
Abstract
Objectives:
To manage the mandibular traumas, for the expression of the complex anatomy or pathology in education of health sciences related branches, a model of the traumatized mandible is indispensable. For these, different 3D-print-technologies can be used. The aim of this study is, to measure how close these 3D-printed-models are to human-mandible (trueness) and the effectiveness of CT and CBCT at this point.
Study design:
One-dry-human-mandible and 10-models manufactured by five different 3D-printers in four different-kinds of additive-manufacturing technology (Fused-Deposition-Modeling (FDM), Stereolithography (SLA), Binder-jetting (BJ), Polyjet (PJ)) were used, five-anatomic-landmarks and eight-distances were measured and evaluated. Mandible’s data were constructed based on DICOM-3.0 data from CBCT and CT scans. Images were opened in MIMICS (software-program).
Results:
Study compared the devices that produced models with the same dry human-mandible. It was seen that the model with the highest margin of error (132.5 mm) was manufactured by Fused-deposition-modeling device using CT-data. In terms of distance to real-data, the model with the lowest error was generated by Binder-Jetting (ZCorp) with CBCT-data. Models produced with CBCT-data are closer to dry-human-mandible than models with CT-data.
Conclusion:
The current study shows that CBCT generates significantly better data than CT in producing mandibular models. The first choice for manufacturing of human mandible is BJ and the second choice is the technology of SLA.
Keywords
Introduction
Maxillofacial region traumas are the most common injuries occurring in the face and jaw due to accidents, sports, and violence.1,2 The regional distribution of fractures in the mandible according to their frequency can be listed as; condyle, corpus, symphysis, ramus, and coronoid process.1,3,4 It is challenging to replicate the intricate structure of the mandible in minute detail.
In recent decades, mortality rates have decreased significantly due to advances in trauma-management. 5 A crucial element in managing the treatment-protocol is the model of the customized-traumatized-mandible, which is indispensable for preoperative evaluation. Sometimes, customized-implant production is required for mandibular reconstruction surgeries, or 3-Dimensional (3D) models are needed to represent this complex anatomy or pathology in undergraduate and postgraduate-education in health-sciences-related fields. In today’s technology, these productions are carried out using 3D-printing or additive-manufacturing techniques. 6
The most important reasons for choosing additive-manufacturing-technology are; it does not require additional production steps such as production-line-setup or mold-design, the design can be put into production immediately and objects can be obtained using less material than subtractive-manufacturing method. In addition, 3D-printers stand out from other methods with their capability of high geometric-accuracy and resolution. 7 Additive-manufacturing first appeared in the 1980s with stereolithography (SLA). 8 Afterward Fused-Deposition-Modeling (FDM), Selective-Laser-Sintering (SLS), and Direct-Metal-Laser-Sintering (DMLS) were commercialized and marketed in the first half of the 1990s.9,10
FDM, SLA, Poly-jet (PJ, Material-jetting), and Binder-jetting (BJ) can be listed as technologies that make plastic-production. Multicolor prints can be achieved at a low cost with FDM. But some layer traces may appear on the outer surface of the object (ladder-effect) resulting in a lower surface quality, slower printing speed and is not well suited for the production of metal-parts limit its applicability.11,12 SLA excels at creating smooth surfaces with high accuracy. 13 Nevertheless, the removal of support struts can be labor-intensive. 14 PJ is a superior technology that allows for the printing of more than one material or colored parts or hard and soft parts simultaneously. 15 It enables the creation of parts with varying mechanical properties, smooth surfaces, and intricate geometries on a single piece. 16 However high cost and longtime of production can be limiting factors.14,17 In BJ dimensional-distortions due to thermal-effects do not occur because there is no heating process involved. This offers a wide selection of materials; colored parts can be produced at a low cost.
3D-printers that work by different additive-manufacturing methods exhibit varying levels of sensitivity. Irrespective of the purpose of production, it is crucial to ensure that the models precisely replicate reality in terms of quantitative-values. The shape of the part desired to be produced has an impact on dimensional-stability.
When deciding to undertake any production, clinicians or engineers should be well-informed about the most accurate method and device for achieving the desired-model. All of these productions are based on various data formats (such as .stl/DICOM). Data can be generated through Computerized-Tomography (CT) or Cone-Beam-Computerized-Tomography (CBCT).
