
Abstract
The endothelial glycocalyx plays a critical role in the regulation of vascular structure and functions. Previous studies have demonstrated that sevoflurane, a volatile anesthetic, can preserve the endothelial glycocalyx in heart tissues against ischemia-reperfusion injury. However, little is known about the effects of sevoflurane pretreatment on the vascular structure and functions of liver tissues following ischemia-reperfusion injury. To this end, female Sprague-Dawley rats (n = 28) were anesthetized either with ketamine (80–120 mg/kg, i.p.) or with one minimum alveolar concentration (MAC) sevoflurane (2% v/v). Following in vivo hepatic ischemia procedure, the liver was isolated and reperfusion was produced. During the period of reperfusion, liver reperfusion samples were collected, and the concentrations of heparan sulfate and syndecan-1 (Syn-1), and the levels of aspartate aminotransferase (AST) and alanine aminotransferase (ALT) enzymes, were measured. The morphology of hepatocytes and endothelial glycocalyx were then assessed by using the light and electron microscopies, respectively. Ischemia-reperfusion increased the release of HS and Syn-1, and elevated the levels of ALT and AST in a time-dependent manner. However, sevoflurane pretreatment reduced the release of HS and Syn-1and attenuated the levels of ALT and AST, in a time-dependent manner, as compared with ketamine pretreatment. Furthermore, sevoflurane pretreatment decreased the shedding of endothelial glycocalyx and hepatocytes necrosis. Sevoflurane pretreatment preserved the endothelial glycocalyx in the liver tissue against ischemia-reperfusion injury. The effect appears to help protect hepatocytes against ischemia-reperfusion-induced necrosis.
Introduction
The endothelial glycocalyx is a carbohydrate-rich layer covering the vascular endothelium, with a thickness in the range of 0.4–0.5 μm. It is connected to the endothelium mainly through polymeric chains of proteoglycans and glycoproteins,1–3 thus forming a network containing various molecules including heparan sulfate and syndecan-1 (Syn-1).4,5 The endothelial glycocalyx interacts intensely and dynamically in vivo with all plasma constituents, such as plasma proteins and glycosaminoglycans. In effect, they form a functional endothelial surface layer (ESL) with a thickness exceeding 1 μm. 6
The endothelial glycocalyx plays a critical role in the regulation of vascular permeability. 7 The destruction of the endothelial glycocalyx increases vascular permeability to various macromolecules, proteins, and cells, as well as reduces capillary density and interrupts blood flow in the capillary bed. Importantly, some studies even indicate that damage to endothelial glycocalyx may trigger inflammatory response. 2 Hence, the protection or the restoration of damaged endothelial glycocalyx is a promising therapeutic aim in both the acute critical care setting and the management and treatment of chronic vascular conditions. 8
Previous studies have demonstrated that sevoflurane, a volatile anesthetic, can protect various organs or tissues against ischemia-reperfusion injury, including the brain, heart, intestine, and lung, in both humans and laboratory animals.9–14 Furthermore, sevoflurane can preserve the endothelial glycocalyx against ischemia-reperfusion injury in heart tissue. 10 Some studies examined the effects of sevoflurane pretreatment on hepatic tissues following the ischemia-reperfusion injury.12,13,15–18 The available data on this issue are, however, limited and often inconclusive. In particular, there is little information on the effect of sevoflurane pretreatment on the endothelial glycocalix.12,13 Therefore, the present study examined the effects of sevoflurane pretreatment on the endothelial glycocalyx in the liver tissue in rats.
Materials and methods
Animals
Female Sprague-Dawley rats (weight range, 360–450 g) were individually housed in a temperature- and humidity-controlled vivarium under a 12 h light/dark cycle. Rats had free access to rat chow daily with water ad libitum. The food was withheld for 12 h before the experiment, but free access to water was allowed. The local Institutional Animal Care and Use Committee approved all animal experiments. The housing and treatment of the rats followed the guidelines of the “Guide for the Care and Use of Laboratory Rats” (Institute of Laboratory Animal Resources, Commission on Life Sciences 2011).
Hepatic ischemia and reperfusion
Rats were anesthetized with either ketamine (80–120 mg/kg, i. p.) or 2% sevoflurane in a gas chamber for 30 min. These agents are found to induce patient to anesthesia equally quick, having very similar pharmacokinetics. 19
Sevoflurane in a humidified 30% oxygen carrier gas at 2–3 L/min was delivered to the chamber using an agent-specific vaporizer (Datex-Ohmeda, Madison, WI, USA). Rats were then placed on a heating pad and under a warming light to maintain the body temperature at approximately 37°C. Under aseptic conditions, a laparotomy was performed to access the liver for mobilization (after dividing ligamenture attachments). To prevent portal vein pooling, heparin (125 IU/kg) was administered intravenously.
