
Abstract
Introduction
The clinical course of COVID-19 is characterized by a dysregulated immune response that follows viral infection. This hyper-immune response causes the release of pro-inflammatory cytokines such as interleukin-6 (IL-6), interleukin-1 (IL-1), interleukin-17 (IL-17), and tumor necrosis factor-alpha (TNF-α), ultimately leading to tissue damage and multiple organ failure. 1 The COVID-19 vaccine has shown efficient protection from severe complications.2,3 However, infections with SARS-CoV-2 are still spread worldwide and new variants are being detected.4,5 Therefore, it is still necessary to improve therapeutic strategies to reduce the replication of SARS-CoV-2, interfere with the early phases of infection, and treat patients experiencing the hyper-immune response.
Antiviral agents inhibit the mechanisms of viral replication and transcription. 6 Among these agents, remdesivir binds to the viral RNA-dependent RNA polymerase and has been approved by the FDA and EMA for COVID-19 treatment in different settings, including outpatients and hospitalized patients requiring oxygen.7,8
Anti-inflammatory agents act in a more advanced stage of the disease than antiviral agents and aim to dampen the effects of inflammatory cytokines to reduce acute respiratory distress syndrome (ARDS). The use of anti-inflammatory agents targeting IL-6, IL-6 receptor, and IL-1 has been described in clinical practice.9–12 Canakinumab, a fully human monoclonal anti-IL-1β antibody, has been shown to neutralize IL-1β signaling, thereby reducing inflammation in different settings.13,14 It has proven to be effective and safe in early intervention for COVID-19.12,15 In this work, we aimed to expand the knowledge on potential therapeutic interventions for moderate-to-severe COVID-19 by the description of the outcome of real-world data of hospitalized patients treated with the combination of canakinumab and remdesivir plus the standard of care therapy.
Patients and methods
Patients
This is a retrospective cohort study describing the outcome of combination therapy with canakinumab and remdesivir as add-on to standard of care (SOC) treatment in moderate-to-severe COVID-19 patients with elevated reactive pro-inflammatory markers and low oxygen saturation values. The study was conducted at the “Annunziata” Hospital, Cosenza, Italy, between August and November 2021. The local authorized institutional review board and ethics committee was notified and approved the study. “Annunziata” Hospital, Cosenza, Italy, provided a letter of permission authorizing the study. The safety and effectiveness of outcomes were overseen by the local monitoring board. As per Italian law, no study registration number was required. 16 Written informed consent was obtained from all subjects before the study.
Inclusion and exclusion criteria
Inclusion criteria were as follows: adults with SARS-CoV-2 infection detected by PCR, pneumonia diagnosed by chest computed tomography (CT), and with evidence of cytokine release syndrome (CRS) identified through the following lab tests: CRP >20 mg/L, ferritin >600 ng/L, and IL-6 >40 pg/mL.
Moreover, values of SpO2 below the reference values (i.e., between 93 and 97%), arterial PaCO2 below 35–45 mmHg, and PaO2 below 80–100 mmHg were also considered.
COVID-19 patients were excluded from the study in case of an active bacterial, viral, or parasitic infection, low white blood cell counts, a weak immune system, 17 a history of human immunodeficiency virus, hepatitis B or C infection, or recurrent infections. Patients who had recently received any live vaccine, who presented malignancies, and patients with any chronic auto-inflammatory condition were also excluded from the study.
Pharmacological treatments
SOC treatment included high-dose dexamethasone (dexamethasone-phosphate 12 mg/day on days 1–7 and then 8 mg/day on days 8–14) or an equivalent dose of another corticosteroid (e.g., prednisone, methylprednisolone, or hydrocortisone), a therapeutic dose of heparin for non-pregnant patients with elevated D-dimer levels and no increased bleeding risk, a high-dose of doxofylline intravenously (IV) (in a 1 h infusion, all patients received 200 mg doxofylline IV), oral colchicine (1 mg daily for 10 days or until discharge), and antibiotic therapy (Ceftriaxone 2 g/day IV or doxycycline 100 mg BID).
In addition to SOC treatment, canakinumab 450 mg (for patients ≥40 and <60 kg), 600 mg (for those between ≥60 and <80 kg), or 750 mg (for patients ≥80 kg) in 250 mL of 5% dextrose was administered as a single dose by IV infusion over the course of 2 h on day 1.
Remdesivir was administered IV at a loading dose of 200 mg on day 1, followed by daily, 1 h infusion of 100 mg for a maximum of 4 days, for a total duration of 5 days.
