
Abstract
Objective:
Military personnel in Canada and elsewhere have been found to have higher rates of certain mental disorders relative to their corresponding general populations. However, published Canadian data have only adjusted for age and sex differences between the populations. Additional differences in the sociodemographic composition, labour force characteristics, and childhood trauma exposure in the populations could be driving these prevalence differences. Our objective is to compare the prevalence of past-year mental disorders and suicidal behaviours in the Canadian Armed Forces Regular Force with the rates in a representative, matched sample of Canadians in the general population (CGP).
Methods:
Data sources were the 2013 Canadian Forces Mental Health Survey and the 2012 Canadian Community Health Survey–Mental Health. CGP sample was restricted to match the age range, employment status, and history of chronic conditions of Regular Force personnel. An iterative proportional fitting method was used to approximate the marginal distribution of sociodemographic and childhood trauma variables in both samples.
Results:
Relative to the matched CGP, Regular Force personnel had significantly higher rates of past-year major depressive episode, generalized anxiety disorder, and suicide ideation. However, lower rates of alcohol use disorder were seen in Regular Force personnel relative to the matched CGP sample.
Conclusions:
Factors other than differences in sociodemographic composition and history of childhood trauma account for the excess burden of mental disorders and suicidal behaviours in the Canadian Armed Forces. Explanations to explore in future research include occupational trauma, selection effects, and differences in the context of administration of the 2 surveys.
Clinical Implications
The Canadian Armed Forces’ mental health system must be scaled to address the excess burden of mental disorders. Research to understand this excess burden should target occupational trauma exposure, selection effects, and survey context as explanations.
Limitations
Trauma exposure and posttraumatic stress disorder were not assessed in the general population mental health survey. The comparison could only match the populations on the basis of factors measured in both surveys.
Mental disorders and suicidal behaviours are prevalent and impactful in military
1
–6
and civilian
6
–8
populations. In 2002, there were differences in past-year mental disorder prevalence between Regular Force military personnel and Canadians in the general population (CGP), the most notable of which were a significantly increased risk of past-year depression
9
and a lower risk of past-year suicide attempts.
6
However, much has changed in the Canadian Armed Forces (CAF) since 2002, including the deployment of more than 40 000 personnel in support of the mission in Afghanistan.
10
This mission has exposed many personnel to traumatic events with potential mental health effects.
2
–4,11
Concurrently, the CAF strengthened its mental health system to better meet the needs of its personnel. Preliminary analysis of survey data from 2013 showed substantially higher prevalence of major depressive episode (MDE), generalized anxiety disorder (GAD), and alcohol use disorders in Regular Force personnel than in the CGP.
12
Understanding the health effects of military service through comparisons of military and general populations requires truly comparable nonmilitary samples. CAF personnel have a distinct sociodemographic composition, and they are a distinct part of the labour force. 9 CAF personnel are predominantly male and younger than the general population, 12 and Regular Force personnel are reasonably well remunerated and employed full-time. 9 They must meet health and fitness standards at recruitment and maintain these during service. However, past comparative analyses of the CAF population have largely adjusted only for age and sex. 13 Most international studies have also shown higher prevalence of mental disorders in military populations relative to their corresponding general population, but none have used highly comparable survey data. 14 –16 Moreover, none have accounted for past child abuse victimization, which contributes heavily to mental disorders and suicide 17,18 and appears to be more prevalent in military personnel compared with civilians. 19 Finally, findings from other nations may not apply to the CAF. 4
The objective of this study is to compare the prevalence of past-year mental disorders and suicidal behaviours in CAF Regular Force personnel with sociodemographically comparable individuals in the CGP.
