
Abstract
Cardiovascular disease represents a major threat to human health with vascular atherosclerosis contributing significantly to its cause, particularly due to the ease of rupture of atherosclerotic plaques. The stability of atherosclerotic plaques is influenced by a variety of factors, including intraplaque neovascularization, the inflammatory response, smooth muscle cells and macrophages, and core lipid volumes. Thus, the investigation of factors affecting the stability of atherosclerotic plaques is of great significance for the development of new drugs for the treatment of atherosclerotic diseases. MicroRNAs are small single-stranded non-coding RNAs between 17 and 22 nucleotides in length. They are translated together with the untranslated region (UTR) of the target gene mRNA, where the completeness of base-pairing can influence the translation or degradation of the target genes. MicroRNAs can thus regulate gene expression at the post-transcriptional level and have been demonstrated to be extensively involved in the regulation of various factors affecting plaque stability. In this paper, we review microRNA development, factors affecting atherosclerotic plaque stability, and the relationship between microRNAs and plaque stability, with the aim of describing the mechanisms by which microRNAs affect gene and protein expression in relation to atherosclerosis progression (including plaque rupture) to suggest new therapeutic targets for atherosclerotic disease.
Background
Atherosclerosis is the main cause of cardiovascular and cerebrovascular diseases, with the rupture and shedding of unstable plaque leading to atherosclerosis-related complications.1,2 At present, relevant imaging examinations can only detect lesions showing structural changes and are unable to predict future plaque instability. 3 microRNAs are small RNAs that are mainly involved in the regulation of post-transcriptional translation of genes in mammals. 4 Studies have shown that microRNAs can attach to and silence genes involved in the atherogenesis pathway, thereby inhibiting the expression of proteins and cellular functions involved in regulating the stability of atherosclerotic plaques. It is thus possible that microRNAs may represent new targets for research to prevent and treat atherosclerotic diseases.5–7 This article aimed to review the role of microRNAs in gene and protein expression in relation to the progression of atherosclerosis, including plaque rupture, to provide new ideas for the prevention of atherosclerotic diseases.
MicroRNA
The discovery of microRNA
In 1993, a small-molecule RNA was first discovered in nematodes. This was found to bind to the non-coding regions of the three ends of target messenger RNAs through complementary base-pairing and thus inhibit the translation of the target mRNA to protein, significantly influencing nematode development; this microRNA was termed miR-LIN4. 8 Subsequent research revealed that microRNAs represent a class of small single-stranded non-coding RNAs with lengths between 17 and 22 nucleotides, and which are mainly involved in the regulation of post-transcriptional translation of genes in vivo. To date, approximately 1000 human microRNAs have been discovered, accounting for 1% of the total number of human genes. They have been shown to regulate the expression of more than 30% of related target genes at a post-transcriptional level and, consequently, to play significant roles in the modulation of modulate the entire process of human growth and development and the occurrence and development of various diseases.9,10
Mechanism of microRNA synthesis
The primary product of microRNA transcription in the nucleus is cleaved by the ribozyme DROSHA RNase into a pre-microRNA of 70 nucleotides in length. This is then transported to the cytoplasm by various transporters. In the cytoplasm, the pre-microRNA is cleaved by DICER endonuclease into a double-stranded microRNA with a length between 17 and 22 nucleotides. 11 This double-stranded microRNA contains mismatched nucleotide sequences at the 5′ end, resulting in structural instability at the 5′ end, and the eventual formation of a single-stranded microRNA with mature biological functions, most of which are derived from the nucleotide sequence at the 5′ end. 12 In addition, very few microRNAs can be processed from intronic RNAs and exons that have no protein-coding function.13,14
Mechanism of microRNA interaction with proteins and genes