Biochemical analysis and instrumental tests
At admission and before the start of the canakinumab + remdesivir + SOC treatment, biochemical markers (including plasma IL-6, CRP, haptoglobin [Hp], and fibrinogen), a hemogram (with platelet-related blood indices), arterial hemogasanalysis, and different prognostic markers18–20 for early mortality were evaluated.
In addition, the determination of the presence and distribution of ground-glass opacity (GGO), 21 through CT imaging, was assessed for each patient.
Hospitalized patients treated with combination therapy (canakinumab + remdesivir + SOC) were assessed for nasopharyngeal normalized viral load, measured by the cycle threshold after collection with swabs through validated devices, at admission and at days 3, 6, 9, 12, and 15. Participants were followed for a total of 28 days. Biochemical markers were re-evaluated at day 7 of canakinumab + remdesivir + SOC treatment.
Endpoints of the study
Primary endpoints of the study were variation of biochemical and hematological prognostic markers evaluated at day 7 of canakinumab + remdesivir + SOC treatment versus baseline. Secondary endpoint was variation of arterial hemogasanalysis parameters after 7 days of canakinumab + remdesivir + SOC treatment versus baseline. Distribution of GGO on day 7 was investigated by CT imaging as exploratory outcome measure.
Statistical analysis
Paired t test, performed with GraphPad Prism version 8.0.0 for Windows (GraphPad Software, San Diego, California, USA) was applied to compare biochemical, hematological marker, and arterial hemogasanalysis values at baseline versus 7 days of canakinumab + remdesivir + SOC treatment. D’Agostino and Pearson omnibus test to check for normal distribution was applied, and Wilcoxon matched-pairs signed rank test was used when Gaussian distribution was not assumed. Bonferroni correction was applied to correct for multiple comparison. p-Values <.05 (according to the relative adjusted values) were considered significant.
Results
One hundred-twenty patients were enrolled, and a total of 17 patients with moderate-to-severe illness were included in the study. Figure 1 reports the patient flow chart and summarizes the pharmacological interventions. Patients’ characteristics at admission are reported in Table 1. The patients were prevalently males, 10/17 (59%), and the median age was 64 years (range: 39–85 years). All patients showed fever at admission, 15/17 (88%) presented dyspnea, and 12/17 (71%) had a cough. The CT characteristics at admission were assessed using a semi-quantitative visual scoring system (VSQ) as previously reported.12,21 By VSQ, 10/17 patients (59%) showed an involvement of the chest between 26 and 50%, 5/17 patients (29%) had 51% to 75% of chest involvement while one patient (6%, the one with the fatal outcome) presented an involvement of the chest of more than 75% (Table 1). Patient flow chart and summary of the pharmacological interventions. Patient demographics and clinical characteristics upon presentation (N = 17). aValues calculated out of 16 patients; one patient transferred to the intensive care unit after 3 days. GGO: ground-glass opacity; VSQ: visual semi-quantitative CT assessment of the chest.

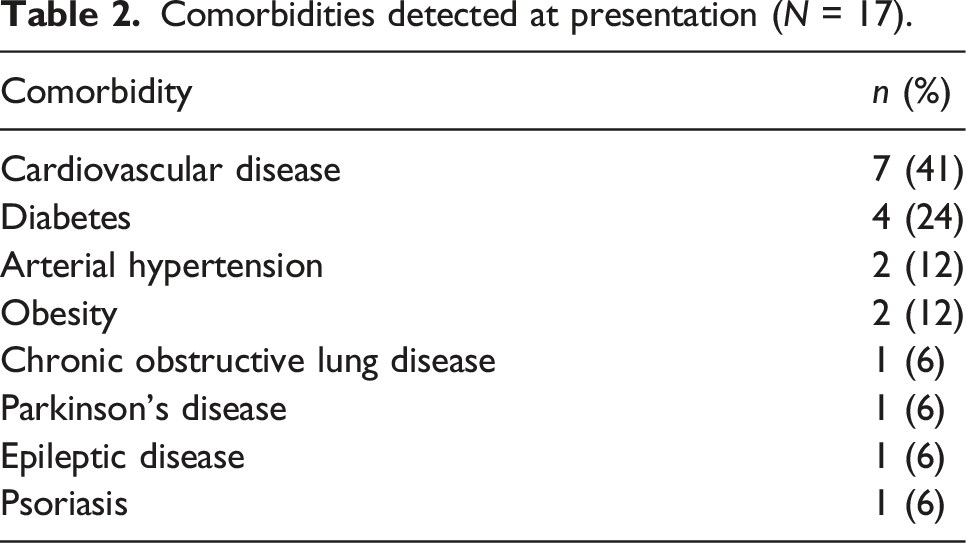
Comorbidities detected at presentation (N = 17).