Methods
Populations and Samples
Data sources were the 2013 Canadian Forces Mental Health Survey (CFMHS) 20 and the 2012 Canadian Community Health Survey–Mental Health (CCHS-MH). 21 Both surveys adopted a sampling framework to ensure the representativeness of the samples. The data were collected face to face by Statistics Canada interviewers using a computer-assisted personal interview (CAPI) method. 20,21
For this analysis, the military sample consisted of serving CAF Regular Force personnel (n = 6696, response rate = 79.8%). 20 The general population sample consisted of noninstitutionalized individuals aged 15 years and older living in private dwellings in the 10 provinces (n = 25 113, overall response rate = 69.8%), excluding full-time members of the CAF, persons living on reserves and other Aboriginal settlements, and the institutionalized population (together comprising less than 3% of the Canadian population). 21
Measures
Mental Disorders
The surveys used the World Health Organization Composite International Diagnostic Interview (WHO-CIDI) to assess past-year mental disorders, using Diagnostic and Statistical Manual of the American Psychiatric Association, fourth edition (DSM-IV) criteria. 22 WHO-CIDI is a lay-administered instrument with good consistency with clinical diagnostic instruments. 23,24 MDE, GAD, and AUD (alcohol abuse or alcohol dependence) were the only mental disorders that were assessed in both surveys.
Suicidal Behaviours
Past-year suicidal ideation (thoughts and plans) was assessed by asking the respondents whether they had “seriously thought about committing suicide or taking [their] own life,” or “made a plan for committing suicide” during the 12 months preceding the interview. Past-year suicide attempts were assessed by using the question of whether respondents “attempted suicide or tried to take [their] own life” in the past 12 months.
Sociodemographic Characteristics
Sociodemographic variables included age (<25, 25 to 34, 35 to 44, 45 to 54, and ≥55 years), sex, race (white, nonwhite, and multiple), marital status (married/common law, widowed/separated/divorced, and never married), education (less than secondary, secondary, some postsecondary, and postsecondary completion), personal income (<$20 000, $20 000 to $39 999, $40 000 to $59 999, $60 000 to $79 999, and ≥$80 000), and province of residence (Atlantic, Quebec, Ontario, Prairies, and British Columbia).
Child Abuse Victimization
Child abuse history (witnessing domestic violence, physical abuse, and sexual abuse) was assessed by asking respondents aged 18 years and older 6 questions from the Childhood Experiences of Violence Questionnaire.
25
Witnessing domestic violence was assessed by asking the respondent how many times they “saw or heard any one of [their] parents, step-parents, or guardians hit each other or another adult in [their] home.” Childhood physical abuse was assessed by asking the respondent how many times an adult had “slapped [them] on the face, head, or ears, or hit or spanked with something hard to hurt [them],” “pushed, grabbed, shoved, or thrown something at [them] to hurt [them],” or “kicked, bitten, punched, choked, burned [them], or physically attacked [them] in some way
To approximate the Regular Force population, we restricted the CCHS-MH sample to those who were 1) full-time employed, 2) aged 18 to 60 years, 3) not recently immigrated (hence, not eligible for CAF service), and 4) not reporting any physical or mental chronic conditions that would typically make them unfit for military service.
CAF medical fitness decisions are driven by individualized medical employment limitations, as opposed to blanket exclusions for those with specific diagnoses. 26 The exclusionary conditions were therefore identified in consultation with physicians in the Medical Standards Section of the CAF’s Directorate of Medical Policy. The following conditions were judged to more likely than not result in medical employment limitations incompatible with CAF service: chronic bronchitis, emphysema or chronic obstructive pulmonary disease, heart disease, stroke, Crohn’s disease, ulcerative colitis, bowel incontinence, epilepsy, Alzheimer’s disease, chronic fatigue syndrome, multiple chemical sensitivities, schizophrenia or other psychosis, bipolar disorder, mania, dysthymia, or eating disorder. Respondents with self-reported body mass index ≥35 kg/m2 were also excluded.
