
Abstract
Objectives
To evaluate the ABO blood type and indirect bilirubin to predict early mortality in adults with severe COVID-19.
Methods
This retrospective observational study was conducted on 268 adult patients with laboratory-confirmed COVID-19 who had attended the intensive care unit (ICU), Quena general hospital and Luxor International Hospital, and other hospitals or centers for the treatment of COVID-19, during the period from January 2021 till December 2021.
Results
Relation between mortality and ABO group were highly significant, as we found non-O blood group with more risk of early mortality and intensive care unit admission ICU. There were significant differences between dead and alive cases as regards platelets, white blood cells WBCs (neutrophil, lymphocyte), albumin, liver enzymes aspartate transeferase (AST), alanine transferase (ALT), total direct and indirect bilirubin, creatinine, and urea.
Conclusion
There was a highly significant relation between dead cases and ABO blood group as between the O and non-O groups; also, group O was associated with less severe manifestations and or ventilation and less mortality in patients with severe COVID-19 infection. Direct bilirubin >0.5 was found to be the best predictor for mortality in cases with COVID-19 so indirect bilirubin may be considered a good protector against complications of the infection.
Introduction
Coronavirus pandemics (SARS-CoV-2) may cause the severe acute respiratory syndrome. 1
This virus infection has placed a tremendous burden on healthcare and public health systems worldwide. So many continuous efforts from researchers on biological characteristics, investigating potential usage as markers for COVID-19 risk and severity. Prediction or early detection of individuals who will get morbid, need to be hospitalized, or die could allow more specific public health measures and reduce the pressure on overburdened health systems which is called “risk factor epidemiology.” 2
SARS-CoV-2 is prone to genetic evolution resulting in multiple variants that may have different characteristics compared to its ancestral strains. Periodic genomic sequencing of viral samples is of fundamental importance, especially in a global pandemic setting. 3
One study stated that type A is the most common blood group (35.12%) in Egypt followed by O at 31.94%, then by B at 23.12%, while AB had the least at 9.74%. According to the Rhesus blood group (RH), 91.78% of the donor population were Rh positive and 8.22% were Rh negative. 4
Multiple studies have shown that the ABO blood group is an important independent risk factor for cardiovascular disease and venous thromboembolism (VTE). The risk of thrombosis is significantly reduced in blood group O compared to non-O individuals. 1 And more evidence demonstrates that COVID-19 is associated with significantly disordered hemostasis and the effect of thrombosis through the lung vasculature contributes to acute respiratory distress syndrome (ARDS). 5
Genetic factors have a great influence on the outcome of SARS which have been studied frequently. 6 Since O blood group individuals were shown to have very low risks of infection compared to non-O individuals. 7 Histo-blood group antigens are present not only on erythrocytes but also on many epithelial cells, which are their main site of expression. 8 Since SARS-CoV replicates in lung and respiratory tracts epithelial cells and also the digestive tracts that can express ABH carbohydrate epitopes, scientists found that the S protein of virions produced by either A or B persons could be decorated with A or B carbohydrate epitopes, respectively. Natural anti-A or -B antibodies from blood groups O, B, and A persons could bind to the S protein and block its interaction with ACE2, thereby preventing infection. 9
Bilirubin level is a universally accepted marker for monitoring liver damage. Patients who have elevated serum bilirubin usually get worse prognoses and more severe disease. 10
Like alveolar type II cells, bile duct epithelial cells have ACE2 receptors. However, hepatocytes may express ACE2 receptors at 0.2 concentration found in bile duct epithelial cells. These findings suggest that bile duct epithelial cell damage may represent another mechanism of liver tissue injury. 11
The goal of this research was to evaluate the ABO blood type and indirect bilirubin to predict early mortality in adults with severe COVID-19.
Methods
An observational study was conducted on 268 adult patients with laboratory-confirmed COVID-19 who were recruited retrospectively at the intensive care unit (ICU), Quena general hospital and Luxor International Hospital, and Menoufia University Hospitals during the period from January 2021 to December 2021.
All patients were subjected to standard controlled care protocol for COVID-19 infection according to guideline recommendations of the World Health Organization (WHO).
