
Abstract
Objective:
The present guidelines address the pharmacotherapy of schizophrenia in adults across different stages, phases, and symptom domains.
Method:
Guidelines were developed using the ADAPTE process, which takes advantage of existing guidelines. Six guidelines were identified for adaptation, with recommendations extracted from each. For those specific to the pharmacotherapy of schizophrenia in adults, a working group selected between guidelines and recommendations to create an adapted guideline.
Results:
Recommendations can be categorized into 6 areas that include 1) first-episode schizophrenia, 2) acute exacerbation, 3) relapse prevention and maintenance treatment, 4) treatment-resistant schizophrenia, 5) clozapine-resistant schizophrenia, and 6) specific symptom domains. For each category, recommendations are made based on the available evidence, which is discussed and linked to other established guidelines.
Conclusions:
In most cases, evidence-based recommendations are made that can be used to guide current clinical treatment and decision making. Notably, however, there is a paucity of established evidence to guide treatment decision making in the case of clozapine-resistant schizophrenia, a subsample that represents a sizable proportion of those with schizophrenia.
Keywords
The present guidelines address the pharmacological treatment of schizophrenia across different stages and phases of the illness, in addition to different symptom domains. They are part of the updated Canadian Schizophrenia Guidelines, developed for the treatment of schizophrenia and related disorders and reflecting the Canadian Health Care System (see Guidelines Introduction for details). In brief, they build on previously published guidelines, 1 with multidisciplinary teams of experts, patients, and family carers providing input across a number of selected topics.
Target users are health care professionals, with recommendations provided as guidance to physicians and patients to improve the overall standard of care.
The following principles guided the development of the present guideline:
Schizophrenia represents a heterogeneous group of disorders that may differentially affect presentation, course, treatment response, and outcome. Common to these different groups is psychosis, which is integral to the diagnosis of schizophrenia and schizophrenia spectrum disorders. Antipsychotic medications play a central role in recommendations related to pharmacotherapy. Over the course of schizophrenia, psychotic symptoms can wax and wane, and decision making regarding use of antipsychotics is influenced by treatment response and side effects, as well as phase of illness (acute vs. stable). Other symptom domains besides psychosis can be observed as well in the context of schizophrenia and schizophrenia spectrum disorders; accordingly, other types of medications may also be recommended during the course of treatment.
To capture these aforementioned principles, recommendations are categorized into 6 areas:
First-episode schizophrenia Acute exacerbation Relapse prevention and maintenance treatment Treatment-resistant schizophrenia Clozapine-resistant schizophrenia Specific symptom domains
While the guidelines are meant to address general principles related to pharmacotherapy, they do not speak to the numerous more specific issues that clinicians must also contend with daily in optimizing treatment (e.g., switching strategies, side effect profiles, drug interactions, etc.).
Methods
The methods for the Canadian Schizophrenia Guidelines are described in brief here; please see the Introduction and Methodology article, which precedes the different guidelines in this issue, for an in-depth description.
The guidelines were developed using the ADAPTE process. 2 Recognizing that the development of guidelines requires substantial resources, the ADAPTE process was created to take advantage of existing guidelines and reduce duplication of effort.
The first phase of the ADAPTE process, the Set Up Phase, involved preparing for the ADAPTE process. We assembled a national multidisciplinary panel from across Canada, including stakeholders with expertise in schizophrenia and mental health, health policy, patient advocacy, and lived experience with schizophrenia. Endorsement bodies for the guidelines include the Canadian Psychiatric Association and the Schizophrenia Society of Canada, who were also heavily involved in the dissemination and implementation strategy.
The second phase of the ADAPTE process, the adaptation phase, involves the process of identifying specific health questions; searching for and retrieving guidelines; assessing guideline quality, currency, content, consistency, and applicability; decision making around adaptation; and preparing the draft adapted guideline. We searched for guidelines on schizophrenia in guideline clearinghouses and on the websites of well-established guideline developers for mental health disorders including the National Institute for Health and Care Excellence (NICE), the Scottish Intercollegiate Guidelines Network (SIGN), the American Psychiatric Association, the American Academy of Child and Adolescent Psychiatry, and the European Psychiatric Association. A MEDLINE search was also performed using the term guideline as publication type and schizophrenia as title or clinical topic. Inclusion criteria were that the guideline needed to be published after 2010, be written in English, and that recommendations had to be developed using a defined and systematic process.