CT is an ideal imaging-method, especially in lesions involving the bone, as it provide detailed bone information. CBCT is an effective 3D-imaging-technology compared to medical-CT, creates accurate sub-millimetric resolution, diagnostic-quality images, enabling imaging of the osseous structures in maxillofacial-region with lower radiation-dose and cost. 18 Measurements obtained from CBCT appear to be sufficiently accurate and reliable enough for research and clinical-use, with a mean absolute-error of less than 1.5 mm.3,4,19
In this study, we assessed the trueness of mandibular-models printed using different techniques. Additionally, the difference between CT and CBCT images was evaluated in terms of trueness for producing a mandibular-model. The first null hypothesis of this study posits that there will be differences in the accuracy of the lengths between the anatomical-landmarks in the models obtained from different 3D-printers. The second null hypothesis suggests that there will be either no size differences or very minimal size differences between 3D-models produced from data of CT and CBCT imaging-methods.
Methods
Mandibular models were generated using five-different 3D-printers based on images CBCT (3D-Accuitomo-Morita-Japan) and CT (Toshiba-Aquilion-One-320-Slice-CT-Scanner) imaging techniques from a dry human mandible (n = 10) as shown in Figure 1. The CBCT image was acquired at University of Health Sciences, Gülhane Faculty of Dentistry. The CT image was obtained at University of Health Sciences, Gülhane Training and Research Hospital. The study model was depicted in Figure 2. The aim of this study is, to measure how close these models are to dry-human-mandible (trueness). Thus, the sensitivity of the models to be produced for the craniomaxillofacial-region will be evaluated. The study protocol was approved by the Ethics-Committee in the University of Health Sciences, as it complied with the ethical standards of the Research-Ethics-Committee of the University of Health Sciences, Ankara, Turkey (Ref.2023/345).

Dry human mandible.
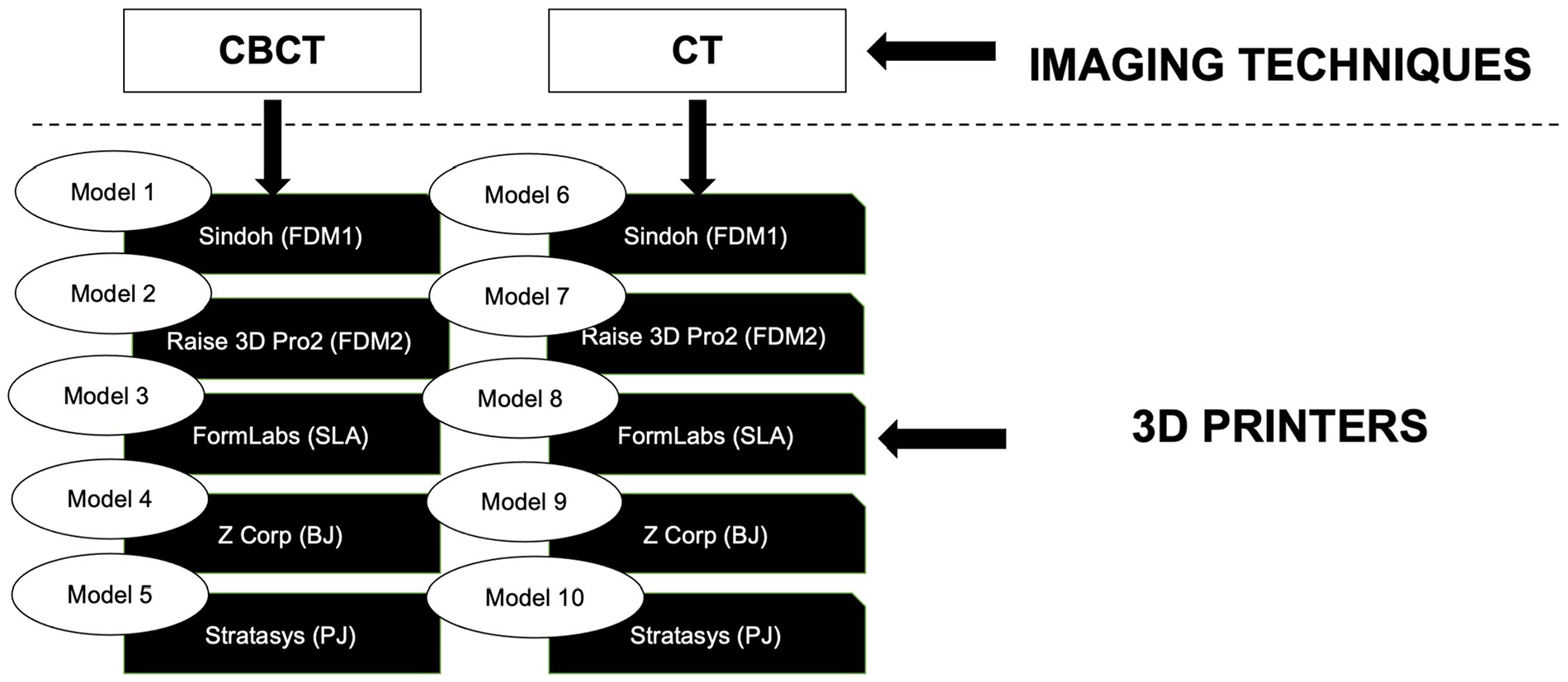
Study model, prepared according to the imaging techniques from which the .stl data of the study models were obtained and production technologies of these models.
