
Abstract
Objective:
The aim of this study is to compare Canadian suicide rates with other external causes of death to examine potential poisoning misclassifications as a contributor to suicide underreporting.
Method:
The study used Statistics Canada mortality data from 2000 to 2011 to calculate sex-and age-specific ratios by external cause of injury codes.
Results:
The overall Canadian suicide rate, as well as the poisoning suicide rate, declined over the study timeframe by an average annual percentage change (AAPC) of 1.0% each year. However, unintentional and undetermined poisonings increased significantly during the timeframe. Unintentional poisoning mortality (primarily narcotics and hallucinogens, including opioids) increased in proportion to suicides for both sexes, although females were consistently higher. The undetermined death to suicide ratio was higher and increasing for females. Poisonings of undetermined intent increased over time to comprise 47% to 80% of the undetermined death category for males and females combined.
Conclusions:
Canadian poisoning suicide rates declined, in contrast to rising unintentional and undetermined poisoning mortality rates. This trend is similar to that of the United States, supporting the hypothesis that misclassification of poisoning deaths may also be an issue in Canada.
Clinical Implications
Reliable statistics on suicide are essential to public health monitoring and suicide prevention programs in Canada.
Overall suicide rates have been decreasing in Canada; however, further exploration of the role of poisoning deaths and misclassifications to the overall suicide rate is required to understand this as a true decrease.
Limitations
This is an observational study in which underreporting of poisoning suicides due to misclassification can only be inferred.
Detailed description of type of poisoning agent involved in death is limited by ICD-10 external cause coding.
Canada has reported a modest reduction in overall suicide rates since 2000, with variation by age and sex; however, there were still almost 4000 suicides in 2011. 1 –3 The underreporting of suicide is a recognized concern in Canada and internationally. 4 –11 In particular, Rockett et al. 12 examined the countertrends of a declining suicide rate and an increasing unintentional poisoning mortality rate in the United States between 1987 and 2006 and concluded that misclassification may have contributed to changes in the suicide rate. However, there is no comparable Canadian research. Accurate surveillance of suicide is critical for effective research, prevention, and psychiatric interventions. 13,14
In Canada, all deaths that are unexpected, unexplained, or by violence are investigated by a coroner or medical examiner (C/ME). Coroners and medical examiners function under a provincial or territorial mandate. Although there are minor differences between the provinces, deaths by poisoning and deaths by suicide are investigated to some extent by all Canadian jurisdictions. The final opinions on cause and manner of death are reported to the Vital Statistics agencies of their respective jurisdictions. There is no national death investigative authority and no relevant national standards for medicolegal death investigation. Beginning in 2006, C/ME reports from most provinces have been collected and summarized within the Canadian Coroner and Medical Examiner Database (CCMED) of Statistics Canada. The CCMED still requires the signing of a number of agreements before it can qualify as a national database. The proportion of deaths investigated by a provincial coroner or medical examiner can range from 7% to 45% each year, although this varies greatly across provinces and territories. 15 After an investigation, which may or may not include autopsy, the C/MEs assign a cause of death (e.g., intoxication) and a manner of death (i.e., natural, accident, undetermined, homicide, or suicide). This informs the assignment of an external cause code from the International Statistical Classification of Diseases, 10th Revision (ICD-10).