Statistical Analyses
Prevalence estimates were calculated using survey and bootstrap weights generated by Statistics Canada for each survey. To strengthen comparability with Regular Force personnel, an iterative proportional fitting (IPF) procedure 27,28 was applied to adjust the survey and bootstrap weights in the restricted CGP sample so that the marginal distribution of key sociodemographic variables (age, sex, ethnicity, education, marital status, personal income, and province of residence) and child abuse victimization variables (witnessing domestic violence, physical abuse, and sexual abuse) corresponded to their marginal distribution in the Regular Force. These variables were chosen because they were available in both surveys, had substantially different distributions across the 2 samples, and had a significant association with mental disorders or suicidal behaviour. 29,30
IPF is an enhanced weighting procedure used for adjusting the sample weights in a survey in order to reduce the potential for bias and improve the reliability of survey estimates. Its main advantages over the standard methods of adjustment such as post-stratification are that it allows for the inclusion of a greater variety of variables to control for the distribution of the final sample weights and it does not require the combining or collapsing of categories of variables when dealing with small sample sizes within post-stratification categories. IPF makes adjustments for each sociodemographic and child abuse victimization variable individually by applying an iterative process to survey and bootstrap weights in the restricted CGP sample until it was representative of the Regular Force population. 31 These weights were calculated in SAS 9.3 software (SAS Institute Inc, Cary, NC) with an enhanced IPF algorithm 32 and were then used to estimate the prevalence of past-year mental disorders and suicidal behaviours in the matched CGP sample. The corresponding 95% confidence intervals for all prevalence estimates were obtained using bootstrap methods. Proportions are significantly different if their 95% confidence intervals do not overlap.