When imaging with CBCT, the dry mandible was positioned horizontally and raised on a platform made of suitably sized boxes and books. For CT-imaging, it was placed horizontally on the device’s motorized platform. The images were recorded in Digital Imaging and Communications in Medicine (DICOM-3.0) format after the reconstruction process. The DICOM data were prepared as slices with a thickness of 0.5 mm in the axial, sagittal, and coronal planes. The segmentation progress was performed using MIMICS-software on the axial-plane to remove any scattering and undesirable artifacts from the images. For CBCT images, minimal removal was required since there were very few artifacts.
The images obtained from CT showed more noise in comparison to those from CBCT. Consequently, the CT-images underwent an additional segmentation process to eliminate the noise. During the cleaning of these artifacts, it was necessary to exclude the teeth on the mandible due to the extensive removals required. However, since the teeth on dry-human-mandible were distant from the anatomical landmarks used for evaluation, their removal did not impact the study.
After these processes, the images were prepared for production using 3D-printers in .stl output format. The Segmentation and Manufacturing Processes were conducted at the University of Health Sciences, Medical Design and Manufacturing Center (MDMC/METÜM).
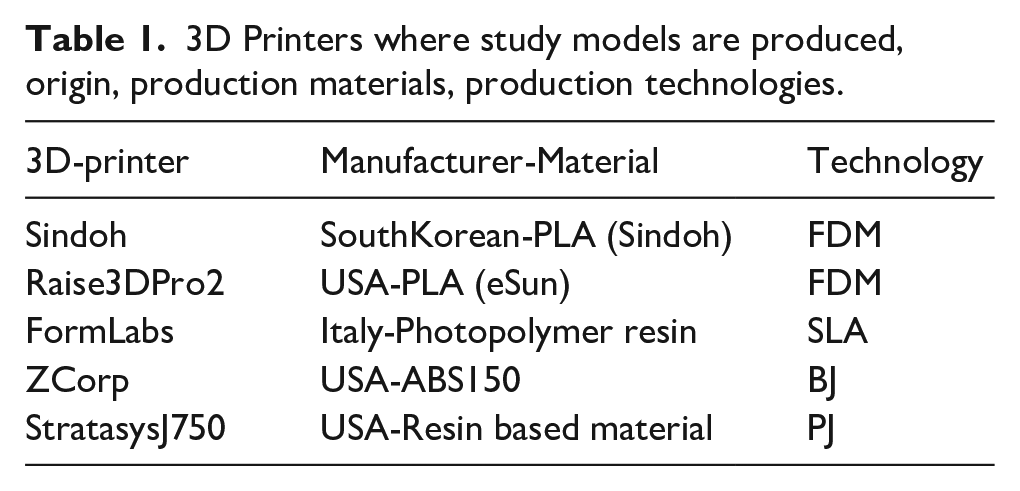
The Manufacturing process involved five different 3D-printers and four different additive-manufacturing techniques, as outlined in Table 1.
3D Printers where study models are produced, origin, production materials, production technologies.
Model-1 and Model-6 were created using FDM (n = 2).
Model-2 and Model-7 were produced using the same technology; FDM with another printer (n = 2).
Model-3 and Model-8 were manufactured through SLA (n = 2).
Model-4 and Model-9 were generated using BJ (n = 2).
Model-5 and Model-10 were produced through PJ (n = 2) (see Figure 3).
