
Abstract
Objective:
The 2013 Canadian Forces Mental Health Survey (CFMHS) collected detailed information on mental health problems, their impacts, occupational and nonoccupational determinants of mental health, and the use of mental health services from a random sample of 8200 serving personnel. The objective of this article is to provide a firm scientific foundation for understanding and interpreting the CFMHS findings.
Methods:
This narrative review first provides a snapshot of the Canadian Armed Forces (CAF), focusing on 2 key determinants of mental health: the deployment of more than 40,000 personnel in support of the mission in Afghanistan and the extensive renewal of the CAF mental health system. The findings of recent population-based CAF mental health research are reviewed, with a focus on findings from the very similar mental health survey done in 2002. Finally, key aspects of the methods of the 2013 CFMHS are presented.
Results:
The findings of 20 peer-reviewed publications using the 2002 mental health survey data are reviewed, along with those of 25 publications from other major CAF mental health research projects executed over the past decade.
Conclusions:
More than a decade of population-based mental health research in the CAF has provided a detailed picture of its mental health and use of mental health services. This knowledge base and the homology of the 2013 survey with the 2002 CAF survey and general population surveys in 2002 and 2012 will provide an unusual opportunity to use the CFMHS to situate mental health in the CAF in a historical and societal perspective.
Clinical Implications
Clinicians caring for CAF personnel and veterans can draw upon a firm knowledge base to inform their clinical practices.
The CAF’s experience with trauma-related disorders and with mental health services renewal may inform service delivery for all Canadians.
Limitations
This is a narrative review, which may therefore be particularly susceptible to bias.
The 2013 CFMHS will not be able to answer many important questions, particularly those surrounding the performance of specific aspects of the CAF mental health system.
The past 14 years of armed conflict in southwest Asia have focused unprecedented attention on the mental health of military personnel in Western nations. The Canadian Armed Forces (CAF) have had a robust mental research program since the late 1990s, in recognition of the unique needs of its personnel. 1 Many studies have been undertaken, including mental health surveys, 2,3 health services research projects using administrative data, 4 –9 biomedical research looking at the basic mechanisms of health and disease, 10 –15 and clinical research on new approaches to diagnosis and treatment. 16
In mid-2013, Statistics Canada collected survey data from 8200 serving military personnel via the 2013 Canadian Forces Mental Health Survey (CFMHS), 17 with the goal of providing an updated picture of the mental health of the CAF since the time of a similar mental health survey executed in 2002. 2 Understanding the survey findings demands a firm understanding of the context of mental health in the CAF over the past 14 years and of the methods of the survey itself.
The article is intended to serve as a reference document for those less familiar with the CAF context that 1) provides a snapshot of the structure of the CAF today; 2) describes the CAF mental health system and its evolution; 3) describes the deployment experience of CAF personnel, with a focus on the mission in Afghanistan; 4) summarizes the results of the 2002 mental health survey; 5) summarizes other recent population-based mental research findings in the CAF; 6) provides an overview of objectives and methods of the 2013 CFMHS; and 7) identifies key data sources from other populations that serve as points of reference.
We have erred on the side of presenting unpublished findings, where we were sufficiently confident in the underlying methods, where the work had been presented at scientific meetings, and where we felt that the findings contributed to the overall narrative. Consistent with the Canadian Journal of Psychiatry’s editorial standards, these findings have been flagged as an “unpublished observation.” Readers are encouraged to treat these particular findings with caution.
The CAF Today
The mandate of the CAF includes protecting Canada and defending its sovereignty; defending North America in cooperation with the United States, Canada’s closest ally; and contributing to international peace and security through operations around the world, most often in partnership with allies from other countries.
The CAF has 2 components, the Regular (RegF) and Reserve Forces (ResF), which counted 68,000 and 40,000 active personnel, respectively, around the time of the CFMHS. The RegF consists of personnel who have committed to full-time service for a specified period of time. ResF personnel consist of several subcomponents, the largest and most relevant of which is the Primary Reserves, which have similar qualifications as RegF personnel and engage in similar duties and roles but are employed on a part-time and/or noncontinuous basis. Primary ResF personnel may deploy on international operations, although such deployments are essentially voluntary.
The CAF mental health system largely serves RegF personnel. ResF personnel generally access the civilian mental health system, although they may receive CAF treatment during periods of full-time service (e.g., while deployed) or for service-related medical conditions.
The CAF Mental Health System
During the 1990s, significant cuts were made to the CAF and its health services as part of post–Cold War restructuring and deficit reduction efforts. 1 By the year 2000, mental health and most other specialty services had been outsourced to external civilian providers. It quickly became apparent that this approach was not meeting the needs of the many personnel who were coming forward with service-related mental disorders. Weaknesses in other parts of the CAF’s health system had also become manifest.
The Rx2000 project was launched in 2000, with an ultimate goal of reinforcing the Canadian Forces Health Services to better meet the health needs of personnel and the CAF’s need for a fit, capable force. Table 1 provides a summary of some of the most important changes in the CAF mental health system. 1
Key Milestones in the Evolution of the CAF Mental Health System, 1990-2015.
