
Abstract
Background:
Varicocele is the most common correctable cause of male infertility. The treatment of varicocele is surgery. However, which patients will benefit from the surgery is controversial. Our aims to investigate the effect of systemic immune-inflammation index (SII) and systemic inflammatory response index (SIRI) on varicocelectomy success.
Methods:
Patients who underwent varicocelectomy in our clinic between January 2016 and June 2022 were analyzed retrospectively. Varicocelectomy success was defined as >50% increase in post-operative total motile sperm count (TMSC) in those with pre- operative TMSC > 5 million and at least 100% increase in those with <5 million. The patients were divided into two groups as benefiting from the treatment (Group 1) and no benefits (Group 2).
Results:
Of the 207 patients who underwent varicocelectomy, 144 (69.6%) of them improved their semen parameters, and 63 (30.4%) did not. The optimum cut-off value of SII was 334.6, with an AUC of 0.733 (95% CI: 0.665–0.813). The best cut-off value for SIRI of 0.882, with an AUC of 0.692 (95% CI: 0.607–0.772). The highest sensitivity and specificity were 0.692 and 0.601 (p < 0.001). In the multivariate analysis, only SII (OR: 3.152, 95% CI: 1.316–7.358; p = 0.003) and SIRI (OR: 2.919, 95% CI: 1.472–5.774; p = 0.002) were independent predictive factors for varicocelectomy success.
Conclusions:
Our results showed that preoperative SII and SIRI values were lower in infertile patients who underwent successful varicocelectomy. Therefore, we think that these parameters will be useful in identifying patients who will benefit before varicocelectomy.
Keywords
Introduction
Varicocele is the formation of a tortuous structure due to obstruction in the veins in the panpiniform plexus of the spermatic cord. Varicocele has an incidence of 15% in adolescence with 90% being left-sided and 10% being right-sided. 1 The patient is visually examined at room temperature. During the Valsalva maneuver, the spermatic cord is palpated. They are graded as follows: grade 1, palpated with Valsalva; grade 2, palpated without Valsalva; grade 3, easily visible. 2 Indications for treatment include symptomatic varicocele, causing testicular atrophy, and abnormality of at least two sperm samples. The advantages of the subinguinal microscopic approach are less arterial and lymphatic damage and less complications, but it takes time to learn and requires experimentation. 3 In studies, some improvement in spermiogram parameters was observed after varicocelectomy operation, while others did not. 4 That is why various data are needed to predict the success of the operation. There are many studies conducted on this subject and nomograms created. 5
Current data indicate that varicocele is responsible for a large number of etiologies, including pathophysiological hyperthermia, oxidative stress, apoptosis, inflammation, and hormonal effects on infertility. 6 One of the most evaluated parameters among the pathophysiological mechanisms related to the negative effect of varicocele on fertility is inflammation. It is reported that an increase in cytokines such as seminal epithelial neutrophil-activating factor-78 (ENA-78), and IL-1β in testicular tissue as a result of varicocele can cause infertility by many mechanisms.7,8 These increased cytokines are found in the tunica albuginea, interstitial tissues, and germ cells and seminiferous can cause damage to the tubules. Certain changes in peripheral blood cell elements signal the response to various inflammatory diseases. 9 In previous studies in patients with varicocele, neutrophil-lymphocyte ratio (NLR), lymphocyte-monocyte ratio (LMR) and platelet-lymphocyte ratio (PLR) were used to predict prognosis. 10 In addition, the systemic immune inflammation index (SII) and systemic inflammation response index (SIRI) in inflammatory diseases and various cancers have been studied as more complex inflammatory markers.11,12 Since 2014, a new index called the SII (neutrophil × platelet/lymphocyte) has been used. In addition, the effects of SIRI (neutrophil × monocyte/lymphocyte) on predicting the prognosis of various cancers and inflammatory diseases have also been studied.13,14 The present study aimed to examine the impact of SII and SIRI on varicocelectomy success.
Materials and methods
The varicocelectomy data of our clinic between July 2016 and July 2022 were evaluated retrospectively. The necessary ethics board acceptance was acquired (protocol no: 2022/07/02). Azoospermic patients and patients with missing clinical, laboratory and follow-up data were excluded from the study.