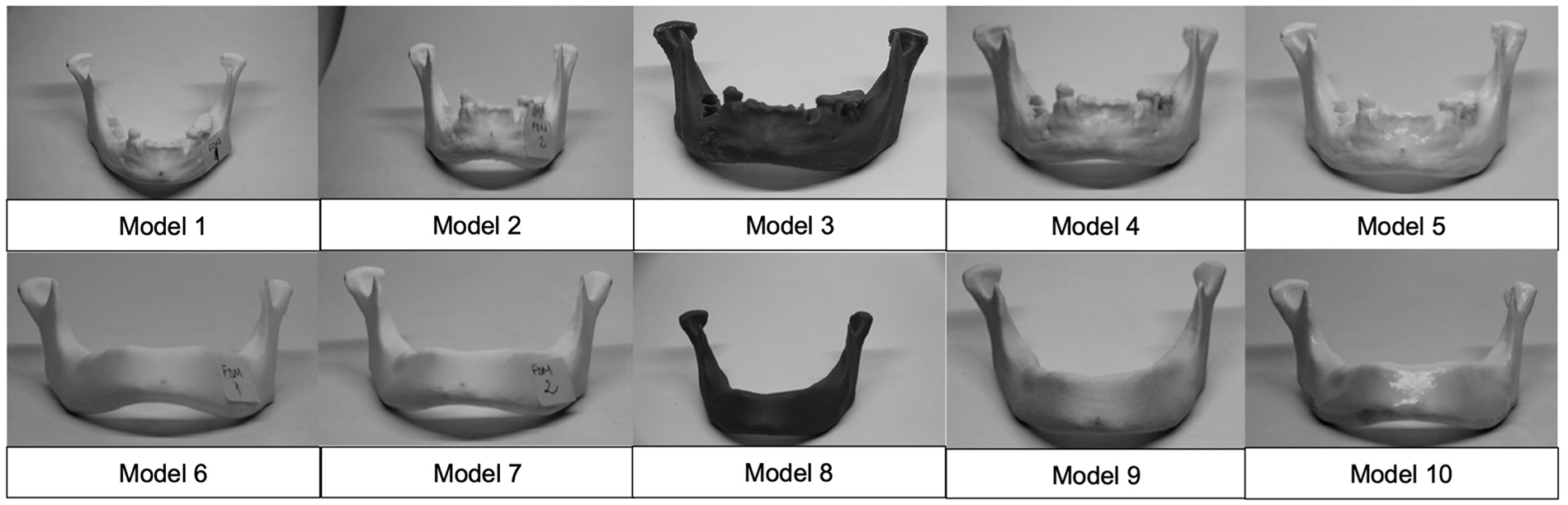
The models that manufactured by additive manufacturing technologies. Model 1-2-3-4-5 were manufactured from CBCT data, model 6-7-8-9-10 were manufactured from CT data.
Anatomical landmarks
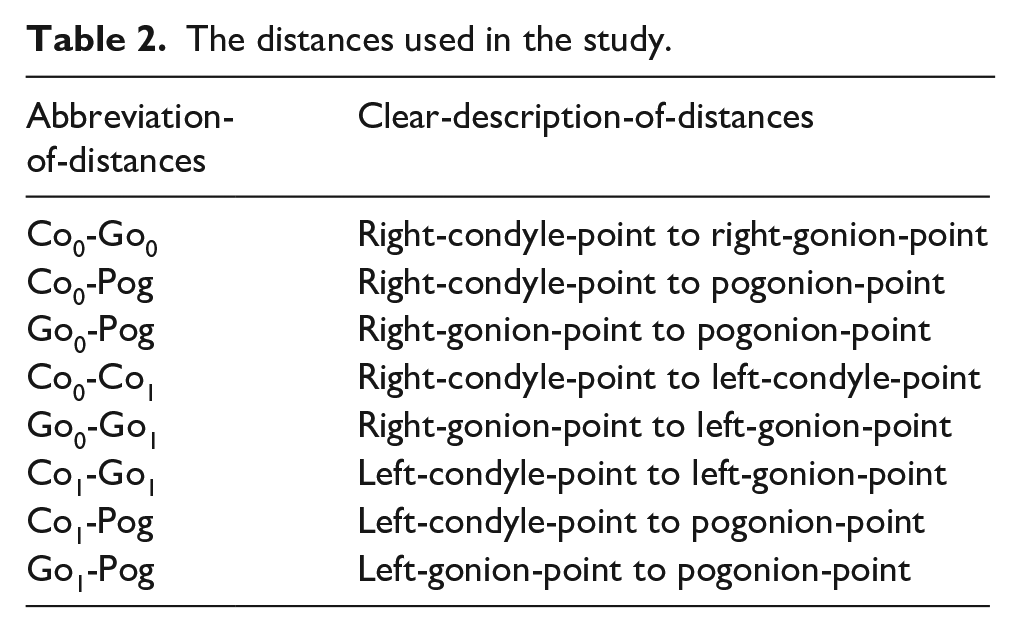
For this study, three cephalometric-points—Condyle (Co)/Gonion (Go)/Pogonion (Pog) were selected. These specific points were chosen because they define the outer boundaries of the mandible and represent areas with the most pronounced curvature. Points on the right were marked with the number “0” (Co0/Go0), while those on the left were marked with the number “1” (Co1/Go1). Pog, being unique, didn’t receive a numerical designation.