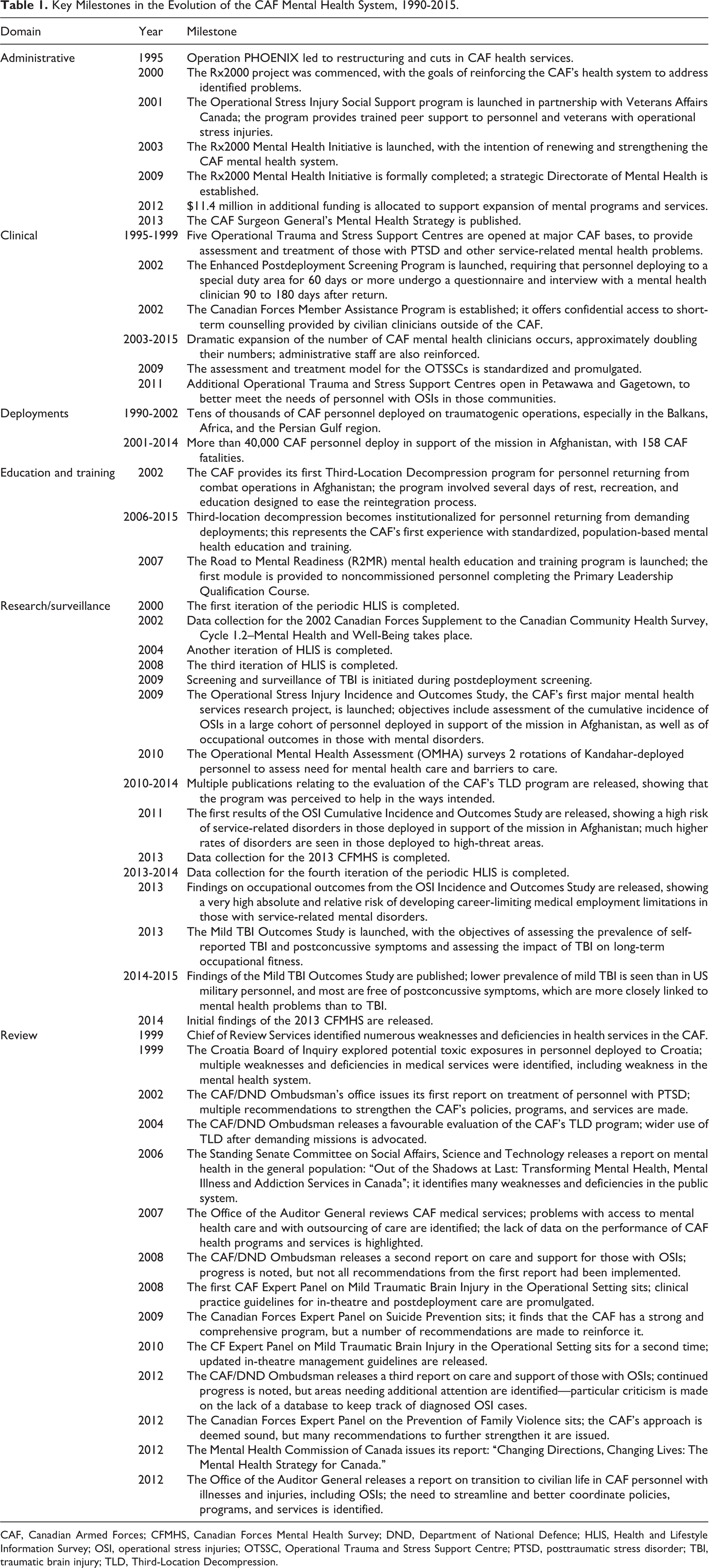
CAF, Canadian Armed Forces; CFMHS, Canadian Forces Mental Health Survey; DND, Department of National Defence; HLIS, Health and Lifestyle Information Survey; OSI, operational stress injuries; OTSSC, Operational Trauma and Stress Support Centre; PTSD, posttraumatic stress disorder; TBI, traumatic brain injury; TLD, Third-Location Decompression.
Today, CAF personnel access a comprehensive mental health system, with coordination and strategic guidance provided by the Directorate of Mental Health. The system has 3 key components: research to advance knowledge in military mental health; education to enhance mental health literacy, change attitudes, and build resilience; and clinical and rehabilitative services for those with identified needs. 1
The Road to Mental Readiness (R2MR) program 18 provides mandatory training to personnel across the deployment cycle and during career progression, while the Strengthening the Forces (StF) health promotion program provides largely elective training to individuals or units. 1
Clinical services encompass mandatory mental health screening (predeployment, postdeployment, and during periodic health evaluations) and clinical mental health care. For clinical services, CAF personnel can access 5 separate clinical programs, including primary care, psychosocial services (an open-access mental health program staffed largely by social workers), 2 referral-based specialty mental health programs (one for those with operational trauma and the other for nonoperational mental health problems), and the Canadian Forces Member Assistance Program (CFMAP). CFMAP is the CAF’s employee assistance program, offering open-access, confidential short-term counselling by outside civilian providers. 1
The CAF’s specialty mental health programs employ a mix of uniformed and civilian psychiatrists, psychologists, social workers, mental health nurses, and chaplains to provide a collaborative approach to care. For operational trauma, the assessment process is standardized nationally as are the evidence-based, trauma-focused treatments that are provided. 1
The CAF and Its Operational Experience
Military operations may involve exposure to traumatic events that can leave a lasting imprint on the mental health of personnel. 5 Hence, an understanding of mental health in the CAF requires an understanding of the operational experience of currently serving personnel.
The Mission in Afghanistan, 2002-2013
Canada’s involvement in the mission in Afghanistan 19 began in October 2001 and officially ended in March 2014. Over the initial period of this mission, covering October 2001 to December 2011, CAF activities were focused on establishing security that was essential to promote the country’s development and to foster an environment that was conducive to the improvement of Afghan life. During this period, the Navy deployed numerous major vessels in and around the Arabian Gulf from 2001 to 2012, with roles that included force protection, fleet support, and maritime interdiction. Army personnel focused on combat and peace support operations in Kabul (2003-2005) and Kandahar Province (in 2002 and 2005-2011), where most of the 158 CAF mission-related fatalities occurred. Air Force personnel contributed strategic/tactical airlift and long-range patrol/surveillance capabilities over the full duration of the mission; most Air Force personnel were stationed in the United Arab Emirates. During the later phase of Canada’s involvement (May 2011 to March 2014), CAF personnel provided training and professional development to the national security forces of Afghanistan, which also included specialized training in fields such as medicine, logistics, signals, and air operations—all largely in Kabul. 19
As of 23 September 2012 (the date the sampling frame was struck for the 2013 survey), 43,680 unique CAF members had deployed in support of the mission in Afghanistan to locations outside of North America or Europe. Of these, 35,311 were still serving on that date (30,454 Regular Force members and 4857 Reserve Force members). By the time of data collection (April to August 2013), 29,060 of the Regular Forces members and 4480 of the Reserve Forces members were still in service and eligible for the survey, based on the sampling weights in the 2013 CFMHS.