Partial warm-hepatic ischemia was produced for 45 min by placement of vascular microclips across the hilum of the median and left lateral lobes. Sham animals were subjected to anesthesia, laparotomy, and mobilization of the liver only. After 45 min of ischemia, the liver was isolated and placed into 0°C ice-water mixture for 3 min. The liver was then suspended, and a catheter, which was connected to the perfusion device, was introduced into the portal vein. The perfusion rate was 30 mL/h of HLR (histidine, lactobionate, and raffinose) solution.
Experimental protocols
Four different protocols (n = 7 each) were used. In group A (Ketamine/No Ischemia), rats were anesthetized with ketamine, but no ischemia was introduced. In group B, rats were anesthetized with ketamine and ischemia was introduced (Ketamine/Ischemia). In group C, rats were anesthetized with sevoflurane, but no ischemia was introduced (Sevoflurane/No Ischemia). In group D, rats were anesthetized with sevoflurane, and ischemia was introduced (Sevoflurane/Ischemia).
Hepatic sample collection and analysis
Ischemia-reperfusion injury is a phenomenon in which cellular damage in a hypoxic organ is accentuated following the restoration of oxygen delivery.20–22 Ischemia-reperfusion injury in the liver is an important cause of damage occurring during surgical procedures and the common cause of graft dysfunction.23,24
Therefore, minimizing the adverse effects of ischemia/reperfusion injury could improve outcomes in liver surgery, increasing the number of patients who successfully recover from major liver surgery. Sevoflurane is logically selected for that perusal, due to its pharmacokinetics. 25
Baseline samples were collected during the last 3 min of ischemia (T0). During the 40 min of perfusion, the samples were collected at around 0–2.5 min (T1), 5–7.5 min (T2), 15–17.5 min (T3), and 35–37.5 min (T4). The samples were immediately stored in a refrigerator at −20°C. Enzyme-linked immunosorbent assay (ELISA) was used to measure the concentrations of HS and Syn-1. An automated chemistry analyzer (Olympus Automated Chemistry Analyzer AU5400, Japan) was used to measure the levels of alanine aminotransferase (ALT) and aspartate aminotransferase (AST).
Light and electron microscopy
Morphological changes in the liver cells and the perivascular inflammation were visualized and interpreted using the light microscopy after Sudan staining. The morphological changes in the endothelial glycocalyx were visualized and interpreted using the electron microscopy (Phillip ScM10, Philips Electronics, The Netherlands).
Data analysis
Data were analyzed using the analyses of variance (ANOVAs) with repeated measures and Tukey post hoc tests, when appropriate. Alpha was set at 0.05.
Ethical considerations
This study and the protocol have been reviewed by the Institutional Review Board of the First Hospital of Jilin University, Changchun, China and the board finds a study to be by national and institutional ethical standards.
Results
Effects of sevoflurane pretreatment on the concentrations of HS and Syn-1 and the levels of ALT and AST
Upon the beginning of reperfusion, the hepatic ischemia robustly increased the concentrations of HS and Syn-1, and elevated the levels of ALT and AST (all ischemia main effects, F(1, 24) = 18.90–21.72, P = 0.0001; Figure 1). However, the sevoflurane pretreatment reduced the concentrations of HS and Syn-1, and decreased the levels of ALT and AST, in a time-dependent manner (all anesthesia main and interaction effects, F(1–3, 24) = 15.18–25.83, P = 0.001–0.006; Figure 1).

Effects of sevoflurane pretreatment on the release of (a) heparin sulfate and (b) syndecan-1, and the levels of (c) alanine aminotransferase (ALT) and (d) aspartate aminotransferase (AST). Baseline samples were collected during the last 3 min of ischemia (T0). During the 40 min of perfusion, the samples were collected around 0–2.5 min (T1), 5–7.5 min (T2), 15–17.5 min (T3), and 35–37.5 min (T4). Asterisks represent significant difference related to no ischemia control groups (ANOVA ischemia simple main effect, Tukey test, P <0.05). Plus signs represent significant difference relatedto ketamine control group (ANOVA treatment simple main effect, Tukey test, P <0.05).
Specifically, ischemia increased the HS concentration at 0–2.5 min (T1), but not at 5–7.5 min (T2), 15–17.5 min (T3), and 35–37.5 min (T4), in the ketamine-pretreated rats, as compared with no ischemia controls (Tukey test, P <0.05; Figure 1a). However, the sevoflurane pretreatment reduced the HS concentration at 0–2.5 min (T1) in the ischemic rats, as compared with the ketamine-pretreated ischemic rats (Tukey test, P <0.05; Figure 1a).