The distances selected for measurement were assessed using a digital-caliper-tool. These measurements were conducted on both 3D-printed models and the dry-human-mandible, and the results were subsequently evaluated for accuracy (trueness). The starting and ending points of the measurements are presented in Table 2.
The distances used in the study.
In this study, five anatomic-landmarks (cephalometric-points) and eight distances were used on dry-human-mandible and 10-models were manufactured by 3D-printers. Comparisons were conducted between models and the dry-mandible. The accuracy between CT and CBCT imaging-methods has also been evaluated.
Descriptive-statistics and statistical-tests were em-ployed to assess the significance and compare results. Kolmogorov-Smirnov Normality-test and Shapiro-Wilk Normality-test are compiled to test the normality of the data. Kruskal-Wallis was used for the results of machines as non-normal distribution of data and independent five-groups. Subsequently, the Mann-Whitney-U test was employed to determine the significance of the difference between CT and CBCT results. Following these, mean-square-error and deviations were performed to compare the results.
Results
Focused on the comparison of models and measurements data non-normally distributed (p < 0.00) between independent-groups. The data were consisted of eight-observations; mean/median/variance/standard-deviation/min/max were shown in Table 3. Significant difference were detected between printers (p = 0.009) as a result of the Kruskal-Wallis. Statistical calculations were performed to calculate the error associated with each device. It was seen that the model with the highest margin of error was manufactured by FDM1 using CT-data. Measurement values the furthest from the real mandible was the FDM1-model was manufactured from CT-data.
Mean, median, variance, standard deviation, min and max of the study’s data were show.
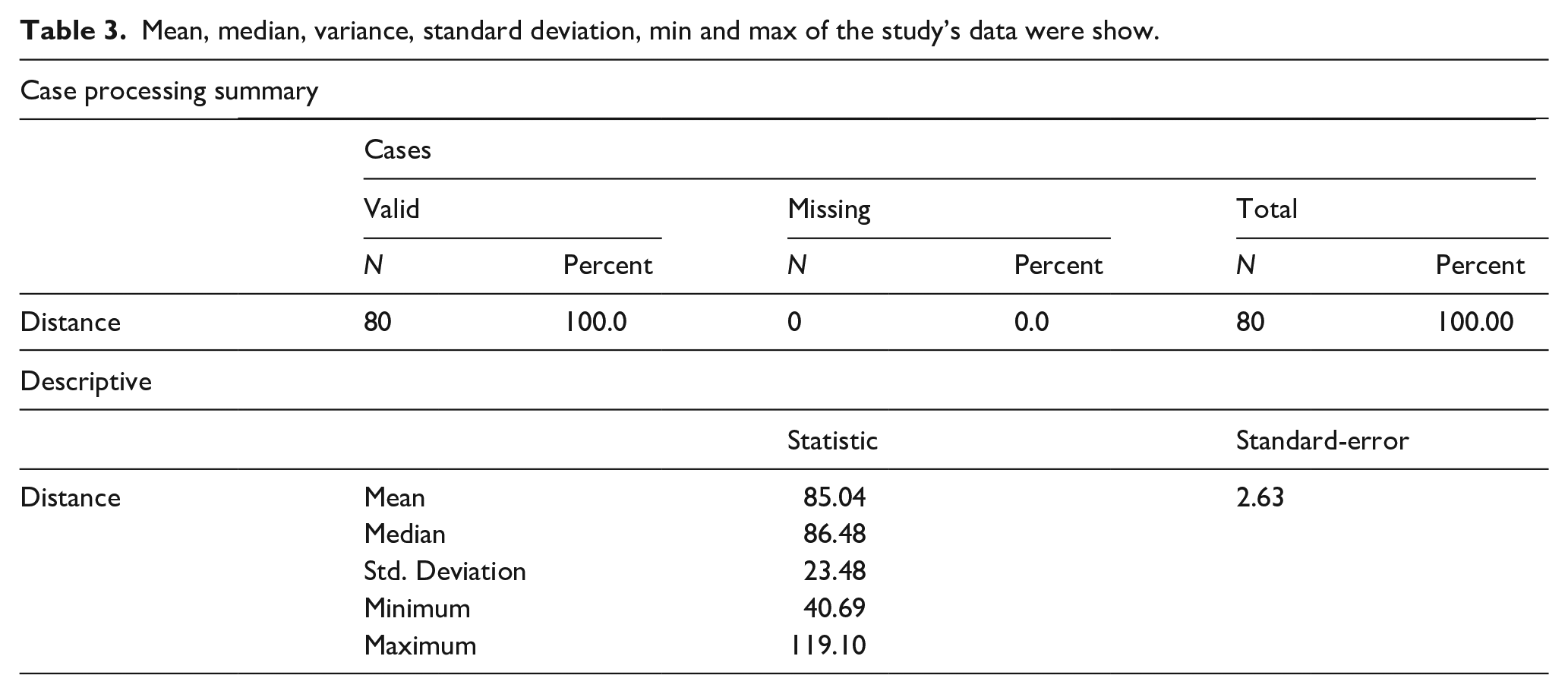
In all groups examined, in terms of distance to real-data, the model with the lowest error was generated by BJ with CBCT-data.
