
Abstract
Urinary bladder cancer (BC) is one of the most frequent malignancies and the ninth most common malignancy worldwide. The objective of this study is to assess the role of multiparametric magnetic resonance imaging (mp-MRI) in predicting the invasiveness of urinary bladder space occupying lesions. Thirty-five patients diagnosed with bladder masses underwent an mp-MRI study. The results of three image sets were analysed and compared with the histopathological results as a reference standard: T2-weighted image (T2WI) plus dynamic contrast-enhanced (DCE), T2WI plus diffusion-weighted images (DWI), and mp-MRI, including T2WI plus DWI and DCE. The diagnostic accuracy of mp-MRI was evaluated using receiver operating characteristic curve analysis. We discovered a highly significant correlation between muscle invasiveness as staged by HPE (Histopathological examination) and mp-MRI utilising a VI-RADS score >3 (p 0.001) with a sensitivity of 100% and a specificity of 85.7%. With a diagnostic accuracy of 77.14%, a sensitivity of 92.31%, a specificity of 72.72%, a positive predictive value of 66.67%, and a negative predictive value of 94.11%, In terms of muscle invasiveness, there is good concordance between HPE staging and mp-MRI utilising the VI-RADS score. The mean apparent diffusion coefficient (ADC) values were higher in low grades than in high grades. The ROC curve study revealed a very strong correlation between HPE grade and ADC (p = 0.045). In 77.14% of patients, Mp-MRI correctly identified the local T stage. Mp-MRI is imaging biomarker for invasiveness and grade of tumour. The tumours with high grade are more invasive. However, the diagnostic accuracy of mp-MRI in determining muscle invasiveness is not very high and it overstages the disease in some cases (33.3%). Its clinical usefulness in determining muscle invasiveness before TURBT and histopathological examination can be questioned.
Keywords
Introduction
Urinary bladder cancer (BC) incidence rises as the age advances, and the male-to-female ratio is roughly 3:1. 1 More than 90% of bladder cancers are urothelial in origin. 2 and at diagnosis, 80% of them are non-muscle invasive. 3
The presence or absence of muscle invasion is the most crucial factor in the local staging of bladder cancer. While many approaches have been tried to increase bladder cancer staging accuracy, there is still a need for cutting-edge imaging equipment to optimise pre-operative staging and enhance treatment outcomes.
The current gold standard for detecting whether muscle invasion is present or absent is found to be TURBT.4,5 However, it has been discovered that TURBT commonly needs to be repeated and that it inaccurately determines tumour grade in up to 15% of patients and underestimates T stage in up to 40% of patients. 6
The development of multiparametric MRI (mp-MRI), which combines anatomic T1 and T2 weighted images (T1WI and T2WI) with functional sequences like diffusion-weighted imaging (DWI) and dynamic contrast-enhanced MRI (DCE-MR), increases the precision of cancer detection and staging. 7 The VI-RADS score (Vesical Imaging Reporting and Data System) was recently developed to provide a systematic method for imaging and reporting mp-MRI for bladder cancer. 8
With an emphasis on distinguishing between non-muscle invasive bladder cancer (NMIBC) and muscle-invasive bladder cancer (MIBC), the current study aims to investigate the potential of mp-MRI in predicting the invasiveness of urinary bladder space-occupying lesions. We also want to examine the correlation between mp-MRI and histological grade and the agreement between VI-RADS score based on mp-MRI and histopathological staging. This information can aid in determining the appropriate treatment plan for patients with bladder cancer. Ultimately, the findings of this study may lead to improved diagnostic accuracy and better patient outcomes in the management of bladder cancer.
Patients and methods
Our study was conducted in tertiary care centre. It is a prospective observational study. We recruited 40 subjects, with no randomisation. Five patients were excluded due to inadequate MRI examination, and 35 were included for analysis. Our study population includes newly diagnosed treatment naïve bladder tumour patients. Each patient is primarily diagnosed by USG(Ultrasonography) or CT abdomen examination. They were further evaluated by MRI pelvis (plain plus contrast) examination for VI-RADS scoring and ADC value (Apparent diffusion coefficient) with standardised MRI protocol. All selected patients have been subjected to TURBT and histopathological findings were noted. Each patient we evaluated the estimated Glomerular filtration rate (e-GFR) before performing a plain and contrast MRI examination. We included both male and female patients of age more than 18 years with a cystoscopically diagnosed bladder tumour and excluded patients with age group of less than 18 years, Patients with general contraindications of MRI examination (pacemaker, metallic implants, neurostimulators, cochlear implants, claustrophobia), Patients with contraindication for TURBT (unfit for anaesthesia, urethral stricture), eGFR less than 60 ml/min/m2 of body surface area, allergic to MRI contrast agent, receiving radiotherapy and or chemotherapy, patients with advanced disease (both locally advanced disease, AJCC-TNM staging IIIA, IIIB and patients having advanced disease and or distant metastasis, AJCC-TNM staging IVA, IVB) and unwilling to give consent.