Statistics Canada’s confidentiality guidelines 20,21 required that 1) only weighted descriptive output was approved for release and 2) weighted sample estimates were rounded to the nearest 20.
Results
Table 1 identifies disparities in the distribution of the sociodemographic variables between the Regular Force and civilian populations (overall, restricted, and matched as noted in the Methods). The Regular Force was much younger: only 1.58% of Regular Force personnel were aged 55 years and older, compared with 34.74% in the CCHS-MH sample and 10.98% in the restricted full-time employed CGP sample. The Regular Force had a much higher proportion of male participants (86.16% compared with 49.15% in CCHS-MH sample and 56.98% in the restricted CGP sample, respectively). The proportion of the Regular Force without completed secondary school (4.08%) was much lower than in the general adult population (14.82%) and the full-time employed CGP sample (8.00%). Dramatic differences in personal income were noted. Only 5.67% of Regular Force personnel had a personal income lower than $40 000, compared with 55.64% of adults in the CCHS-MH sample and 33.76% of full-time employed civilians. Nonwhites represented less than 10% in the Regular Force compared with more than 20% in the CGP samples.
Distribution of sociodemographic characteristics in Regular Force personnel, the CGP, and the restricted full-time employed population.
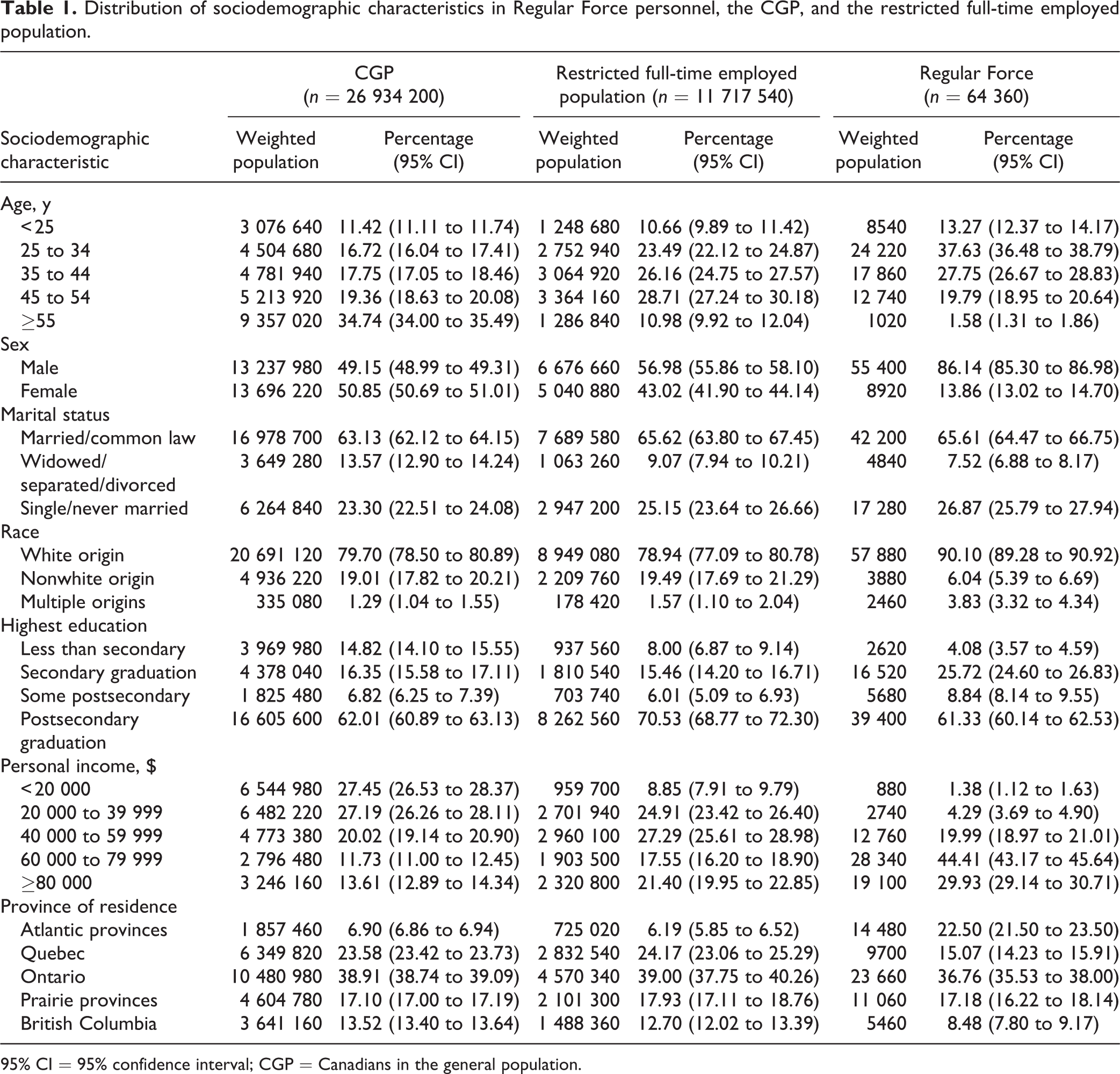
95% CI = 95% confidence interval; CGP = Canadians in the general population.
The distribution of child abuse victimization is presented in Table 2. The majority of Regular Force personnel (61.27%) reported some form of childhood physical abuse at least once. The corresponding proportions in the adult and restricted CGP were lower (42.21% and 43.40%, respectively). Similarly, exposure to domestic violence was more frequently reported by Regular Force personnel (18.31% compared with 15.08% in CCHS-MH sample and 14.68% in matched civilians). However, sexual abuse was less frequent in the Regular Force (7.58%) and the restricted CGP sample (8.05%) than in the adult CGP (10.14%).
Distribution of child abuse victimization in Regular Force personnel, the CGP, and the restricted full-time employed civilian population.
