
Abstract
Objective:
Reports show disparities in the health care of persons with severe mental illness (SMI), including in countries with universal health insurance. However, the moderating effect on disparities of specific mental health legislation is yet to be studied. The study aimed to investigate equality of health care for people with SMI in a country with a national health insurance and a comprehensive rehabilitation law for persons with mental disabilities.
Method:
A case-control epidemiological study compared health services (laboratory tests, visits to specialists, and medications) provided to users with and without a history of schizophrenia and bipolar disorder (N = 52,131) and with regard to a subgroup of users with diabetes (n = 16,280). In addition, we examined the mortality rates of the study population.
Results:
While service users with schizophrenia were somewhat less likely to meet the same indexes of care as controls, those with bipolar disorder did not differ from their counterparts. Yet, mortality risk among service users with schizophrenia and bipolar disorder was 2.4 and 1.7 times higher, respectively. Rates of services to persons with SMI and comorbid diabetes did not differ from their counterparts.
Conclusions:
In Israel, a country with a national health insurance and a rehabilitation law for persons with mental disabilities, service users with bipolar disorder receive equitable levels of general health care. For users with schizophrenia, the disparities exist in some of the health care measures but to a smaller extent than in other countries with universal health insurance. In contrast, mortality rates are elevated in persons with SMI.
Persons with severe mental illness (SMI) are at increased risk for physical comorbidity and premature death. 1 –6 Inequality in health care for people with SMI seems to play a major role in what has been termed “the scandal of premature mortality.” 7 Findings on health disparities were shown in the United States, including in population groups protected by special insurance systems (e.g., Army veterans), 8 –11 as well as in countries with national health insurance, where care is not dependent on out-of-pocket expenditure (e.g., Australia, 12 Canada, 13 Denmark, 14 Israel, 15 Sweden, 16 and Taiwan 17 ). These studies frequently focused on persons with SMI and chronic somatic comorbidities. The rationale to study persons with comorbidities (e.g., cardiovascular disease or diabetes) is that they represent subpopulations with increased health care demands and are appropriate to test the equal provision of services by the health systems.
Type 2 diabetes is a particularly important somatic comorbidity frequently used to trace health disparities in the treatment of chronic physical conditions among people with SMI. First, their prevalence rates are elevated, 2- to 3-fold in people with schizophrenia and bipolar disorder. 18,19 There is a considerable literature on the health-related adverse effects of antipsychotic agents, and in particular, atypical antipsychotics appear to induce weight gain and metabolic abnormalities. 20 Second, if the screening rate for diabetes is lower than needed, the omission may lead to prolonged periods of deficient glycemic control. 21 Third, persons with SMI and comorbid diabetes are less likely to receive standard levels of diabetes care. 18,22 It is thus not surprising that among people with diabetes an elevated mortality rate, as high as 150%, was reported in those with schizophrenia and bipolar disorder compared to controls. 23 Thus, we will study if the adherence to the guidelines of diabetes care are met in persons with SMI. 24
Israel, like the above-noted countries, has a national health insurance law (1995) that mandates universal and comprehensive health care. Also, people reaching a threshold of mental disability receive a “basket of services” mandated by the rehabilitation law, including the “appointment of a treatment coordinator who is responsible for implementation and coordination of the provision of all the services for the mentally disabled person.” 25 Positive clinical and psychosocial outcomes were reported. 26 –28 For example, higher probability to stay in the community after discharge and shorter rehospitalisation periods were found among those who received rehabilitation services. 27
Objective
This study examines disparities in health care provided to persons with schizophrenia or bipolar disorder and their respective mortality rates, in a country with national health insurance and a mental disability legislation. Also, health care of persons with schizophrenia or bipolar disorder and comorbid diabetes is examined as a test case of users requiring markedly more services.
Methods
The study was based on a prospective historical design, with data collected 2000 to 2009. Ethical approval was granted by the head management of the health provider, Clalit Health Services (CHS). Participants’ identity was undisclosed to the authors.
Identification of Persons with Severe and Persistent Mental Disorder
Psychiatric care in Israel is freely available by law to all de jure residents. 29 To identify the sample of persons with schizophrenia and bipolar disorder, we used the Psychiatric Case Register (PCR). The PCR is legally mandated to maintain a cumulative record of all psychiatric hospitalisations in mental and general hospitals. 30,31 The PCR provided the subjects’ sociodemographic information and psychiatric diagnoses upon admission and discharge based on the International Classification of Diseases, Tenth Revision (ICD-10 32 ) (prior systems have been updated). Tests of agreement between research and PCR diagnoses were found satisfactory. 33,34 The following inclusion criteria were applied: 1) persons with last discharge diagnosis of schizophrenia (F20-F29) or bipolar disorder (F31), 2) born prior to 1960 (age >40 at the start of the follow-up period), and 3) alive by the year 2000. The reason for the age criterion was to include service users in greater need for health services (e.g., older users).