Imaging was done with 3.0 Tesla MRI Machine (GE Healthcare) Signa 3T Hdxt with 8US TORSOPA coil. Patients were fasted for 4–6 h and withheld urine for at least 2 h before MRI examination, with no drinking or urination thereafter until the MRI examination is complete. MRI Pulse Sequences: The entire pelvis is imaged from aortic bifurcation to the inferior margin of the symphysis pubis.
Tl W SEQUENCE. Imaging plane: axial (FSE- XL/90)
T2W sequences: Imaging plane: Axial, Sagittal, and or coronal (FRFSE)
Nonenhanced and Gadolinium Enhanced DCE 3d Tl W Sequences: Imaging Plane: Axial (M3D/LAVA/12)
Contrast material injection with gadolinium Chelate with dose according to body weight at the rate of 2 ml/s, up to a total volume of 20 ml in patients with adequate eGFR. Axial and coronal FIESTA sequences are taken before DCE imaging for localisation of bolus tracker at the bifurcation of aorta into bilateral common iliac arteries. Three sets of contrast enhanced images were obtained 17–131 s after injection of contrast material. Summary of MRI imaging parameters:

SPIN ECHO EPI DWI (b = 400, 800, 1000 s/mm2) with ADC map:
Imaging plane: Axial
Summary of DWI parameters:
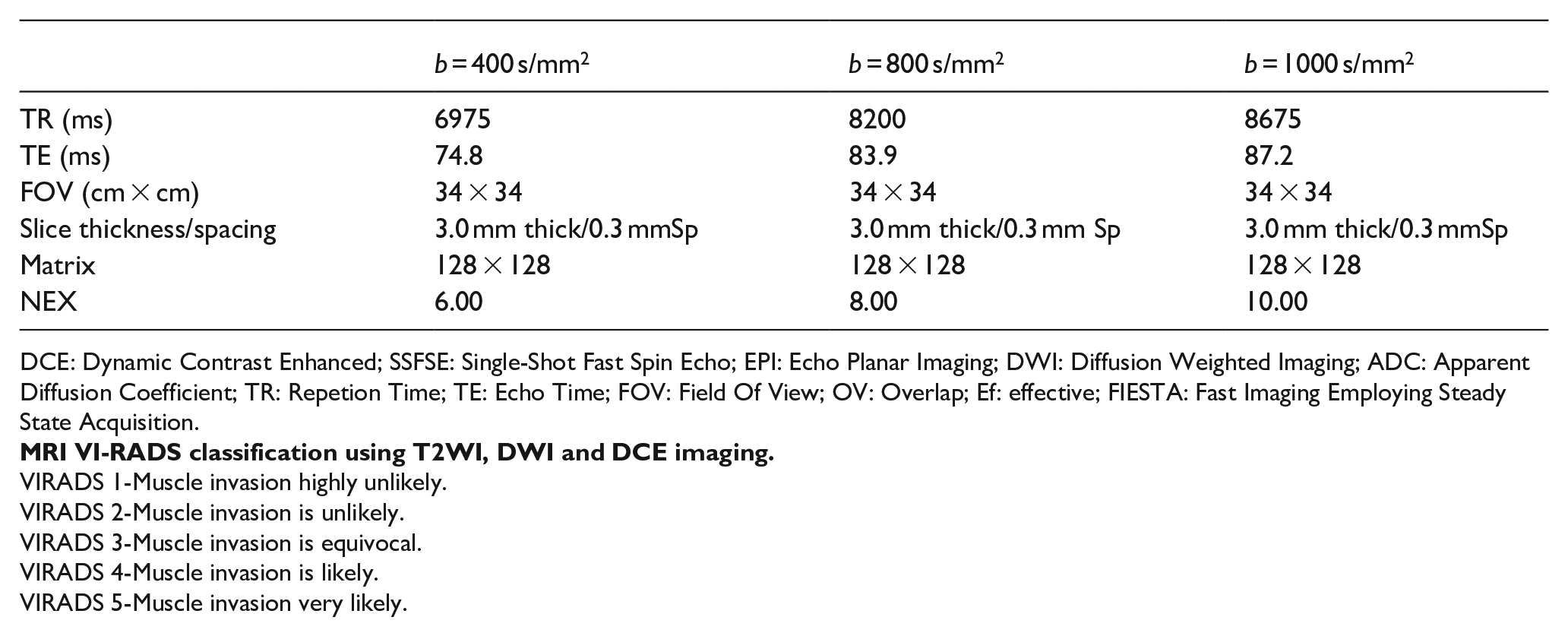
DCE: Dynamic Contrast Enhanced; SSFSE: Single-Shot Fast Spin Echo; EPI: Echo Planar Imaging; DWI: Diffusion Weighted Imaging; ADC: Apparent Diffusion Coefficient; TR: Repetion Time; TE: Echo Time; FOV: Field Of View; OV: Overlap; Ef: effective; FIESTA: Fast Imaging Employing Steady State Acquisition.
