
Abstract
Objectives
Acute exacerbations (AEs) of chronic obstructive pulmonary disease (COPD) can affect health status, hospitalization and readmission rates, and disease progression. This study aimed to identify independent markers associated with COPD AEs.
Methods
This study included male patients with COPD and collected data regarding their AEs and baseline clinical parameters.
Results
We included 149 male patients. Among them, 58 were included in the year 0 high-AE group and 91 in the low-AE group. Multivariate analysis revealed that the high-AE group had higher white blood cell count, lower serum albumin level, and post-bronchodilator (BD) forced expiratory volume in one second (FEV1) (%) with a combined receiver operating characteristic curve (ROC) of 0.721 (p < 0.001). Additionally, 34 patients were included in the year 1 high-AE group and 70 in the low-AE group (p < 0.001). Multivariate analysis revealed that the high-AE group had higher platelet count, positive asthma history, and lower pre-BD FEV1 (%) with a combined ROC of 0.782 (p < 0.001).
Conclusion
In male patients with COPD, baseline white blood cell count, albumin level, and post-BD FEV1 (%) were correlated with year 0 AE; on the other hand, baseline platelet count, positive asthma history, and pre-BD FEV1 (%) were associated with year 1 AE.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) caused more than three million deaths in 2012 and is in the top three causes of death worldwide. 1 Four clinical phenotypes (groups A–D) can be identified according to the severity of airflow limitation, results of symptom questionnaires, and frequency of annual acute exacerbation (AE). Frequent exacerbators are characterized by rapid deterioration of lung function, resulting in reduced physical activity, poorer quality of life, and an increased mortality risk.1–3
COPD exacerbations are defined as acute deterioration of respiratory symptoms requiring additional therapy and affecting health status, hospitalization and readmission rates, and disease progression. 1 Mortality after admission due to COPD AE could be up to 26.2% after 1 year and 64.3% after 5 years. 4 Mortality rate and exacerbation risk was highest in Global Initiative for Chronic Obstructive Lung Disease (GOLD) group D patients according to analysis of England Clinical Practice Research Datalink and Hospital Episode Statistics database. 5 A review article about AE of COPD conducted by Mathioudakis et al. 2 summarized several factors associated with AE, including C-reactive protein (CRP), fibrinogen, white blood cell (WBC) count, pulmonary artery to aorta diameter ratio, dyspnea score, circulating lung tissue injury biomarkers, eosinophilia, troponin-I, N-terminal-pro-brain natriuretic peptide. The author also mentioned an analysis on 119 blood biomarkers based on COPDGene and SPIROMICS cohort which showed limited values of blood markers in predicting AE, but this may be due to patient population bias. Considering these diverse findings, this study aimed to identify the independent markers associated with COPD AEs.
Materials and methods
This is an observational and prospective study. We screened 364 patients with a history of COPD or suspected COPD from the Pulmonary Clinic of Kaohsiung Chang Gung Memorial Hospital during May 2013 and July 2017. This study was approved by the Institutional Review Board of Chang Gung Memorial Hospital (IRB: 103–3366B). Written informed consent was obtained from each participant. Definition, inclusion and exclusion criteria, and AE were defined according to GOLD guidelines. Data regarding patients’ baseline characteristics, chest radiograph, and pulmonary function test were collected at enrollment and 1 year after. Both lung function tests and blood sampling were performed at stable disease, which must be more than 4 weeks after last exacerbation. We didn’t interfere with each doctors’ clinical decision, but we routinely took chest radiograph if COPD AE was suspected.
This study included patients diagnosed with COPD based on the following characteristics: male, age >40 years, smoking history ≥10 pack-years, and post-bronchodilator (BD) FEV1/forced vital capacity (FVC) < 70%. BD responsiveness was defined a post-BD improvement in FEV1 of >200 ml and 12%. Patients with a history of tuberculosis, bronchiectasis, lung cancer, or recent admission (≤4 weeks) were excluded.
COPD AE was defined as worsening of at least two major symptoms (dyspnea, sputum volume, and sputum purulence). Moderate AE was defined as administration of oral antibiotics or systemic steroid. Severe AE was defined as emergency room stay for >24 h or admission.