We identified 28,579 persons diagnosed with schizophrenia and 4145 with bipolar disorder who met the inclusion criteria (N = 32,904). The collected information included year of first and last psychiatric hospitalisation, total number of admissions, and accumulative length of hospital stay (Table 1). The latter was recorded annually (2000-2009) to account for the episodes of hospitalisation when the service user was treated by the mental hospital solely. Severity indicator of the disorder was based on the median number of hospitalisations, calculated separately for persons diagnosed with each disorder: schizophrenia (median, 4) and bipolar (median, 3). Each person was defined as affected by lower (below the median of the respective group) or higher degree of severity (above the median).
Sociodemographic Characteristics of the Sample and Clinical Data of Service Users Diagnosed with Schizophrenia or Bipolar Disorder.
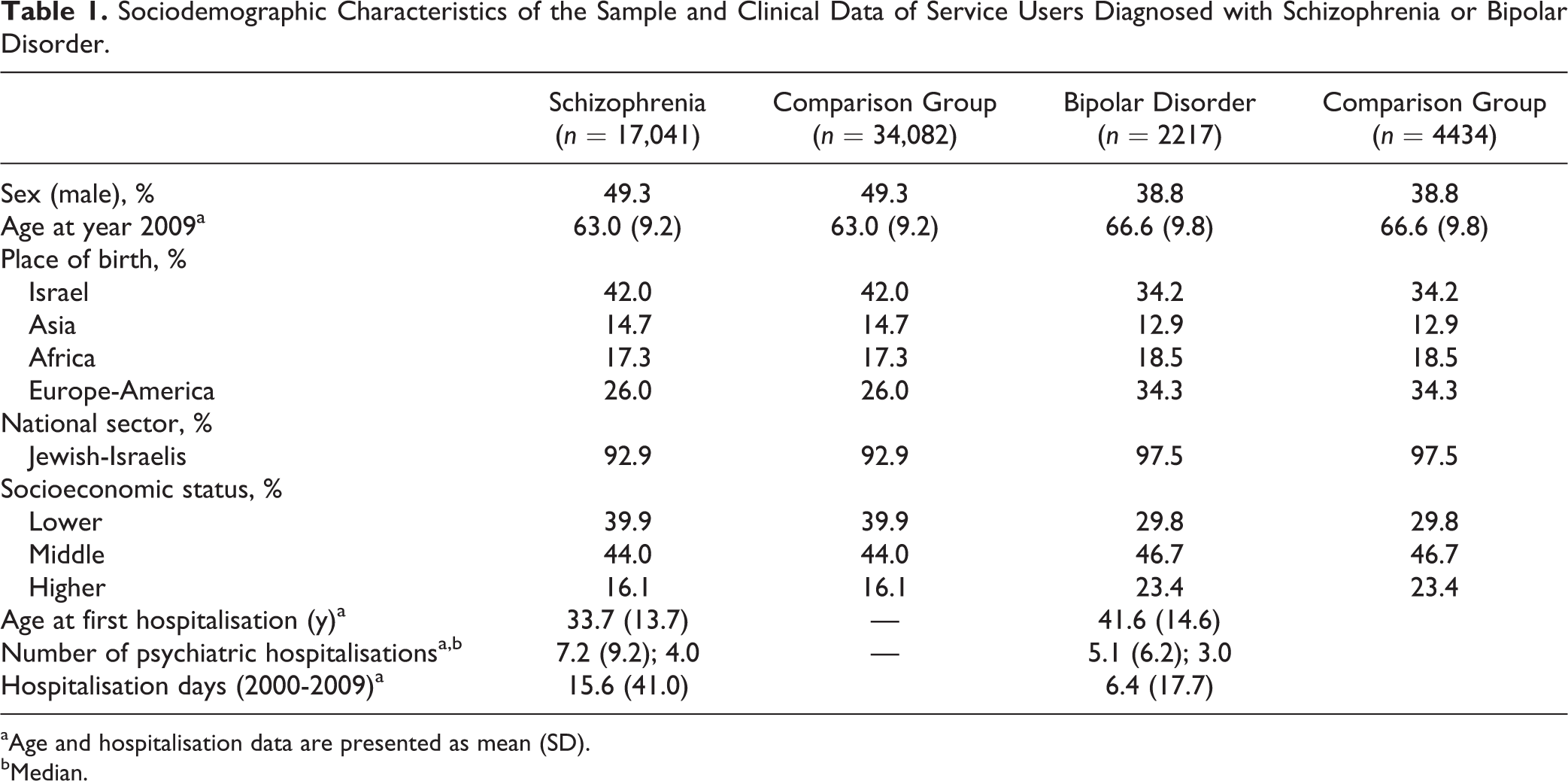
aAge and hospitalisation data are presented as mean (SD).
bMedian.