VIRADS 1-Muscle invasion highly unlikely.
VIRADS 2-Muscle invasion is unlikely.
VIRADS 3-Muscle invasion is equivocal.
VIRADS 4-Muscle invasion is likely.
VIRADS 5-Muscle invasion very likely.
Results
The data were tabulated in Microsoft Excel and analysed with SPSS V.24 software. The continuous variables were presented with mean and standard deviation. The categorical variables were presented with frequency and percentage. Independent t-test, chi-square test, Receiver operating characteristic (ROC) curve, sensitivity, specificity, positive predictive value, negative predictive value, logistic regression and kappa statistics were used for the statistical analysis. The p-value ⩽ 0.05 was considered statistically significant.
Total 35 patients were included in our study. Out of 35 patients, 26 were male and 9 were female. The median age was 58 (52–67) years. 98% of patients presented haematuria. 34.3% of patients had risk factor of smoking. Among the study subjects 22 patients (63%) belong to histologically proven non-muscle invasive bladder tumours (NMIBC) and 13 patients (37%) have muscle invasive bladder tumours (MIBC). Histologically high-grade and low-grade tumours are seen in 57%, and 43% of the study population respectively. Median value of bladder SOL in each patient was 2. As per tumour morphology, most of the tumours are sessile variants (85%); other morphological types are polypoidal (9%), papillary (2%), and sessile with stalk (4%).
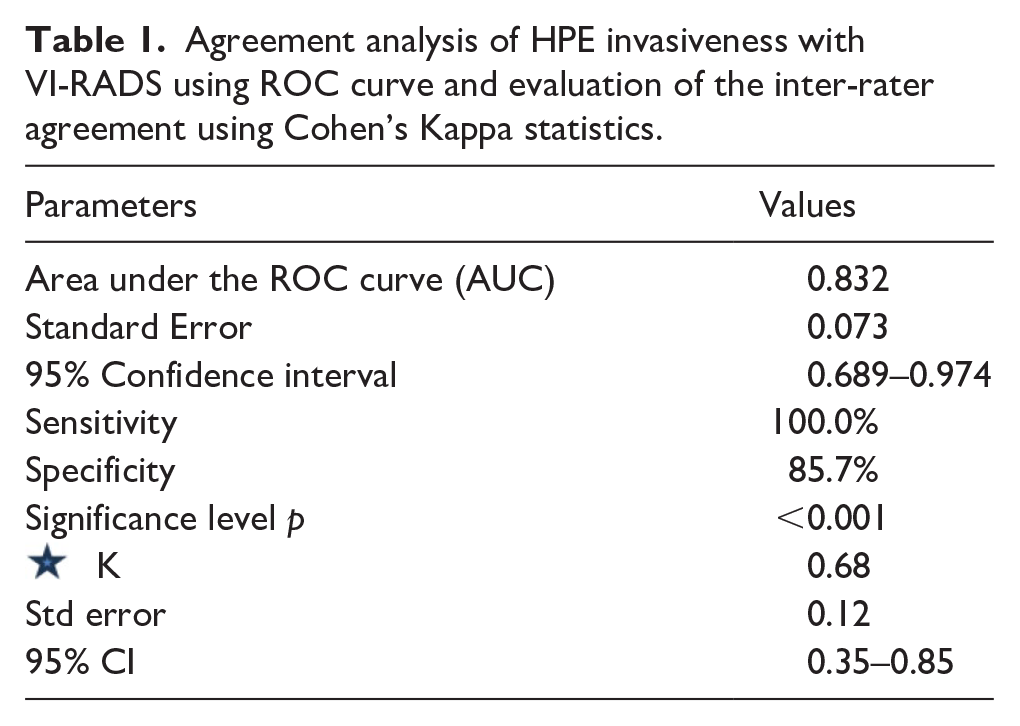
Receiver operating characteristic curve (ROC) analysis was used to calculate the area under the curve (AUC) to evaluate the agreement between mp-MRI using VI-RADS score with HPE (Histopathological examination) of bladder tumours to understand muscle invasiveness. A significantly strong agreement between VI-RADS score with HPE (Histopathological examination) staging of muscle invasiveness (p < 0.001) was found from the ROC curve. It demonstrates VI-RADS score cutoff value more than 3 with corresponding sensitivity of 100% and specificity of 85.7%.