Furthermore, ischemia produced a trend towards higher Syn-1 concentration at 0–2.5 min (T1), 5–7.5 min (T2) and 15–17.5 min (T3), but not at 35–37.5 min (T4), in the ketamine-pretreated rats, as compared with the controls without ischemia (Figure 1b). However, the sevoflurane pretreatment reduced the Syn-1 concentration at 0–2.5 min (T1), 5–7.5 min (T2), and 15–17.5 min (T3), but not at 35–37.5 min (T4) in the ischemic rats, as compared with the ketamine-pretreated ischemic rats (Tukey test, P <0.05; Figure 1b).
Additionally, ischemia robustly increased the level of ALT at 0–2.5 min (T1), 5–7.5 min (T2), and 15–17.5 min (T3), but not at 35–37.5 min (T4), in the ketamine-pretreated rats, as compared with no ischemia controls (Figure 1c). However, the pretreatment with sevoflurane reduced the level of ALT at 15–17.5 min (T3), but not at 0–2.5 min (T1), 5–7.5 min (T2), and 35–37.5 min (T4) in the ischemic rats, as compared with the ketamine-pretreated ischemic rats (Tukey test, P <0.05; Figure 1c).
Finally, ischemia robustly increased the level of AST at all time intervals in the ketamine-pretreated rats, as compared with the controls without ischemia (Figure 1d). However, the sevoflurane pretreatment reduced the level of AST at 5–7.5 min (T2), but not at 0–2.5 min (T1), 15–17.5 min (T3), and 35–37.5 min (T4) in the ischemic rats, as compared with the ketamine-pretreated ischemic rats (Tukey test, P <0.05; Figure 1d).
Effects of sevoflurane pretreatment on the necrosis of hepatocytes
Following ischemia-reperfusion injury, liver tissues exhibited sinusoidal congestion, with many red blood cells presented, in the ketamine-treated rats (Figure 2a). Extensive punctate necrosis and irregularly zonal necrosis of hepatocytes were also observed (Figure 2a). Additionally, numerous adjacent hepatocytes showed the phenomenon of strip-shaped and/or sheet-shaped vacuolar changes and karyopyknosis (Figure 2b).

Representative light microscopy images of Sudan-stained liver tissues showing the effects of ischemia reperfusion on the necrosis of hepatocytes (a) in (a, b) ketamine-treated rats and (c, d) sevoflurane-treated rats. (a, c) Light microscopy, ×200 and (b, d) light microscopy, ×400. Note the sinusoidal congestion (b) with a large amount of many red blood cells (c) in (a). Additionally, numerous adjacent hepatocytes showed the phenomenon of strip-shaped and/or sheet-shaped vacuolar changes and karyopyknosis (d) in (b). In the sevoflurane-treated rats, however, the liver tissues exhibited diffuse sinusoidal congestion, with only a few red blood cells presented and only scattered punctate necrosis of hepatocytes, following the ischemia-reperfusion injury (c). the adjacent hepatocytes showed moderate vacuolar changes. The outline of the nucleus became irregular in some cells, and the signs of chromatin condensation and cell necrosis started to appear (e) in (d).
In the sevoflurane-treated rats, however, the liver tissues exhibited diffuse sinusoidal congestion, with only a few red blood cells presented, following the ischemia-reperfusion injury (Figure 2c). There was only scattered punctate necrosis of hepatocytes in the center of the field of view (Figure 2c). Furthermore, the adjacent hepatocytes showed moderate vacuolar changes. The outline of the nucleus became irregular in some cells, and the signs of chromatin condensation and cell necrosis started to appear (Figure 2d).
Effects of sevoflurane pretreatment on the endothelial glycocalyx
In the rats treated with ketamine, the endothelial glycocalyx was almost intact when the ischemia-reperfusion was not introduced (Figure 3a). Furthermore, following the ischemia-reperfusion injury, the endothelial glycocalyx was substantially damaged in these rats (Figure 3b). However, after the ischemia-reperfusion injury, the endothelial glycocalyx was preserved to a greater extent in the rats treated with sevoflurane (Figure 3c).