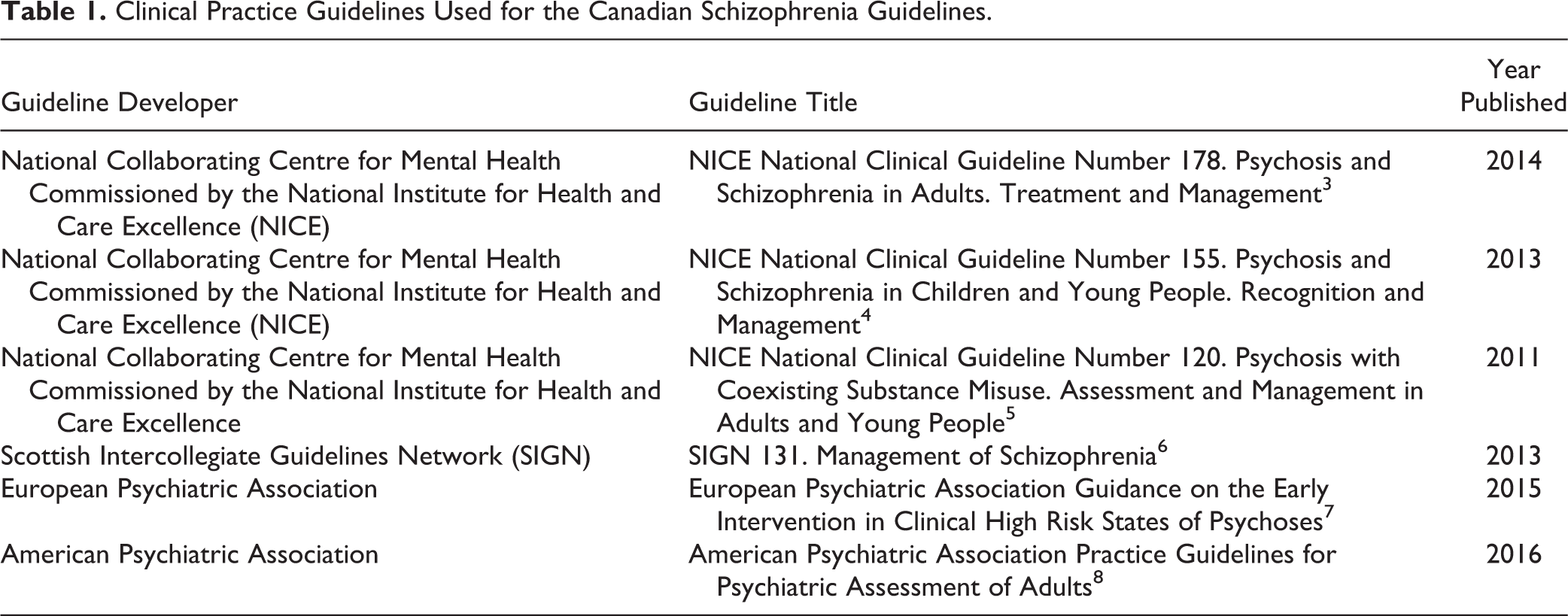
We identified 8 current guidelines that were potentially suitable for adaptation. These guidelines were reviewed and evaluated in duplicate using the AGREE II tool, 2 an instrument to evaluate the methodological rigor and transparency in which a guideline is developed. Based on this evaluation, we determined that the 6 guidelines were of suitable quality and content for adaptation (see Table 1). Recommendations from each guideline were extracted and divided based on content and reviewed by the relevant working group. Following the ADAPTE process, working groups selected between guidelines and recommendations to create an adapted guideline. Each working group carefully examined each recommendation, the evidence from which the recommendation was derived, and the acceptability and applicability of the recommendation to the Canadian context.
Clinical Practice Guidelines Used for the Canadian Schizophrenia Guidelines.
After reviewing the recommendations from the guidelines, the working groups decided which recommendations to accept and which to reject and which recommendations were acceptable but needed to be modified. Care was taken when modifying existing recommendations not to change the recommendations to such an extent that they were no longer in keeping with the evidence on which they were based. Please see the appendix for how and why recommendations in this article were modified from their original form.
De novo recommendations were made in situations in which it was felt a recommendation was needed but none of the existing guidelines provided recommendations addressing the situation or topic. When de novo recommendations were created, the SIGN methodology was followed for the levels of evidence and the grades of recommendation (see Table 2).