Peripheral venous blood sampling was performed in the clinic’s central laboratory according to standard procedures. Routine blood tests (including neutrophils, lymphocytes, monocytes, and platelets) were evaluated with the Mindray BC-6800 automated hematology analyzer.
Fasting bloods were picked up prior to 9:00 am to measure hormonal values (FSH, LH, and testosterone). Electrochemiluminescence immunoassay method was used for hormonal analysis.
Sperm preparation and analysis
Minimum two semen instances were examined before varicocelectomy and 6 months thereafter the operation in patients with varicocele. Before the semen test, the patients were sexually abstinent for at least 72 h. All semen analyzes were performed within 60 min. Semen volume, total sperm count, and total motile sperm count (TMSC) were enrolled. The result with the highest TMSC before and after surgery was accepted as the reference. Patients were categorized according to the improvement in sperm analysis values. In postoperative semen analysis, a more than 50% increase in post-operative total motile sperm count (TMSC) in those with pre- operative TMSC > 5 million and at least 100% increase in those with <5 million were determined as recovery criteria. 15 Group 1 was defined as those who improved and Group 2 as those who did not.
Surgical procedure
After a 2–3 cm sub-inguinal incision under spinal or general anesthesia, the spermatic cord is identified. Under 20x microscopic magnification, the spermatic vessels were carefully dissected; only the dilated veins were ligated, preserving other structures such as arteries, vas deferens, and lymphatics. Then, all layers were duly switched and the process was terminated.
Follow-up
All patients were called for follow-up at 1 month, 3 months, and every 3 months for a year. Semen analysis was repeated at least 6 and 12 months after the varicocelectomy operation. Pregnancy status was learned after the operation by receiving telephone and e-mail information from the patients. During the routine controls of the patient, detailed information about the semen analysis changes, and pregnancy results were entried.
Statistical analysis
Statistical analyzes were performed with SPSS Statistics software version 25.0 (IBM, Armonk, NY). The normality of the distribution of the data was investigated with the Shapiro-Wilk testis. Continuous variables were described as proper means and standard deviations or medians and interquartile ranges. Analysis of categorical variables was done with chi-square and Fisher’s exact tests. Quantitative variables were analyzed with Student’s t test and Mann-Whitney U tests. Comparison of the two dependent variables was made with the paired samples t-test. Receiver operating characteristic (ROC) curve analysis was used to describe optimum thresholds with the area under the curve (AUC). Multivariate logistic regression analysis was performed for predictive factors of varicocelectomy success. A p-value of less than 0.05 was defined as statistical significance.
Results
Of the 207 patients who underwent varicocelectomy, 144 (69.6%) of them improved their semen parameters (Group1), and 63 (30.4%) did not (Group 2). The mean age was 24.9 ± 5.4 years. General characteristics of the patients, laboratory, and semen parameters are summarized in Table 1. There were some minor complications after surgery; 4 (1.9%) of these patients had testicular pain, 6 (2.9%) edema, 5 (2.4%) wound infection, and 5 (2.4%) hydrocele.
The general characteristics, laboratory and semen parameters of patients.