International studies suggest that suicides are underestimated due to misclassification into other ICD-10 external cause of death categories, particularly unintentional and undetermined intents and when poisoning was the method. 16 –24 South Korea reported increasing suicide rates following improved accuracy in their manner of death classifications, suggesting an earlier masking of suicides among other categories. 25 A recent Canadian study by Auger et al. 26 reported that the inclusion of undetermined intent injuries could increase reported suicides by up to 26.5% for men and 37.7% for women; however, this study did not examine suicides misclassified as accidents. Earlier studies have estimated suicide rates to be underreported by 10% to 30% 5,11,20 due to difficulty in obtaining evidence to definitively rule on or diagnose intent for C/MEs, respectively. 27,28
The proposed causes of suicide misclassification are complex and include stigma, frequency, and extent of autopsies; disagreement amongst death investigators on burden of proof; lack of national death reporting standards; variation in local resources; changing attitudes of officials (e.g., police, coroners) and families involved; age and sex or subgroup of the decedent 6,8,10,21 ; rise in opioid poisonings 24,29,30 ; and the method or injury mechanism of death. 7 Violent forms of suicide, including firearms, asphyxia (includes hanging), and jumping, are more likely to be classified as suicide compared with other methods such as poisoning, which may provide more time to intervene, if discovered. 27,31
The purpose of this study is to present Canadian suicide rates between 2000 and 2011 by method or injury mechanism (e.g., poisoning), age, and sex in comparison to other external causes of death (unintentional, undetermined) to examine potential suicide misclassification.
Methods
Mortality data from 2000 to 2011, for ages 15 years and older, by sex, and selected external causes of injury (hanging, strangulation, and suffocation [henceforth referred to as hanging]; firearms; or poisoning, which are the leading causes of suicide) were retrieved from the Public Health Agency of Canada holdings of the Canadian Vital Statistics: Death Database (CVS: D) and the Canadian Socio-Economic Information Management System (CANSIM; accessed 2014 Dec). The external cause of injury or poisoning death was classified according to the ICD-10, adopted in Canada in 2000.
Statistical Analysis
Mortality rates for time trends were age-standardized using the direct method and the 1991 Canadian census population. 32 The average annual percentage change (AAPC), which is a weighted average of the annual percent changes (APCs), was calculated using Joinpoint software, providing the magnitude of trends for time periods identified by Joinpoints. 33
Based on the methodology described by Rockett et al.,
12
sex- and age-specific ratios were calculated by external cause of injury codes in each year (2000-2011): Ratio A (number of poisoning suicides/number of suicides) provides a measure of the relative use of poisonings as a means of suicide and allows observation of the change in this proportion over time. Ratio B (number of undetermined deaths [all nature of injuries]/number of suicides): by providing a ratio of unclassified intent deaths (undetermined) to those definitively classified as suicides, as well as assuming that some proportion of undetermined cases are in fact unidentified suicides, a crude measure of suicide underenumeration can be obtained. Since it is unlikely that all deaths of unclassified intent are actually misreported suicides, this ratio represents the maximum possible proportion of suicides misclassified as undetermined. Ratio C (number of unintentional poisonings/number of suicides) provides a second potential measure of suicide underenumeration, assuming that some proportion of unintentional poisonings are misclassified suicides, and again provides the maximal value possible. Ratio D (number of undetermined poisoning deaths/number of undetermined deaths [all nature of injuries]) provides a measure of what proportion of undetermined deaths are due to poisoning.
Results
The overall age-standardized suicide rate among Canadians 15 years and older has decreased slightly between 2000 and 2011, from 14.4/100,000 to 12.6/100,000 (AAPC, –1.0%; 95% CI, –1.6 to –0.4). The suicide rate decrease is due primarily to the decline in the male-standardized rates from 22.6 to 19.2/100,000 (AAPC, –2.0%; 95% CI, –3.0 to –0.9) while female suicide rates held constant at around 6.0/100,000 during this time period. Among males, the overall decrease is explained by declining rates of suicide by firearms (AAPC, –3.7%; 95% CI, –4.8 to –2.6) and poisoning (AAPC, –1.9%; 95% CI, –3.0 to –0.8). The female suicide rate overall remained flat, as the leading methods of suicide, poisoning and hanging, demonstrated no significant change.
A Joinpoint model was applied to poisoning rates by intent, as illustrated in Figure 1. Unintentional poisonings increased significantly by an APC of 7.4% between 2004 and 2011, while the undetermined poisoning rate jumped between 2000 and 2003 by an APC of 41.8% and then flattened. Suicide poisoning rates decreased by an AAPC of 1.2%, a steady but slight decline over the timeframe.