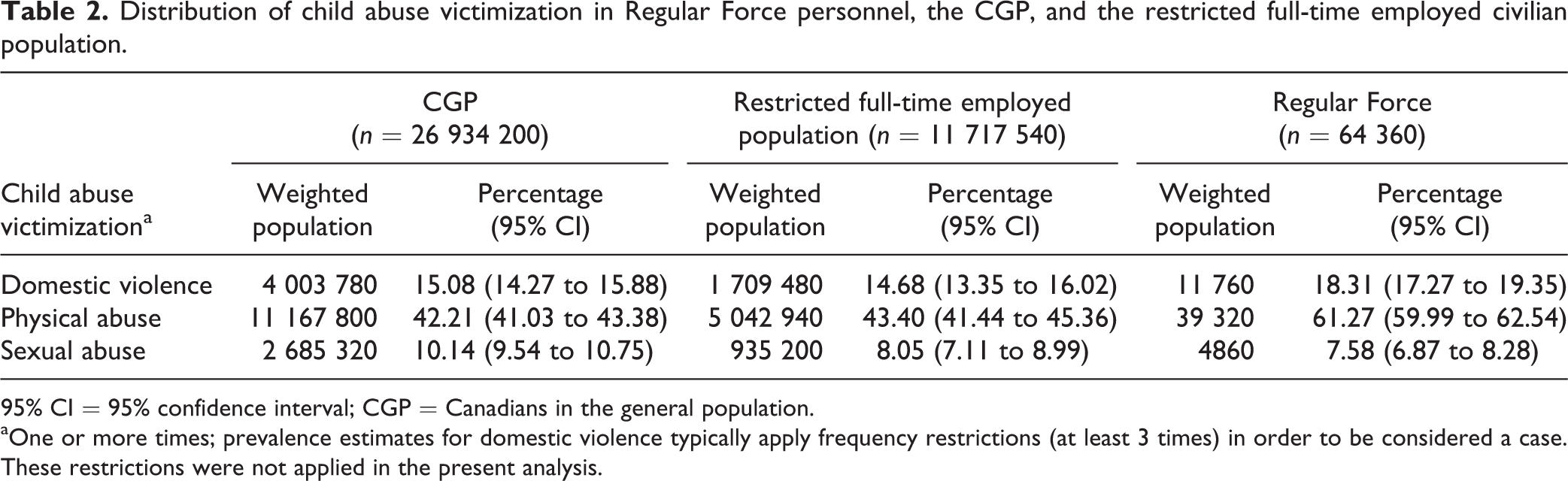
95% CI = 95% confidence interval; CGP = Canadians in the general population.
aOne or more times; prevalence estimates for domestic violence typically apply frequency restrictions (at least 3 times) in order to be considered a case. These restrictions were not applied in the present analysis.
Table 3 presents the rates of mental disorders and suicidal behaviours in Regular Force and the sequential CGP subsamples. The last 2 columns of this sequence show the expected rates in a representative sample of Canadian general population with similar sociodemographic characteristics and history of childhood trauma as Regular Force personnel. With the exception of AUD, the prevalence of mental disorders and suicidal behaviours was much lower in civilian samples than in Regular Force personnel. Specifically, the rates of past-year MDE in the full adult CGP (4.65%), the restricted CGP subsample (3.48%), and the CGP subsample with the same sociodemographic composition as Regular Force personnel (2.75%) were significantly lower than the rate in Regular Force personnel (7.96%). The same pattern held for past-year GAD: 4.69% in the Regular Force, 2.60% in the full sample, 1.81% in the restricted CGP subsample, and 1.28% in the subsample matched for sociodemographics. Past-year suicide ideation was lower in the restricted civilian subsample (2.09%) and in the sociodemographically matched civilians (1.46%) than in the Regular Force (4.32%). Similarly, past-year suicide attempts were much lower in the restricted civilian subsample than in the Regular Force. AUD was the only condition in which the rates were substantially higher in the fully matched civilians (6.62%) than in Regular Force personnel (4.49%).
Prevalence of past-year mental disorders and suicidal behaviours in Regular Force personnel, CGP, restricted, and matched full-time employed civilian populations.