General Health Services
Data from CHS, with 4.2 million insured persons, were extracted from its electronic database. The sampling frame (N = 1,040,000) was defined according to the second and third inclusion criteria (i.e., age >40 and alive at year 2000). Information was gathered annually from 2000 to 2009, except for some information made available from 2002 onwards when the CHS established a central database.
The following information was collected: Sociodemographic: sex, year and place of birth, national sector (Jewish- and Arab-Israelis), year of death, and socioeconomic status. The latter was based on information gathered by the Central Bureau of Statistics on average income level by region of residence. Each clinic’s geographical location was used as a proxy for income level and applied to rank the socioeconomic status of the user: lower (income deciles 1-3), middle (deciles 4-7), and higher (deciles 8-10). Medical diagnosis: type 2 diabetes mellitus (E11) was recorded.
30
Data were extracted from the service users’ files, including the respective dates of diagnosis. Laboratory tests: the number of annual tests was recorded: blood cholesterol fraction tests (low-density lipoprotein [LDL]) (2002-2009) haemoglobin A1C tests (2002-2009), stress tests (2000-2009), and chest X-rays (2000-2009). Also, the lowest and highest results of estimated LDL cholesterol and haemoglobin A1C tests were recorded annually (2002-2009). Only the highest annual level was used since most service users did not take more than a single annual test, and thus the lowest and highest results were identical. Haemoglobin A1C is measured primarily to ascertain the average plasma glucose concentration over prolonged periods of time and is required in the utilization of second-generation antipsychotic medications because of their associated risk for diabetes. There are a few reasons to assume that haemoglobin A1C and LDL tests would be taken by the service users in our study. First, since the participants in our study were relatively aged, there is firm base to hypothesize that they do undergo physical tests. Second, with the increase of awareness to preventive medicine in the context of metabolic syndrome and diabetes, such tests are part of the Quality Indicators Program, promoted by the Israeli Ministry of Health. While A1C tests are recommended on an annual basis for persons diagnosed with diabetes, no clear recommendation is present with regard to people of the general population who are not diagnosed. Visits to specialists: number of annual visits, excluding psychiatrists (2000-2009). Drug utilization: number of months per year in which insulin and noninsulin antidiabetic medications were dispensed to service users (2000-2009). For each drug category, the mean months of utilization per year were calculated (2000-2009).
Linkage Procedure and Selection of a Matched Control Group
The data extracted from the PCR and CHS databases were merged according to the personal ID. To generate matched control groups, we defined an algorithm based on age (groups of 3 consecutive years), sex, place of origin (Israel, Asia, Africa, Europe-America), socioeconomic status (higher, middle, lower), and national sector (Jewish- and Arab-Israelis). This enabled us to produce matched control pairs (2:1 ratio) for each case and to separate between service users with schizophrenia from those with bipolar disorder, each having a different matched control group. If the service user with SMI had missing information on one of the matching variables, comparison subjects with missing data on that same variable were chosen. Service users were omitted if the mean annual psychiatric hospitalisation was over 270 days. Accordingly, 336 service users with schizophrenia and 6 with bipolar disorder were omitted. The linkage yielded 17,041 service users diagnosed with schizophrenia and 2217 with bipolar disorder in the CHS database. They were matched respectively to 34,082 and 4434 service users with identical sociodemographic characteristics (Table 1).
Data Analysis
The associations between the diagnostic groups and respective counterparts (schizophrenia-comparison, bipolar-comparison) and laboratory tests, chest X-ray, stress test, visits to specialists, and drug utilization were analyzed using analysis of variance (ANOVA) and logistic regression. Outcomes of the logistic regression tests were estimated using odds ratios (ORs) and 95% confidence intervals (95% CIs). Univariate analysis was conducted first for all models to test the association between medical procedures and potential confounders. Adjusted analysis followed to control for confounding variables showing univariate associations at the level of P < 0.1 with the outcome variables. Effects of SMI severity (low/high) were compared within each diagnosis (schizophrenia, bipolar) using ANOVA.