The biological functions performed by microRNAs involve the silencing of target mRNAs in the cytoplasm, thus inhibiting the expression of target genes, together with acting in the nucleus to bind to the promoter regions of target genes resulting in their silencing or overexpression, or even binding to exosomes that are secreted from the cell and exert specific effects on other cells. 15 microRNAs can also interact with a variety of proteins during maturation. microRNA biogenesis first occurs in the nucleus, where the RNase III complex DROSHA cuts pri-miRNA into pre-microRNA. Once the pre-microRNAs are exported to the cytoplasm by Exportin 5, the RNase III complex DICER/TARBP2 recognizes their hairpin-like structures and processes them to produce mature microRNAs of approximately 22 nucleotides in length. The mature microRNA is then loaded onto AGO2, which promotes the formation of an mRNA-induced silencing complex (RISC). AGO2 and its family members are considered the only RNA-binding proteins that interact with mature microRNAs.16,17
The interaction between microRNA and microRNA has not been fully defined. Before the discovery of naturally occurring microRNA sponges, some research groups used artificial microRNA sponges as microRNA inhibitors, thereby inhibiting the downstream effects of microRNAs. Studies have shown that microRNAs can target multiple genes, and a single gene can be regulated by multiple microRNAs, indicating co-regulation between microRNAs. For example, studies have found that miR-124 and miR-203 synergically suppressed the ZEB2 pathway associated with the epithelial-mesenchymal transition (EMT) in clear cell renal carcinoma, and synergistic effects between miR-141-3p and miR-145-5p were also observed to regulate target genes in the same tumor.18–20 Increasing evidence strongly suggests that novel microRNA therapies may have significant potential for the treatment of diseases in the future. Although the modulation of some key microRNAs can successfully reverse the pathological process, it is believed that intrinsic synergistic effects between microRNAs may be more effective in disease treatment.
The relationships between microRNAs and long non-coding RNAs (lncRNAs) are also unclear, although studies have found that there is obvious crosstalk between the two RNA species, leading to binding competition between microRNAs and lncRNAs for their targets. LncRNAs act by isolating microRNAs, leading either to silencing of the microRNA or downregulation of target mRNAs, similar to the action of a sponge that can absorb the microRNA and thus reduce its level. The first evidence of an lncRNA as a functional target of a microRNA is the reverse transcript of the cell proliferation-associated protein CDR1 which is a circular RNA (circRNA) that is perfectly complementary to miR-671. 21 MiR-671 can modulate the expression of CDR1, suggesting that antisense transcripts of non-coding RNAs can be used directly as microRNA targets, which is an important starting point for the study of the sponge phenomenon. Changes in circRNA abundance can regulate microRNA activity to target genes accordingly. CircRNA sponges contain large numbers of microRNA binding sites. Overexpression of the circRNA leads to downregulation of the microRNA, thus reducing the inhibitory effects of the microRNA on its downstream mRNA targets and reducing the expression of downstream target genes. A study found that circRNA 0003645 showed carcinogenic effects by sponging the removal of miR-1299 in liver cancer cells. 22
Atherosclerotic plaque progression
Atherosclerotic lesions are found mainly in medium and large arteries, such as the aorta and coronary arteries. The normal structure of the arterial wall is made up of three layers, namely, the outermost outer membrane, which is rich in nerve endings, mast cells, and microvessels that function to nourish the outer membrane, the middle membrane layer consisting of quiescent smooth muscle cells, and a well-organized extracellular matrix composed of elastin, collagen, and other macromolecules, and, lastly, the innermost layer, the intima, which is the site of atherosclerotic plaque formation. Damage to the arterial endothelium is caused by various pathogenic risk factors in the earliest stages of atherosclerosis, followed by oxidative modification of low-density lipoprotein (LDL) in the sub-endothelium to form oxidized low-density lipoprotein (ox-LDL). Monocytes can bind to adhesion molecules expressed by activated endothelial cells and chemokines can promote the migration of the monocyte-adhesion molecule complexes within the arterial wall. Monocytes migrate into the endothelium and mature into macrophages, which can phagocytose 0x-LDL and further differentiate into vesicular cells, a process that causes extracellular matrix deposition and the proliferation and migration of adjacent vascular smooth muscle cells (VSMCs), leading to the formation of fibrous plaques. Plaque formation in the vasculature causes luminal narrowing, reduced