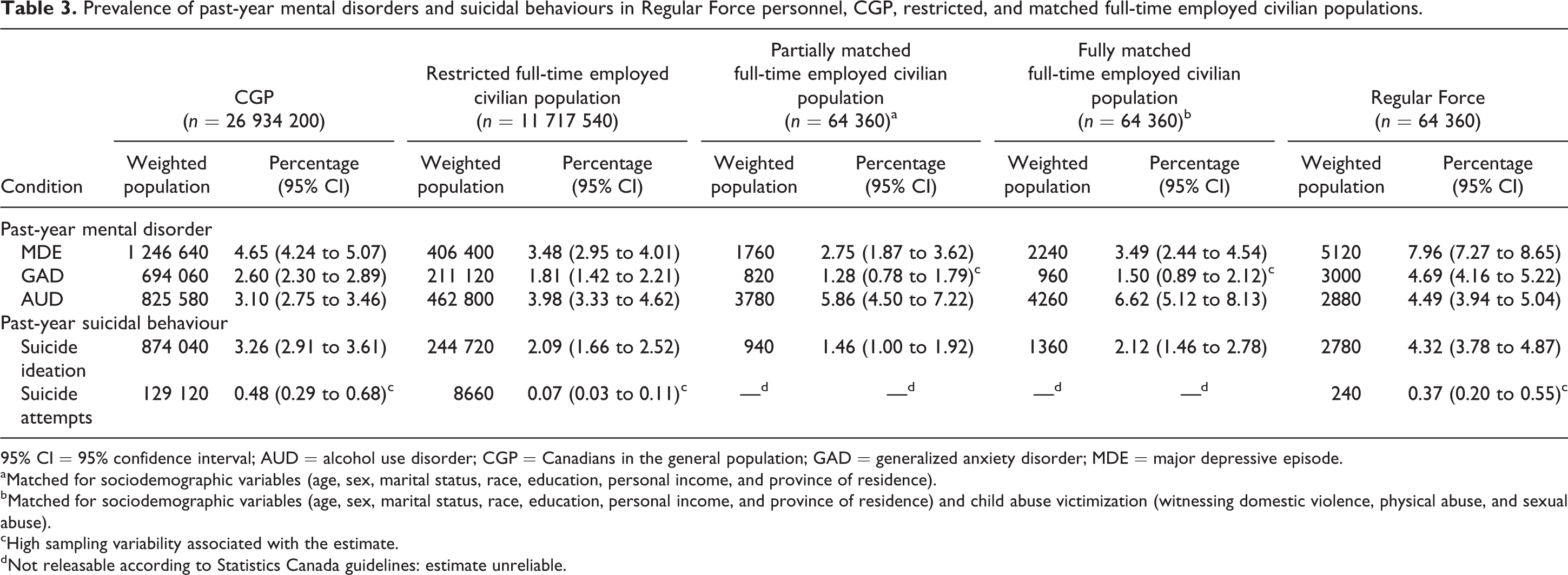
95% CI = 95% confidence interval; AUD = alcohol use disorder; CGP = Canadians in the general population; GAD = generalized anxiety disorder; MDE = major depressive episode.
aMatched for sociodemographic variables (age, sex, marital status, race, education, personal income, and province of residence).
bMatched for sociodemographic variables (age, sex, marital status, race, education, personal income, and province of residence) and child abuse victimization (witnessing domestic violence, physical abuse, and sexual abuse).
cHigh sampling variability associated with the estimate.
dNot releasable according to Statistics Canada guidelines: estimate unreliable.
The addition of child abuse victimization variables narrowed but did not eliminate the differences in prevalence estimates across most conditions. The exception was AUD, in which the differences widened after matching for childhood trauma.
Discussion
Summary of Key Findings
To our knowledge, this is the first study to compare the prevalence of mental disorders and suicidal behaviours in a representative sample of Canadian military personnel and a sociodemographically comparable group of Canadians. With 1 notable exception (AUD), the prevalence estimates of past-year mental disorders, and suicidal behaviours analyzed in this study were higher in Regular Force personnel than in the matched CGP. The differences in rates between the samples remained substantial, even after further adjustment for child abuse victimization.
Comparison With Other Findings
Our finding of higher prevalence of mood and anxiety disorders in military personnel coheres with other comparisons. One US study showed higher rates of 30-day major depressive disorder and GAD in nondeployed soldiers than in sociodemographically comparable civilians. 14 Another US study on lifetime disorders showed a higher rate of GAD in new soldiers than in corresponding matched civilians, 15 although no differences in MDE were detected, perhaps owing to the high sampling error associated with the estimates in the calibrated civilian sample. In addition, a recent UK study showed that serving military personnel were twice as likely to endorse symptoms of probable common mental disorders than employed individuals in the general population, after accounting for demographic differences between the samples. 16 Likewise, Australian military personnel had an excess of depression, posttraumatic stress disorder (PTSD), and suicidal ideation relative to the demographically similar general population. 33
Comparison of rates of AUD in military vs. civilian populations has yielded more divergent findings. Our finding of lower risk of AUD in CAF personnel relative to fully matched civilians, coheres with similar findings in Australia. 33 However, no military-civilian differences were seen in US soldiers, 14 while higher rates of high-risk drinking were seen in UK military personnel relative to the UK household population. 34 We do not have a ready explanation for these divergent findings except to note that of these comparisons, ours used the most comparable survey data with optimal assessment of AUD using the CIDI. As noted earlier, higher rates of the mood and anxiety disorders that often drive comorbid substance use disorders have been noted in military personnel in all four nations (Canada, Australia, the US, and the UK), suggesting that that factor does not account for the differences in the relative prevalence of AUD in military and civilian populations in those nations. It is possible instead that there are relative differences in the military and civilian social environments in different nations with respect to normative drinking behaviour.