All patients with severe COVID-19 included in this study were divided into two groups: Group A: survivor adult COVID-19 patients. Group B: non-survivor adult COVID-19 patients
Ethical consideration
Institutional Research Board (IRB); approval of the study protocol obtained by Ethical Scientific Committee of Menoufia faculty of medicine (No. 1483/22-1-2022) and with the Helsinki Declaration of 1975, entitled, “Blood group O and indirect bilirubin are associated with lower, early COVID-19 – related mortality” also, Quena general hospital and Luxor International Hospital local ethical committee dated 24-1-2022.
All participants were volunteers. Informed written consent was taken from all patients or relatives (if the patient was unable to inform or write consent) after explaining the aim of the study.
Inclusion criteria
All patients (> 18 years), laboratory-confirmed COVID-19, and severe or critical COVID-19. The diagnosis of COVID-19 was created according to the definition established by World Health Organization (WHO) interim. 12
According to the level of lymphocyte, d-dimer, High sensitivity cardiac troponin T and I (hsCTnI), and high sensitivity C-reactive protein (hs-CRP), we classified patients with severe COVID-19 into subgroups. For each factor, cut points used to define a high level were as follows: Lymphocyte 21 μg/mL, hs-CTnI >15.6 pg/mL, and hs-CRP >100 mg/L. The high-risk group indicated an elevation in two or more factors, while the low-risk group indicated an elevation in one or no factors.
We retrospectively collected information from all patients including demographic data (age, sex, past, and present history…etc.), clinical characteristics, vital signs, ABO blood type, and laboratory findings.
Blood routine test; complete blood count CBC, albumin, globulin, aspartate aminotransferase, alanine aminotransferase, total bilirubin, direct bilirubin, creatinine, blood urea nitrogen, lactate dehydrogenase LDH. Infection-related biomarkers (procalcitonin, ferritin, hs-CRP).
Exclusion criteria
1. Patients under the age of 18 years old 2. Patients with malignancy 3. Pregnant females 4. Patients with chronic liver or kidney diseases 5. Patients with any other signs of infections rather than COVID-19 infection
Study outcomes
The study outcomes collected from reviewing medical records mainly consisted of the following: ICU early mortality within 7 days, patients developed multiorgan failure, time from illness onset to ICU admission, time from illness onset to death or discharge, SARS-CoV-2 RT-PCR test.
Statistical analysis
Statistical analysis A software tool was used to examine all statistical analyses (SPSS 22.0 for Mac; SPSS Inc., Chicago, IL, USA). Visual (histograms and probability plots) and analysis (Kolmogorov–Smirnov, and Shapiro–Wilk tests) approaches were used to evaluate if the data were regularly distributed. Numbers and proportions are used to represent different variables. The mean and standard deviation are used to represent the dependent variable. Because all ongoing measures were normally distributed, the unpaired sample t-test was utilized to analyze quantitative data. The factors of increased primary patency (PTA) after 1 year of PTA were determined using logistic regression analysis. The cut-off which discriminates between survivor and non-survivor was used. The variables used in the regression were respiratory rate (RR), pulse rate (PR), O2 saturation, international normalized ratio (INR), activated partial thromboplastin time (PTT), D-dimer, platelets, lymphocytes, aspartate transferase (AST), alanine transferase (ALT), total bilirubin (mg\dl), indirect-bilirubin (mg\dl), creatinine, blood urea nitrogen BUN (mmol/l), treatment given, and lastly, the invasive mechanical ventilation. A statistically substantial p-value of < 0.05 was used.
Result
Our study was conducted on 268 adult patients with laboratory-confirmed COVID-19.
Cases according descriptive data (n = 268).

Correlation between early mortality and demographic, clinical data, laboratory investigations and treatment given (n = 268).

χ2: Chi square test: Student t-test; ICU: intensive care unit.
p: p value for association between different categories.
*Statistically significant at p ≤ .05.
The cut off which discriminate between survivor and non-survivor was used.
Total bilirubin (mg/dl), Direct bilirubin (mg/dl), Indirect-bilirubin (mg/dl), partial thromboplastin time PTT (sec), D-dimer (pg/ml), lactate dehydrogenase LDH (u/l)), C-reactive protein CRP (mg/l), Ferritin (μg/ml), Procalcitonin (pg/ml), hemoglobin Hb (gm/dl), white blood cells WBCs (*103/ml), Platelet (*103/ml), Neutrophil (*103/ml), Lymphocyte (*103/ml), Albumin (mg/dl), AST (U/L), ALT (U/L), Creatinine (md/dl), blood urea nitrogen BUN (mmol/l).