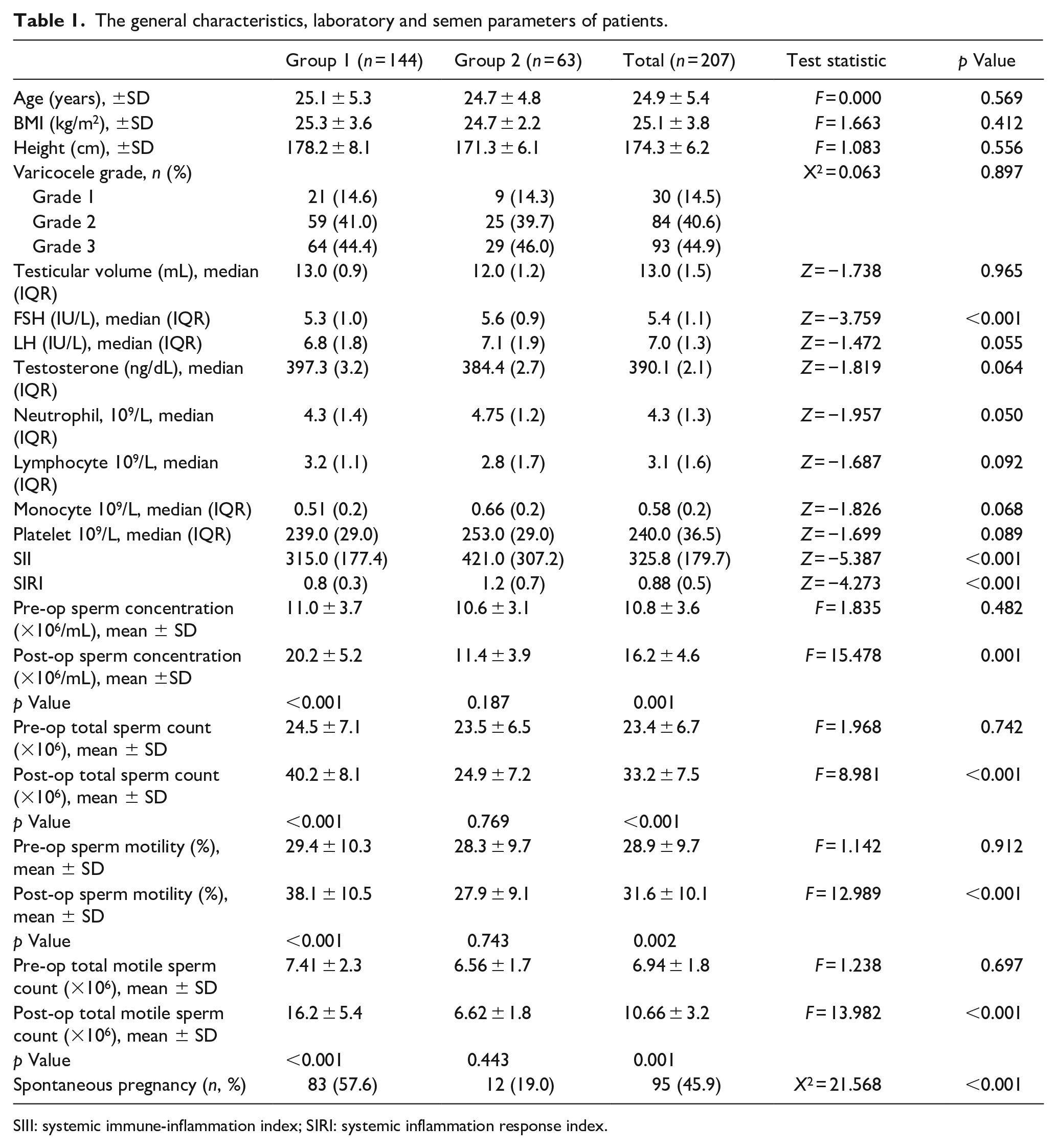
SIII: systemic immune-inflammation index; SIRI: systemic inflammation response index.
The patients in group 1 have significantly lower median FSH (5.3vs 5.6, p < 0.001), SII (315vs 421, p < 0.001) and SIRI (0.8vs 1.2, p < 0.001) levels than group 2. Significant improvements were observed in all semen parameters in group 1 after surgery. The spontaneous pregnancy rate was significantly higher in group 1 in the follow-up after varicocelectomy (57.6%vs 19.0%, p < 0.001) (Table 1).
ROC analysis results are summarized in Table 2. The best cut-off value of FSH was 5.49 IU/L, with an AUC of 0.674 (95% CI: 0.591–0.756). The highest sensitivity and specificity were 0.665 and 0.609 (p < 0.001). The optimum cut-off value that the SII could predict varicocelectomy’s success was 334.6, with an AUC of 0.733 (95% CI: 0.665–0.813). The highest sensitivity and specificity were 0.725 and 0.606 (p < 0.001). We determined the best cut-off value for SIRI of 0.882, which estimated varicocelectomy success with an AUC of 0.692 (95% CI: 0.607–0.772). The highest sensitivity and specificity were 0.692 and 0.601 (p < 0.001) (Figure 1).