Among the 364 patients, 210 met the inclusion criteria. Furthermore, 61 patients were excluded due to suspected asthma–COPD overlapping syndrome as defined by the following characteristics: (I) COPD diagnosis; (II) positive BD responsiveness; and (III) blood eosinophil level >3%; or history of atopic diseases, including asthma, allergic rhinitis, or atopic dermatitis.
Dyspnea severity was surveyed by using modified Medical Research Council (mMRC) score and COPD assessment test (CAT) score.6,7 Ratio indexes of baseline blood examination were defined as below. The lymphocyte-to-monocyte ratio (LMR) was calculated by dividing the lymphocyte count by the monocyte count. The neutrophil-to-lymphocyte ratio (NLR) was calculated by dividing the neutrophil count by the lymphocyte count. Systemic immune–inflammation index (SII) was calculated as follows: platelet count × neutrophil count/lymphocyte count. 8 The platelet-to-lymphocyte ratio (PLR) was calculated by dividing the platelet count by the lymphocyte count. Systemic inflammation response index (SIRI) was calculated as neutrophil count × monocyte count/lymphocyte count. 8
Statistical analysis
Statistical analyses were performed using SPSS version 21.0 (SPSS Inc., Chicago, IL, USA). Categorical variables were compared using the Chi-square test and presented as frequency with percentage. Continuous variables are presented as median with interquartile range and were compared using the non-parametric Mann–Whitney U-test. To adjust for confounding factors, stepwise multivariate analysis was performed using binary logistic regression analysis. Receiver operating characteristic (ROC) curve was used to predict accuracy of candidate predictor. Independent variables were combined to produce a prediction score by a formula based on binary logistic regression to increase predictive accuracy. Statistical significance was set at a p-value of <0.05.
Results
Patient and clinical characteristics
A total of 149 male patients with COPD were included in the final analysis. The flowchart of participants is shown in Figure 1. Inclusion and exclusion flowchart of patient selection. ACOS: asthma–COPD overlapping syndrome; BD: bronchodilator; COPD: chronic obstructive pulmonary disease; FEV1: forced expiratory volume in one second; FVC: forced vital capacity.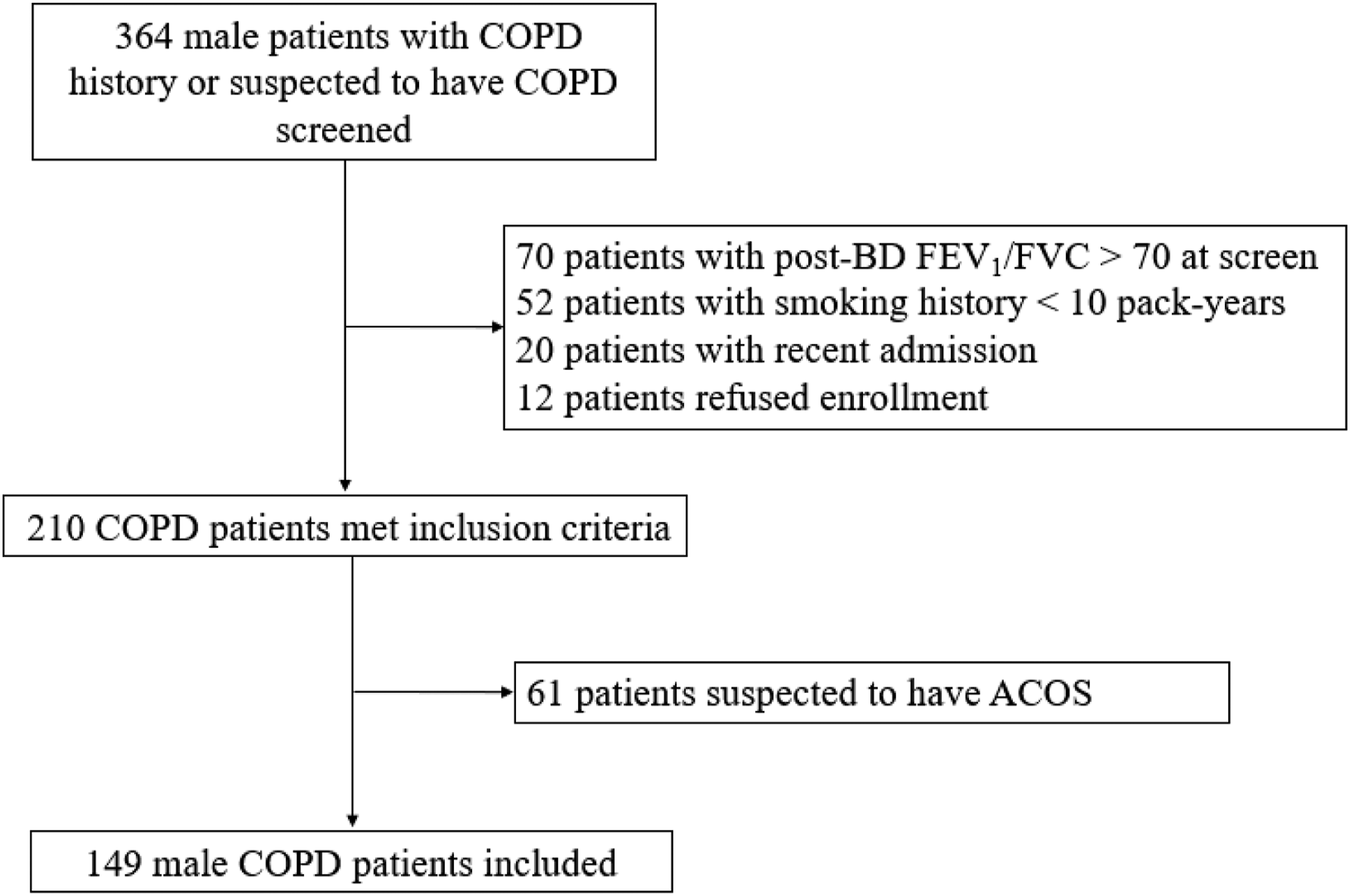