Afghanistan-related deployment characteristics in those still serving at the time of the survey are shown in Table 2. Three-quarters had deployed only once, with a typical cumulative duration of deployments of 121 to 240 days. Slightly more than half had deployed to Kandahar only. Only one-third had deployed in support of the mission within the 4 years preceding the survey. About half had had other international deployments over the course of their career.
Summary of Deployment Characteristics for CAF Personnel Who Had an Afghanistan-Related Deployment and Were Still Serving at the Time of the 2013 Canadian Forces Mental Health Survey.a
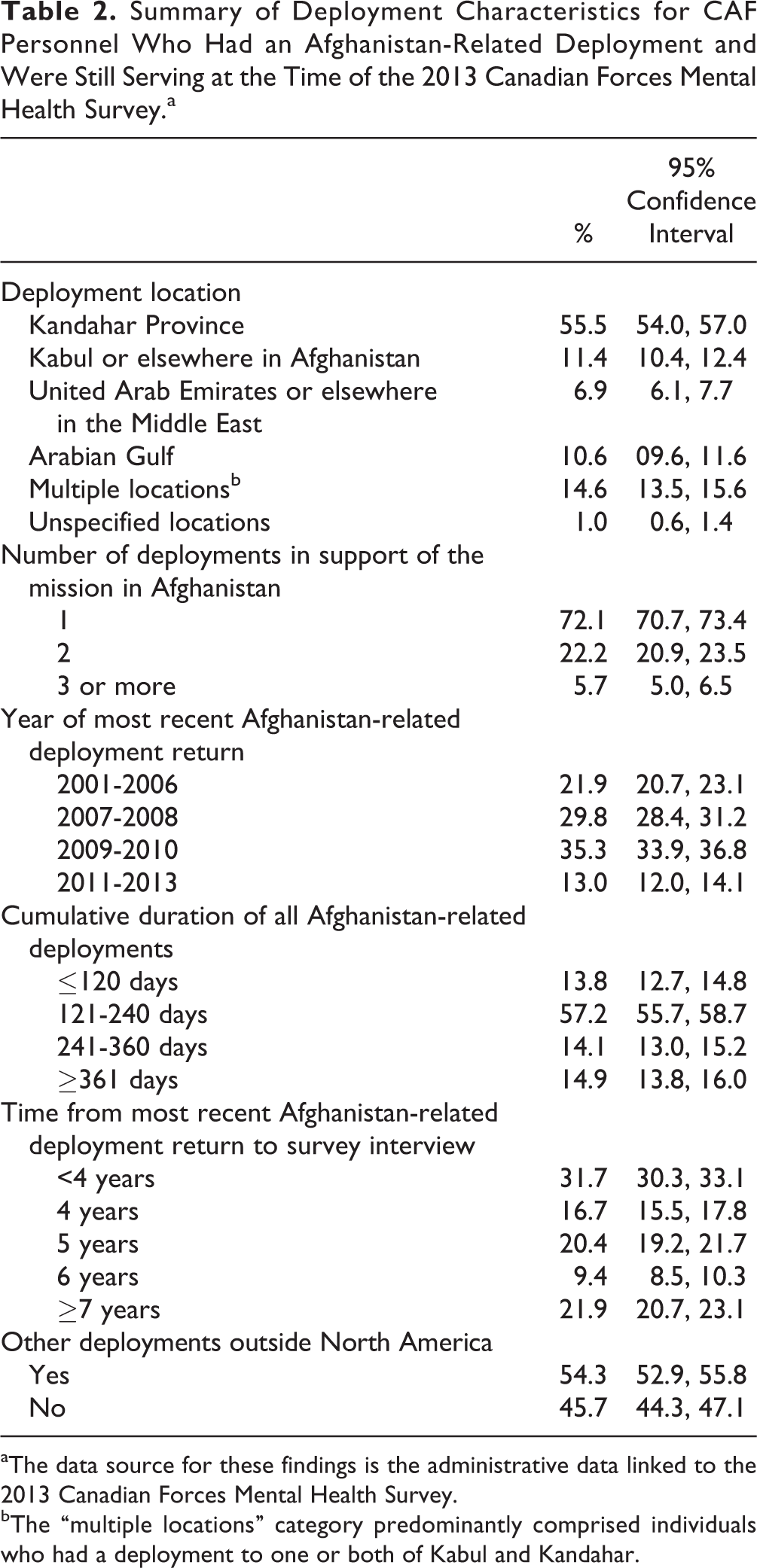
aThe data source for these findings is the administrative data linked to the 2013 Canadian Forces Mental Health Survey.
bThe “multiple locations” category predominantly comprised individuals who had a deployment to one or both of Kabul and Kandahar.
Other Major Operations
Over the period following the Korean War but prior to 2002, the CAF’s involvement in international operations was largely in the form of peacekeeping, peace support, or humanitarian aid to areas experiencing natural or other disasters. CAF personnel have also been deployed domestically, especially for disaster recovery and relief, including floods, forest fires, ice storms, and the crash of Swissair Flight 111. Some of larger international operations took place in Cyprus, the Persian Gulf region, the former Yugoslavia, Cambodia, Somalia, Uganda, Rwanda, Haiti, and East Timor.
While Afghanistan-related North Atlantic Treaty Organization (NATO) deployments predominated starting in 2002, thousands of personnel also deployed on United Nations missions over the same period, including contributions to security and stability in Haiti, assisting with the implementation of a peace agreement in Sierra Leone as well as the establishment of its armed forces, supporting the implementation of a peace agreement in Sudan, peacekeeping in the Nigeria and Cameroon region, providing humanitarian aid in Liberia, peacekeeping assistance in the Democratic Republic of Congo, peacekeeping in Ethiopia and Eritrea, assisting with the formation of institutions for a representative government in Iraq, and peacekeeping between Israeli and Syrian forces in the Golan Heights area. As a member of NATO, the CAF has also participated in the response to the rebellion in Libya and the NATO mission to protect noncombatants during the conflicts in the former Republic of Yugoslavia and later in a peacekeeping role in Bosnia-Herzegovina. Humanitarian assistance has been provided in response to earthquakes in Pakistan and Haiti, a tsunami affecting Sri Lanka, tropical cyclones in Haiti and the Philippines, and a need for departure assistance for Canadians in Lebanon during the outbreak of armed conflict.