ROC analysis of parameters affecting varicocelectomy success.
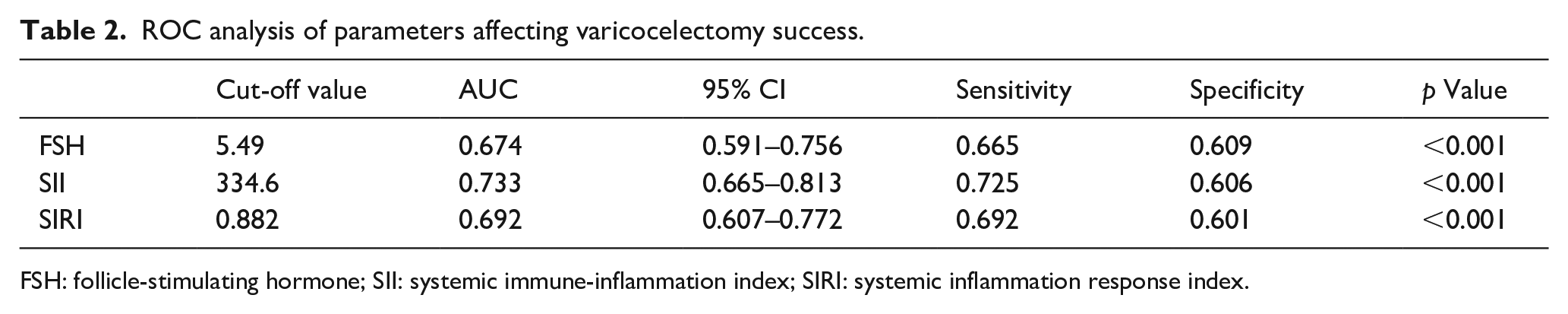
FSH: follicle-stimulating hormone; SII: systemic immune-inflammation index; SIRI: systemic inflammation response index.
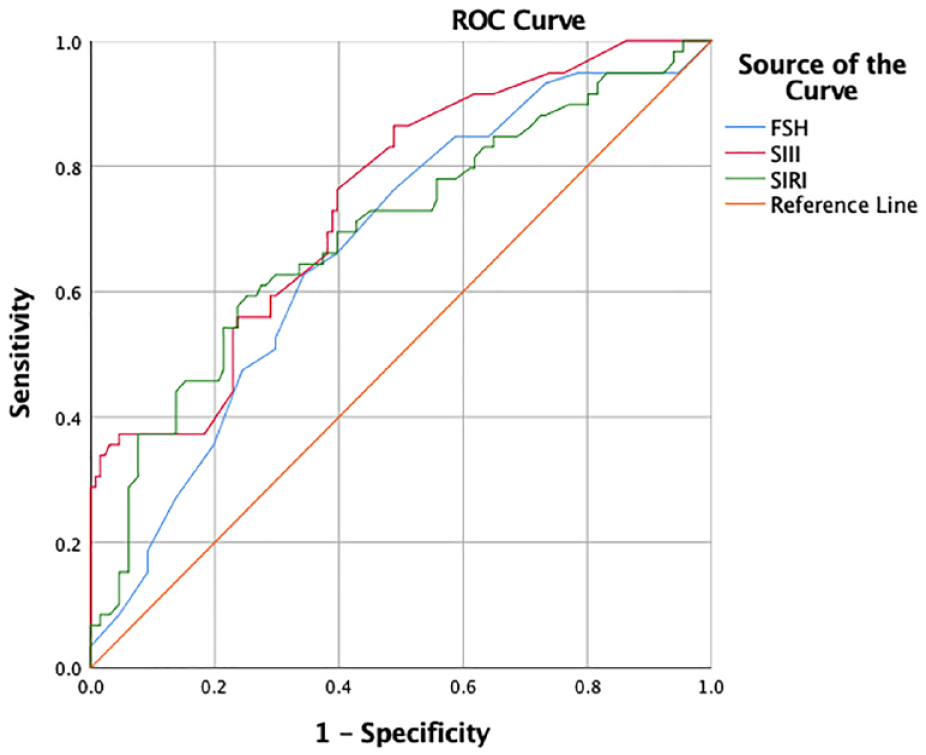
Receiver operating characteristic (ROC) analysis of follicle-stimulating hormone (FSH), systemic immune-inflammation index (SII) and systemic inflammation response index (SIRI).