Comparisons of baseline clinical parameters between year 0 high-AE group and low-AE group.

6-MWT: 6-min walk test; AE: acute exacerbation; ACCI: age-adjusted Charlson Comorbidity Index; AEC: absolute eosinophil count; BD: bronchodilator; BMI: body mass index; CAT: COPD assessment test; FEF25%–75%: forced expiratory flow between 25% and 75% of vital capacity; FEV1: forced expiratory volume in one second; FVC: forced vital capacity; ICS: inhaled corticosteroids; LAMA: long-acting muscarinic antagonists; LABA: long-acting beta2-agonists; LMR: lymphocyte-to-monocyte ratio; mMRC: modified Medical Research Council; NLR: neutrophil-to-lymphocyte ratio; PLR: platelet-to-lymphocyte ratio; PLT: platelet; RBC: red blood cell; SII: systemic immune–inflammation index; SIRI: systemic inflammation response index; WBC: white blood cell. *LAMA+LABA+ICS
During year 0, the high-AE group had higher blood WBC count, neutrophil differential count, NLR, SII, SIRI, mMRC score, and CAT score than the low-AE group. However, the high-AE group revealed lower lymphocyte percentage, LMR, red blood cell (RBC) count, albumin level, pre-BD FVC (%), pre-BD FEV1 (%), pre-BD forced mid-expiratory flow (FEF25%–75%) (%), post-BD FVC (%), post-BD FEV1 (%), and post-BD FEF25%–75% (%) in year 0. Additionally, during year 0, the high-AE group required more long-acting beta2-agonist (LABA)–inhaled corticosteroids and less single LABA inhalers for maintenance therapy.
Comparisons of baseline clinical parameters between year 1 high-AE group and low-AE group.

6-MWT: 6-min walk test; AE: acute exacerbation; ACCI: Age-adjusted Charlson Comorbidity Index; AEC: absolute eosinophil count; BD: bronchodilator; BMI: body mass index; CAT: COPD assessment test; FEF25%–75%: forced expiratory flow between 25% and 75% of vital capacity; FEV1: forced expiratory volume in one second; FVC: forced vital capacity; LMR: lymphocyte-to-monocyte ratio; mMRC: modified Medical Research Council; NLR: neutrophil-to-lymphocyte ratio; PLR: platelet-to-lymphocyte ratio; PLT: platelet; RBC: red blood cell; SII: systemic immune–inflammation index; SIRI: systemic inflammation response index; WBC: white blood cell.