 Cohen’s kappa (κ) statistic was used to evaluate the degree of agreement. The K value can be interpreted as follows (<0.20 considered poor, 0.21–0.40 considered fair, 0.41–0.60 considered moderate, 0.61–0.80 considered good, and 0.81–1.00 considered excellent). The level of confidence was kept at 95% hence a p-value < 0.05 indicated a significant association. Cohen’s kappa statistics reveal good agreement (kappa – 0.61–0.80) between mp-MRI using VI-RADS score with HPE staging for muscle invasiveness. So, the extent of harmony between radiologic and histopathological staging results was greatest when using mp-MRI denoting high diagnostic performance (Table 1, Figure 1).
Cohen’s kappa (κ) statistic was used to evaluate the degree of agreement. The K value can be interpreted as follows (<0.20 considered poor, 0.21–0.40 considered fair, 0.41–0.60 considered moderate, 0.61–0.80 considered good, and 0.81–1.00 considered excellent). The level of confidence was kept at 95% hence a p-value < 0.05 indicated a significant association. Cohen’s kappa statistics reveal good agreement (kappa – 0.61–0.80) between mp-MRI using VI-RADS score with HPE staging for muscle invasiveness. So, the extent of harmony between radiologic and histopathological staging results was greatest when using mp-MRI denoting high diagnostic performance (Table 1, Figure 1).
Agreement analysis of HPE invasiveness with VI-RADS using ROC curve and evaluation of the inter-rater agreement using Cohen’s Kappa statistics.
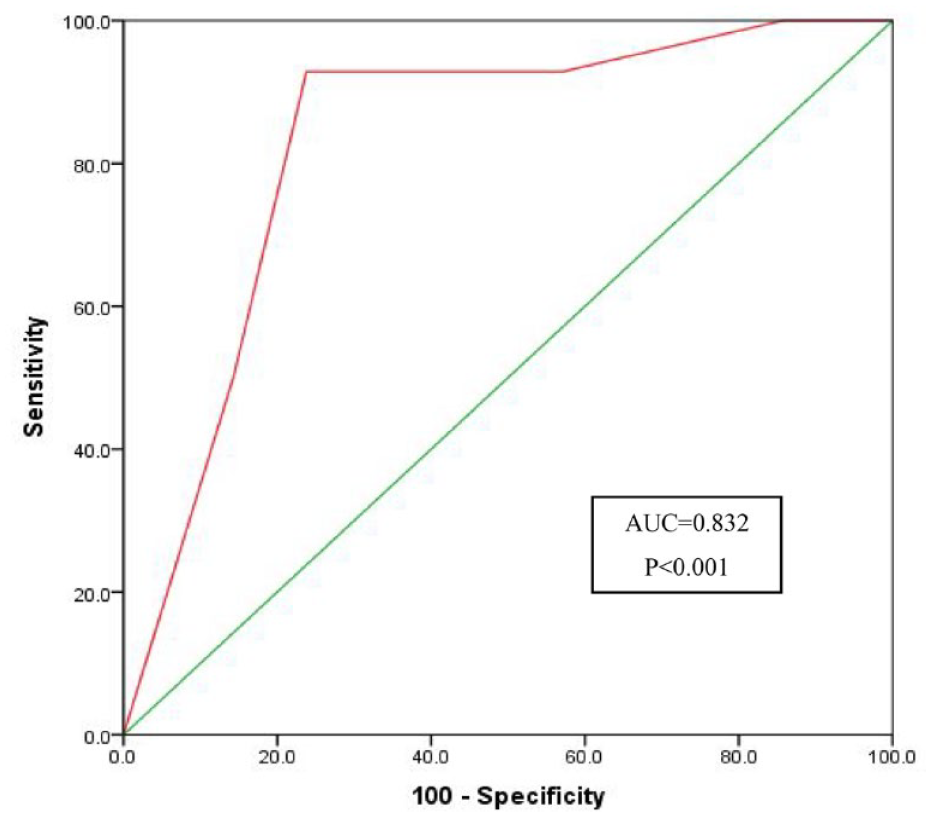
ROC curve analysis of VI-RADS score with HPE staging of bladder tumour muscle invasiveness.