The 2002 Mental Health Survey
The Canadian Forces Supplement to the Canadian Community Health Survey, Cycle 1.2–Mental Health and Well-Being (CCHS-CFS) was a population-based survey of serving Canadian military personnel conducted by Statistics Canada in 2002. 2 It was the first large-scale assessment of mental health in the CAF. Data collection occurred concurrently with a very similar mental health survey of Canadians in the general population.
The survey used a stratified random sample of currently serving RegF and ResF personnel (n = 5155 and 3286; response rate: 79.5% and 83.5%, respectively). 2 Consenting participants completed a computer-assisted personal interview with Statistics Canada personnel. The World Health Organization Composite International Diagnostic Interview 20 (CIDI) version 2.1 was used to assess mental disorders. Other modules examined the impact of mental health issues, risk and resilience factors, and services use. A full listing of the modules in the survey is provided in Table 3.
Comparison of Survey Content of the 2002 and 2013 Canadian Forces Mental Health Surveys and of the 2012 Canadian Community Health Survey–Mental Health and Well-Being.
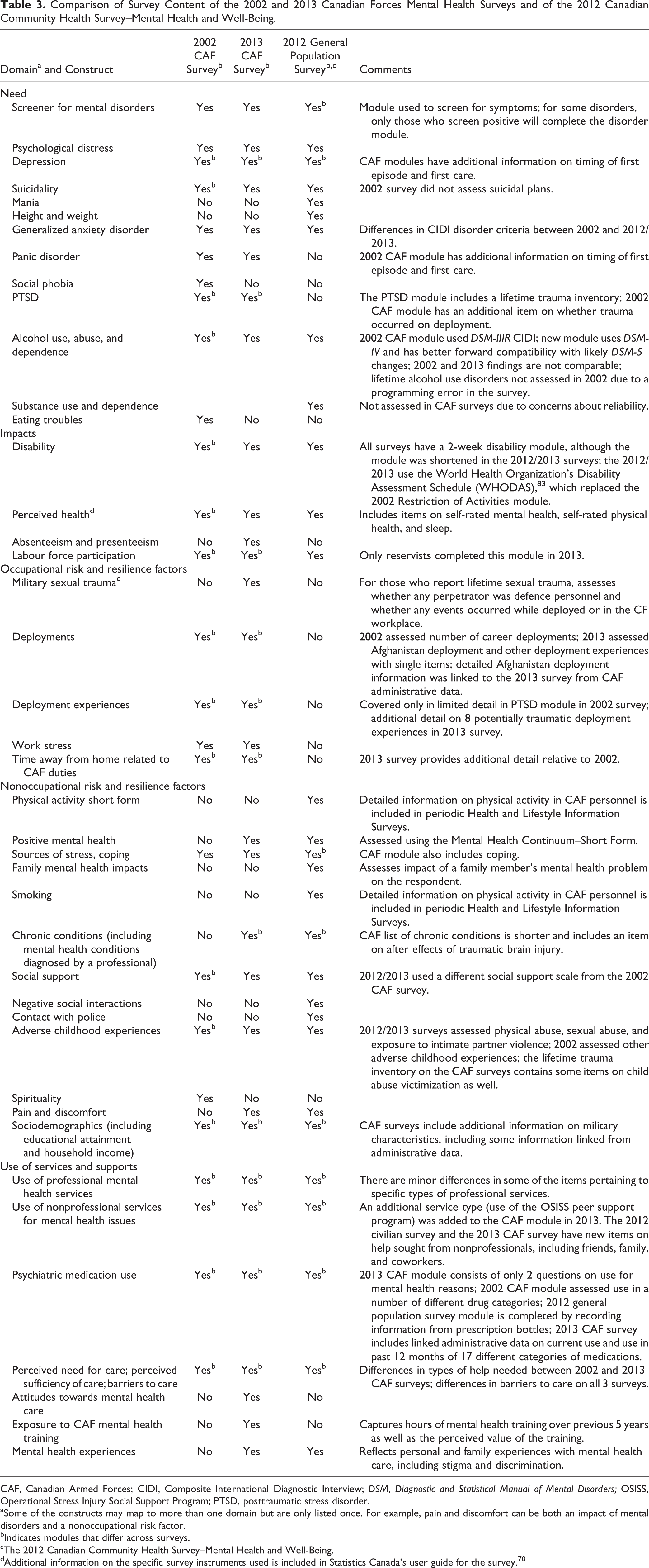
CAF, Canadian Armed Forces; CIDI, Composite International Diagnostic Interview; DSM, Diagnostic and Statistical Manual of Mental Disorders; OSISS, Operational Stress Injury Social Support Program; PTSD, posttraumatic stress disorder.
aSome of the constructs may map to more than one domain but are only listed once. For example, pain and discomfort can be both an impact of mental disorders and a nonoccupational risk factor.
bIndicates modules that differ across surveys.
cThe 2012 Canadian Community Health Survey–Mental Health and Well-Being.
dAdditional information on the specific survey instruments used is included in Statistics Canada’s user guide for the survey. 70
Key Findings
The first peer-reviewed publication of the survey findings emerged in 2006 21 —4 years after data collection occurred. Since that time, a total of 20 peer-reviewed publications have used the survey data.