blood flow, and ultimately tissue ischemia. If the risk factors for the development of atherosclerosis persist, there is a recurrent damage-repair process that results in the thinning of the fibrous cap, lipid pools, and the necrotic core of the atheromatous plaque, which eventually progresses to an unstable plaque. In the presence of hemodynamic changes, the arterial endothelium can retract and thus its continuity can be interrupted, eventually exposing the subendothelial tissue. This can activate platelets in the blood, causing them to adhere to the intima and form wall thrombi. Unstable (vulnerable) plaques are characterized by a thin fibrous cap, a large lipid pool that is prone to rupture, and the presence of numerous macrophages and a small number of smooth muscle cells. Plaque rupture is the result of a number of factors. 23
Atherosclerotic plaque rupture
Atherosclerotic plaques are composed of extracellular lipid particles, foam cells, and debris that accumulate within the intima of the arterial wall and form a lipid or necrotic core. The core is enveloped by a layer of collagen-rich matrix and smooth muscle cells covered by endothelial cells, termed the fibrous cap. Infiltration of inflammatory cells (mainly T cells and macrophages) occurs with the promotion of plaque progression and thrombosis, which in turn leads to acute intravascular events. The two most common causes of thrombosis are plaque rupture and surface erosion. The plaque ruptures when the fibrous cap covering the surface of the necrotic core splits, exposing the highly thrombogenic core to blood flow. Plaque erosion is caused by endothelial injury or exfoliation and overlying thrombus formation without significant rupture of the fibrous cap. Plaques prone to erosion tend to have high proteoglycan contents and low lipid contents, usually without significant infiltration of inflammatory cells. If plaque rupture or erosion occurs in an environment that is conducive to thrombosis, occlusive thrombosis results and can, in turn, cause acute symptomatic vascular events. In other settings where antithrombotic factors predominate, this can inhibit thrombosis and promote plaque healing. 24 Atherosclerosis is a disseminated process that begins in early childhood and develops asymptomatically in adulthood. In later life, it is clinically manifested by ischemic coronary syndromes, stroke, and peripheral arterial disease. So-called cardiovascular risk factors, including hyperlipidemia, hypertension, diabetes, and tobacco, have a significant impact on the progression of atherosclerosis. 25
Factors affecting the stability of atherosclerotic plaque
Factors affecting the stability of atherosclerotic plaques include both internal and external factors. The internal factors mainly include the density of new blood vessels, the size of eccentric lipids in plaques, inflammation, the thickness of the surface fiber cap, and the contents of smooth muscle cells and macrophages. External factors refer essentially to changes in mechanical and shear stress caused by hemodynamics.26,27 The combination of these internal and external factors determines whether the plaque ruptures or not, with the internal factors often playing a leading role. The present review mainly discusses the influence of internal factors on the stability of atherosclerotic plaque.
Neovascularization and plaque stability
Angiogenesis refers to the process in which endothelial cells form new blood vessels. This is based on the original vessels and involves both budding and non-budding. In atherosclerosis, due to the reduced blood supply within the plaque, long-term hypoxia and inflammation can induce angiogenesis, resulting in the growth of blood vessels into the plaque under the control of the vascular endothelial growth factor signaling pathway. 28 Neovascular endothelial cells are loosely connected and are highly permeable, which is conducive to the exchange of blood oxygen. However, neovascular endothelial cells are both structurally simple and extremely fragile, making them easy to rupture and increasing the instability of the plaque. It has been found that the density of new blood vessels in ruptured atherosclerotic plaques is significantly higher than that in unruptured plaques, and the density of new blood vessels was observed to be positively correlated with plaque stability. 29 Ross et al. 30 believed that angiogenesis is an important marker for the transformation of atherosclerotic stable plaque to unstable plaque; thus, the investigation of factors associated with the angiogenesis pathway would be helpful for the development of drugs to stabilize plaque, which is extremely important for the prevention of atherosclerotic complications.