Arterial hemogasanalysis at admission and 7 days after the administration of canakinumab + remdesivir + SOC (N = 17).

an = 16.
bWilcoxon matched-pairs signed rank test was applied as normality test failed.
cPaired t test after D’Agostino and Pearson omnibus test was applied.
The median hospitalization time was 12.5 days (range: 7–35 days): this value was calculated from the data of 16 patients, excluding the patient that was transferred to the intensive care unit after 3 days.
Fifteen patients out of seventeen (88%) did not experience complications during the treatment. One patient out of seventeen (6%) developed a mild-to-moderate pneumomediastinal flap involving the superior mediastinum and extending cranially, with the involvement of the soft tissues of the supraclavicular regions and part of the proximal tract of the anterior thoracic wall. This situation was eventually resolved, and the patient was discharged.
Inflammatory markers measured at admission and 7 days after the administration of canakinumab + remdesivir + SOC (N = 17).

aN = 15.
bWilcoxon matched-pairs signed rank test was applied as normality test failed.
cN = 16.
dPaired t test after D’Agostino and Pearson omnibus test was applied.
eN = 13.
fN = 9.
gN = 14.
Significant values are reported in italics.
In addition, hematological prognostic markers such as neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), CRP-to-lymphocyte ratio (CLR), monocyte-to-lymphocyte ratio (MLR), and derived neutrophil-to-lymphocyte ratio (dNLR) were determined. After 7 days of combination treatment, NLR, CLR, and dNLR were reduced (Table 4).
A negative viral load, detected by the nasopharyngeal test, was obtained for each patient between 7 and 14 days after the start of the combination therapy.
A panel of lymphocyte subset analysis was performed on 10/17 patients (59%) at admission (supplementary table S1).
No unforeseen adverse events were reported in patients during the treatment with canakinumab + remdesivir + SOC.
Discussion
COVID-19 is, to this day, an emergency for the healthcare system. The constant evolution of the virus and the identification of new variants raise concerns regarding the infection and the chance of experiencing severe complications. Despite the advances made in the past 2 years, new therapeutic alternatives are constantly being tested. In this work, we disclose our experience with the combination therapy of canakinumab and remdesivir, in addition to SOC, for the treatment of moderate-to-severe hospitalized patients and clear signs of a hyperinflammatory response. We document that after 7 days of treatment, patients showed a significant improvement in the markers of inflammation, with the only exception of procalcitonin. CRP, LDH, D-dimer, and ferritin values remained higher than the normal range but showed a clear improvement with respect to basal values. Another advancement was detected in the O2 saturation after 7 days for the majority of patients; one patient was admitted to the ICU after 3 days with a fatal prognosis. After a median of 12.5 days of hospitalization, all the other patients recovered and were discharged.
Among the common prognostic markers evaluated for COVID-19 severity and patient mortality,18,22 NLR and CLR were found to be elevated at admission in our cohort of patients but were reduced after 7 days of combination treatment. PLR also showed a decrease, although to a lesser extent than NLR and CLR, while MLR resulted unchanged. The wide variation of hematological values registered at admission, which could depend either on the different severity of the disease or on individual variability, could have played a role in this evaluation. We cannot exclude that these markers could be eventually significantly reduced after a longer time, that is, 14 days from the start of the treatment. Unfortunately, hematological values were not available at all the time points for all the patients, and a proper analysis was not feasible.
Interestingly, also dNLR resulted reduced after canakinumab + remdesivir + SOC treatment. dNLR is a derived measure of NLR which describes the level of neutrophils in the peripheral blood: a high level of circulating neutrophils can indicate the increased activation of innate immunity upon infection and/or inflammation. In cancer, elevated dNLR levels are markers of a poor prognosis and may indicate a reduced response to treatments.19,23 Similarly, this marker is being considered as a good indicator of the prognosis of COVID-19 and other infective diseases.20,24 In the study of Asghar et al., the median (interquartile range) baseline value of dNLR for COVID-19 hospitalized patients was 4.00 (2.33–6.14), similar to the value reported in our cohort. The limited number of patients studied notwithstanding, the good outcome described with its reduction may deserve further attention in clinical studies, especially in response to anti-inflammatory treatment(s), as in the case of canakinumab in the present study.
Computed tomography imaging at 7 days showed a progression toward a more organized tissue phase, which is in line with the standard resolution process in the lungs. Indeed, this finding led to a positive outcome in the majority of patients that gradually reduced O2 therapy until dismission. These data indicate the positive response in our patients with medium-to-severe pneumonia at admission, except for one patient.