Rates of diabetes were analyzed using logistic regression models. Persons with SMI with first psychiatric hospitalisation record from year 2000 onwards were omitted from the analysis if the diagnosis of diabetes preceded the psychiatric record. The number of follow-up years since diabetes diagnosis (min = 1, max = 10) was accounted in all analyses. Adjusted analysis followed univariate analysis to control for potential cofounders. Mortality rates during the follow-up period (start, January 1, 2000; end, December 31, 2009) were analyzed using Cox proportional hazards models to estimate hazard ratios (HRs) and 95% CI. Analysis was performed using the SPSS 21.0 software (SPSS, Inc., an IBM Company, Chicago, IL).
Results
Service Users Diagnosed with Schizophrenia
Less annual LDL and stress tests, chest X-rays, and visits to specialists were recorded for service users diagnosed with schizophrenia than among counterparts (Table 2). Throughout the study period, 9.5% of the service users with schizophrenia and 7.4% of the comparison group had no LDL test (univariate OR, 0.98 [95% CI, 0.96 to 0.99]; adjusted OR, 0.99 [95% CI, 0.93 to 1.04]). The mean LDL level was slightly lower among service users with schizophrenia (mean ± SD, 126.0 ± 29.7) than in the comparison group (126.6 ± 27.9) (unadjusted F = 5.4, df = 1, 44,163, P = 0.02; adjusted F = 5.0, df = 1, 43,611, P = 0.026). In contrast, haemoglobin A1C test was done more frequently among service users with schizophrenia (Table 2). Throughout the follow-up period, 43.5% of the service users with schizophrenia did at least 1 haemoglobin A1C test compared to 38.9% of the matched control (univariate OR, 1.12 [95% CI, 1.09 to 1.15]; adjusted OR, 0.98 [95% CI, 0.92 to 1.04]). Higher haemoglobin A1C level was recorded in service users with schizophrenia (6.9% ± 1.7%) compared to controls (6.8% ± 1.5%) (unadjusted F = 11.3, df = 1, 19,430, P = 0.001; adjusted F = 16.7, df = 1, 19,199, P < 0.001). According to severity, the mean annual visits to specialists was higher among service users with schizophrenia with lower (2.7 ± 3.4) compared to higher severity (2.4 ± 3.4) (unadjusted F = 47.3, df = 1, 17,039, P < 0.001; adjusted F = 41.5, df = 1, 16,731, P = 0.01).
Annual Rate of Recorded Health Measures among Service Users with Schizophrenia and Matched Controls.
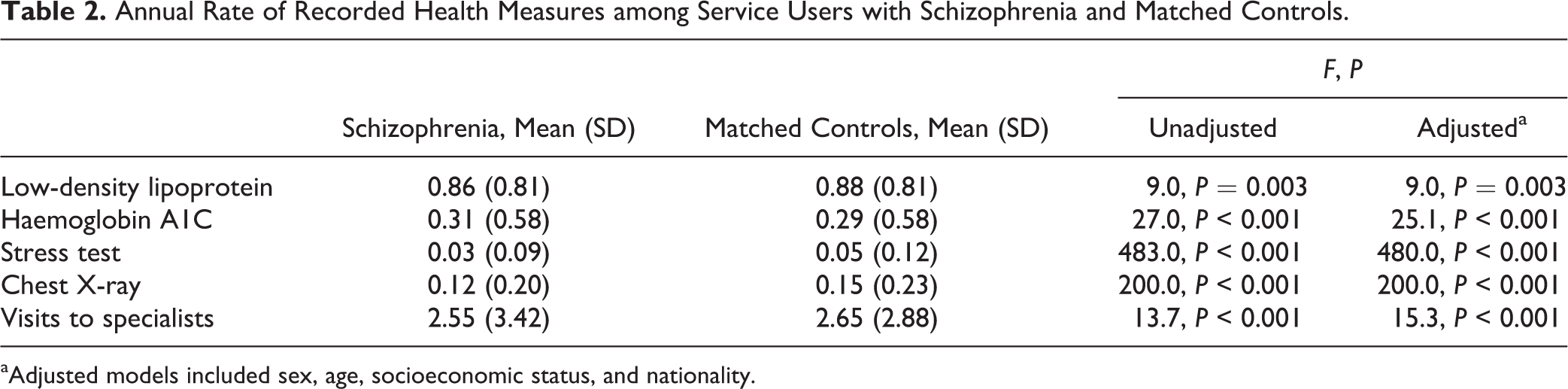
aAdjusted models included sex, age, socioeconomic status, and nationality.