These studies provide useful international points of comparison with our own findings, suggesting that higher rates of common mental disorders are not unique to the Canadian military. However, each has important limitations, including noncontemporaneous military and civilian samples, 14 –16,33 different survey modes, 14 –16,33 use of brief instruments for assessment of mental disorders, 14,16 and low response rates. 33
Our finding of higher rates of depression in CAF personnel relative to the CGP is also in accord with past CAF findings. In 2002, however, a distinct pattern of differences was seen in the prevalence of past-year mental disorders and suicidal behaviours between CAF Regular Force personnel and the CGP. 6,9 Specifically, an increased age/sex-adjusted risk of past-year MDE 9,13 and of panic disorder was observed; no differences were seen for the other mental health problems assessed on both the military and CGP surveys (specifically, social phobia, 13 alcohol dependence, 9 or suicidal ideation 6 ). Neither PTSD nor GAD was assessed in the 2002 CGP survey. 13 However, a lower prevalence of past-year suicide attempts was seen in Canadian military personnel (Regular Force and Reserve Force combined) than in the 2002 CGP, although less extensive adjustments were used relative to our analysis. 6
Limitations
Our study has several limitations. First, both surveys were cross-sectional and retrospective in nature, relying on respondents’ self-reporting of symptoms over varying time periods. Second, other important mental disorders were not evaluated in both surveys, limiting our capacity to compare the samples on a wider range of mental disorders, including those with special relevance for the military, such as PTSD. Likewise, with the exception of child abuse victimization, no other traumatic events were assessed in both surveys, precluding us from matching the samples on additional intrapersonal and occupation-related traumatic events. Third, the surveys did not collect any information about the age of enlistment, precluding analysis of the contribution of preenlistment mental disorders, which have been shown to be prevalent in US 29,30 and Australian 35 military personnel. Finally, we could only match on characteristics assessed in both surveys.
Notwithstanding these limitations, the cross-population comparison was facilitated by the use of the same interview instrument (WHO-CIDI), the same mental disorder definitions (DSM-IV), the same computerized interviewing method (CAPI), and similar sampling designs in both surveys. The comparison was further enhanced by the use of a robust adjustment method (IPF) to match the 2 populations on a comprehensive set of key covariates.
Implications
The significant and clinically meaningful higher burden of past-year MDE, GAD, suicidal ideation, and suicide attempts in the CAF relative to CGP warrants an explanation. We can reasonably conclude that these differences are not attributable to the common methodological problems that complicate such comparisons, especially lack of highly comparable survey data and the failure to use a sufficiently similar general population comparison group. The implications of the findings depend heavily on their driving factors. We discuss here 4 potential differences in the military and general populations that may be driving our findings: 1) trauma exposure, 2) mental health systems, 3) selection effects, and 4) survey context effects.
Military personnel have a significant risk of exposure to occupational trauma, which is known to increase the risk of many mental disorders. 1 Of the survey population, 45% had deployed in support of the mission in Afghanistan. 36 Furthermore, 35% of the population had been exposed to combat in the past, and 34% and 14% had exposure to peacekeeping or to atrocities, respectively. 37 Those deployed in support of the mission in Afghanistan had higher rates of MDE, PTSD, and GAD. 36 Occupational trauma in military personnel occurs in addition to other sources of lifetime trauma to which any Canadian may be exposed; some Canadians also have work-related trauma exposure. Unfortunately, lifetime trauma exposure other than child abuse victimization was not assessed in the CCHS-MH survey, precluding formal exploration of this hypothesis.