In the multivariate analysis, only SII (OR: 3.152, 95% CI: 1.316–7.358; p = 0.003) and SIRI (OR: 2.919, 95% CI: 1.472–5.774; p = 0.002) were independent predictive factors for varicocelectomy success (Table 3).
Univariate and multivariate logistic regression analyses of parameters for predicting varicocelectomy success.

FSH: follicle-stimulating hormone; SII: systemic immune-inflammation index; SIRI: systemic inflammation response index.
Discussion
Varicocele is the most common known cause of male infertility. Varicocele causes infertility due to various mechanisms. Inflammation is one of these reasons. It is reported that the increase of cytokines such as ENA-78, and IL-1β in testicular tissue in varicocele patients can cause infertility by many mechanisms.6,16 Some studies try to explain the effects of inflammation on infertility. Nallella et al., thought that the increase in reactive oxygen species (ROS) and the decrease in antioxidant capacity in varicocele patients were effective in varicocele-induced infertility. Besides, they found increased levels of IL-18, which increases neutrophil activation and increases the inflammatory process, in varicocele patients. 17 SII and SIRI have been proposed as a simple, economical, and easily detectable new inflammatory index and have received more attention in recent years; It is calculated according to peripheral neutrophil, platelet, monocytes, and lymphocyte counts. SII and SIRI are related to the occurrence, progression, and prognosis of various diseases in humans such as bleeding disorders, connective tissue diseases, inflammatory diseases, and various malignant tumors.11,18,19
Higher SII and SIRI levels indicated an increased inflammatory response and poor prognosis, according to the findings of previous studies. SII and SIRI values have been studied previously in various cancers and diseases. In a meta-analysis by Li et al., it was found that in urinary system cancers, SII value was associated with overall survival time, while high SII values were associated with a large tumor, advanced tumor stage, and poor differentiation of the tumor. 20 In the study by Cao et al. meta-analysis revealed that high pretreatment SII levels in bladder cancer patients were significantly associated with worse overall survival, cancer-specific survival, and relapse-free survival. 21 In a study with Bechet’s patients, the SII value was shown to be worse. It was higher in active Bechet’s patients and the cut-off value was >552.12 × 103/mm3 when deciding on treatment. 11 In addition, a study conducted on patients with aneurysmal subarachnoid hemorrhage, high SII and SIRI values were shown to be associated with poor prognosis. 12 In a retrospective study of 272 patients with ulcerative colitis, SII and other inflammatory data were compared between 82 patients with ulcerative colitis in remission and 190 patients with active ulcerative colitis. As a result, SII value was found to be higher in active ulcerative colitis patients than in remission patients. The cut-off value for SII was found to be 597.66. 22 In a study performed on systemic lupus erythematosus (SLE) patients, SII and SIRI values were found to be higher in patients with SLE compared to the control group when compared to healthy controls. 23 As far as we know, a study on varicocele patients based on SII and SIRI values is not available. Similar to the other diseases mentioned above, we found that patients who benefited from varicocelectomy had significantly lower SII and SIRI values. Accordingly, we believe that it would be useful to report that patients with high SII and SIRI values before varicocelectomy have a low postoperative success rate.
To the best of our knowledge, our study is the first to examine the effect of SII and SIRI on varicocelectomy success. However, it also has some limitations. Firstly, it is a retrospective study. Secondly, it was done with a small number of patients in a single center.
Conclusion
Our study showed that preoperative SII and SIRI values were lower in patients who benefited from varicocelectomy operation. We believe that low preoperative SII (334.6 × 103/mm3) and SIRI (0.882 × 103/mm3) levels will be beneficial in specifying patients who would utility from surgery in infertile men with varicocele.
Footnotes
Author contributions
E.O. conceived this idea. All authors were involved in the study design and research ethics practice. E.O. and O.F. collected study data. O.F. did statistical analysis. All authors were involved in the writing of the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.