Obesity is confirmed as a comorbidity associated with a higher risk of severe COVID-19 25 ; also in our small cohort, the fatal outcome was registered in one of the obese patients.
Canakinumab as a therapy to dampen COVID-19 hyperinflammatory response has already been investigated,12,15,26 highlighting positive outcomes both in terms of reduction of inflammation markers and oxygen saturation improvement. The canakinumab + remdesivir + SOC treatment appears even more efficient than canakinumab alone 12 in reducing some inflammatory markers with effective results at 7 days after starting the treatment, although a direct comparison between patients in the same setting should be done as confirmation of the better effectiveness. Indeed, a meta-analysis showed how canakinumab treatment is associated with reduced mortality, reduced likelihood of developing severe COVID-19 disease, and reduced levels of CRP. 27 Despite the limited number of studies and patients included in the analysis, we believe there is a valid rationale to support additional research on the use of canakinumab in COVID-19. In this light, the choice to test the combination of canakinumab + remdesivir + SOC was done to combine the anti-IL-1β effect targeting the cytokine storm and the antiviral features of remdesivir to reduce virus replication ability and dampen the first steps of infection.
The use of remdesivir in COVID-19 patients has been extensively investigated and some adverse events such as bacteremia and bradycardia have been reported in the literature as being associated to its use.28,29 Moreover, remdesivir administration in moderate-severe and critically severe COVID-19 was also associated to better survival when given prior to high-flow oxygen support and to a lower rate of occurrence of arterial thrombotic events.30,31 In our cohort, we did not observe increased bacterial super-infections nor bradycardia or arterial thrombotic events. We cannot comment on the positive outcome on patient survival of remdesivir administration during low-flow oxygen support as the whole cohort considered in the present study was treated with remdesivir already in a situation of mechanical ventilation. Nevertheless, we could show that the combination canakinumab + remdesivir + SOC allows a better survival also to patients in critical conditions. The cohort tested is anyway small compared to the one investigated in the aforementioned studies, and we cannot exclude that some of these events could be observed when considering larger number of patients. Currently, the use of this combination therapy is poorly explored mainly due to the lack of data about canakinumab treatment. Nevertheless, the reduction of the inflammatory markers, the absence of severe side effects as a result of our experience and confirmed by a literature review, and the low complications registered suggest the need of expanding the studies to obtain a better characterization of the therapy’s usefulness in the clinical setting.
This study presents limitations due to the small cohort of patients, the absence of a proper control group, the reduced follow-up time, its retrospective design, and the recruitment of patients at a single center. No power calculation was done for the estimation of sample size selected for the study. Despite the small number of included patients, this is a retrospective analysis and not a pilot study. Nevertheless, these patients represent the real-world clinical practice even in the current days when vaccination is widely available. There is a need to expand the tools for COVID-19 treatment, especially for fragile patients characterized by the presence of different comorbidities.
Conclusions
Combination treatment of canakinumab and remdesivir, in addition to SOC, in the early stage of moderate-to-severe COVID-19 showed promising outcomes in terms of safety and effectiveness. This combination has the potential to reduce inflammatory and hematological prognostic markers after 7 days of treatment, making it a potential intervention for hospitalized patients.
Supplemental Material
Supplemental Material - Use of canakinumab and remdesivir in moderate-severe COVID-19 patients: A retrospective analysis
Supplemental Material for Use of canakinumab and remdesivir in moderate-severe COVID-19 patients: A retrospective analysis by Antonio Mastroianni, Valeria Vangeli, Luciana Chidichimo, Filippo Urso, Giuseppe De Marco, Alfredo Zanolini, Francesca Greco, Maria V Mauro and Sonia Greco in International Journal of Immunopathology and Pharmacology.
Footnotes
Acknowledgments
Editorial support was provided by Barbara Bartolini, PhD and Francesca La Rosa, PhD on behalf of Health Publishing & Services Srl. This assistance was funded by Novartis Farma SpA.
Author contributions
All authors contributed to study design and data collection. A.M. analyzed the results and drafted the manuscript. All authors revised the manuscript. All authors have read and approved the final version of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from “Annunziata” Hospital, Cosenza, Internal Committee, according to the Italian Law (CIRCOLARE MINISTERIALE N. 6, 2 September 2002, published on G.U. n. 214, 12 September 2002), which specifies that observational studies need to be notified to the local ethics committee which will be then proceed either to a formal approval or to a simple acknowledgment of the ongoing study. A letter of permission that authorizes the study has been obtained by “Annunziata” Hospital, Cosenza.
Informed consent
Written informed consent was obtained from all subjects before the study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.