Furthermore, the comparison criteria were switched from device to imaging-techniques. It was observed that models produced using CBCT-data were closer to the dry-human-mandible compared to models created using CT-data. The machine errors of the models produced with CT-data were very high compared to CBCT.
The percentage of deviations of models from the real were evaluated for the machines. BJ (ZCorp)-CBCT model achieved the closest result to the dry-human-mandible with the highest trueness, of error of 0.8%, which is less than 1%. On the other hand, the FDM1-CT model gave the result of the furthest from the real with 5.5%.
As the data of CT and CBCT were numeric and not distributed normally, the Mann-Whitney-U-test was used to compare the difference between CT and CBCT. There was a significant difference between the results (p = 0.007).
The results of the models produced with CT and CBCT data for each printer were combined. The model with the lowest error rate was produced using the BJ-technology. This was followed by the PJ-technology. Models produced using the Raise-pro device, which works with FDM-technology, and models produced using SLA had nearly identical error-rates. The model with the highest error-rate was once again produced using the FDM-technology, but this time with the Sindoh device.
The root-means-square errors (RMSE) of machines were calculated. Measurements obtained from models generated by CBCT-images have shown numerical accuracy that is 20-times closer to reality compared to measurements on models generated by CT-images (Table 4).
RMSE of the imaging techniques according to real human mandible, deviation of percentage of imaging technics from the real.
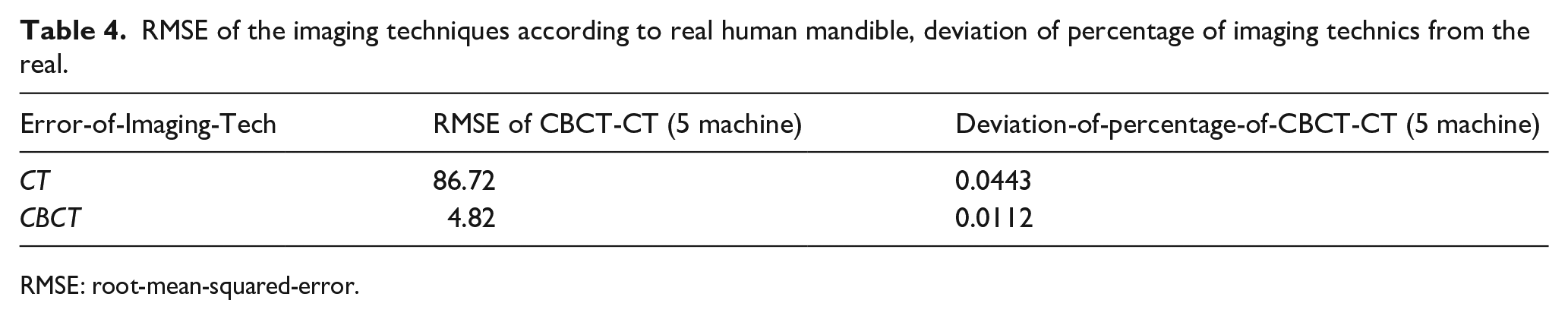
RMSE: root-mean-squared-error.
The distance to real-data (RMSE) for the models generated by CBCT was less than the ones generated by CT. The trueness of the models obtained from the CBCT-data was significantly higher (Figure 4).