Disorder Prevalence and Other Indictors of Need
Among lifetime mental disorders in the RegF and ResF combined, major depressive episode (MDE) had the highest prevalence at 14.9%, followed by social phobia (8.2%), posttraumatic stress disorder (PTSD) (6.5%), generalized anxiety disorder (GAD) (4.4%), and panic disorder (3.3%). 22 Of the RegF, 15.1% had 1 or more of the 6 past-year disorders covered in the survey. 2 The most prevalent past-year disorder in RegF personnel was depression (7.6%); past-year PTSD occurred in 2.7%. 23 The 12-month prevalence of any past-year mood or anxiety disorder was lower among ResF members (12.7%). 23 Alcohol dependence was the most commonly reported disorder among ResF members (6.2%). 2 With the exception of alcohol dependence, the prevalence of past-year disorders was lower in ResF than RegF personnel. 2
The most striking difference between the military and the age-sex matched general population was a much higher prevalence of past-year depression in RegF personnel (7.6% vs. 4.3%). 2,24 However, the clinical characteristics of depression were remarkably similar (Erickson J, Kinley DJ, Bolton J, Enns M, Zamorski MA, Sareen J, 2013, unpublished observation). Past-year panic disorder was also slightly more prevalent in the RegF relative to civilians (2.2% vs. 1.4%). 2,24 No other military–general population differences were seen in the disorders assessed by both surveys or in suicidal ideation. 25 However, military personnel had lower rates of past-year suicide attempts relative to the general population. 25 Neither lifetime trauma exposure nor PTSD was assessed on the general population survey, precluding comparison of prevalence rates.
Sareen et al. 26 proposed a broader conceptualization of “need,” beyond simply meeting diagnostic criteria for a disorder. By also including a past-year perceived need for care or use of mental health services, they found that almost one-third of personnel met this expanded definition. 26
Impacts
Few studies using the 2002 Canadian Forces Supplement data have examined the impact of mental disorders. Expected impairments were seen in functional status in personnel with depression (Erickson J et al., 2013, unpublished observation), social phobia, 27 and GAD. 28
Occupational Risk and Resilience Factors
Combat, peacekeeping, and exposure to atrocities were associated with a number of past-year mental health outcomes. 26,29 However, occupational trauma accounted for only a small fraction of the overall burden of past-year disorders (9% in men, 6% in women) 30 and none of the burden of suicidal ideation 29 ; only PTSD had a substantial population attributable fraction (PAF) for combat or peacekeeping (46% in men, 24% in women). 30
Nonoccupational Risk and Resilience Factors
Adverse childhood experiences showed a higher overall PAF than military experiences for any adult-onset mood and/or anxiety disorder: 16.4% for men and 19.5% for women. 29 Nelson et al. 31 found a dose-response relationship of number of lifetime traumatic events and adverse mental health outcomes (past-year PTSD, depression, suicidal ideation); depression mediated the relationship between the number of lifetime traumatic events and past-year suicidal ideation. 31 Mota et al. 32 also noted the association between occupational and nonoccupational trauma and suicidality. Finally, Mota et al. 33 found that social support was protective against mental health problems for both male and female military members. Active coping was also somewhat protective for certain disorders in men. 33
Use of Services and Supports
Fikretoglu et al. 34 found that 11.2% saw a mental or medical health professional in the year prior to the survey; 42.6% of those with a past-year disorder had received such services, 23 although this was higher for certain disorders, such as panic disorder at 74.5%. 35 Most of those who had sought care over the previous year had had 5 or fewer visits. 34
Sareen et al. 36 found that, after adjusting for mental disorders, perceived need for care was associated with many factors, including deployment, exposure to combat and witnessing atrocities, and long-term restriction in activities. Further analyses of service use have suggested that virtually all individuals with a lifetime disorder will eventually make contact for treatment. 22 However, the estimated median duration of delay ranged between 3 and 26 years, depending on the disorder. 22 In particular, the median delay for PTSD was found to be 7 years. 22
The leading contributor to not seeking care for a mental disorder was failure to recognize an unmet need for care, seen in 84.0% to 96.5% of those with a disorder. 23 The most commonly reported barrier (among those who did articulate an unmet need for care) was ambiguous (“lack of trust in military health, administration or social services”), endorsed by about half of the respondents, followed by “other reasons.” 23,26 Surprisingly, perceived stigma (“afraid of what others might think”) was not commonly endorsed by respondents as a barrier to care. 23,26 RegF personnel were more likely than those in the general population to have sought care for mental health problems (Mota NP, Mota N, Klassen K, Fikretoglu D, Zamorski MA, Sareen J, 2013, unpublished observation; Fikretoglu, Liu A, Zamorski MA, Jetly R, 2015, unpublished observation).
Fikretoglu et al. 23 found past-year mental health service use to be higher in females (20.3%) than males (11.5%). Seeking treatment for PTSD was associated with the type of traumatic event and cumulative lifetime trauma exposure; the likelihood of seeking treatment was higher following exposure to multiple types of trauma. 21,37
Psychiatric need variables were consistently related to service use likelihood and intensity. 34 However, a significant proportion of contacts for both mental health and medical providers were initiated by those without a mental disorder in the past year, suggesting that meeting diagnostic criteria for a mental disorder is not a perfect measure of need for services. 34
Miscellaneous Findings
Delayed-onset PTSD was found to be relatively rare (overall prevalence <1%; 8.5% of lifetime PTSD was delayed-onset). 38 Other studies have focused on issues such as medication use in those with depression 39 and service use among particular subgroups of personnel. 27 One study identified some gender-specific differences in the symptom profile of depression in CAF personnel and other Canadians. 40 Finally, Park 41 completed an extensive analysis of the mental health of CAF personnel, including many comparisons with Canadians in the general population.
Limitations
There have been many changes to the CAF since 2002, including many Afghanistan-related deployments and the reinforcement of the CAF mental health system. Thus, the primary limitation of the 2002 survey is that the findings are likely no longer an accurate assessment of mental health in the CAF. A second key limitation is that it only captured serving personnel and therefore cannot provide a complete picture of the impact of military service across the life course; recent veteran surveys, however, have helped fill this gap. 42,43 A final key set of limitations are those inherent in any cross-sectional mental health survey.