Mortality
During the follow-up period, deaths were recorded in 18.7% of the service users with schizophrenia and in 8.2% among counterparts, a 2.4-fold risk at any fixed point of time (adjusted HR, 2.39; 95% CI, 2.29 to 2.51). The median age of death was lower among service users diagnosed with schizophrenia (67 years) than controls (71 years).
Diabetes
Higher rates of diabetes were found among service users with schizophrenia (n = 5134, 30.6%) compared to controls (n = 9189, 27.0%) (univariate OR, 1.19 [95% CI, 1.14 to 1.24]; adjusted OR, 1.18 [95% CI, 1.13 to 1.23]). The former were diagnosed at an earlier age (59.5 ± 8.8) than controls (61.2 ± 9.1) (unadjusted F = 126, df = 1, 14,321, P < 0.001; adjusted F = 22.3, df = 1, 14,065, P < 0.001).
We compared between service users with comorbid schizophrenia and diabetes and controls with diabetes. Annual haemoglobin A1C tests were slightly lower among service users with schizophrenia (1.8 ± 1.9) than among counterparts (1.9 ± 1.8) (unadjusted F = 10.4, df = 1, 10,656, P < 0.001; adjusted F = 21.1, df = 1, 10,495, P < 0.001). The haemoglobin A1C level was minimally lower among the former (7.7% ± 1.8%) than among counterparts (7.8% ± 1.6%) (unadjusted F = 4.9, df = 1, 8934, P = 0.027; adjusted F = 6.6, df = 1, 8804, P = 0.01). Less annual LDL tests were done by service users with schizophrenia (1.1 ± 0.8) than in counterparts (1.2 ± 0.8) (unadjusted F = 37.5, df = 1, 13,330, P < 0.001; adjusted F = 48.4, df = 1, 13,117, P < 0.001), but the LDL level was similar in both groups (schizophrenia: 121.8 ± 29.2; control: 120.5 ± 27.9; P = 0.22). A higher rate of the service users with schizophrenia (76.4%) used antidiabetic medications compared with their counterparts (70.8%) (univariate OR, 1.34 [95% CI, 1.24 to 1.45]; adjusted OR, 1.29 [95% CI, 1.20 to 1.40]) (Table 3).
Use of Antidiabetic Medications among Service Users with Schizophrenia and Matched Controls.
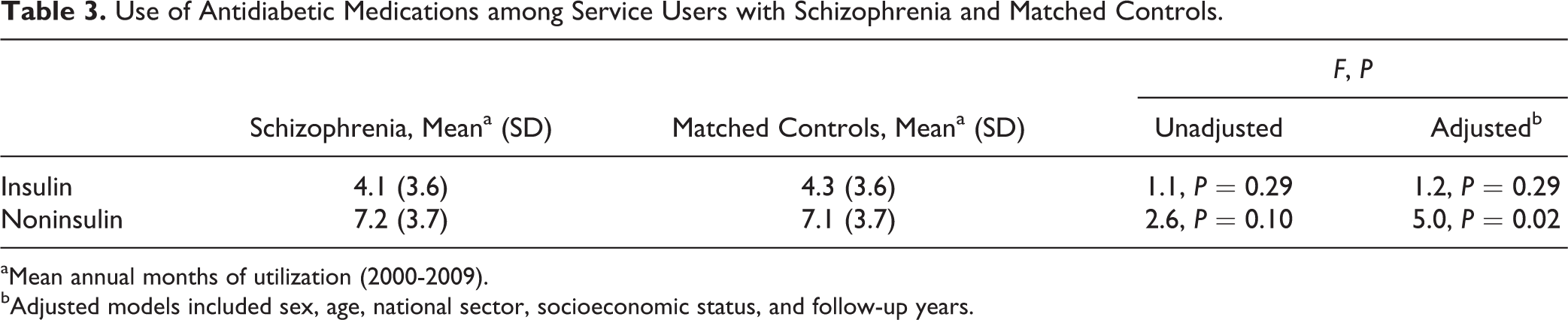
aMean annual months of utilization (2000-2009).
bAdjusted models included sex, age, national sector, socioeconomic status, and follow-up years.
No differences between persons with lower and higher severity of schizophrenia by number of annual haemoglobin A1C tests and level were found or in the utilisation of antidiabetic medications.