Grade/strength of recommendation classification systems for included guidelines.a
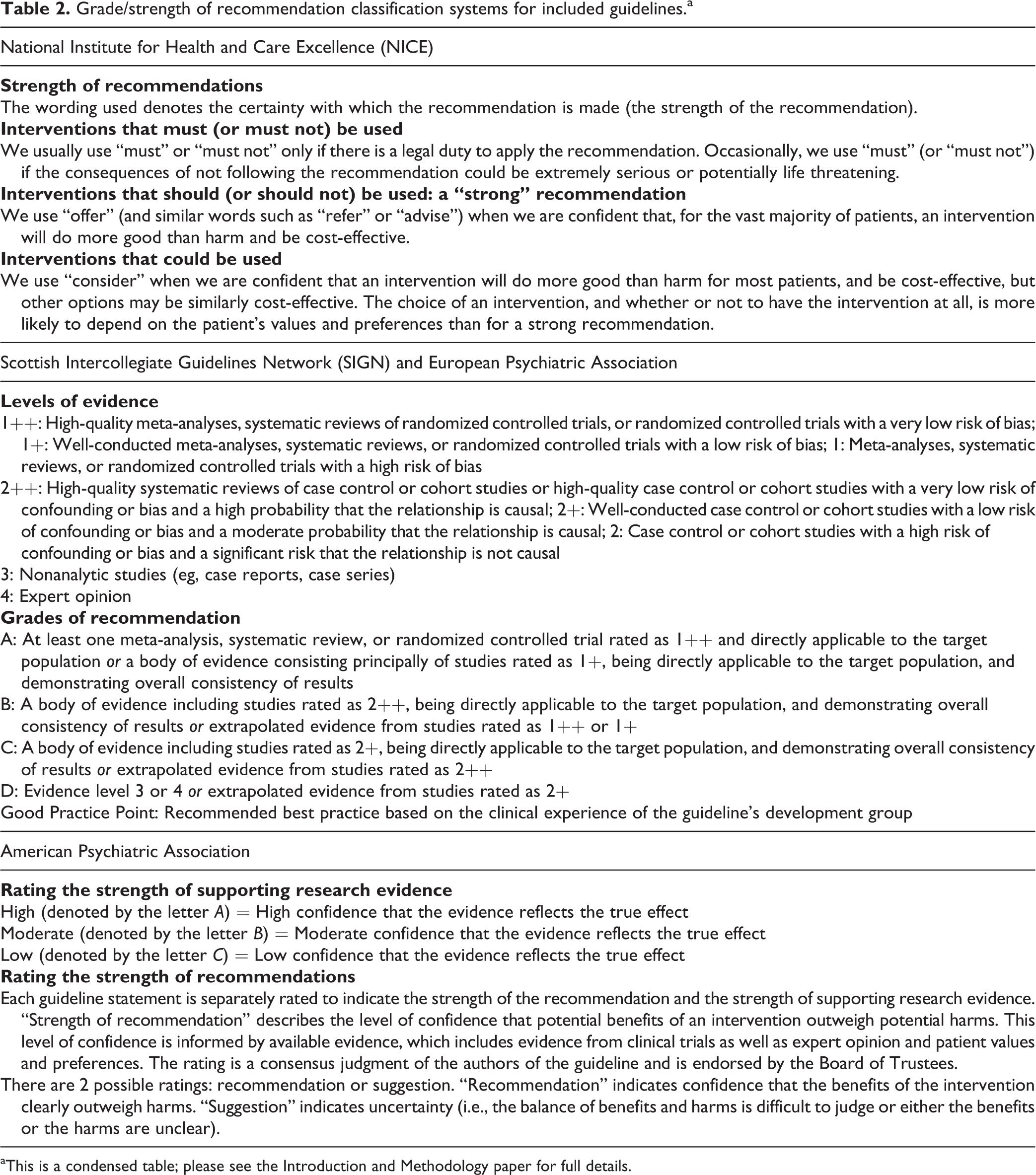
aThis is a condensed table; please see the Introduction and Methodology paper for full details.
Each working group developed a final list of recommendations from the included guidelines that were presented to the entire guideline panel at an in-person consensus meeting. Working group leaders presented each recommendation and its rationale to the panel. Anonymous voting by the entire panel using clicker technology was performed for each recommendation. Recommendations required agreement by 80% of the group to be included in the Canadian guidelines. If a recommendation did not receive 80% agreement, the group discussed the recommendation and whether minor modifications to the recommendation would alter the likelihood that the recommendation would pass. In these situations, recommendations were modified (as described above) and the group revoted at a later date using an online anonymous survey. Whenever modifications in wording were made to original recommendations, the text “modified recommendation from” appears in the Canadian Schizophrenia Guidelines, and the source of each recommendation is written beside the recommendation statement.
The strength or grade of the recommendation is provided in brackets if applicable, using the system from which the recommendation came. The grades of recommendation for each reference guideline and their meaning are explained in brief in Table 1 (see the Introduction and Methodology chapter for a more detailed description). Once the voting and consensus process was completed, each working group created a separate manuscript that contains all the recommendations adapted from the included guidelines, with accompanying text explaining the rationale for each recommendation.