Inflammatory response and plaque stability
Atherosclerosis is a chronic inflammatory disease and inflammation is involved in the pathophysiological process of atherosclerosis. 31 In the initial stages, ox-LDL represents the main initiator, and its cytotoxic effect can damage vascular endothelial cells directly, leading to changes in endothelial permeability, resulting in the passage of lipids and cellular components through the damaged endothelium and their subsequent deposition in the intima. Furthermore, the oxidation of low-density lipoprotein cholesterol (LDL-c), as well as the influence of monocyte chemotactic protein 1 and platelet-derived growth factor, alters the lymphocyte and monocyte composition of the overall blood leukocyte content within the damaged skin adhesion, leading to aggregation and leukocyte adhesion under the influence of inflammatory cytokines in the blood vessels, resulting in chronic inflammation. In addition, monocytes can transform into monocyte macrophages under the stimulation of monocyte chemotactic protein 1, and the latter can transform into macrophage-derived foam cells through surface receptor-mediated phagocytosis of ox-LDL, occurring at advanced stages of atherosclerosis. 32 The inflammatory environment leads to lipid modification, resulting in increased cytotoxicity, together with the rupture of foam cells, necrosis, and disintegration within the lipid core of the atherosclerotic plaque. In addition, macrophages produce a variety of inflammatory cytokines, such as C-reactive protein, tumor necrosis factor α(TNF-α), and interleukin-6 (IL-6), which induce the production of regulatory molecules. The latter enter the bloodstream to further drive the progression of atherosclerotic plaque. The inflammatory response can also increase plaque instability and accelerate its rupture. On the one hand, the inflammatory response can lead to increased activation of endothelial cells and increased production of cell adhesion molecules, leading to the increased formation of foam cells, thus increasing the amount of lipid within the plaque and increasing the volume of the lipid core. On the other hand, the inflammatory response can also promote the proliferation of macrophages and the activation and secretion of interferon γ, which inhibits smooth muscle cell proliferation and collagen fiber synthesis. In addition, inflammation can induce vasospasm and increase plaque instability by affecting plaque mechanics. 33 Stable angina pectoris can evolve into unstable angina pectoris or even acute myocardial infarction, reflecting the transformation of atherosclerotic plaques from stable to unstable plaques. The expression levels of inflammatory cytokines are often used to evaluate the presence and strength of the inflammatory response. Studies have found that the expression levels of IL-6 and TNF-α in patients with stable angina pectoris are significantly lower than those in patients with unstable angina pectoris. The levels of IL-6 and TNF-α in patients with unstable angina pectoris were found to be significantly lower than those in patients with acute myocardial infarction, indicating that plaque stability was closely related to the inflammatory response.34,35
Smooth muscle cells, macrophages, and endothelial cells are associated with plaque stability
Mature atheromatous plaques consist of a soft atheromatous substance rich in lipids (the necrotic lipid core) and a fibrous cap. It has been found that the fibrous cap is mainly composed of dense collagen fibers, scattered vascular smooth muscle cells, macrophages, and a small amount of elastic fibers, while unstable plaque frequently has a thin fibrous cap. 36 Vascular smooth muscle cells can produce interstitial glue to increase the stability of atherosclerotic plaques, while macrophages can release a variety of matrix metalloproteinases (MMPs), such as MMP-9 and MMP-2. These enzymes can hydrolyze interstitial collagen and extracellular matrix components to reduce the stability of plaques. Therefore, the contents of smooth muscle cells and macrophages in plaques are also important factors affecting plaque stability.37,38 It was found that the apoptosis rate of smooth muscle cells in plaques of patients with unstable angina patients was higher than that in patients with stable angina, and reduced macrophage apoptosis may contribute to plaque stability.39,40 In addition, vascular smooth muscle cells can also affect plaque stability by influencing vascular remodeling, inflammation, calcification, and other factors associated with the plaque. Macrophages can also transform into foam cells and phagocytose lipids to increase the volume of the lipid core, leading to reduced plaque stability.