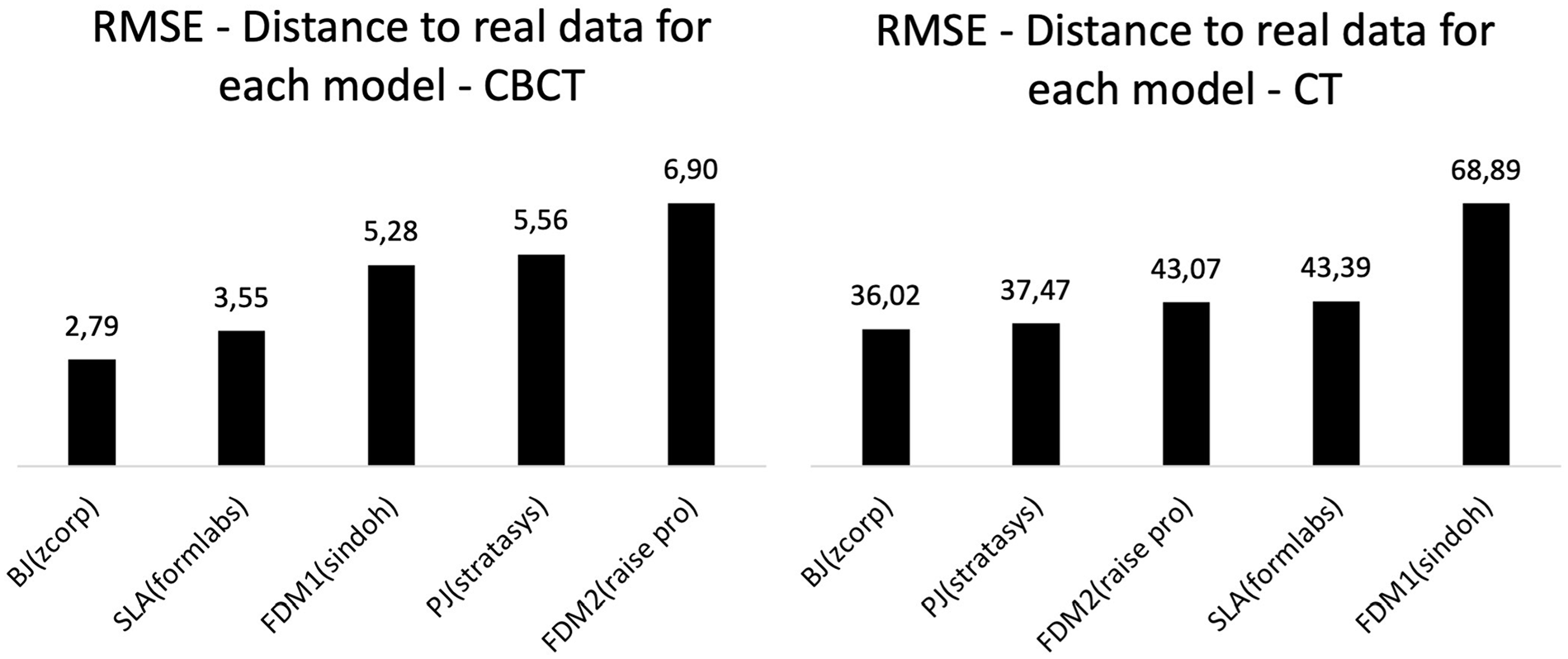
RMSE values of all models produced from CBCT and CT.
The Kruskal-Wallis test was conducted to evaluate the models obtained from both CT and CBCT images within themselves Significant differences were found among the models generated from both CT (p = 0.036) and CBCT (p = 0.049) images. Based on these results, it can be said that regardless of whether the model is produced by CT or CBCT-data, BJ-technology is superior to the others in terms of the production of a mandible that is the closest to the real one.
The limitations of the study
In the study, DICOM-data required for 3D-production were obtained with CT and CBCT-techniques. There was a large amount of noise-artifact in the images obtained with the CT-technique. To perform 3D-production, the noise was cleaned in the MIMICS-program. However, there were dimensional losses in the image in this cleaning process and the dimensional accuracy of the models obtained from these data was low. Noise in tomography-images was a limitation in evaluating CT accuracy.
Discussion
The objective of this study was to evaluate and compare the 3D-printers’ accuracy and dimensional suitability through CT and CBCT for the 3D-modeling process. Based on the results, the first null hypothesis stating that the lengths between the anatomical-landmarks would differ in the models produced by different 3D-printers was accepted. However, the second null hypothesis, which suggested that there would be no or very minor differences between 3D-models produced from data obtained by CT and CBCT, was rejected. Dimensionally significant differences were revealed in the models obtained using different imaging-technique data.
Accuracy stands as one of the most crucial evaluation parameters in the realm of 3D-printing. The present study was assessed the lengths based on deviation-calculations.
Türker et al. were evaluated SLA 3D-printing technology on mandibula with different dental-guide designs by using artificial-intelligence. Similar to our study, the productions made using SLA-technology exhibited measurements remarkably close to the real. 20 In another study conducted by Chen et al., 21 it was reported that while PolyJet-technology exhibited higher repeatability and accuracy than SLA-technology in the production of maxillary surgical-templates, the difference between them may not be clinically significant. Based on these, it can be said that technology of both SLA and PJ have produced highly realistic successful models.