Key Findings of Other CAF Population-Based Mental Health Research Projects
Operational Stress Injury Incidence and Outcomes Study
Limitations in the existing data on the mental health impact of the mission in Afghanistan 4,19 led to this cohort study of personnel who deployed over the period during 2001 to 2008. 5 Mental disorder diagnoses were assessed via medical records for a random sample of more than 2000 individuals. Of the cohort, 19.0% had a mental disorder diagnosis over a median postdeployment follow-up of 3.7 years; 13.5% had a mental disorder that was attributed to an Afghanistan deployment by a CAF clinician. 5 PTSD was the most prevalent Afghanistan deployment-related condition, affecting 8% of the cohort. 5 Significantly higher cumulative incidence was seen after more prolonged follow-up, with close to 20% being diagnosed with an Afghanistan deployment-related disorder within 7 years of their return. 5 Independent risk factors for mental disorders included deployment to higher-threat locations (i.e., Kandahar, for which the cumulative incidence approached 30% towards the end of the follow-up period), service in the Army, and lower rank. 5
Individuals with an Afghanistan deployment-related mental disorder had a high absolute and relative risk of adverse military occupational outcome relative to those without a mental disorder diagnosis, while those with other mental disorders had an intermediate risk. 6 Additional analyses showed that delay to care had decreased over time and that shorter delays to care were associated with more favourable occupational outcomes. 7 As well, it was noted that occupational outcomes were better for those diagnosed more recently. 7
Operational Mental Health Assessment
The Operational Mental Health Assessment (OMHA) was a cross-sectional prevalence survey of CAF personnel deployed to Kandahar that was conducted in-theatre. 3 While 8.5% exceeded conventional screening thresholds for symptoms of acute traumatic stress, major depression, or generalized anxiety, only 26% of those with these problems were interested in getting help. 3 However, mental health–related occupational impairment was primarily seen in those with subthreshold mental health symptoms. 3
Perceived structural barriers to care were, as expected, greater in more isolated locations. 44 Stigma surprisingly showed no association with care-seeking propensity, while other negative attitudes toward care (e.g., that it was ineffective) did have the expected negative association. 44 A separate analysis validated the K10 distress scale in the operational environment. 45
Mild Traumatic Brain Injury Outcomes Study
This population-based study on CAF members deployed in support of the mission in Afghanistan found that 5.2% self-reported mild traumatic brain injury (MTBI) while deployed, a rate well below similar US studies. 8 Most were no longer symptomatic in the postdeployment period. The strongest predictor of persistent postconcussive symptoms was mental health problems as opposed to MTBI. 8
MTBI proved to be associated with an increased risk of career-limiting medical employment limitations compared with those with no MTBI (adjusted hazard ratio = 1.64), but clinicians attributed these limitations largely to either mental health problems or musculoskeletal conditions and not to neurologic disorders (Garber BG, Rusu C, Zamorski MA, Boulos D, 2014, unpublished observation). This finding further emphasizes the importance of mental health problems as a determinant of outcomes in those with MTBI.
Miscellaneous Studies and Reviews
A series of studies on the CAF’s Third-Location Decompression (TLD) program in Cyprus showed that the program was well received and was perceived to have had the intended effects on easing the reintegration process after return from a combat deployment. 46 The educational program was a major contributor to the program’s perceived value, 47 and a later revision to the program was associated with significantly better short-term outcomes. 48,49 The TLD data were also used in a cross-national comparison of stigma and barriers to care, showing lower rates in the CAF than in its allies in the United States, the United Kingdom, Australia, or New Zealand. 50 Several studies have exploited data collected as part of the Recruit Health Questionnaire, a routine survey administered to CAF recruits since 2003. Key studies include the validation of a higher-order model of resilience, 51 prospective validation of resilience by linkage of the Recruit Health Questionnaire to postdeployment screening data 52 and to administrative data on attrition, 53 exploration of the role of premilitary mental health on postconcussive symptoms, 54 and a longitudinal evaluation of the stability of resilience. 55
The CAF has executed 4 periodic Health and Lifestyle Information Surveys (HLIS) since 2000. 56 –58 These surveys have basic content on mental health, determinants of mental health, and use of mental health services. There has been a single peer-reviewed publication using HLIS data to explore the role of mental health in intimate partner violence in CAF families. 59 Periodic reports on suicide surveillance have been issued. 60,61 Finally, the CAF, Veterans Affairs Canada, and Statistics Canada completed a record linkage study on mortality of a large cohort of personnel with military service. 62 The analysis showed no elevated risk for suicide in the cohort, relative to other Canadians. 62 However, there was an elevated risk of suicide in male personnel after their release from the CAF (standardized mortality ratio = 1.46). 62
Several recent reviews capture the CAF’s approach to suicide prevention, 63 the mental health impact of the mission in Afghanistan, 19 an evidence-based assessment of mental health in the CAF, 64 and key research on need, stigma, and barriers to care. 65
Synthesis of Research Findings
The past dozen years of mental health research have provided a clear and detailed picture of the mental health of CAF personnel. The most consistent finding is that in any given year, most CAF personnel are in good mental health, but there is always an important minority who could benefit from additional services or supports, including but not limited to clinical mental health services. Mental disorders are associated with significant impacts for the member and for the CAF as an organization. 6 Distress or perceived psychosocial problems in the absence of mental disorder also have significant impacts on occupational functioning, 3 highlighting the need to broaden our conceptualization of “need for help” to include those individuals as well as those with diagnosable disorders in our prevention and control efforts. 65 The 2002 CCHS-CFS showed a surprisingly small contribution of occupational trauma to the burden of mental illness. 30 More recent research suggests a larger contribution, 5,66 presumably as a result of the mission in Afghanistan.
In 2002 at least, there was a significant “need-care gap” in that only a minority of personnel with past-year disorders had sought professional mental health care, 23,26 and the intensity of services use was low. 34 Significant delays to first care were seen in 2002, although more recent findings suggest that delays may be falling, at least for those with service-related disorders. 7 A broad range of barriers to care is seen, with the failure to recognize an unmet need for care being, by far, the most prevalent barrier, 23 a phenomenon that also applies to Canadians in the general population. 67 Among those with a perceived unmet need for care, lack of confidence in the CAF’s system was the most prevalent barrier, as opposed to stigma. 23
These research findings have shaped the renewal of the CAF’s mental health system and its mental health strategy. 1 Recognition of the lower than expected contribution of operations to the burden of mental disorders (in 2002, at least) and the greater prevalence of depression than PTSD served to broaden the CAF’s focus on mental health beyond service-related PTSD. That only a minority of those with past-year disorders had sought care and that long delays to care were the norm drove reinforcements in the clinical mental health capacity and other efforts to overcome barriers to care. The broad range of barriers to care (and the lower than anticipated prominence of stigma as a barrier) inspired greater attention to the full range of barriers to care in mass communications and in mental health education and training. Finally, the prominence of failure to recognize a need for care in the face of a disorder led to efforts to reinforce that aspect of mental health literacy.