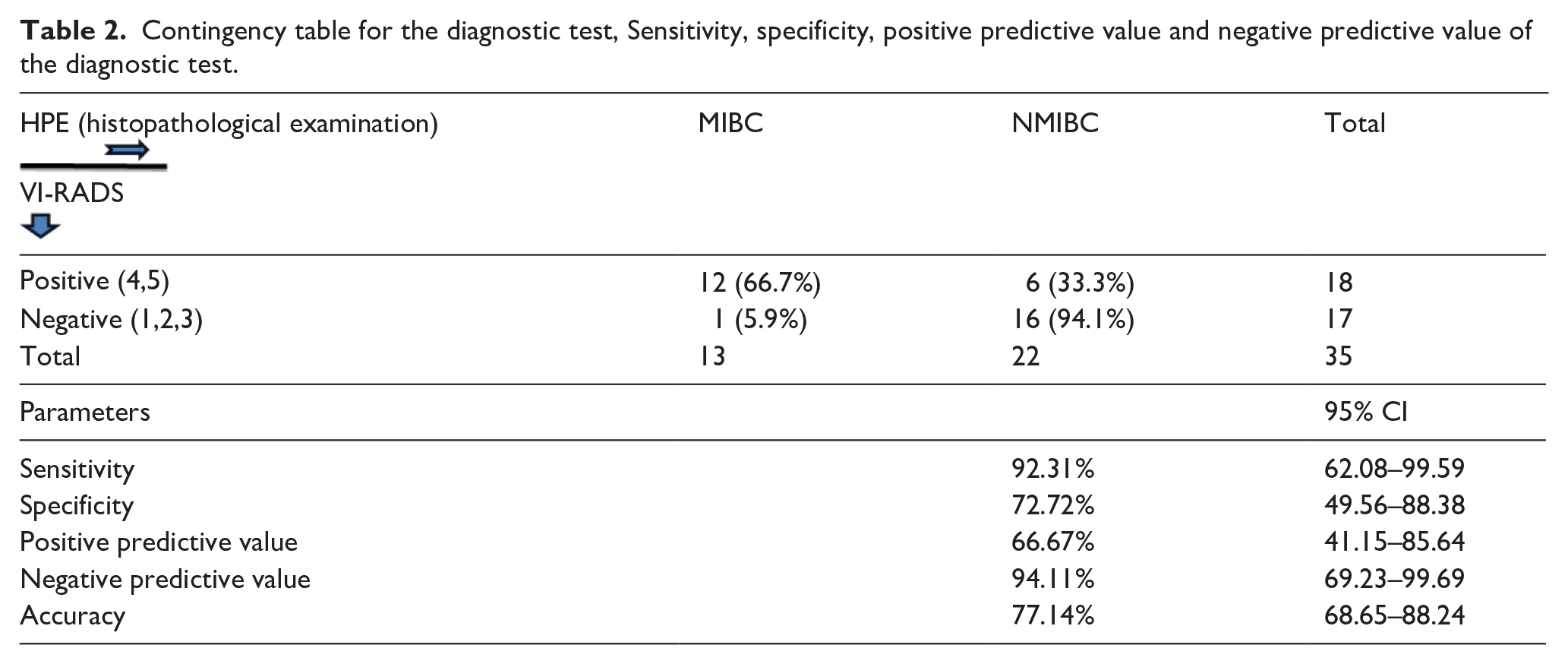
The contingency table is prepared based on ROC curve determined cut-off VI-RADS score. Out of 18 patients diagnosed with muscle-invasive bladder carcinoma according to mp-MRI using VIRADS score 4 and 5, 12 (66.7%) patients were diagnosed as histologically proven MIBC. Out of 18 patients diagnosed as muscle-invasive bladder carcinoma by mp-MRI using VI-RADS score 4 and 5, 6 patients came out to be NMIBC. So Mp-MRI overstage the disease in 6 (33.3%) patients.
Diagnostic test contingency table analysis reveals that the diagnostic accuracy of mp-MRI showing VIRADS score >3 in detecting bladder tumour muscle invasiveness is 77.14% (68.65%–88.24%) with sensitivity 92.31% (62.08%–99.59%), specificity 72.72% (49.56%–88.38%), positive predictive value 66.67% (41.15%–85.64%), and negative predictive value 94.11% (69.23%–99.69%) (Table 2).
Contingency table for the diagnostic test, Sensitivity, specificity, positive predictive value and negative predictive value of the diagnostic test.