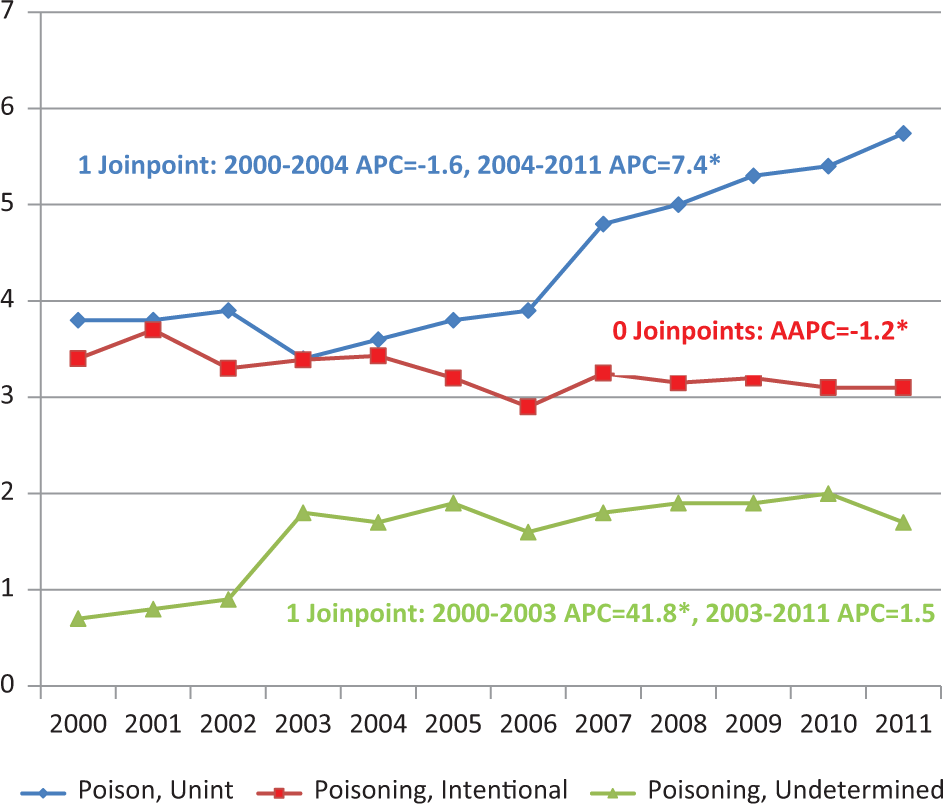
Poisoning mortality rates by intent, males and females combined, 15 years and older, Canada, 2000 to 2011 (age-standardized Canada, 1991).
Table 1 provides analysis of poisoning deaths by intent and substance. Drugs account for the majority of all poisoning deaths, regardless of intent (i.e., 83% in 2011, up from 72% in 2000). Both unintentional and undetermined poisonings were consistently and overwhelmingly comprised of drug deaths but experienced no important shift in the proportion of cases with drug involvement or the predominance of male cases (around two-thirds). However, the proportion of alcohol-related deaths did increase to surpass gases/vapours in both these categories. These patterns held when comparing males and females over time. Among intentional poisonings, drug-related deaths for both sexes combined rose from 57% in 2000 to 77% in 2011 and, in contrast to other intents, were equally distributed by sex; however, the proportion of female poisoning suicides involving drugs reached 89% in 2011 compared with 67% among males. This increase was accompanied by a decrease in gas/vapour suicides among both sexes, yet still accounting for 32% of male poisoning suicides in 2011.
Poisoning Deaths in Canada, 2011, by ICD-10 External Cause Code, Males and Females Combined, 15 Years and Older.
