
Abstract
With only 16 cases reported in the literature, the mostly benign granular cell tumour of the urinary bladder is exceptionally rare. We present the case of a 68-year old patient with one of these lesions demonstrating our histological findings including several immunohistochemical stainings used to differentiate between other more common entities.
Introduction
Granular cell tumours - also known as myoblastomas - are unusual, in most cases benign neoplasms which are commonly found in the head and neck region, especially the tongue, but can also occur in other tissues such as skin, vulva, breast, larynx or oesophagus. So far, no more than 16 reported cases have originated in the urinary bladder, with only 2 presenting malignant entities. We herein report one case of a benign lesion in the urinary bladder which occurred in a 68-year old male and review the literature with emphasis on the immunohistochemical pattern of the tumour.
Case Report
We report the case of a 68-year old patient who presented to our urologic department for removal of a double-J ureteral stent which had been placed two months earlier during kidney transplantation. On flexible cystoscopy, a suspicious lesion of the vesical mucosa - measuring about 1 cm in diameter - was seen. The finding appeared solid with a smooth surface and did not resemble the typical papillary aspect of a transitional cell carcinoma. In the following, we performed transurethral resection of the tumour. Due to close proximity to the resected area the double-J catheter in the ureter of the transplanted kidney was left in place (Figure 1). The lateral wall of the bladder showed a mass of connective tissue interspersed with cells that contained round nuclei with small granules and eosinophilic cytoplasm with a foamy aspect. Between these cells a dense capillary system could be found. Overall, there was no cellular atypia and mitoses were virtually non-existent (Figure 2). Further immunostaining revealed a positive reaction towards S-100-protein and negativity for epithelial (Pan-cytokeratin AE1/AE3, KL-1) markers. Staining for CD68 (PGM-1 as a marker for macrophages and monocytes), CD 45 (revealing relations toward leucocytes) and actin-filaments showed no positive reaction. The proliferative index (Ki-67-staining) was less than 1%, all these findings adding up to the most probable diagnosis of a benign granular cell tumour of the urinary bladder (Figure 3). In addition, we performed in situ hybridization for Epstein-Barr encoded RNA (EBER), as several cases of Epstein-Barr virus associated smooth muscle tumours (EBV-SMT) occurring after organ transplantation have been reported; the most common sites for these neoplasms being the liver, lung and spleen.1,2 However, our analysis remained negative; no staining of nuclei in tumour cells was seen thus ruling out the possibility of an EBV-related tumour.
Vesical mucosa on flexible cystoscopy with the granular cell tumour in the centre (*).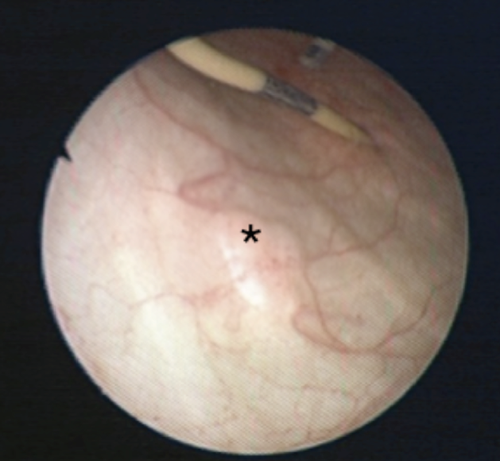
Haematoxylin and Eosin staining, magnification 400×.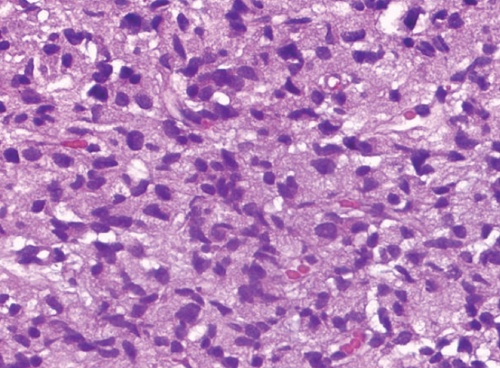
S-100 staining, magnification 200×.
The analysis of a urine sample showed clusters of cells with abundant cytoplasm with small vacuoles. In between a small amount of erythrocytes and inflammatory cells were found; no tumourous structures were present.