Service Users Diagnosed with Bipolar Disorder
The average annual blood tests and visits to specialists were higher among service users diagnosed with bipolar disorder, while no differences were found for stress tests and chest X-rays (Table 4). Throughout the study period, a higher rate of service users with bipolar disorder (49.0%) than their counterparts (40.9%) had at least 1 haemoglobin A1C test (univariate OR, 1.20; 95% CI, 1.11 to 1.30) but not in the adjusted analysis (adjusted OR, 0.96; 95% CI, 0.82 to 1.13). During the study period, 94.4% of the service users with bipolar disorder and 94.0% of their counterparts had at least 1 LDL test (univariate OR, 1.00; 95% CI, 0.95 to 1.06). The mean LDL level was slightly higher among service users with bipolar disorder (128.9 ± 29.3) than in controls (125.9 ± 27.0) (unadjusted F = 15.0, df = 1, 5849, P < 0.001; adjusted F = 14.7, df = 1, 5768, P < 0.001), while no difference in haemoglobin A1C level was observed (bipolar disorder: 6.7% ± 1.5%; controls: 6.7% ± 1.4%; P = 0.16).
Annual Rate of Recorded Health Measures among Service Users with Bipolar Disorder and Matched Controls.
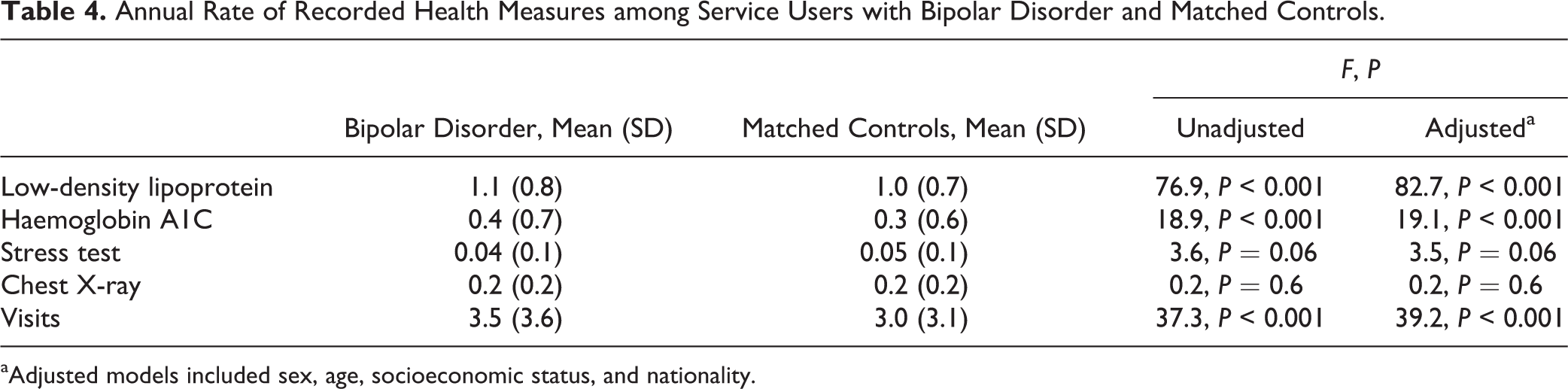
aAdjusted models included sex, age, socioeconomic status, and nationality.
The mean annual visits to specialists were higher among service users with bipolar disorder with lower (3.7 ± 3.7) compared to higher severity (3.3 ± 3.4) (unadjusted F = 8.5, df = 1, 2215, P < 0.001; adjusted F = 6.3, df = 1, 2163, P = 0.01).
Mortality
During the follow-up period, deaths were recorded in 19.4% of the service users diagnosed with bipolar disorder in contrast to 11.2% of the controls, a 1.7-fold risk at any fixed point of time (adjusted HR, 1.71; 95% CI, 1.52 to 1.93). The median age of death was slightly lower among service users diagnosed with bipolar disorder (73.5 y) than controls (74.0 y).
Diabetes
Higher rate of diabetes were noted among service users with bipolar disorder (n = 680, 31.8%) than their counterparts (n = 1277, 28.8%) (univariate OR, 1.16 [95% CI, 1.03 to 1.29]; adjusted OR, 1.14 [95% CI, 1.01 to 1.27]). The age of diagnosis did not differ between service users with bipolar disorder (63.7 ± 8.9) and their counterparts (64.2 ± 9.4) (P = 0.28).