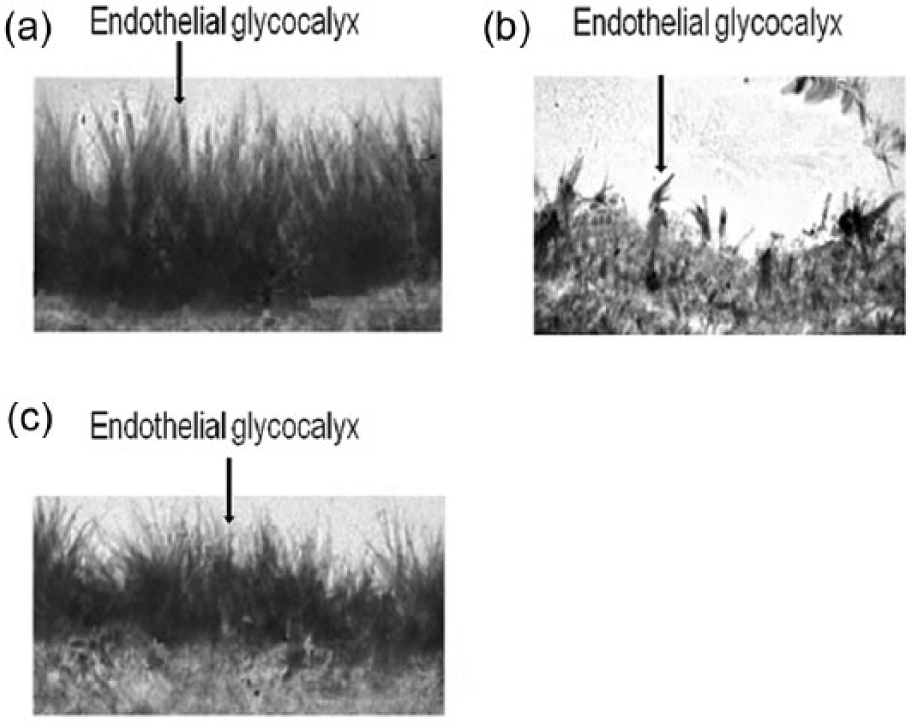
Representative electron microscopy images (Phillip ScM10, Philips Electronics, The Netherlands) are showing the endothelial glycocalyx in liver tissues in rats. (a) The endothelial glycocalyx in the liver tissue of ketamine-treated rats without ischemia. (b) The endothelial glycocalyx in the liver tissue of ketamine-treated rats following the ischemia reperfusion. (c) The endothelial glycocalyx in the liver tissue of sevoflurane-treated rats following the ischemia reperfusion. Photographs are work of GL from the Department of Hepatobiliary and Pancreatic Surgery, The First Hospital of Jilin University.
Discussion
The present study is the first to demonstrate that sevoflurane has protecting effects on the liver endothelial glycocalyx in rats. Sevoflurane can inhibit the shedding of HS and Syn-1 after ischemia-reperfusion injury. It also attenuates the levels of ALT and AST, the commonly used indicators of hepatocellular damage, in liver tissues. 26 The endothelial glycocalyx is a functional barrier and plays a critical role in maintaining the physiologically normal vascular permeability, and it can also prevent the adhesion of white blood cells and platelets to the walls of blood vessels.7,16,27 Hence, the present study suggested that sevoflurane is likely to be therapeutically effective in reducing the liver tissue edema and inflammation induced by the ischemia-reperfusion injury. 17
However, the endothelial glycocalyx is quite fragile, and requires complex environmental conditions to maintain its physiological role.1,2 For instance, the endothelial glycocalyx of normal thickness (0.4–0.5 μm) is observed only in vivo, but not in the cultured endothelial cells. 1 In the present study, we confirmed that ischemia-reperfusion injury can cause degradation of endothelial glycocalyx in liver tissues.2,8,10,27,28 Pretreatment with sevoflurane significantly reduced the shedding of HS and Syn-1 after the ischemia-reperfusion injury.12,13 Similarly, the ischemia-reperfusion injury can cause the destruction of the endothelial glycocalyx in the heart tissues of guinea pigs and humans. 3 Thus, our results are consistent with the previously reported observations.