During the finalization phase, the Canadian Schizophrenia Guidelines were externally reviewed by those who will be affected by its uptake: practitioners, policy makers, health administrators, and patients and their families. The external review asked questions about whether the users approve of the draft guideline, strengths and weaknesses, and suggested modifications. The process was facilitated through the Canadian Journal of Psychiatry and the Schizophrenia Society of Canada. The Canadian Psychiatric Association Clinical Practice Guidelines Committee reviewed and approved the guideline methodology process.
Recommendations: Pharmacotherapy of Schizophrenia in Adults
A. First-Episode Schizophrenia
Recommendation 1: Use of Antipsychotics
For patients with first-episode psychosis, antipsychotic medication should be recommended.
[Modified from NICE (Strong recommendation)]
“First-episode psychosis” and “first-episode schizophrenia” are frequently used interchangeably because, in the earliest stages of treatment, specific diagnosis may remain unclear (e.g., related to concomitant substance abuse or brief duration of illness at the time of assessment/intervention). A diagnosis of schizophrenia requires continuous signs over a period of at least 6 months, 9 although, even then, clinicians must be vigilant regarding the possibility of change in diagnosis. 10 A recent meta-analysis has reported high diagnostic specificity for first-episode schizophrenia spectrum psychoses. 11 In terms of treatment effects, a recently published meta-analysis examining acute antipsychotic use in early schizophrenia concluded that data were too limited to assess outcomes, highlighting the lack of evidence comparing pharmacological interventions to placebo or other treatments. 12 Ethical concerns discourage placebo-controlled trials in this population, although antipsychotic efficacy has been established through studies evaluating relapse rates in the face of antipsychotic discontinuation following treatment for a first episode. 13,14 Three meta-analyses support a relationship between shorter duration of untreated psychosis and improved outcomes, although the magnitude of the association is modest and there are limited data evaluating differences over the longer term. 15 –17
Recommendation 2: Antipsychotic Choice
Choice of antipsychotic medication should be made by the patient and physician together, taking into account views of a carer where appropriate. Provide information and discuss the likely benefits and side effects of each drug.
[NICE (Strong recommendation)]
The inconsistency of findings argues against established clinical superiority for a specific antipsychotic in first-episode schizophrenia or, in fact, antipsychotic class (i.e., second-generation antipsychotic [SGA] vs. first-generation antipsychotic [FGA]). In meta-analyses specific to early or first-episode schizophrenia, one reported no differences between antipsychotic class in terms of efficacy or discontinuation rates but clear side effect differences. 18 A more recent meta-analysis reported that SGAs were superior to FGAs in terms of all-cause discontinuation rates (number needed to treat = 12), although, again, they appeared similar in terms of changes in total psychopathology. 19 Decision making is routinely guided by side effect profile, which differs between and within medication classes. Just as side effects, including motor and metabolic, can be more pronounced in antipsychotic-naïve first-episode patients, 20,21 blinded randomized controlled trials (RCTs) confirm that response rates are higher in those with a first episode. 22 –24 This may introduce a ceiling effect that diminishes the likelihood of capturing differences in efficacy between agents and/or drug class in the first-episode patient group. As well as side effects, decision making should address information regarding what constitutes a medication trial (e.g., dosing, duration, response patterns) and options in the face of a suboptimal response.
Recommendation 3: Acute Antipsychotic Treatment
Following initiation of an antipsychotic medication for patients in the first episode of psychosis, the medication should be continued for at least 2 weeks unless there are significant tolerability issues. Assessment of dose and response should be monitored during the early phase of prescribing. Where there is poor response to medication, there should be assessment of medication adherence and substance use before lack of response can definitely be established. If there is no response to medication after 4 weeks, despite dose optimization, a change in antipsychotic should be considered. Where there is partial response, this should be reassessed after 8 weeks unless there are significant adverse events.
[SIGN (Grade D)]
The objective in acute treatment is an adequate clinical trial in terms of dose and duration. The evidence suggests that an adequate trial should be between 4 and 6 weeks. 25,26 This said, treatment must be individualized to accommodate tolerability and trajectory of response, both of which can vary between individuals. 27,28 In addition, it is essential to take into account nonpharmacological factors that can compromise response, in particular antipsychotic nonadherence and/or comorbid substance abuse. 29 Evidence indicates that clinicians’ capacity to accurately identify those who are nonadherent is limited, 30,31 and complementing this with other strategies such as psychoeducation, simplified dosing regimens (e.g., once vs. twice daily), blister packs, use of dosettes, caregiver support, pill counts, and therapeutic drug monitoring may prove useful. 32 In addition, consideration should be given to different formulations. 33 In the case of long-acting injections (LAIs), earlier use in the course of treatment has been advocated, as has the point that discussions regarding their use should not be confined to only those for whom nonadherence is a concern. 34
Recommendation 4: Antipsychotic Dose and Trial Duration
Target the lower end of the therapeutic effective dose range of antipsychotics to be used in individuals in the first episode of schizophrenia and titrate according to efficacy and tolerability.