From Table 2, the cut-off which discriminates between survivor and non-survivor was used. The variables affecting mortality were respiratory rate (RR), pulse rate (PR), O2 saturation, international normalized ratio (INR), activated partial thromboplastin time (PTT), D-dimer, platelets, lymphocytes, aspartate transferase (AST), alanine transferase (ALT), total bilirubin (mg\dl), indirect-bilirubin (mg\dl), creatinine, blood urea nitrogen BUN (mmol/l), treatment given, and lastly, the invasive mechanical ventilation. The cut-off level discriminates between survivor and non-survivor. Then, the univariate and multivariate logistic regression analysis was used showing that the total bilirubin hazard ratio was 0.182 in dead cases than alive, the indirect bilirubin hazard ratio was 894.2 in dead cases than alive cases, and D-dimer was 0.039 in died cases than alive cases.
Prognostic performance for total bilirubin to predict early mortality, direct-bilirubin to predict early mortality, indirect-bilirubin to predict early mortality.

AUC: Area Under a Curve; p value: Probability value; CI: Confidence Intervals; PPV: positive predictive value; NPV: negative predictive value.
*Statistically significant at p ≤ .05.
Univariate analysis for the parameters affecting early mortality.
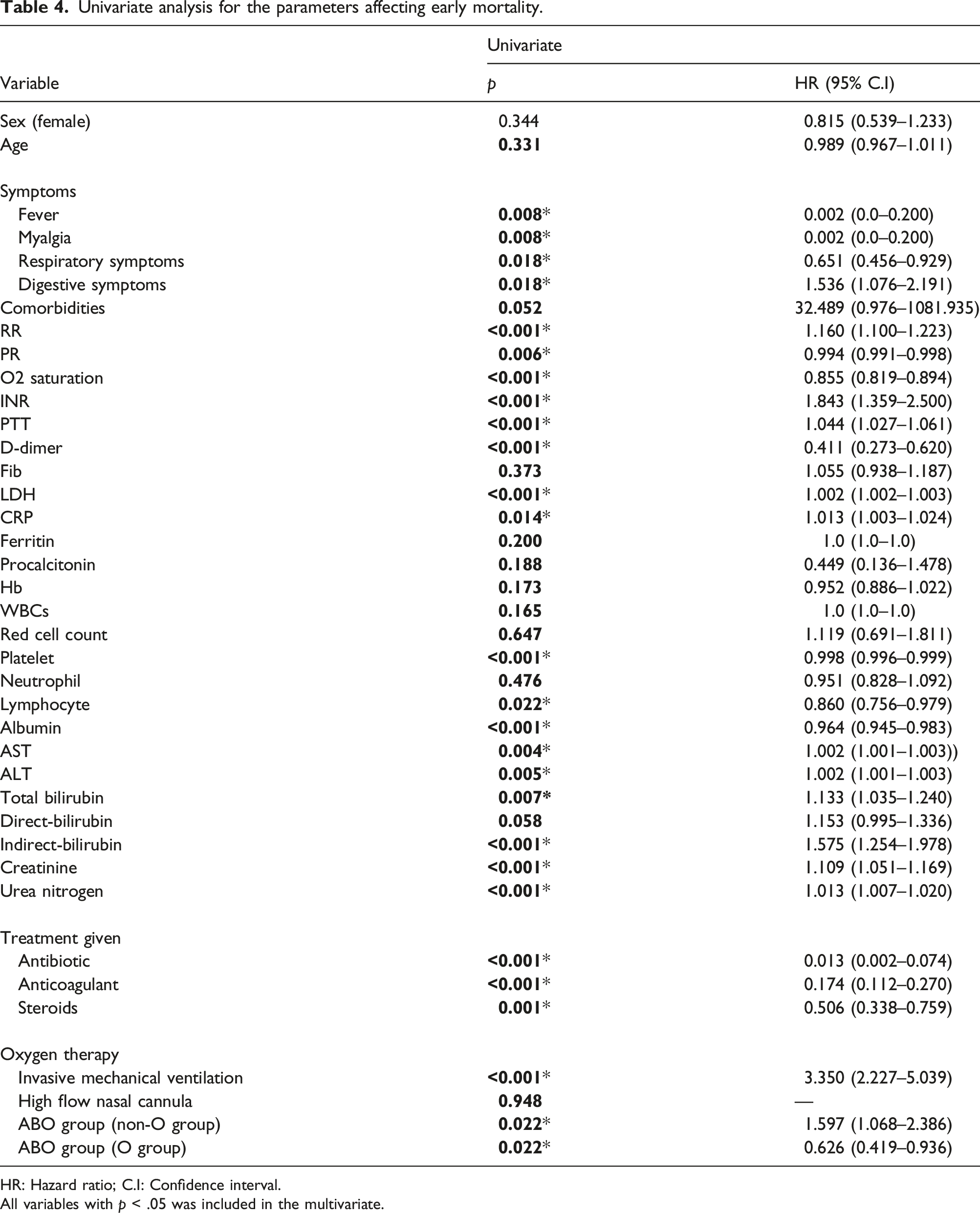
HR: Hazard ratio; C.I: Confidence interval.