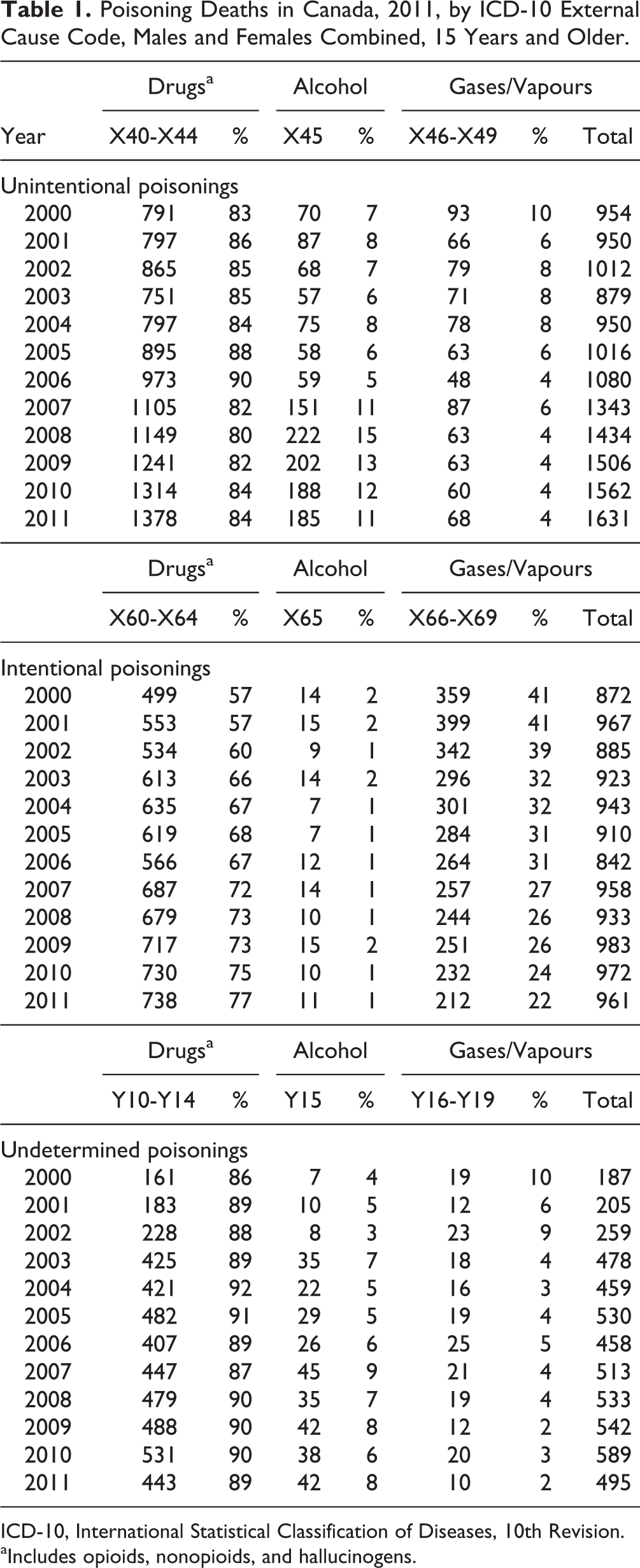
ICD-10, International Statistical Classification of Diseases, 10th Revision.
aIncludes opioids, nonopioids, and hallucinogens.
Figure 2 illustrates unintentional poisonings associated with certain drug categories or alcohol (ICD-10 codes X40-X44, X45), where there was a rise in mortality associated with narcotics and hallucinogens (X42) (which includes opioids), as well as other and unspecified drugs (X44) and alcohol (X45) in 2006, all contributing to the rising unintentional poisoning mortality rates. Although there were around twice as many unintentional poisoning cases among males as females, similar patterns were observed among both sexes.