Stepwise multivariate analysis of independent factors associated with year 0 and year 1 high-AE groups.

AE: acute exacerbation; BD: bronchodilator; FEV1: forced expiratory volume in one second; WBC: white blood cell.
Performance of prediction score by ROC curve analysis
We performed ROC curve analysis of year 0 AEs by combining the three covariates albumin level, WBC count, and post-BD FEV1 (%) to produce a prediction score of year 0 AEs in a model formula using binary logistic regression analysis, as shown in Figure 2. ROC curves of prediction score of year 0 and year 1 AEs.AE: acute exacerbation; ROC: receiver operating characteristic.
Prediction score of year 1 AEs was performed by combining the three covariates platelet count, positive asthma history, and pre-BD FEV1 (%) using the same method. For prediction score of year 0 AEs, area under curve (AUC) was 0.721, 95% CI was 0.630–0.811, and p-value was <0.001. A cutoff point of Youden’s index for the probability of year 0 AEs was calculated at 0.443, with sensitivity and specificity of 0.586 and 0.857, respectively. AUC of year 1 AE prediction score was 0.782, with 95% CI of 0.687–0.878, and p-value of <0.001; Youden’s index was 0.524, with sensitivity and specificity of 0.824 and 0.700, respectively.
Discussion
In the current study, we identified hypoalbuminemia, leukocytosis, and lower post-BD FEV1 (%) as three independent risk factors associated with frequent exacerbation in the past 1 year, while thrombocytosis, positive asthma history, and lower pre-BD FEV1 (%) as independent predictors for frequent exacerbation in the next 1 year. Furthermore, by using the ROC curve analyses, we demonstrated that year 0 AE prediction score, which combines the former three independent risk factors, could accurately correlate with frequent exacerbation in the past 1 year, while year 1 AE prediction score, which combines the later three independent predictors, could accurately predict frequent exacerbation in the next 1 year.
Serum biomarkers associated with chronic obstructive pulmonary disease Acute exacerbations
COPD is a disease characterized by both chronic lung and systemic inflammation, which can worsen comorbidities. 1 Agustí et al. 9 found several systemic biomarkers in peripheral blood that are associated with all-cause mortality and exacerbation frequency in patients with COPD including WBC count, CRP, interleukin (IL)-6, IL-8, fibrinogen, and tumor necrosis factor-α. The ECLIPSE study identified different biomarkers correlated with different aspects of COPD; among them, fibrinogen level was correlated with symptoms, exercise capacity, exacerbation rate, and BODE index; further, low levels of vitamin D were correlated with emphysema, 6-min walk distance, airway reactivity, and Clara cell secretory protein-16 levels. 10 Stephen et al. summarized biomarkers of COPD, and serum markers including fibrinogen in association with AE risk, eosinophil count in prediction of inhaled corticosteroid therapy response were categorized as most viable candidates; other less viable candidates included club cell secretory protein 16, surfactant protein D, and soluble receptor for advanced glycation end products (sRAGE). 11 In both COPDGene and ECLIPSE cohort, sRAGE and CRP were associated with previous year total exacerbation frequency. 12 Regarding elements of peripheral blood complete blood count and differential count, COPD AEs were associated with decreased lymphocyte count and mean platelet volume (MPV) 13 and increased WBC and neutrophil count, platelet–monocyte aggregation, platelet reactivity, NLR, and PLR.10,13–16 Among them, NLR was positively correlated with severity of COPD AEs 17 and NLR > 5 strongly predicts mortality and longer hospital stay in patients hospitalized due to COPD AE. 18
In our study, a higher WBC count was associated with increased risk of year 0 AEs, which is consistent with those of previous studies.10,13 However, this was inconsistent with the reports of Hurst et al., 19 which found that increased WBC count was associated with year 1 AEs. This discrepancy may be due to the small number of patients in this study or other unknown confounding factors.