The 2013 CAF Mental Health Survey
Objectives
The objectives of the 2013 survey flowed naturally from the foregoing circumstances and research findings. Specifically, it sought to understand how mental health and the use of mental health services had evolved in the CAF since 2002, with a focus on the effects of the mission in Afghanistan and on the renewal of the CAF mental health system.
Conceptual Framework
The primary conceptual framework for the survey was Adler and Castro’s “Occupational Mental Health Model for the Military.” 68 The model is intended to provide “a framework for understanding the relationship between occupationally relevant demands and subsequent mental health adjustment, taking into account individual and organizational resources that can mitigate the impact of those demands.” 68 It highlights determinants of mental health that are especially important in military organizations, such as occupational trauma, military culture, leadership, morale, and unit cohesion. It also identifies the full range of targets for interventions to mitigate mental disorders and improve mental health, again focusing on those that the military has leveraged more than most other employers, such as mental health screening, universal resilience training, and delivery of clinical mental health services. Finally, it highlights outcomes that are especially relevant to the military, including operational readiness, performance, and attrition.
Methods
This section summarizes the most important methodological details for those trying to understand the survey findings; researchers wishing to the use the data will find more detailed documentation on Statistics Canada’s website. 69
Content
The survey contains 32 modules, many of which overlap with modules in the 2002 CAF survey and the 2012 civilian surveys (Table 3). As with the 2002 survey, the centre of gravity of the survey is the reliable assessment of common past-year and lifetime mental disorders using the CIDI, version 3.0. 17 The survey modules map to 1 or more of 5 domains, including 1) need (e.g., mental disorders, psychologic distress), 2) impacts (e.g., disability, absenteeism, presenteeism), 3) occupational risk and resilience factors (e.g., exposure to deployment-related trauma, time away from home), 4) nonoccupational risk and resilience factors (e.g., positive mental health, social support, chronic physical health problems), and 5) use of services and supports (e.g., use of clinical mental health services, barriers to care, exposure to resilience training).
Sample
The target population for the survey was 1) serving CAF Primary Reserve Force personnel who had deployed in support of the mission in Afghanistan (n = 4578) and 2) serving CAF Regular Force personnel (n = 67,776, of whom 30,454 had deployed in support of the mission in Afghanistan). The decision to exclude veterans and Reserve Force personnel who had not deployed in support of the mission in Afghanistan was driven by the primary survey objectives and by the availability of other survey data in those populations. The sample frame was established via a query of the CAF’s Human Resources Information System in September 2012. Afghanistan mission deployment status was determined using cross-validated data from several complementary administrative data sources. The frame was divided into 9 strata based on component (RegF or ResF), 3 rank categories, and Afghanistan mission deployment status (for RegF personnel only, as only Afghanistan mission–deployed ResF personnel were included).
Data Collection
Data collection took place between April and August 2013, between 7 and 11 months after the frame was struck. This delay was due to the need to prepare the sample for stratification and to verify contact information. Potential respondents first received a letter in the mail describing the survey and indicating that they had been randomly selected for it. Interviewers were trained Statistics Canada personnel who had substantial experience in administrating household surveys, including the 2012 Canadian Community Health Survey–Mental Health and Well-Being. Standard Statistics Canada data collection quality control procedures were followed. Statistics Canada personnel telephoned potential respondents in their workplace or, if unsuccessful, at their home to recruit them for the survey. The CAF provided contact tracing assistance when required. Statistics Canada procedures for contacting potential respondents and minimizing nonresponse were followed. Respondents were surveyed face-to-face by Statistics Canada personnel using a computer-assisted personal interview. Interviews took place in a private room in the workplace or in another private location if requested by the respondent.
Response Rate
In total, 6996 Regular Force and 1469 Reserve Force personnel responded, yielding final response rates of 79.6% and 78.8%, respectively, after exclusion of out-of-scope respondents. 70 Stratum-specific response rates were highly consistent, ranging from 76.0% to 81.4%. 70 The leading reasons for being out of scope were 1) being out of country or in remote areas during the entire data collection period (7.6% of sample) and 2) release from the CAF in the period between the date the frame was struck and the data collection period (3.7% of sample). For ResF personnel, the leading reasons were release from the CAF before the collection period (11.2% of the sample, reflecting the high expected turnover in the ResF) and 2) being out of country or in remote areas during the data collection period (7.6% of sample).
The primary reasons for being out of country for the duration of the survey were out-of-country postings (prolonged placements in a foreign country, generally along with family members) and deployments (shorter placements in operational settings, without family members). Personnel selected for remote locations, for postings, and for deployments must complete psychosocial screening, meaning that their mental health at the time of their selection was likely better than average, consistent with the well-known “healthy warrior effect.” 71 In the RegF, a substantial fraction of releases are for medical reasons, and mental disorders contribute heavily to those medical releases, 6 meaning that the mental health of released personnel is presumably poorer than those who remain in service. In contrast, in ResF personnel, nearly all releases are voluntary. The net effect of these complex factors on the survey findings in ResF and RegF personnel is unfortunately unclear.
Weighting
Statistics Canada calculated the final weight for each case, which reflected the initial sampling weight, removal of out-of-scope units, and adjustment for person nonresponse. Statistics Canada also created replicate weights for 500 bootstrap samples, to be used for variance calculations.