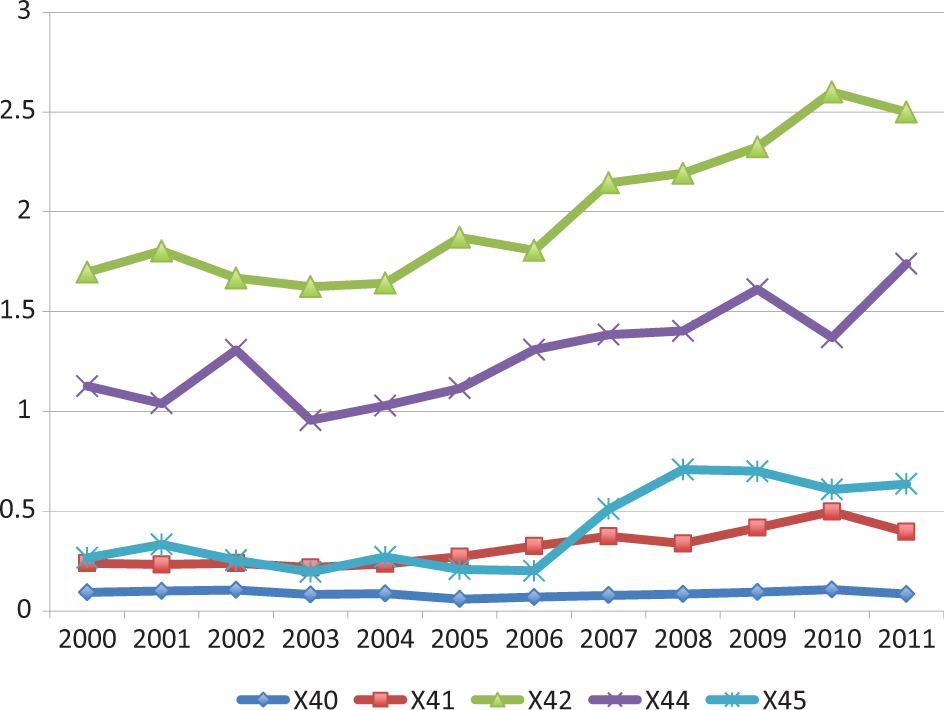
Rates of unintentional poisonings associated with drugs and alcohol, ICD-10 codes X40 to X42, X44 to X45, males and females combined, 2000 to 2011, age 15 years and older, Canada (age-standardized Canada, 1991). Drugs: [X40], Nonopioid analgesics, antipyretics and antirheumatics; [X41], Antiepileptic, sedative-hypnotic, antiparkinsonism and psychotropic drugs; [X42], Narcotics and psychodysleptics (hallucinogens); [X44], Other/unspecified drugs, medicaments and biological substances; Alcohol: [X45], Alcohol.
Ratio A: Poisoning Suicides/Suicides
Overall, poisoning suicides accounted for about 20% of all male and almost 50% of all female suicides aged 25 years and older; poisoning was a less frequent method of suicide among 15- to 24-year-old males and females (around 10% and 20%, respectively). Over the study period, these proportions manifested no clear trend among either sex (data not shown), with the exception of 25- to 44-year-old males, who registered a slight decrease, and among females 45 years and older, for whom poisoning became a more prevalent method of suicide (50%-60%).
Ratio B: Undetermined Deaths/Suicides
Figure 3 illustrates the ratio of all undetermined intent death classifications (regardless of nature of injury; i.e., drowning, poisoning, firearm) to all suicide death classifications. The male ratio held steady after 2003, whereas the female ratio was higher than that of males and increasing.
Ratio B: all undetermined intent deaths to all suicides, age 15 years and older, by sex, Canada, 2000 to 2011.