The time-dependent protective effects of sevoflurane on the shedding of HS and Syn-1 are likely dependent on the physiological association between these molecules and the endothelial glycocalyx, as well as the concentration of sevoflurane in the tissue.12,13 While HS is located on the surface of the endothelial glycocalyx and has a relatively loose association with the endothelial glycocalyx, Syn-1 is a core component of the endothelial glycocalyx and is located in its deeper layers.3,8,10,16,27–29 Therefore, when the endothelial glycocalyx is damaged, the peak of the HS release appeared earlier than that of Syn-1 (Figure 1a). Relatively loose association of HS with the endothelial glycocalyx likely contributes to the limited protective effect of sevoflurane on the shedding of HS at the beginning of the reperfusion.11–16,18,29 Conversely, Syn-1 has a solid association with the endothelial glycocalyx. As a result, the peak of the Syn-1 release appeared much later during reperfusion.9,10,12,13,15,17,29 Thus, sevoflurane appears to have profound preserving effect on the shedding of Syn-1 (Figure 1b). Also, the protective effect of sevoflurane on the shedding of HS may also depend on the concentration of sevoflurane in the tissues. Since the concentration of sevoflurane is likely to decrease in the liver tissue during the reperfusion, its protective effects on the shedding of HS should weaken over time.15,29 Further studies are needed to examine the effects of different concentrations of sevoflurane during the pretreatment on the subsequent protective effects of sevoflurane on the shedding of HS and Syn-1.9,11,15,18
The reduction of the activation of various adhesion molecules during the reperfusion is likely to contribute to the protective effects of sevoflurane pretreatment on the hepatocytes.1,27 Adhesion molecules are a class of small proteins that are also associated with the endothelial glycocalyx. During the ischemia-reperfusion injury, the loss of the endothelial glycocalyx will lead to the exposure of various adhesion molecules in the blood vessels. Once activated, they can bind to the white blood cells and platelets and induce an inflammatory response in the tissues. 1 Hence, the vascular endothelial glycocalyx is critical for the maintenance of vascular permeability and inhibition of the inflammatory responses in the liver tissues.1,21,30,31 The destruction of vascular endothelial glycocalyx in the liver tissues can alter the vascular permeability and disrupt the barrier function of the vascular endothelium.1,8,30 Eventually, it will cause a wide range of liver tissue edema, liver cell necrosis, and platelet aggregations. However, the present study demonstrated that sevoflurane pretreatment could protect hepatocytes against the inflammation induced by the ischemia-reperfusion injury (Figure 2). Specifically, it can reduce the liver tissue edema and decrease the punctate necrosis and the vacuolar changes of hepatocytes during reperfusion. Additionally, the pretreatment with sevoflurane can attenuate the aggregations of macrophages and neutrophils in the liver sinusoid. The protective effect is also reflected by the attenuation of the levels of ALT and AST, which are robustly induced following the ischemia reperfusion (Figure 1c, d). Therefore, future studies will be important in investigating the effects of sevoflurane on the activation of various adhesion molecules.
Furthermore, sevoflurane may protect hepatocytes against ischemia-reperfusion injury by attenuation of the toxicity of polymorphonuclear leukocytes. Polymorphonuclear leukocytes play an important role in ischemia-reperfusion injury in many organs, including the liver. They may not only induce mildly protective inflammation, but also cause excessive inflammation, which may lead to further tissue or organ damage. In the inflammatory response, when the organ or tissue is exposed to inflammation mediators 11,21,31–33 the surface expression of the intercellular adhesion molecules on the polymorphonuclear leukocytes could be increased, what might activate these cells via β2 integrin-dependent mechanism. 30 Once the polymorphonuclear leukocytes are activated, they gather close to the liver vascular bed and further trigger the complement activation, as well as induce the activation of the platelet-activating factor. 21 In normal conditions, these activated polymorphonuclear leukocytes can also gather in the vicinity of sinusoids and postsinusoidal or portal venules without triggering the liver tissue injury.17,18 However, the degradation of the endothelial glycocalyx caused by ischemia-reperfusion injury can increase the vascular permeability, leading to the migration of polymorphonuclear leukocytes out of blood, extravasation into the parenchymal cells (i.e. hepatocytes), and the subsequent development of substantial necrosis of hepatocytes.15,31 Therefore, in addition to the preservation of vascular barrier function and, consequently, the preventing of the migration of polymorphonuclear leukocytes into the hepatocytes, the pretreatment with sevoflurane may decrease the β2 integrin-dependent activation of polymorphonuclear leukocytes in the liver. Further studies will be required to test this hypothesis.
Conclusion
In summary, although the protective mechanisms of the sevoflurane pretreatment on the endothelial glycocalyx are still not fully established, it is likely that sevoflurane can target multiple enzymes and processes associated with glucocalix. Previous studies have demonstrated that sevoflurane pretreatment can attenuate the release of lysosomal cathepsin B, thus reducing the degradation of the endothelial glycocalyx by lysosomal enzymes. 10 Additionally, sevoflurane can competitively bind to heparinases and reduce their function, 34 thus reducing the hydrolysis of the endothelial glycocalyx. Therefore, further studies on the effects of sevoflurane on the endothelial glycocalyx may not only reveal the functional significance of the endothelial glycocalyx in the ischemia-reperfusion injury, but also shed light on the development of effective pharmacotherapies for the prevention and treatment of this injury.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.