Low-density lipoprotein and plaque stability
Low-density lipoprotein plays an important role in plaque stability. When there is an excess of LDL, especially ox-LDL, the cholesterol is deposited on the artery walls, resulting in atherosclerotic changes. Several studies have shown that plaques with a lipid core volume greater than 40% of the total plaque volume are more likely to rupture. 41 Studies have also shown that LDL levels are closely associated with the stability of atherosclerotic plaque. Oxidized LDL can not only stimulate the production of adhesion molecules by endothelial cells but can also cause the adhesion and aggregation of monocytes and macrophages, resulting in inflammatory reactions. Macrophages attached to the damaged endothelium can also phagocytose ox-LDL to form foam cells, and the substances released after the foam cells burst are important components of the lipid core. 42 In addition, ox-LDL can also be used as an antigen to stimulate the body to produce antibodies. Studies have found that the levels of anti-oxidant LDL antibodies are significantly elevated in acute myocardial infarction and unstable angina pectoris, indicating that LDL is likely to shift the balance towards unstable plaque. 43
The relationship between microRNA and plaque stability
microRNAs are documented to be involved in various diseases and can also indirectly affect the stability of plaque by regulating the above factors. 44
MicroRNAs are associated with angiogenesis in atherosclerosis
Promote angiogenesis-associated microRNAs.

Inhibition angiogenesis-associated microRNAs.
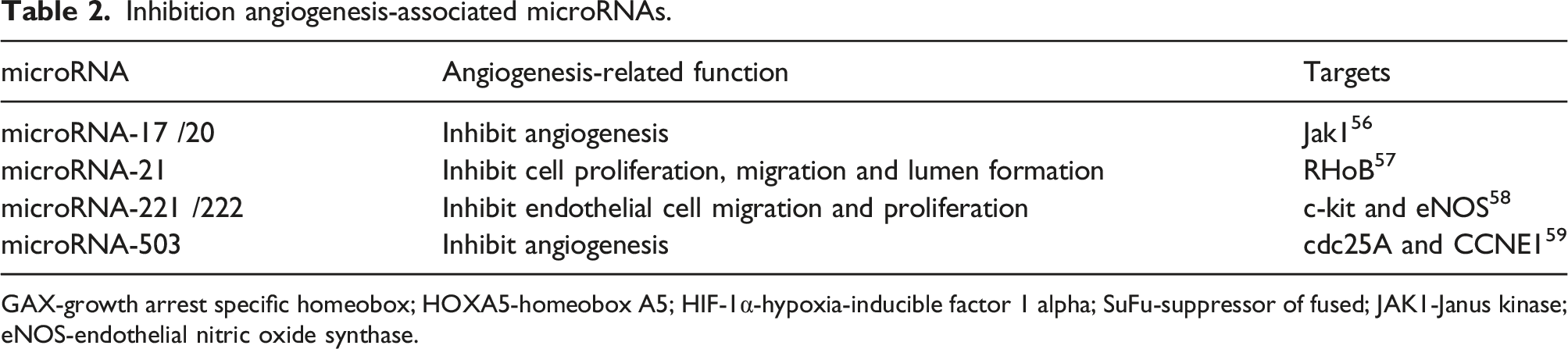
GAX-growth arrest specific homeobox; HOXA5-homeobox A5; HIF-1α-hypoxia-inducible factor 1 alpha; SuFu-suppressor of fused; JAK1-Janus kinase; eNOS-endothelial nitric oxide synthase.
MicroRNAs are associated with inflammatory responses in atherosclerosis
microRNAs associated with inflammation in atherosclerosis.

SRA-steroid receptor activator; TNF-6-tumor necrosis factor 6; IL-6-interleukin 6; ICAM-1-intercellular cell adhesion molecule; ROCK1-Rho-associated kinase 1; NF-κB-nuclear factor kappa-B; p-STAT3-p-signal transducers and activators of transcription.