All variables with p < .05 was included in the multivariate.
Univariate and multivariate logistic regression analysis for the parameters affecting early mortality.

HR: Hazard ratio; C.I: Confidence interval.
aAll variables with p < .05 was included in the multivariate.
*Statistically significant at p ≤ .05.
Discussion
For more than 2 years, several articles demonstrated an association between the ABO blood group and COVID-19. These include papers by Zhao et al., 13 Zietz et al., 14 Zeng et al. 15 Li et al., 5 and Wu et al., 16 all agreeing that group A individuals would have a higher risk of becoming infected, and group O individuals would have a lower risk. 17
As regards ABO blood group distribution among our cases, there were 32% had O blood group while 68% were non-O blood group. Survivors have significantly more O blood group (p < .001) and this was consistent with Du and his colleagues, 18 who suggested that individuals with blood group O may be less susceptible to SARS-CoV-2. Also, Zhao and his colleagues 13 found that blood group A was associated with an increased risk, whereas blood group O was associated with a decreased risk.
Reports from Muñiz-Diaz and others observed a significant difference in the ABO blood group distribution (p = .0023): blood group A was more common among infected patients, standing at the limit of statistical significance, and group O was significantly less prevalent, proving the expected protective effect. 17
Against our results, Vázquez-Medina et al., 19 reported that group O was the most frequent blood type among 1999 patients (84.3%), followed by group A (11.3%), B (3.5%), and AB (0.72%). Blood group A was associated with a lower hazard of death among COVID-19 patients compared with group O (adjusted HR = 0.72, 95% IC 0.55–0.95, p = .02). Groups B, AB, and RhD were not significantly associated with the outcome. Also, the study done by Kanderet al., 20 reported that ABO blood type and RhD status do not appear to influence mortality or morbidity in a general critically ill patient population. These findings should be interpreted with caution considering the high heterogeneity found between the studies when analyzing the risk of infection and the low or very low quality of the evidence.
SARS-CoV-2 envelope and also, SARS-CoV-2 S protein resembles A-like antigens expressed on the cells of group O individuals. So naturally occurring anti-A antibodies are produced and have a role in the prevention of infection by binding, blocking the interaction between the SARS-CoV-2 S protein and ACE2 receptor, which may prevent viral entry into the lung epithelium while group A individuals have increased ACE-1 activity which may lead to increased COVID-19 severity and have increased von Willebrand factor (VWF) and factor VIII levels which may lead to increased COVID-19 severity. 21
As regards the total, direct, and indirect bilirubin and their relation to COVID-19 severity, we found that the median values of total (1.6 vs 2.2), direct (0.5 vs 0.9), and indirect (1.1 vs 1.3) bilirubin were significantly higher among no survivor group, which was consistent with Sapha and Aisha, 21 who suggested that mild hyperbilirubinemia could be led to a beneficial “adapt and response” during sepsis in particular and critical illness in general.
Also, Duc et al., 22 observed that the serum bilirubin level increased in the two-hit + bilirubin group (approximately 0.22 mg/dL ± 0.04) compared with the same group (0.03 mg/dL ± 0.02) and two-hit group (0.13 mg/dL ± 0.03). These levels are still normal range (<0.5 mg/dL). Thus, the mild hyperbilirubinemia in the two-hit + bilirubin group may be a positive adaptive.