Annual haemoglobin A1C tests (bipolar disorder: 1.9 ± 1.8; comparison: 1.9 ± 1.7; P = 0.84) and haemoglobin A1C level (bipolar disorder: 7.5% ± 1.6%; comparison: 7.6% ± 1.4%; P = 0.3) did not differ between the groups. Annual LDL tests did not differ between service users with bipolar disorder (1.4 ± 0.9) and their counterparts (1.3 ± 0.8) (P = 0.09), but the level of LDL was higher in service users with bipolar disorder (124.8 ± 29.7) than their counterparts (118.3 ± 26.7) (unadjusted F = 21.8, df = 1, 1729, P < 0.001; adjusted F = 20.6, df = 1, 1692, P < 0.001). Similar rates of service users with bipolar disorder (75.4%) and their counterparts (74.7%) used antidiabetic medication throughout the follow-up period (P = 0.38). The annual utilisation did not differ between the groups (Table 5).
Use of Antidiabetic Medications among Service Users with a Bipolar Disorder and Matched Controls.
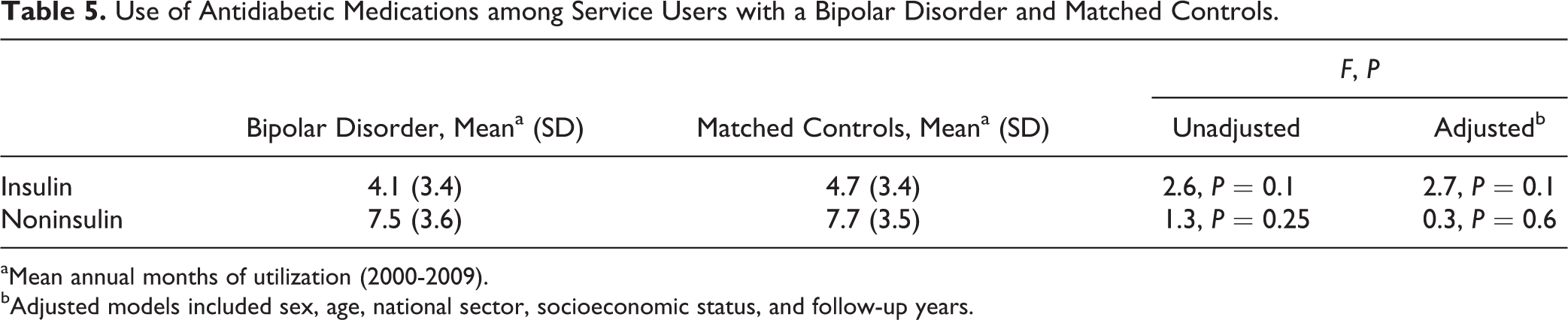
aMean annual months of utilization (2000-2009).
bAdjusted models included sex, age, national sector, socioeconomic status, and follow-up years.
No differences between persons with lower and higher severity of bipolar disorder by number of annual haemoglobin A1C tests and level were found or in the utilization of antidiabetic medications.
Discussion
The results showed limited health care disparities among service users with SMI. Slightly lower measures of LDL, stress tests, chest X-rays, and visits to specialists were found among persons with schizophrenia. In contrast, among persons with bipolar disorder, the results often showed a reversed pattern: they either did not differ or had higher health care measures than their counterparts. Among both groups of service users, lower severity of the psychiatric condition was associated with more visits to specialists. In addition, among both groups of service users, no disparities were noted in the health services provided to those with comorbid diabetes. However, premature mortality was unfailingly higher among the SMI groups compared to controls.
Differences were noted between service users with schizophrenia and bipolar disorder and their respective controls. In almost all comparisons, users with bipolar disorder differed less from their counterparts or even had higher health care measure rates. This may reflect longer periods of illness remission and/or better functioning than among persons with schizophrenia. This explanation is partly supported by the observed effects of illness severity on the use of health services among service users with SMI. Analogous findings were reported on persons with comorbid cardiovascular illness in the United Kingdom 35 and Taiwan, 17 as well as among persons with SMI and comorbid diabetes in the United Kingdom. 36 However, a Danish study reported less cardiovascular medication prescriptions to persons with either schizophrenia or bipolar disorder. 37 In addition, among Medicaid enrollees in the United States, disparities of diabetes care were present for both schizophrenia and bipolar disorder patients. 38
Based on previous findings of health care disparities among service users with a comorbid cardiovascular disorder in Israel, we hypothesized that diabetes care for persons with SMI will fail to meet the standards of the general population. 15 This hypothesis was disproved, a finding that should be highlighted. The increased rate of diabetes amongst service users with SMI adds to the burden carried by this vulnerable population. 18,19 It is possible that the equality of care we found may be attributed to the availability, accessibility, and the quality of the specialized services in Israel. Specifically, according to the National Quality Indicators Program (NQIP), the treatment of persons with diabetes should follow current standards of medical care, 24 including annual haemoglobin A1C and LDL tests and the use of antidiabetic medications. The CHS has implemented the NQIP’s recommendations since 2001 in both primary care and specialized diabetes clinics, enabling improved follow-up and case management. The positive outcomes of the program are supported by our study. Importantly, these services are facilitated by the National Health Insurance that grants all service users free and direct care. Conceivably, the availability of services provided by the rehabilitation law (see above) could be an enabling factor, although it was not directly tested here.