There are many differences in the military mental health system relative to the public system, 38 and these could, in theory, contribute to the observed differences in prevalence differences. However, on a conceptual basis at least, the CAF has addressed most of the structural barriers to care that plague the Canadian public mental health care system. 10,38 Recent findings from the survey data used in our analysis confirm that these efforts have resulted in greater recognition of unmet need and greater likelihood of perceived need being met through services. 39 We therefore believe that it is unlikely that weaknesses in the military mental health system explain the higher prevalence rates we documented.
These prevalence differences could also relate to complex selection effects that occur at the time of recruitment and on an ongoing basis during service as those who develop mental disorders get disproportionately released for medical and other reasons. 40 Once in service, this selection effect should put downward pressure on military rates relative to those in the general population. Although it may contribute to prevalence differences, it cannot explain the much higher prevalence we have documented in CAF personnel.
Selection effects at the time of recruitment have less clear effects on prevalence differences. There is the perception that those selected for military service represent a disproportionately healthy segment of the population, given the rigorous screening and selection procedures in place. While these procedures would most likely have screened out those with chronic physical disorders or severe psychiatric illnesses, (including schizophrenia and perhaps more severe forms of bipolar disorder), the reality is more complicated. For mental disorders, screening and selection processes in an all-volunteer military such as the CAF are strongly dependent on truthful disclosure of past problems on the part of a motivated applicant. Many of the mental disorders in the young male demographic that seeks military service have onset in young adulthood. 41 Indeed, simulation studies in the US Army suggest that the vast majority of individuals with MDE, GAD, and AUD had their onset before the age of recruitment. 29,30 Subsequent studies using new recruits 15 and nondeployed soldiers 14 partially replicated these findings, suggesting that the differences in prevalence estimates between the military and matched civilians may be related at least in part to the high rates of lifetime disorders that predate military service. Why military service appeals to those with an increased risk for early-onset mental disorders is unclear. Unfortunately, information on the timing of mental disorder onset was not captured in our general population survey, precluding formal exploration of this phenomenon in the CAF. 15
Finally, it has been suggested that occupational mental health studies are associated with framing effects, in which personnel view such surveys as a mechanism to communicate their occupational stress concerns. 16,42 Indeed, a recent meta-analysis showed higher rates of mental health symptoms in occupational surveys. 42 However, the studies in question used brief screening questionnaires with often unsatisfactory response rates. Our data cannot formally explore this interesting issue directly, but our methods all argue against technical factors such as low response rates as an explanation for possible contextual effects.
Conclusions
To return to the important issue of implications, the primary implication of our findings is simply that the CAF mental health system must be scaled and resourced to address the truly disproportionate burden of mental health problems relative to the CGP: The differences cannot be dismissed as simple technical factors in the analysis. Indeed, investments over the past decade have expanded and reinforced the CAF system, 38 and there is emerging evidence that these efforts have borne fruit. 39,43
Occupational trauma remains an attractive target for CAF prevention and control efforts, even if we could not formally explore its contribution to prevalence differences. Research along these lines will depend on better population-based data on trauma exposure and its consequences in the CGP. We believe that the CAF mental health system is, if anything, stronger than the public system in Canada 38 ; hence, this cannot account for the higher prevalence rates we documented. Further evaluation of the performance of the military health system is nevertheless important, and it may ultimately lead to stronger systems of prevention and care for all Canadians. Finally, the important questions as to the role of selection effects on the prevalence of mental disorders in military personnel and of contextual survey effects must be addressed in studies designed to rigorously test those important factors.
Footnotes
Acknowledgements
The authors would like to thank Anne M. Gadermann and Maria Petukhova who provided useful methodological details on one of their papers.
Authors’ Note
The opinions expressed in this paper are those of the authors and do not represent the official policy of the Department of National Defence, the Canadian Armed Forces, or the Government of Canada.
An earlier version of this paper was presented at the Military and Veteran Health Research Forum; 2014 Nov 24-26; Toronto (ON).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Department of National Defence, which provided salary support to the authors.