[Modified from SIGN (Grade D)]
There has been a shift in how antipsychotics are administered in acute psychosis. Historically, practice routinely involved high doses from the onset of treatment, with a possible reduction during the maintenance phase of treatment. In contrast, the approach now favours initiation at doses in line with the lower end of therapeutic dose recommendations. 35 An adequate clinical trial involves an initial titration phase over several weeks, followed thereafter by a period of approximately 6 weeks on an adequate therapeutic dose (i.e., operationalized as the midpoint or beyond of the licensed therapeutic dose range). 26 In contrast to what was thought in earlier years, much of the antipsychotic effect is evident in the first several weeks of treatment. 36 Individuals can undergo antipsychotic trials that may not be considered adequate clinical trials because of different factors including inadequate dose or trial duration, medication nonadherence, comorbid substance abuse, or a combination thereof. This becomes important in establishing when an individual meets criteria for treatment resistance and eligibility for clozapine.
Recommendation 5: Antipsychotic Continuation
Following resolution of positive symptoms of the first episode of schizophrenia, the duration of maintenance treatment with antipsychotics should be at least 18 months.
[Modified from SIGN (Grade D)]
The question of how long an individual must continue treatment once symptoms have resolved following a first episode of psychosis arises routinely in clinical practice. This is not surprising as this is generally a young population, and the idea of having to maintain treatment in the absence of symptoms, particularly in light of their side effect profile, is difficult to accept. Older, longitudinal studies suggest that between 1% and 20% of individuals experience only a single episode of psychosis 37,38 ; however, there are no clearly established markers, biological or clinical, that can be used to guide this decision making. Current evidence indicates that relapse rates are high in the face of antipsychotic discontinuation; moreover, attaining remission and/or stabilization for a period of time on maintenance treatment does not eliminate this risk. 13,14,39 For example, in a 5-year follow-up study of first-episode patients who had responded to treatment (N = 104), the cumulative risk of a first relapse was 82% and the risk of a first or second relapse was 5 times greater in those not taking medication as compared with those who were. 14 Finally, there is also evidence, albeit not in the form of RCTs, that response can be compromised in the face of relapse. 40,41 Research studies continue to explore the possibility that a guided discontinuation strategy may be used in selected patients.
B. Acute Exacerbation
Recommendation 1
Following an increase or change of antipsychotic medication in response to acute exacerbation of schizophrenia, the medication should be continued for at least 4 weeks unless there are significant tolerability issues. Where a partial response is seen after review at 4 weeks, the medication should be reassessed after 8 weeks unless there are significant adverse effects.
[Modified from SIGN (Grade D)]
The course of schizophrenia is frequently characterized by symptoms that wax and wane; continued antipsychotic use appears to diminish, but not eliminate, risk. 42,43 While exacerbations may be self-contained, there are occasions where intervention is required, routinely in the form of antipsychotic dose adjustments or a switch to another antipsychotic. A worsening of symptoms may be linked to issues such as antipsychotic nonadherence and/or substance abuse, 44,45 and as part of longer-term management, it is important that these be addressed. Exacerbations under these sorts of circumstances do not constitute a failed antipsychotic trial, and decisions regarding a switch in antipsychotic or use of higher doses over the longer term need to take this information into account. For example, a switch in formulation to a depot or LAI antipsychotic may represent the preferred strategy in an individual in whom antipsychotic nonadherence plays a clear role in acute exacerbations. However, it is also recognized that relapse can occur in the absence of such clear risk factors, 46 and repeated exacerbations may support higher doses, if effective, or a switch to another antipsychotic. Two clearly identified adequate but failed antipsychotic trials establish the diagnosis of treatment-resistant schizophrenia, at which point clozapine is the treatment of choice. 26
C. Relapse Prevention and Maintenance Treatment
Recommendation 1: Antipsychotic Dose
Following an acute episode of schizophrenia, individuals should be offered maintenance treatment with antipsychotic medication at low or moderate regular dosing of around 300 to 400 mg of chlorpromazine equivalents, 4 to 6 mg of risperidone, or other equivalents daily.