You-Fan et al., 23 reported that the relationships between serum bilirubin concentrations and essential trace elements status have also been revealed in an adult population since serum bilirubin maintains anti-inflammatory, anti-oxidative, and immunosuppressive features even in the general population. Therefore, serum bilirubin is a promising biomarker to assess the severity and prognosis of certain diseases.
As regards, early ICU mortality within 7 days was 34.7% among included cases, while the death rate was 58.2% among included cases of the study during hospitalization. While in the meta-analysis by Dessie and Zewotir, 24 showed that the pooled prevalence of mortality among hospitalized patients with COVID-19 was 17.62% (95% CI 14.26–21.57%, 42 studies, and 423,117 patients). Older age has shown an increased risk of mortality due to coronavirus and the pooled odds ratio and hazard ratio were 2.61 and 1.31, respectively.
The better prognosis and less death were in the O group phenotype and this may be explained by a prospective study at two different moments during the hospital stay in COVID-19 patients, which confirmed both lower rates of hospital admission and a lower risk of intubation or death in the O blood group. This was associated with higher levels in all statistically significant cytokines, except for hepatocyte growth factor (HGF), at the first moment, and a consequent significant drop after 6 days of hospital stay. Those findings would also explain an early and effective activation of the immune response in the O blood group, associating a rapid viral clearance of the viral infection. 25
We found that there was a highly significant relation between dead cases and ABO. This may be due to the implication of the affinity of viral S protein and its adaptation to ACE2 receptors which was demonstrated in a study, (by Li and others 2005), on SARS-CoV which might be the same for COVID-19. They also compare S proteins of SARS-CoV isolated during the 2002–2003 SARS outbreak and during the much less severe 2003–2004 outbreak, and from palm civets, a possible source of SARS-CoV found in humans. All three S proteins bound to and utilized palm-civet ACE2 efficiently, but the latter two S proteins utilized human ACE2 markedly less efficiently than that obtained during the earlier human outbreak. 26
Also, in line with our results, the study by Mammen et al., 27 reported that there was a statistically significant correlation between mortality and invasive ventilation, duration of invasive ventilation, and hospital stay as we found that there was a significantly higher in invasive mechanical ventilation (58% vs 0%) among died cases but noninvasive mechanical ventilation was significantly lower in non-survivors (41% vs 82%), p-value < .001.
A conflicting report from Zietz and his colleagues 14 found Type A had a lower risk of intubation and death compared with types AB and O. Only type B had inconsistent effects between intubation and death—type B increased risk of intubation and decreased risk of death compared to type O.
As well, Grasselli et al., 28 reported that the need for invasive or noninvasive mechanical ventilation was associated with mortality.
The current study showed that the mean age among included cases was 58.13 years with a male predominance of 64.9% with statistically significant differences between survivors and non-survivor.
Our findings were supported by Vázquez-Medina et al., 19 who evaluated 2369 patients; from them, a total of 684 (28.8%) patients died during hospitalization. They found that there were significant differences between survivor and non-survivor as regard sex and age also, the study by Alamdari and his colleagues, 29 enrolled 396 survived and 63 non-survived patients with the average age in the expired group was significantly higher compared to the discharged group; and in total, the men were hospitalized more often than women.
While Martins-Filho et al., 30 enrolled 1207 patients and revealed a statistically non-significant relation between mortality and gender and there was a statistically significant relationship between mortality and age which was against our results.
Consistent with our results, the systematic review and meta-analysis by Dessie and Zewotir, 24 enrolled 42 studies with a total of 423,117 patients and reported that older age has shown an increased risk of mortality due to coronavirus and the pooled odds ratio and hazard ratio (pHR) were 2.61 (95% CI 1.75–3.47) and 1.31 (95% CI 1.11–1.51), respectively. A significant association was found between COVID-19 mortality and males. Furthermore, risk factors associated with severity and death in COVID-19 patients by Du et al., 18 who enrolled a total of 17 articles were included and reported that the risk factors associated with severe illness and death were age and sex.
We found that 67.5% of cases had a fever, 67.5% had myalgia, 64.5% had respiratory symptoms, and 35.8% had digestive symptoms. There was a significantly higher incidence of fever and myalgia among cases who died with p < .001. Our results were supported by Mammen et al., 27 who reported that the most common presenting symptoms were shortness of breath (91.6%), fatigue (78.7%), cough (68.5%), and fever (35%). The frequency of shortness of breath, cough, and fatigue was similar in survivors and non-survivors; however, the presence of fever at admission was significantly associated with death.