The above findings, however, did not translate into the correction of premature mortality among persons with SMI reported in Israel. 1 Thus, unfailingly higher mortality was seen during the follow-up period among both SMI groups compared to controls. Interestingly, based on an identical database of computerized health records, similar findings were reported in the United Kingdom: equality of health services to persons with SMI and comorbid diabetes 36 together with premature mortality. 23 However, it is important to note that while in this study we have found no disparities in the health care of persons with SMI and diabetes, another study of the same data indicated disparities of care to persons with SMI and comorbid cardiovascular disease, which could contribute to the excess mortality. 15
These contrasting results raise a question regarding the health services provided to persons with SMI. Conceivably, equality is not the parameter to use in addressing the needs for specialized care, particularly for users with schizophrenia, in whom the mortality risk is so much higher and a higher care standard should be applied. In line with the concept of equity, specific health care recommendations to persons with SMI were raised in the literature, including case management (e.g., frequent haemoglobin A1C and LDL tests in patients starting antipsychotic medications, structured programs to control weight gain 39,40 ), and policy recommendations. 41 Accordingly, a recent study reported on the efficacy of a structured diabetes care for persons with SMI in reducing mortality rates. 42 Nevertheless, the positive outcome expected from such programs is somewhat tempered by estimations that despite optimal care, the reduction of mortality due to comorbid physical disorders among persons with SMI reaches a ceiling of 50%. 2
This study has several limitations. First, our data are based on the performance of the medical procedures rather than on the examination of doctors’ prescriptions. Therefore, we could not differentiate between possible stigmatic actions of the treating physicians and the users’ adherence to care. 43 This distinction is specifically important with regard to service users with schizophrenia since their clinical condition may compromise their health behavior, compared to the general population. Second, we did not have access to information on risk factors (e.g., smoking and obesity). Third, no information regarding the causes of death was available. For example, a different interpretation would apply if much of the burden is due to external rather than internal causes. Fourth, the data on the people with SMI in our study are based on the PCR, which is a hospitalisation registry, and might not reflect persons with SMI who were never hospitalized. However, this may be more relevant to persons with bipolar disorder since with regard to schizophrenia, more than 90% of diagnosed persons do appear in the PCR. 44 Fifth, much fewer people with bipolar disorder were identified in the PCR compared to people with schizophrenia, although the prevalence rates of these disorders are generally similar. However, 2 aspects related to specific characteristics of mental health care in Israel and the PCR should be considered: 1) based on research diagnostic criteria, a cohort study in Israel reported that the 6-months prevalence rate of bipolar disorder (0.1%) is lower than schizophrenia (0.7%), 45 and 2) based on the former study, a follow-up study found that 93% of the individuals diagnosed with schizophrenia at ages 25 to 34 were present in the PCR. 44 We do not have similar data on persons diagnosed with bipolar disorder, but due to the greater severity of schizophrenia, it is reasonable to assume that the rate is lower. Taken together, these findings suggest that the prevalence of people with bipolar disorder in the PCR is expected to be lower compared to schizophrenia.
We think, however, that the limitations are in part balanced by the large size of the populations investigated, the different nature of the measures used, the careful recording of the information collected on the users, and the consistency of the results.
Conclusion
In a country with a national health insurance and a rehabilitation law for persons with SMI, service users with bipolar disorder receive equitable levels of general health care. Users with schizophrenia receive slightly lower services than the standards but not with regards to persons with comorbid diabetes. These positive effects could be attributed to the existence of specific protective legislation. In contrast, mortality rates remain elevated in persons with SMI.
Footnotes
Acknowledgements
The data used in this report were made available by Inna Pugachova from the PCR and Shachar Merling from CHS. The authors thank Dr. Kenneth Gabbay (Baylor Medical School, Houston) for his comments on diabetes.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Munitz is employed by Clalit Health Services. The authors G.G. and I.L. declare that they have no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by The Israel National Institute for Health Policy and Health Services Research (grant number r/14/2010).
Ethical Standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.