Data Linkage
Respondents provided consent to link survey data with certain CAF administrative data; all linkages were deterministic, using the participant’s unique Service Number. Key characteristics of deployments in support of the mission in Afghanistan were captured through careful cross-validation of several CAF data sources. Data are provided on the month and year of each deployment, the primary deployment location, and the number of days deployed. The number of days deployed was randomly perturbed to minimize the risk of identification of a participant. Unfortunately, similarly detailed data on other career deployments were not available for linkage. Data on psychiatric medication use in 17 classes were extracted from the CAF pharmacy data system, which captures medications dispensed or paid for by the CAF. RegF personnel can receive medications through other means (e.g., private pay, using a spouse’s insurance), although it is not known how frequently this occurs. ResF largely receive medications outside of the CAF system, making their pharmacy data incomplete.
Microdata Access
The survey microdata may be accessed only via Statistics Canada’s Research Data Centres nationwide; there is no public-use microdata file for this survey. Information on submitting analysis proposals and arranging data access can be found on the Statistics Canada website. 72
Ethical Aspects
Ethical aspects of the survey methods and data access were approved by the relevant bodies within Statistics Canada, which serve the function of the Research Ethics Board for its projects. Participation was voluntary, and all respondents provided informed consent.
Coordination of Analysis Efforts
A team of at least 35 government researchers and academic collaborators has started to execute a coordinated analysis plan and to disseminate peer-reviewed publications. Researchers are encouraged to contact the lead author to prevent duplication of analysis efforts and to harmonize methods to maximize comparability of results.
Points of Comparison
A number of other recent data sources can be used as points of comparison to place findings from the 2013 CFMHS in perspective. For example, is a particular prevalence rate higher or lower than expected? The 2013 CFMHS data may be merged with other highly comparable Statistics Canada survey data, including the 2002 CFMHS, 73 the 2002 74 and 2012 mental health surveys done in Canadian civilians, 75 and 2 recent health surveys of recent veterans. 42,43 These provide a unique opportunity to place military mental health in a historical, societal, and life course perspective.
Few comparable population-based military mental health surveys exist elsewhere. The 2010 Australian Defence Force (ADF) Mental Health and Well-Being Study assessed past-year and lifetime disorders with the same instrument used in the 2013 CAF survey (the CIDI 3.0), and it used methods that facilitated comparability with a general population survey in 2007. 76 The ADF study used a 2-stage process for sample selection: a paper-and-pencil screening questionnaire of the entire study population followed by an in-depth interview survey for randomly selected respondents. 77 The final response rate for the survey was unfortunately disappointing (49% for stage 1 and 49% for stage 2, for a final response rate of 24%). 77
The US Army has launched a large-scale, multicomponent mental health research project entitled the Study to Assess Risk and Resilience in Servicemembers (Army STARRS). 78 Two of the component studies (the All Army Survey and the New Soldier Survey) involve paper-and-pencil mental health surveys that have seen excellent response rates. 79 The instruments used for assessment of mental disorders were brief, but there are ongoing efforts to validate their results against clinical interviews. 80 However, differences in the survey population (Army only, with a different age distribution than the CAF), the survey mode, and the survey instruments will constrain direct comparisons with the results of the CAF mental health surveys.
The US Millennium Cohort Study is a large, 25-year longitudinal study of serving personnel and veterans. 81 Participants complete mental health surveys every 3 years, and released personnel (veterans) also complete the surveys. 82 However, that study has had a relatively low participation rate (36%) 82 and a different survey administration approach (paper and pencil or online questionnaire), and it used instruments that are not comparable to those used in the CAF survey.
Veterans Affairs Canada has sponsored 2 large population-based health surveys of CAF veterans released within the previous 15 years: the 2010 Survey on Transition to Civilian Life 43 (STCL, pronounced “stickle”) and the 2013 Life After Service Survey 42 (LASS, pronounced “lass”). Data were collected by Statistics Canada with solid response rates. However, the data were collected by telephone instead of in person, and the mental health problems were not assessed with the detailed CIDI modules used by the CAF in its surveys, precluding direct comparison of prevalence rates. There were, however, 3 mental health measures common to both surveys: 1) assessment of self-reported, diagnosed mental disorders; 2) self-rated mental health; and 3) the K10 psychological distress score.
Conclusion
Mental health in a population is deeply rooted in its particular context, which evolves over time. For the CAF, the deployment of many personnel in support of the mission in Afghanistan and the renewal of its mental health system are key features of the mental health landscape, ones expected to leave an imprint on the mental health of CAF personnel. This article provided a view of that landscape as assessed in the first CAF Mental Health Survey in 2002 and again, albeit in more limited ways in other research studies, at other points in the past decade. This article also described the many significant changes in the CAF landscape needed to understand the evolution of mental health and mental health services use since 2002.
The civilian landscape has also evolved since 2002. The highly comparable civilian data from 2002 and 2012 will demonstrate the effects of that evolution and will provide welcome context to the CAF findings over the same period. Recent veteran survey data provide a glimpse into the lasting imprint of military service on mental health over the life course.
Despite this unprecedented richness in mental health survey data, changes in the prevalence of mental disorders and use of mental health services in the CAF represent the net effect of all of the determinants of mental health over the past decade, including negative ones (traumatic deployment experiences in Afghanistan-deployed personnel) and positive ones (the renewal of the CAF mental health system). While many of these determinants were well assessed by the survey, teasing apart the relative contribution of each will prove difficult, and it will not be accomplished via a single study.
A second key challenge in the interpretation of the survey results is that the changes in the CAF mental health system have been multiple. Use of mental health services, perceived need for care, and the extent to which needs have been met represent the net effect of these changes, most of which have been evolutionary. Many of those changes (e.g., increased use of evidence-based psychotherapy for PTSD) were not captured in the survey data, which will make any observed changes in service use parameters difficult to interpret. In particular, assessments of the quality of care provided and of treatment outcomes using the study data will be limited in their scope and reliability. Those important questions will need to be addressed by other studies using different methods.
Footnotes
Authors’ Note
The opinions expressed in this article are those of the authors and do not represent the official policy or position of the Canadian Armed Forces, the Department of National Defence, or the Government of Canada. A version of this article was presented as a podium presentation at the Military and Veteran Health Research Forum in Toronto, Ontario, 2014 November 24 to 26.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support for this article was provided by the Department of National Defence, which provided salary support to some of the authors.