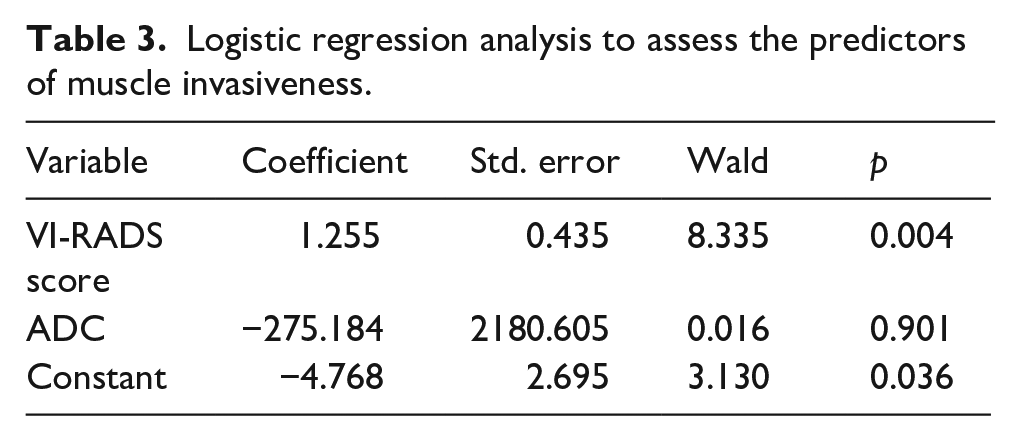
Logistic regression analysis was performed to predict HPE-established muscle invasiveness from suspected imaging-based predictors like VI-RADS score, and ADC value. In this analysis, the outcome variable is dichotomous in nature (MIBC vs NMIBC) and predictors are numerical. The regression model showed that the VI-RADS score was found to be a significant predictor for muscle invasiveness (p = 0.004) (Table 3).
Logistic regression analysis to assess the predictors of muscle invasiveness.
Based on histopathological findings we have analysed relation of tumour grades with invasiveness. It shows among the non-invasive tumours 63.6% are low grade, and among the invasive tumours 92.3% are high grade tumours (p value of <0.001) (using crosstabs with Fisher’s exact test) (Table 4).
HPE invasiveness and grading.
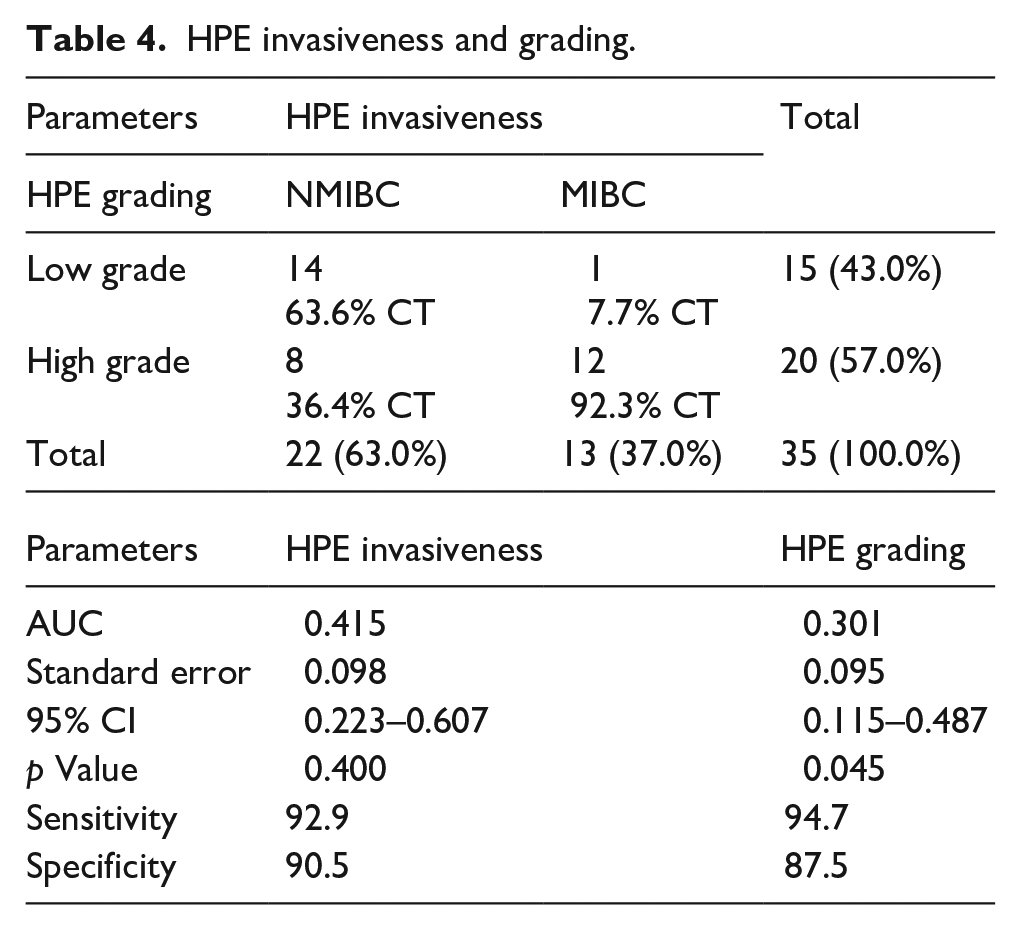
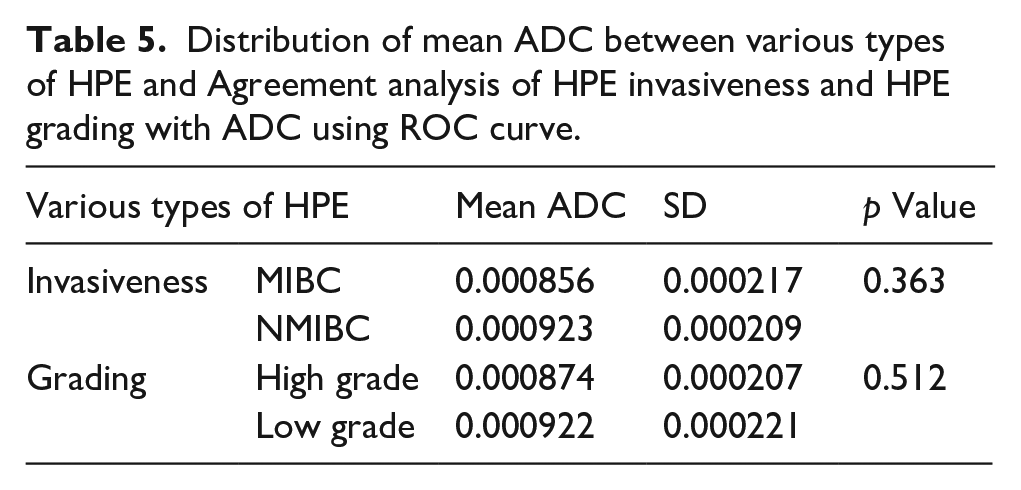
The mean ADC values were found to be higher in NMIBC than MIBC and in Low grade than in High grade, but the differences are not statistically significant (p > 0.05). A significantly strong agreement between HPE grading with ADC (p = 0.045) was found from the ROC curve (Table 5).
Distribution of mean ADC between various types of HPE and Agreement analysis of HPE invasiveness and HPE grading with ADC using ROC curve.
Discussion
Transitional cell carcinoma of urinary bladder is one of the most common malignancies affecting genitourinary tract and is characterised by multifocality and high rate of recurrence. So accurate T staging and grade of bladder carcinoma is important for treatment and management. 7 TURBT is the gold standard for determining the presence or absence of muscle invasion.4,5. TURBT has been found to underestimate T stage in up to 40% of patients, is inaccurate in determining tumour grade in up to 15% of patients, and frequently needs to be repeated. 