Ratio C: Unintentional Poisoning Deaths/Suicides
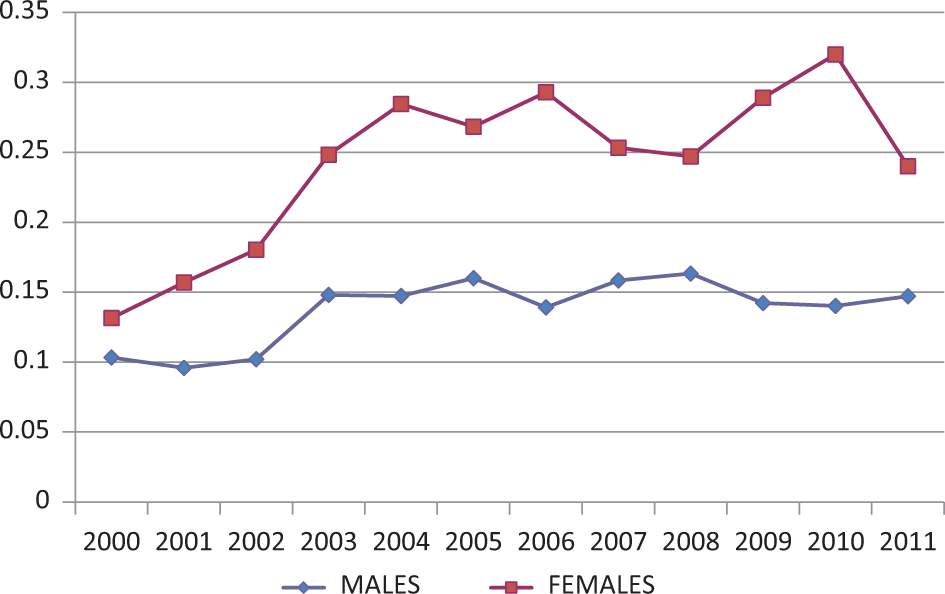
Unintentional poisoning deaths rose in relation to suicides beginning in 2003 (Figure 4) for both sexes, although females were consistently higher.
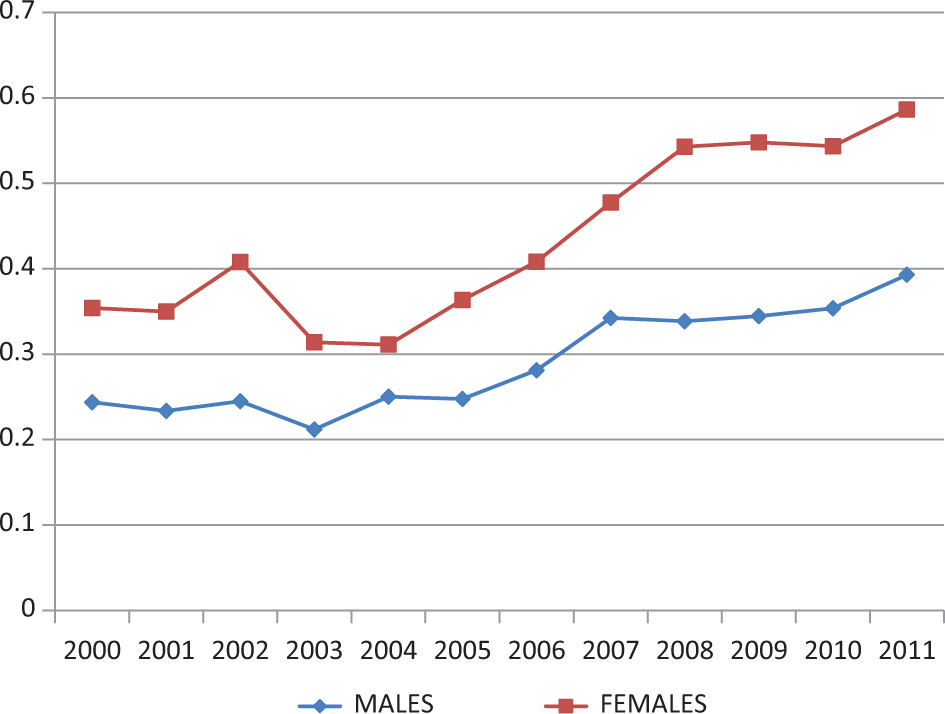
Ratio C: unintentional poisoning deaths to all suicides, 15 years and older, by sex, Canada, 2000 to 2011.