Additional biopsies taken from the same patient in different locations of the bladder showed no signs of any tumourous formations but only revealed a chronic inflammatory process. A follow-up cystoscopy performed 8 weeks afterwards showed no remnants or recurrence of the tumour.
Discussion
Granular cell tumours mostly arise in the upper part of the human body, with approximately two thirds presenting themselves in the head and neck region.3,4 Therefore, such a lesion in the urinary bladder is a very uncommon and rare entity with only 16 reported cases in the literature.5–10 The tumour shows a slight predominance in females, most often occurring between the ages of 30 to 60; 11 nevertheless children affected by this neoplasm have also been reported. 7 Symptoms vary regarding the specific location - tumours situated in the urinary bladder frequently cause chronic hematuria which may lead to severe decrease of hemoglobin and blood pressure. Other less common signs of disease include dysuria, incontinence and abdominal pain.5,7,9
The term myoblastoma was first introduced in 1926 by Abrikossoff who postulated the tumour as being derived from striated muscle cells as a regenerative process after injury to the tissue. 12 Up to now, based on histochemical and ultrastructural findings, three additional theories concerning the histogenesis of granular cell tumours have been discussed: 13 histiogenic origin with histiocytes as the underlying cell population; multicentric origin and the widely favoured neurogenic histogenesis which postulates the derivation from Schwann cells.14–17 However, the overall histogenesis is still poorly understood and although many authors favour a neurogenic origin, either from Schwann cells or modified cells of the neural crest, analysis has failed to identify the direct transition from a Schwann cell to a myo -blastoma.18–20 Histologically, granular cell tumours of all anatomic sites share the same characteristics - they consist of polygonal cells with highly granular cytoplasm with fine eosinophilic granules and scattered larger droplets. 16 There often exists a secondary epithelial hyperplasia if the tumour appears near an epithelial surface. 9 It may be hard to distinguish from more common malignant and benign tumours or lesions derived from macrophages such as malakoplakia which histologically can easily be mistaken. Therefore, in recent years, specific analyses have obtained importance for reaching the accurate diagnosis.
Nowadays immunohistochemical staining is particularly useful to discern these tumours and malignant entities such as sarcomas and carcinomas as GCTs stain positive for the neural crest derived S-100-protein, both cytoplasmic and nuclear and therefore backing the theory of being derived from Schwann cells or similar populations. 20 Furthermore, they frequently reveal positive staining for calretinin, alpha subunit of inhibin, HLA-DR, laminin and various myelin proteins whereas they react negative when exposed to epithelial (cytokeratine), sarcoma (desmin, vimentin) and neuroendocrine (neuron-specific enolase, chromogranin A and synaptophysin) markers.3,7 In addition, benign granular cell tumours hardly ever show a proliferative index (as revealed in staining with Ki-67) exceeding 10%; 3 necrosis and atypical nuclei are absent. Due to the predominantly benign course of the tumour, transurethral resection with sufficiently clear margins is the treatment of choice for most patients. Recurrence however has been described and can be treated by the same course of action - nevertheless, the even more infrequently appearing malignant forms should be approached with a more radical therapy. 6 The first of only two reported malignant cases was treated by complete excision, unfortunately the patient died 17 months afterwards from metastases and local recurrence: 5 the second patient underwent complete surgical excision including radical cystectomy, bilateral salpingo-oophorectomy, hysterectomy, and pelvic lymph node clearance and remained disease-free afterwards. 7 Despite the above mentioned benign histology in this case, we recommended a follow up regimen conforming with the current European Guideline standards for non-muscle invasive bladder cancer, starting with a cystoscopy 3 month after tumour resection and a following cystoscopy after another 9 months as well as yearly cystoscopy for 5 years. 21
Conclusions
Based on the fact that granular cell tumours arising in the urinary bladder are rare events, careful histological examination should be performed to rule out a more malignant variant of the tumour, thus providing the patient with the best treatment. Transurethral resection is sufficient for most cases - in contrast to a more radical approach, performed if a malignant tumour is diagnosed. In recent years, immunohistochemical staining has provided a helpful diagnostic tool to distinguish granular cell tumours from various other entities but nevertheless, because of its rarity, diagnosis still may be challenging.