6 Multiparametric MRI has anatomic and functional sequences (including high-resolution T2WI, DWI and DCE-MRI), and various reports have shown its superiority of it. It shows promising results in detection, staging and follow-up cases of urinary bladder malignancies. 7
It has been demonstrated that bladder carcinomas’ muscle invasiveness can be accurately detected using multiparametric MRI and the VI-RADS score. We need additional data on this reporting method in order to draw meaningful conclusions from systematic reviews and meta-analyses because muscle invasiveness is the primary factor determining treatment modalities and end outcomes. 9
We recruited 40 individuals for our study, of whom 35 were used in the final analysis. 74.2% of the participants in our study were men. A risk factor identified in 34.3% of patients is smoking. 37% of the participants in our study have muscle-invasive bladder tumours, compared to 63% who do not have muscle invasion.
With a sensitivity of 100% and a specificity of 85.7%, we discovered a highly significant correlation between muscle invasiveness as staged by HPE and mp-MRI utilising a VI-RADS score >3 (p 0.001). With a sensitivity of 92.31%, a specificity of 72.72%, a positive predictive value of 66.67%, and a negative predictive value of 94.11%, the current study indicated that the diagnostic accuracy of mp-MRI (VIRADS score >3) in diagnosing bladder tumour muscle invasiveness is 77.14%. Our findings are superior to those made public by Makboul et al., and nearly identical findings were discovered between our research and those of Marchioni et al. and Liu et al.10–13 The agreement between HPE staging for muscle invasiveness and mp-MRI using the VI-RADS score is good (kappa = 0.61–0.80).
We found that VI-RADS score as a significant predictor for muscle invasiveness (p = 0.004) in our study.