Ratio D: Undetermined Poisoning Deaths/Undetermined Deaths
The proportion of undetermined deaths, attributed to poisoning, increased from 47% in 2000 to 80% in 2011 (both sexes combined), with females demonstrating a consistently higher ratio over the time period. This is a particular burden in the 24- to 64-year age group, among both males (80%) and females (90%) (data not shown).
Discussion
During the 12-year observation period, the overall poisoning mortality rate increased, due in part to steadily increasing unintentional poisoning rates beginning in 2004, as well as to the undetermined poisoning rates, which doubled initially until 2003 and then flattened. Although suicide poisoning mortality rates decreased slightly overall, this held as a primary method among females but was less prevalent among males. Undetermined poisoning deaths have risen to comprise the large majority of undetermined deaths among both sexes, but again, with a higher burden among females overall, and in particular for males and females between 25 and 64 years of age.
Across all poisoning intent categories, drugs and medications (overdoses) were the primary cause of death, but it was solely suicide poisonings where an increasing proportion of drug involvement was observed. Over the same period, the proportion of alcohol-related deaths increased within the unintentional and undetermined poisoning categories. Alcohol and drug abuse are known risk factors for suicide, oftentimes consumed in combination, leading potentially to interactions, disinhibition, and impulsivity. 34 The difficulty in disentangling mixed drug and alcohol cases to identify the primary cause of death is complex 35 –39 and may contribute in some part to this trend.
Canadian research has addressed overall changes during this timeframe in youth suicide rates. 1 The Canadian regulatory warnings on antidepressant prescribing initially in youth (but later expanded to all ages) and the serious implications for youth suicide rates, notably in girls 40 –42 and suicide-related morbidity, were explored. 43,44 However, less attention has been given to changes in poisoning suicide rates among adults and, even more fundamentally, the validity of poisoning rates overall.
C/MEs experience difficulties collecting sufficient evidence to ascertain true intent, particularly in poisoning cases. This is of particular concern in cases where the agents involved (e.g., opioids) may produce a secondary gain (e.g., euphoric effects), whereas the intent of a poisoning death involving carbon monoxide is more readily ascertained. We surmise that this issue primarily affects the validity of suicide and unintentional poisoning deaths and rates, since poisoning homicides are exceedingly rare in Canada. These opposing trends are similar to patterns reported in the United States and England and supports the hypothesis that misclassification of poisoning deaths may also be problematic for Canada. Further research is required to determine the extent to which unintentional poisonings (drug overdoses) are truly increasing and what proportion, if any, are misclassified suicides to improve data reliability. At the extreme limit of possibility, the estimates in this study suggest the proportion of suicides potentially misclassified as undetermined deaths could range from 15% to 25% and from 40% to 60% due to unintentional poisonings in 2011.
The rising use, misuse, and abuse of opioids in North America are well documented, 45 –48 as is the associated suicide risk. 36,38 Distinguishing between an intentional and unintentional overdose can be problematic for C/MEs, particularly in opioid overdose cases. 39,45 Canada was the second largest per capita consumer of prescription opioids in 2013, after the United States. 49 Canadian researchers examined opioid prescribing rates among those receiving social assistance in Ontario, reporting an increase of 16.2% in the annual prescribing rate between 2003 and 2008. They found a direct association between opioid dose and opioid-related mortality. 50
In the United States, opioid misuse has been rising since the 1990s, along with an increase in associated mortality, 51,52 and opioid users are reported to have increased rates of substance use disorders in comparison to nonopioid drug users. 53 Opioid prescription overdose deaths increased by 415% among females and 265% among males between 1999 and 2010. 54 Opioid misuse is a growing issue among women, 55,56 as women are more likely to be prescribed opioids than men, and in higher doses, with a more severe clinical profile. 56,57 Opioid overdose is reported as being involved in 1 out of 10 suicides among women in the United States, 54 but we hypothesize that the true proportion is higher.