[Modified from SIGN (Grade B)]
By the late 1980s and early 1990s, investigations began to challenge the high doses of antipsychotics being used in both acute and maintenance treatment. A biphasic relationship between dose and efficacy was reported in a review of this topic, with no improvement and even clinical worsening as doses were increased. 47 A subsequent meta-analysis suggested no clinical benefits with doses exceeding chlorpromazine 375-mg equivalents. 48 Since then, a shift in practice patterns has taken place, with clinicians using lower doses acutely and less aggressive titration; as a result, the optimal antipsychotic dose identified for an individual may better approximate what might constitute the maintenance dose. 35 This said, work continues in an effort to better delineate optimal maintenance dosing. To date, the only empiric strategy for establishing dose equivalents is dopamine D2 occupancy, as measured using in vivo neuroimaging. However, such data are not available on all antipsychotics and, for some (e.g., aripiprazole, clozapine, quetiapine), their pharmacology prevents such comparisons. 49 Dosing may also be affected by such factors as stage of illness (e.g., first episode vs. later stages) as well as age (e.g., geriatrics).
Recommendation 2: Duration of Treatment
Following resolution of positive symptoms of an acute episode of schizophrenia, patients should be offered maintenance treatment and antipsychotic medication for 2 and possibly up to 5 years or longer.
[Modified from SIGN (Grade A)]
Three recent meta-analyses have confirmed the benefits of antipsychotic treatment in relapse prevention. 42,43,50 This was also associated with lower hospitalisation rates and limited evidence of improved quality of life. 42,43 However, the benefit of SGAs versus FGAs was either not identified or, at best, modest. 43,50 As might be expected, those receiving active treatment reported a higher incidence of antipsychotic-related side effects (e.g., weight gain, movement disorders). 43 Of note, maintenance/relapse studies generally represent follow-up periods no longer than a year. 43,50 For example, in one meta-analysis involving 65 trials (N = 6493), the median study duration was 26 weeks (range = 1.75-156). 43 A second meta-analysis, involving 23 RCTs (N = 4504) reported a mean maximum study duration of 61.9 weeks (range = 40-104). 50 It has been established, however, that several years of stabilization do not confer immunity to relapse. In a 5-year follow-up study of first-episode patients with schizophrenia or schizoaffective disorder who had been stabilized at the end of 1 year of antipsychotic treatment (N = 104), 81.9% relapsed by the end of 5 years. 51
Recommendation 3: Antipsychotic Delivery
Patients should be given the option of oral or depot antipsychotic in line with their preference.
[SIGN (Good Practice Point)]
Historically, LAI antipsychotics have been seen as targeting individuals who are nonadherent with oral treatment; indeed, this is why they were developed. 52 More recently, though, the argument has been made that they should be offered as a treatment option to all individuals receiving ongoing antipsychotic therapy. 34,53,54
There is evidence that LAI antipsychotics are now being used earlier in the course of treatment, and a recent review of this topic, which included 3 RCTs, has supported their superiority over oral agents in reducing relapse rates in early schizophrenia. 55 A more recent RCT in first-episode schizophrenia demonstrated better symptom control and a 6-fold reduction in relapse at 1 year with the LAI formulation. 56 Along similar lines, a large nationwide registry study, involving >2500 patients hospitalised for the first time with schizophrenia over a 7-year period, reported risk of rehospitalisation for those on LAI treatment to be approximately one-third of that for patients on oral treatment; notably, only a minority of patients adhered to their initial antipsychotic during the first 60 days of treatment. 57 In contrast, there have been other meta-analyses 58 –60 as well as randomized trials 61,62 that have challenged the benefit of LAIs. The case has been made, however, that study design may play a significant role in negative findings. More specifically, it has been suggested that the rigor of RCTs, with their focus on efficacy, results in the exclusion of individuals who are nonadherent, a group that would benefit from LAI treatment and one more readily captured through more naturalistic trials focused on effectiveness. 63 –65
Finally, while patient preference is seen as important, there may be circumstances that do not allow this option (e.g., community treatment orders).
D. Treatment-Resistant Schizophrenia (TRS)
Recommendation 1: Clozapine
Clozapine should be offered to patients who have TRS.
[SIGN (Grade A)]
It is estimated that 25% to 30% of individuals with schizophrenia meet criteria for TRS. 66,67 In this population, RCTs have reported response rates in the range of 30% to 60% with clozapine, 68 and established guidelines identify it as the only recommended treatment in TRS. 69 In contrast, use of high doses, switching, and combined antipsychotics have no consistent evidence to support their use. 70 –72 Evidence indicates that clozapine is often delayed or simply not used when indicated. 73 –75 Research and meta-analyses continue to examine the strength of the apparent unique role for clozapine in TRS, and some caveats may exist. 76,77 Details regarding the use of clozapine in TRS have been addressed in the Assessment section.