In the current study, 65.7% of cases had comorbidities and 34.3% were free, most common comorbidities were HTN in 54.5%, asthma in 34.1%, and DM in 29%. There were significantly higher comorbidities among cases who died with a p-value < .001. In agreement with our results, Grasselli et al., 28 revealed that there is a statistically significant relationship between mortality and the presence of either comorbid diabetes or hypertension. As well, the systematic review and meta-analysis by Du et al., 18 revealed that diabetes and hypertension are more likely to develop severe illness or death after being infected with the coronavirus, diabetes, and hypertension. Also, Dessie & Zewotir, 24 reported that the risk of mortality among hospitalized COVID-19 patients is highly influenced by patients with diabetes and hypertension.
Regarding the prognostic performance for different parameters to predict mortality, our analysis revealed that area under the curve (AUC), cut-off, sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV) of total bilirubin, direct bilirubin, indirect bilirubin in predict mortality were (0.767, >1.6, 80.13, 74.11, 81.2, 72.8), (0.897, >0.5, 80.13, 74.11, 81.2, 72.8), (0.681, >1.1, 80.13, 74.11, 81.2, 72.8), respectively. AUC, cut off, sensitivity, specificity, PPV, NPV of D-dimer, serum ferritin in predict mortality were (0.630, >0.9, 41.67, 56.25, 57.0, 40.9), (0.585, >980, 60.26, 48.21, 61.8, 46.6), respectively. It can be seen that direct bilirubin >0.5 was the best predictor for mortality in cases with COVID-19.
By Univariate analysis, significant parameters affecting mortality were symptoms, respiratory rate, pulse rate, O2 saturation, INR, PTT, D-dimer, LDH, CRP, platelet, lymphocyte, AST, ALT, total bilirubin, indirect-bilirubin, creatinine, BUN, treatment given, invasive mechanical ventilation, and ABO group (O and non-O group). As regards multivariate analysis and hazard ratio for factors affecting mortality, the indirect bilirubin hazard ratio was 1412.771 in dead cases than alive, ABO group (non-O group) hazard ratio was 6.326 in dead cases than alive cases, and ABO group (O-group) was 0.158 in died cases than alive cases.
Also, Martins-Filho et al., 30 revealed that the univariate analysis identified eight covariates as candidates for the multivariate model, including age >65 years, non-HIV immunosuppressive disease, obesity, infectious disease, kidney disease, heart disease, hypertension, and diabetes. The standard multivariate regression analysis showed that COVID-19 mortality was significantly associated with age >65 years, following underlying medical conditions: infectious disease, kidney disease, and heart disease.
Limitations
1. The power analysis for sample size calculation wasn’t done. 2. The small number of patients included. 3. Not using a control group of volunteers without COVID-19 infection. 4. As it is a retrospective one, we cannot assess the inflammatory status or cytokine storm by investigations.
Conclusion
There was a highly significant relation between dead cases and ABO blood group as between the O and non-O groups. Also, group O was associated with less severe manifestations and or ventilation and less mortality in patients with severe COVID-19 infection. Also, direct-bilirubin <0.5 was found to be the best predictor for early mortality in adult cases with COVID-19, so indirect bilirubin may be considered a good protector against complications of the infection.
Footnotes
Author contributions
Sabry Abdullah Shoeib made substantial contributions to the conception and share the design of the work; Alaa Efat, Ali Mohamed ElKholy, Osama Saied Hussein Aboelela, and Doaa Mohamed Elshamy made substantial contributions to the conception, and design of the work; the acquisition, analysis, interpretation of data; the creation of new software used in the work, had drafted the work and substantively revised it. All authors have read and approved the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Approval of the study protocol obtained by Ethical Scientific Committee of Menoufia faculty of medicine (No. 1483/22-1-2022) and with the Helsinki Declaration of 1975, entitled “Blood group O and indirect bilirubin are associated with lower, early COVID-19 – related mortality” also, Qena general hospital and Luxor International Hospital local ethical committee dated 24-1-2022.
Informed consent
All participants were volunteers. Informed written consent was taken from all patients or the legally authorized relative (in the event that the patient was unable to inform or write a consent) after explaining the aim of study.