is also true for the number of types of child abuse. Experiencing 2 or more types of abuse results in a higher odds of PNC and MHSU compared to experiencing 1 type of abuse, yet the PAFs for both were almost identical. This was a result of a much smaller proportion of the study population with 2 or more types of abuse compared to 1 type.
PAF estimates also assume that the relationship between the exposure and outcome variables is largely causal and, hence, rely on the removal of confounding between exposure and outcome. The current study calculated PAFs while controlling for several sociodemographic, deployment-related, and mental health variables, thus attempting to isolate the relationship between child abuse and PNC and MHSU. It is likely that mental disorders are situated on the causal pathway between child abuse exposure and PNC and MHSU. Therefore, these results should be interpreted as estimates with the understanding that adjusting for mental disorders will make the AOR and PAF estimates more conservative.
Strengths of this study include 1) the use of a large, representative military data set; 2) the use of the PNCQ, a highly validated measure of PNC, to measure PNC of the respondent; and 3) this is the first study to consider the relationship between child abuse and PNC and MHSU in the military population, filling an important gap in the literature. However, the results of this study should be taken in the context of several limitations. First, PAFs assume a causal relationship between exposure and outcome, and while all efforts were taken to reduce potential confounding between variables, it is likely that unmeasured confounding still exists. As well, it should be noted that PAFs are often computed using incidence data. We have used prevalence data to compute PAFs in this analysis but have done so using an appropriate prevalence formula to estimate the PAFs. Second, due to the cross-sectional nature of the survey, temporality between PNC, MHSU, deployment-related variables, and mental health conditions cannot be determined. Third, not all mental disorders were assessed in the CFMHS; therefore, it is possible that a respondent could be diagnosed with a disorder that was not assessed and hence not captured in the data set. Fourth, the combined prevalence of the 3 self-report mental health conditions assessed in this survey is lower than what has been found in a US military sample using DSM-IV criteria for mental disorders. 38 The self-reported mental disorders in this analysis may be underreported because to answer yes, the respondent needs to have sought help and received a diagnosis. It is possible that some people may have symptoms of the disorders and meet criteria in a module-based assessment but never receive an official diagnosis. Fifth, only 8 DRTEs were assessed, which may not capture all traumatic experiences endured during deployment. Sixth, only 3 types of child abuse were measured, and the data were collected retrospectively. Additionally, there was no measure of childhood neglect or emotional maltreatment.
Conclusion
The findings of the current study underscore the importance of the individual association between child abuse and PNC and MHSU in the military population. It is critical to recognise the contribution of preenlistment experiences to military mental health needs and within the context of providing adequate mental health services. Education programs that target enhancing mental health literacy and resilience in military personnel as well as postdeployment mental health screening efforts could possibly be augmented to include awareness of the mental health need associated with child abuse, thus facilitating access to MHSU.
Footnotes
Acknowledgements
We thank Bryan Garber for his contribution to editing the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Preparation of this article was supported by a CIHR New Investigator Award (Afifi), Research Manitoba Establishment Award (Afifi), CIHR Foundation Grant 333298 (Afifi), and CIHR Foundation Grant 333252 (Sareen). Funding for this article was supported by a research contract from the Government of Canada and by salary support from the Department of National Defense