MicroRNAs in vascular smooth muscle cells, macrophages, and endothelial cells
Vascular smooth muscle cells and macrophages play important roles in the stability of atherosclerotic plaques. MicroRNAs can indirectly affect the stability of plaques by regulating both these cell types. Studies have shown that miR-21 can promote the proliferation of vascular smooth muscle cells, while overexpression of miR-221 and miR-222 can promote the mitotic proliferation of these cells. miR-29 can target DNA methyltransferases responsible for the methylation of the MMP-9 and MMP-2 genes, influencing their expression and promoting the migration of vascular smooth muscle cells and accelerating plaque rupture. miR-155 can enhance the stability of atherosclerotic plaques, which may be related to inhibiting macrophage-mediated degradation of the plaque fibrous cap. 71 miR-124 can inhibit the differentiation of monocytes into macrophages and reduce the risk of plaque rupture by targeting the inhibition of CCAAT enhancer binding protein α. 72 microRNA-22 is thought to affect phenotypic changes by influencing the expression of three genes, namely, MECP2 (methyl CpG binding protein 2), HDAC4 (histone deacetylase 4), and EVI1 (ecotropic viral integration site 1). microRNA-22 influences changes in smooth muscle cells, from contractility to synthesis, most likely through the inhibition of its target genes MECP2, HDAC4, and EVI1. 73 MicroRNAs can also accelerate endothelial cell senescence by affecting endothelial cell function, a phenomenon that has the potential to exacerbate the development of atherosclerosis. In addition, microRNAs can also control the inflammatory state of blood vessels by affecting the activation and infiltration of leukocytes in the vessel walls. Studies have shown that inhibition of miR-126 leads to increased expression of the pro-inflammatory TNF-α which increases NF-κB and stimulates VCAM-1 activity, thereby increasing leukocyte-endothelial cell interactions and thus contributing to the development of atherosclerotic lesions.74,75 In addition, miR-19 was found to inhibit the activity of SOCS3 in perivascular adipose tissue, promote the secretion of inflammatory cytokines and the invasion of macrophages into the endothelial cell layer, and promote the progression of atherosclerotic lesions. 76
MicroRNAs and lipid metabolism
Lipids are closely associated with atherosclerosis, and the concept of lipoprotein dysregulation in the pathogenesis of atherosclerosis has been widely recognized. This is shown by the establishment of animal models of atherosclerosis through the feeding of high-fat diets. Studies have shown that unstable atherosclerotic plaques often have large lipid cores, indicating that lipid is also a factor affecting the stability of atherosclerotic plaques. microRNAs can regulate lipid metabolism. When the body is subjected to various stimuli, the level of lipid-related microRNA in the body may increase or decrease. These changes in lipid-related microRNAs can affect the activities and functions of various enzymes and factors in lipid metabolic pathways, thus influencing lipid metabolism. microRNA-122 is the first microRNA that has been found to be able to regulate fat metabolism. 77 Deficiencies in enzymes related to fat metabolism in miR-122-deficient mice affect lipid synthesis. Furthermore, miR-33 has been shown to play a significant role in fat metabolism, where it regulates anti-Saccharomyces cerevisiae antibody gene targeting and ni man horse disease gene 1 expression to influence cholesterol metabolism pathways, as well as influencing beta oxidation-related gene expression levels to affect the fatty acid and three acyl glycerin metabolic pathways. 78 In addition, miR-370, miR-103, miR-107, miR-758, and miR-106b were all found to regulate lipid metabolism. Disordered lipid metabolism can cause the formation of excessive levels of ox-LDL, leading to increased phagocytosis of the ox-LDL by macrophages and thus promoting the enlargement of the lipid core volume of atherosclerotic plaque.
Future directions
microRNAs are closely associated with the stability of atherosclerotic plaques and may thus represent a new target for predicting plaque stability. Overexpression or downregulation of several microRNAs can increase plaque stability, providing a new direction for the development of plaque stabilization drugs. However, the ways in which microRNAs modulate the stability of atherosclerotic plaques are complex, with different microRNAs having different regulatory sites. However, with advances in genetic engineering and medical technology, investigation into the regulatory mechanisms of microRNAs on the stability of atherosclerotic plaque will result in greater progress.
Conclusions
MicroRNAs play significant roles in the pathophysiology of atherosclerosis by regulating the levels of post-transcriptional gene expression, thereby affecting the levels of intracellular proteins. This can lead to imbalances in endothelial cells, smooth muscle cells, and white blood cells, thereby inducing and increasing the growth of atherosclerotic plaques.
Footnotes
Authors’ contributions
The author confirms being the sole contributor of this work and has approved it for publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
Data available within the article.