Additionally, we found that increased platelet count was independently associated with increased year 1 AEs. Malerba et al. found that the inflammation in COPD potentially causes endothelial dysfunction and platelet activation. Which may explain the increased 1 year AE risk in patients with increased platelet count. 20 In an analysis of COPDGene and SPIROMICS cohort, thrombocytosis was found associated with more previous exacerbations and more severe symptoms. 21 In addition to the number of platelet count, platelet function plays a role in COPD. To assess platelet function, previous studies used MPV, platelet–monocyte aggregation, and platelet reactivity using P2Y12 reactivity index, multiple electrode aggregometry, and optical aggregometry.13–15 Harrison’s et al. found that 1-year mortality risk after admission increased by thrombocytosis and decreased by antiplatelet therapy 22 ; considering this, platelet count is a potential marker of platelet aggregation and inflammation. Therefore, increased platelet count in COPD may represent increased platelet activation related to systemic inflammation, which is more severe during COPD AE. 22
Serum albumin level and chronic obstructive pulmonary disease
We found an association between hypoalbuminemia and year 0 AE frequency, which is consistent with the finding of Chen et al., 23 who reported hypoalbuminemia as a predictor of acute respiratory failure in patients with COPD. Previous studies found that albuminuria is associated with endothelial dysfunction, COPD severity, all-cause mortality, systemic inflammation, GOLD categories, and cardiovascular events.24-26 However, in these studies, the lack of serum albumin data affected the determination of the presence of hypoalbuminemia in patients with COPD. In our study, the urine albumin/creatinine ratio was not evaluated; therefore, hypoalbuminemia may have been influenced by urine albumin loss in addition to COPD severity. Further studies are needed to determine the relationship between hypoalbuminemia and COPD AE.
Asthma history and chronic obstructive pulmonary disease
In our study, positive asthma history was associated with year 1 AEs, but not with year 0 AEs. Among patients with COPD, a significantly large proportion of patients who present with symptoms of a chronic airway disease have features of both asthma and COPD, who are categorized as ACOS, and the prevalence rates have been reported between 15 and 55%. 27 ACOS patients experience more frequent AEs, poorer quality of life, more rapid decline in lung function, and higher mortality. 28 In addition to GOLD guidelines, different definitions for ACOS were proposed. In particular, Soler-Cataluña et al. used increase of post-BD FEV1 of ≥12% and 400 mL, sputum eosinophilia, and positive asthma history as major criteria. 28 On the other hand, Louie et al. 29 used physician diagnosis of asthma and COPD in the same patient, history of evidence of atopy, elevated total IgE level, age of ≥40 years, smoking habit of >10 pack-years, post-BD FEV1 of <80% predicted, and FEV1/FVC of <70%. To minimize the impact of ACOS related AEs in our study, we excluded patients suspected to have ACOS according to the criteria described in the materials and methods section. In our patient group, no significant difference was observed regarding BD response, absolute eosinophil count, and eosinophil percentage between the high-AE and low-AE groups.
At the end of year 1, a significant difference was observed between the number of patients from the year 0 high- and low-AE groups who remained in their respective groups in year 1 (19/38 [50%] and 51/66 [77.3%], respectively). Therefore, frequent AEs may be a predictor. In ECLIPSE study, a history of exacerbations was the most reliable predictor of future AE; others include declining FEV1, decreased quality of life, previous gastroesophageal reflux, and leukocytosis. 19 After 8-year follow-up report, year 1 frequent exacerbations still correlated with year 2 and year 3 frequent exacerbations. 30 Other parameters suggested to have association with future AE included pulmonary artery enlargement detected by computed tomography; combined elevation of CRP, fibrinogen, and leukocyte count; and ACCEPT model created by Adibi et al. 2 However, our multivariate analysis found no significant correlation between the number of year 0 and 1 AEs. This may be due to small sample size and 45 of 149 patients lost follow-up after year 1 in our study.
Despite the exclusion of patients suspected to have ACOS, an increased association remained between positive asthma history and year 1 AE risk, even after multivariate analysis. Therefore, in COPD patients with asthma history, careful evaluation of AE risk is warranted.