Recommendation 2
Clozapine should be considered for patients whose schizophrenia has not responded to two antipsychotics. i
[Modified from SIGN (Grade B)]
The definition of treatment resistance varies across studies, especially with regard to the amount of improvement allowed on a non-clozapine treatment. A common definition of a maximum allowable treatment response has been a relative change in the representative scales (most frequently ≥20% decrease in the Positive and Negative Syndrome Scale). 78 From a clinical perspective, those with only a 20% reduction in positive symptoms after 2 or more adequate courses of non-clozapine antipsychotic medication continue to be a challenge. A systematic review of 26 RCTs of clozapine, including some that had a broader definition than the 20% improvement, found that clozapine had the most consistent evidence for efficacy. 3
E. Clozapine-Resistant Schizophrenia
Recommendation 1: Definition of Clozapine-Resistant Schizophrenia
An adequate antipsychotic medication trial is defined as including the following:
For oral antipsychotic drugs, at least 6 weeks of treatment at the midpoint or greater of the licensed therapeutic dose range
For LAI antipsychotic drugs, at least 6 weeks of treatment following reaching steady state (according to product monograph)
For clozapine, at least 8 but preferably 12 weeks at a dose of ≥400 mg/d is an adequate trial; where available, obtaining trough levels ≥350 ng/mL (1100 nM/L) for once-a-day dosing and ≥250 ng/mL for equal divided dosing is suggested
Documentation of adherence using approaches such as pill counts or dispensing chart reviews and, where available, with antipsychotic plasma levels on at least 1 occasion
Persistence of 2 or more positive symptoms with at least a moderate level of severity, or a single positive symptom with severe or greater severity, following 2 or more adequate trials with different antipsychotic drugs defines antipsychotic treatment–resistant schizophrenia
Following an adequate trial with clozapine, if the criteria above continue to be met, the specifier clozapine-resistant schizophrenia should be added
Recommendation 2
Treatment resistance in schizophrenia is a significant clinical concern and is associated with ongoing disability. The neurobiology of TRS shares some features with treatment-responsive forms of the illness and has other distinct features. 79 Defining antipsychotic treatment requires a strategy for assessing patient symptoms and assessing the adequacy of treatment. There is considerable variability in how treatment resistance is defined, 80 and although the range of symptoms to be included in a definition of treatment resistance continues to be debated, positive symptoms are central. 26 The assessment of response to antipsychotic medications or other treatments receives little attention in practice guidelines yet is critical for clinical decision making, especially regarding clozapine. The Health Canada–approved monograph for Clozaril contains only 1 sentence of guidance: “Non-responsiveness is defined as the lack of satisfactory clinical response, despite treatment with appropriate courses of at least two marketed chemically-unrelated antipsychotic drugs.” 81
[De Novo Recommendation (Good Practice Point)]
A comprehensive literature review examined criteria used in studies of TRS, 82 and subsequent recommendations by this and other groups have developed proposed definitions of this subtype of illness. 78 Such definitions can be used to support decision making for the use of clozapine early in the course of schizophrenia. 83 Assessing adherence is an essential step in identifying resistance to antipsychotic medication but is a significant challenge, 84 so a trial of injectable antipsychotics offers the best test of adherence. The present emphasis is on positive symptom severity and response as the key feature for assessment of treatment resistance. 26 This focus was also at the core of patient selection criteria and outcome assessment in the landmark study of clozapine in TRS. 85 This study required patients to have a moderate level of severity on 2 of 4 Brief Psychiatric Rating Scale (BPRS) items to be included (conceptual disorganization, unusual thought content, suspiciousness, and hallucinatory behaviour). The intent of the BPRS severity measure was that “moderate” would represent the average or modal severity of a symptom in all patients. 86 The anchored version of the BPRS describes “mild” severity of these symptoms as being definitely present, while symptoms at a “moderate” level of severity may or may not have an effect on behaviour but are more frequent, or extensive, than those of mild severity. 87
Recommendation 3: Treatment Options
No recommendation.