It is beyond the scope of this study to claim that the rise in unintentional and undetermined poisonings is due entirely to misclassified suicides or, alternatively, that poisoning suicides are decreasing due to prevention efforts, while accidental overdoses are escalating due to greater access to opioids; the truth, most likely, lies between these 2 extremes. Acceptance that the increase in the unintentional poisoning mortality rate reflects a true rise in accidental drug overdoses would point to an urgent need for prevention that addresses related prescription for pain and possible mood addiction issues, particularly with regards to women. However, if instead the increase is partially a function of suicide misclassification, as found in prior research, 16 –21 then suicide specific prevention strategies, including restricting access to lethal means, 58,59 can be added to the ameliorative mix. Overall, the explanation for the rise may include changes in a complex pathway beginning with substance use, including increased access to drugs, developing into abuse and associated physiological and social consequences, and ending, in some as yet indeterminate number of suicides. 37,39
A high burden of proof is necessary for C/MEs to categorize a death as suicide. 60,61 The subjective and complex nature of investigating and determining intent, particularly in poisoning cases, is made more complicated by the nature of the premorbid emotional/physical state of the individuals in question, who themselves may not be completely aware of their own intent prior to the event 16,30,39,60 or who may experience ambivalence towards death. 24,61,62 When a suicide cannot be definitively declared, the only remaining injury manner-of-death options are unintentional or undetermined. This uncertainty induces underreporting of suicide and overreporting of the other intents. 30 The proportion of deaths subject to autopsy (e.g., may include toxicological and microscopic analysis) in Canada declined from 9.9% in 2000 to 4.8% in 2011 (SC Table 102-0510), further subjecting suicides to misclassification. 6 –8 It is difficult to ascertain if there have been changes over time in the C/ME assessments, as procedures and standards differ by province. No standard protocol is followed.
An international multidisciplinary research team has proposed a new working definition, death from drug self-intoxication (DDSI), to inform users of data from the US Centers for Disease Control and Prevention’s (CDC) National Violent Death Reporting System (NVDRS). Pertinent to poisoning mortality cases, estimated DDSIs comprise all fatal drug self-intoxications whose manner of death was suicide and the great preponderance classified as undetermined or accident. 61 An enhanced category of self-injury mortality, comprising suicides by any method and nonsuicide DDSIs, would represent the 8th leading cause of death in the US versus 10th in the case of suicide alone. 62 Drug use/abuse is a high-risk behaviour that is widely understood to increase the probability of death, leading to difficulties in classifying these cases as accidents, when the complex intent of these deaths may fall along a continuum between purely intentional and unintentional. 63 In Canada, we recommend the inclusion of standardized information by the C/MEs, which would then further enrich the CCMED and inform prevention. 64 We recommend further study and consensus to determine the best approach for Canada.
This study has a number of limitations. As it is a retrospective observational study, it can only describe Canadian trends and suggest potential explanations. Currently, diagnostic codes that detail the specific nature of injury and associated agent or agents for mortality data are unavailable for analysis in Canada and therefore prevent identification of specific drug involvement (i.e., opioid drugs cannot be separated from other types within the X42 category). The administrative data employed provide limited variables and prevent more complex analysis involving potential comorbidities. Unlike the United States, Canada does not yet have a national violent death reporting system that combines multiple data sources, including state and local medical examiner, coroner, law enforcement, crime lab, and vital statistics records, into one surveillance tool. However, the CCMED 15 may be used in the future to help fill this void.
Conclusion
Reliable and valid mortality statistics are essential to public health and clinical medicine. Without this foundation, suicide and other injury surveillance, etiologic research, treatment, rehabilitation, policy, prevention, and evaluation are severely compromised. The findings of this study recommend further research to quantify any potential misclassification and remediate, if necessary, to prevent future error that limits comparability both within Canada, as well as internationally. Consideration should be given in Canada to the need for continual standardized monitoring and analysis of poisoning deaths associated with drugs, across the continuum of decedent intentionality, to enhance prevention and achieve a more accurate accounting of suicide and other self-injury mortality.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.