For each patient, we have calculated the ADC values at b-1000 s/mm2. The mean ADC values were found to be greater in NMIBC than MIBC, according to our research. Though the differences between Low and High grades were shown to have larger mean ADC values, they are not statistically significant (p > 0.05). With an AUC of 0.301, sensitivity of 94.7.2%, and specificity of 87.5%, ROC curve analysis of ADC values with tumour grades having a statistically significant value less than 0.000953 mm2/s can be a helpful cut-off for high-grade tumours. The ROC curve study revealed a very strong correlation between HPE grade and ADC (p = 0.045). Similar outcomes were discovered in previous studies.14,15
In our study, we discovered that higher grades were frequently linked with invasive tumours (p 0.001) because bladder carcinoma tumour grades had a significant impact on treatment options. The mp-MRI is a predictor of both cancer invasiveness and tumour grade, as we have already observed in our work. Additionally, tumour grades themselves mirror how invasive a bladder tumour is, making mp-MRI a useful imaging tool for both factors.
When compared to the earlier study conducted by Badawy et al. 16 which showed diagnostic accuracy of mp-MRI in detecting muscle invasiveness as 91%, but in our study it was 77.14%. Moreover mp-MRI also overstaged the disease in our study by 33.3%.
One of the limitations of our study is small sample size, and we did not independently examine each VI-RADS parameter in our study.
On the other hands we have certain strengths as well; we have done imaging with standardised protocol using single 3-Tesla MRI facility. Imaging report done with consensus of three radiologists. And our study is prospective in nature.
Conclusion
Muscle invasion in cases of urinary bladder cancer can be detected by mp-MRI. In addition to being used to determine the local staging of bladder tumours, mp-MRI also serves as an imaging biomarker for the invasiveness and grading of the tumour. The tumours with high grade are more invasive. However, the diagnostic accuracy of mp-MRI in determining muscle invasiveness is not very high and it overstages the disease in some cases. Its clinical usefulness in determining muscle invasiveness before TURBT and histopathological examination can be questioned (Figure 2).
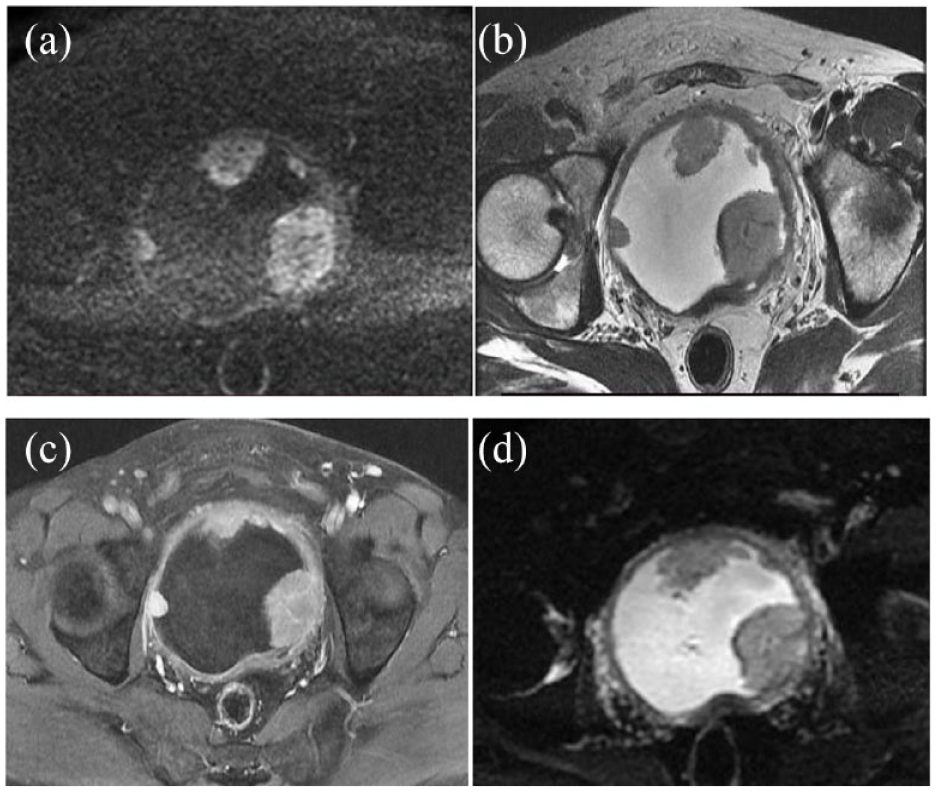
Fifty-two year male with multiple sessile exophytic UB SOLs, largest one in left posterolateral (a) T2 W image shows clear disruption of UB wall and extravesical involvement, (b) DCE image show contrast enhancement with loss of low SI muscularis, (c and d) DWI and ADC images showing disruption of low SI muscularis; VI-RADS score came as 5. Histopathology reveals high grade tumour with muscle invasion.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Presentation at a meeting
Nil