Summary of parameters associated with year 0 or year 1 Acute exacerbations
Among the three parameters associated with year 0 AEs in our study, lower albumin level was the most significant predictor. The association of WBC count and post-BD FEV1 (%) with COPD AE was validated in large cohort studies such as ECLIPSE 19 and ACCEPT model. 31 But the role of albumin in COPD AE is still uncertain. Previous studies suggested the role of albuminuria in COPD severity and GOLD categories,24–26 but didn’t mention the role of albumin in COPD. A large nationwide cohort study including 42,732 patients showed the correlation between hypoalbuminemia and acute respiratory failure in COPD patients, 23 but the cause of acute respiratory failure was not analyzed. These are indirect evidence and further studies are needed. In COPD patients with hypoalbuminemia, we need to evaluate if this is due to other diseases such as liver disease, nephrotic syndrome, etc. If albuminuria exists, careful evaluation of systemic inflammation related to COPD or other diseases is warranted since this is associated with all-cause mortality in COPD patient. 25
In predicting year 1 AE, a history of asthma was the most significant predictor in our study. The association of Pre-BD FEV1 (%) and year 1 AE was inconsistent with ECLIPSE study, 19 which used post-BD lung function parameters. This may be due to small sample size and lost follow-up patients in our study. Although we didn’t find articles about thrombocytosis and year 1 AE, thrombocytosis was found associated with previous exacerbations in COPDGene and SPIROMICS cohort. 21 As we stated in second limitation, a history of asthma was recorded according to patients, so bias do exist. In our study, the risk of year 1 AE was higher in COPD patients with asthma history, even after excluded patients suspected to have ACOS. Thus, we may need to titrate medications more carefully or follow-up more frequently in this patient group.
Our study has several limitations. First, medication use was only recorded if patients used the inhaler for >6 months; additionally, we were unable to ensure patient compliance or the exact timing of inhaler use. Second, asthma history was recorded if the patients claimed that they have been diagnosed by a physician; therefore, we were unable to confirm if the diagnosis was asthma, early COPD, or other conditions that mimic asthma. And some patients with COPD recognized their disease as asthma since they could not understand the difference between asthma and COPD. Although the history of heavy smoking exposure plus post-BD FEV1/FVC <70% does support the diagnosis of COPD, the possibility of chronic asthma with irreversible airway obstruction cannot be excluded. Third, sample size calculation was not done in our study, and sample size was small. Fourth, 45 of 149 patients lost follow-up after 1 year, this could affect the interpretation of our study results. Lastly, year 0 AEs were recorded based on medical or patient reports, which may affect the accuracy of year 0 AE frequency.
Conclusion
In conclusion, baseline WBC count, serum albumin level, and post-BD FEV1 (%) were correlated with year 0 AEs in patients with COPD with moderate accuracy. On the other hand, baseline platelet count, positive asthma history, and pre-BD FEV1 (%) were predictors of year 1 AEs with moderate accuracy.
Footnotes
Acknowledgments
We thank Prof. Sheng-Nan Lu, Prof. Hsueh-Wen Chang, Shin-Yi Chien, Chih-Yun Lin, and the Biostatistics Center, Kaohsiung Chang Gung Memorial Hospital for statistical work.
Author Contributions
Yu-Ping Chang, Shih-Feng Liu and Yung-Che Chen designed the research and data interpretation.
Yu-Ping Chang wrote the manuscript.
Yu-Mu Chen, Ya-Chun Chang, Wen-Feng Fang, Tung-Ying Chao, Chao-Chien Wu, and Huang-Chih Chang helped revise the manuscript.
Meng-Chih Lin helped revise the research.
All authors helped perform the research. All authors have read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Science and Technology, Taiwan (101-2325-B-002-064/102-2325-B-002-087/103-2325-B-002-027/104-2325-B-002-035/105-2325-B-002-030/105-2314-B-182A-092-MY3 to M.C. Lin) and from Chang Gung Memorial Hospital, Taiwan (CMRPG8D1572/CMRPG8F1641/CMRPG8I0151/CMRPG8F1321/ CMRPG8I0152 to Y.C. Chen). The funding body has no role in the design of the study and collection, analysis, and interpretation of data, or in writing the manuscript.
Ethics approval
This study was approved by the Institutional Review Board of Chang Gung Memorial Hospital (IRB: 103-3366B)
Informed consent
Written informed consent was obtained from each participant