In North America, the introduction of clozapine as a treatment for TRS began in the 1990s, and its uptake into widespread clinical use for this population has been slow. 73 –75 Clozapine is not a panacea, with figures suggesting that in the range of 30% to 60% of those with TRS will respond favourably, 68 and in 2006, the first paper was published referring to “ultra-resistant schizophrenia” (i.e., those who demonstrate a suboptimal response to clozapine). 88 Criteria were identified, and since then, further recommendations have been made. The preference of the current guideline is to define these patients as having “clozapine-resistant schizophrenia” as it is a trial of clozapine and suboptimal response that allows them to be distinguished from those with TRS. 26 At this point, it is also unclear as to whether this patient group represents one or more other forms of the illness from the standpoint of treatment response. 26,89
To date, there are no meta-analyses that have globally evaluated the broad array of treatments investigated, which are routinely added to clozapine in the form of augmentation strategies. A limited number of RCTs have been carried out and summarized in more recent reviews. 70 –72
It remains that no one intervention has demonstrated robust and repeated effects that would substantiate its being identified as the established treatment of choice. The addition of other antipsychotics or electroconvulsive therapy has perhaps garnered the most attention, and in both cases, there are RCTs available. Although the SIGN guideline offers a number of possible augmentation strategies, the consensus of the present guideline is that, at present, there is insufficient evidence to make any specific recommendation.
Specific Symptom Domains
Recommendation 1: Aggression and Hostility
The choice of medication for treatment of irritability, hostility, and aggression should be based on patient preference, past experience of antipsychotic treatment, the adverse effect profile, and concurrent medical history. For individuals with TRS accompanied by aggression/hostility, a trial of clozapine is indicated.
[SIGN (Grade D)]
Aggression can be associated with psychosis, and in a recent meta-analysis of risk factors for aggression in individuals with psychosis, almost 90% were diagnosed with schizophrenia. 90 Numerous somatic treatments have been investigated and individual meta-analyses reported (e.g., haloperidol, 91 risperidone, 92 benzodiazepines 93 ), but as of yet, there has been no systematic analysis that has examined the options collectively.
In the past 5 years, there have been numerous reviews of this topic, 94 –102 and each highlights clozapine as a preferred treatment for psychosis associated with aggression. This confirms what was reported in earlier expert consensus guidelines. 103 In addition, a recently published systematic review, specific to clozapine, included 4 RCTs where it was compared with other antipsychotics; all trials found clozapine clinically superior in the treatment of aggression, and this appeared particularly evident in TRS. 104
Recommendation 2: Comorbid Depressive Symptoms
Individuals who meet criteria for depressive disorder should be treated according to relevant clinical practice guidelines for depression, including the use of antidepressants.
[SIGN (Good Practice Point)]
Depression is a common problem for people with schizophrenia at all stages of schizophrenia, with the prevalence of depressive symptoms varying according to the stage of the illness. Retrospective studies have shown that depressive symptoms frequently occur prior to the onset of psychotic symptoms in schizophrenia (i.e., those at clinical high risk of developing the illness), 107 first-episode schizophrenia, 108 and chronic schizophrenia. 109 An earlier systematic review of the use of antidepressants for the treatment of depression in people with schizophrenia provided cautious support, although the overall quality and number of studies was small. 110 A more recent descriptive review reached similar conclusions. 111 Given the large studies required to demonstrate the efficacy of treatments for depression in the general population, this result is not surprising. 112
Conclusion
There are numerous evidence-based recommendations that can assist in guiding clinical decision making related to the pharmacological treatment of schizophrenia in adults. At the same time, there are aspects of treatment where evidence is notably lacking. Examples include the issue of antipsychotic discontinuation in those who have responded effectively to treatment. Who might be eligible, possible predictors, and when this might safely be implemented all represent questions that remain unanswered presently. Similarly, treatment decision making in the case of clozapine-resistant schizophrenia currently faces a paucity of well-established evidence, despite numerous lines of investigation addressing the issue. While other guidelines have made recommendations within this realm, the present panel felt that no specific treatment warranted a firm recommendation at this time. Guidelines, of course, represent a work in progress, and identifying clear gaps in our knowledge might, in fact, be as important as affirming what we presently know.
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Remington has served as a consultant for Neurocrine Biosciences and Synchroneuron, received research support from Novartis and external funding from the Canadian Institutes of Health Research (CIHR) as well as Research Hospital Fund – Canadian Foundation for Innovation (RHF-CFI). Dr. Addington has nothing to disclose. Dr. Honer has received personal fees from Eli Lilly, Lundbeck, Otsuka, and Roche, as well as served on an advisory board for In Silico (no fee). Dr. Ismail has received external funding from the Canadian Institutes of Health Research (CIHR), and personal fees from Janssen, Eli Lilly, Lundbeck, Otsuka, Pfizer, and Sunovion, in addition to the Ontario Brain Institute (CAN-BIND Study). Dr. Raedler has received funding from the Mathison Centre for Mental Health Research and Education, personal fees from Janssen, Allergan, Bristol-Myers Squibb, and Sunovion, as well as clinical trial support from Roche, Forum, Boehringer-Ingelheim, Purdue, and Shire. Dr. Teehan has nothing to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplementary Material
Supplementary material is available for this article online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.