In this study the model that deviated the most from reality was manufactured by FDM-technology (FDM1, Sindoh), .stl data was produced from CT-scan. Conversely the highest trueness values were obtained from BJ-printer (ZCorp) using CBCT-data. The models obtained from CT-data presented lower trueness which can be attributed to the presence of considerable noise in the CT-images acquired with Toshiba-Aquilion-One-320-Slice-CT-Scanner. The soft model required extensive cleaning in MIMICS before production.
Danilo et al compared the technologies of SLS, BJ, and PJ on mandibula by CT-.stl data. Their findings indicated that the model produced by SLS-technology provided measurements closest to reality, followed by PJ and BJ. 22 The present study’s models were generated using both CT and CBCT. When comparing of PJ and BJ-technologies, BJ exhibited higher accuracy in models obtained from both CT and CBCT-.stl-data. Notably while models obtained from CT-data displayed relatively similar measurements, those from CBCT-data showed a more significant margin in favor of BJ in terms of accuracy. This discrepancy suggests that 3D-printing-methods have developed at varying rates over time. Even though the technology of BJ seems superior, has some disadvantages such as high-cost, covering a large area, and long and laborious post-process. In contrast the present study reveals a marginal difference in terms of RMSE between the technology of BJ and SLA. The technology of SLA is superior to BJ in terms of cost, the area it occupies, and ease of post-process. Therefore, it can be stated that within the parameters defined in the study, SLA-technology can be used as an alternative to BJ-technology.
In another study SLS-prototypes (polyamide-powder, DTM, USA) demonstrated higher precision and more accuracy compared to BJ-models (plaster-powder, ZPrinter-310-System, USA) with CT-derived data. 23 However, SLS-technology can be challenging to use due to its cost.
A similar study was conducted using 3D-printing-technologies. But unlike the current study, data was obtained by scanning a human-dry-mandible with an optical-white-light-desktop 3D-scanner. 24 In that, the production closest to real-data was achieved using SLS-technology followed by BJ, Fused-Filament-Fabrication (FFF), PJ and the farthest one emerged with SLA. This study used a scanner for data-digitization while the current study used CT and CBCT. These different digitalization approaches can lead to variations in the results, as confirmed by the results of Msallem’s study. 24
The CT and CBCT that we used in the study were evaluated in terms of additive-manufacturing. The model which was produced by BJ (from-CBCT-data) has the closest measurements to the real-data, followed by SLA. The difference in accuracy for SLA, which was the second most sensitive method in this study, may be attributed to differences in the brand and model of the machine, as well as variations in the digitalization-method of the model. Notably, models obtained from CBCT-data displayed higher accuracy compared to those from CT.
FDM-printer can achieve rapid production. 25 But it may not adequately represent detailed-structures.25,26 However researches indicates that FDM-technology holds a significant place among additive-manufacturing options. 27 It’s crucial to consider why the clinician requires 3D-printing-model. The answer to this question should guide for determining the required accuracy and the choice of 3D-printer. This necessitates effective communication among radiologist, clinical team, and requesting clinician. 14
In another study, FDM, SLA, BJ, PJ, and SLS methods were compared, with .stl-data obtained via industrial-3D-scanner. Overall, all methods provided accurate results. In terms of volumetric-comparison, the best results were achieved with SLA and SLS. 28 In the present study, BJ-technology has outperformed SLA-technology when using CBCT-data for linear-measurements. This outcome suggests that even within the same technology, different brands can yield different results. Additionally, it raises the question of whether data obtained by an industrial-3D-scanner is sufficient for clinical applications.
Some researchers have proposed that dimensional-measurements within a 2% range will not significantly impact the success of surgical procedure. 29 However, this limit suggested by Asaumi should be discussed, as the same accuracy may not be required in all indications, so it may not be universally applicable to all cases.23,30,31
In a study using .stl-data obtained through Multi-Slice-Computerized-Tomography (MSCT)-scanner, Hesham has concluded that SLA and FDM-techniques can be used safely in dental-applications. 32 The current study revealed significant differences in linear-measurements (on-all-3D-printers) between models produced from CT and CBCT-data. But, in Hesham’s study no significant differences were found in linear-measurements in terms of FDM and SLA-technologies. Different digitization methods produces different production outcomes.
For treating hard-tissue losses due to tumors in the maxillofacial region, additive-manufacturing-techniques in the form of customized-implants have been evaluated compared to conventional-methods. It was found that patients treated with customized-products post-surgery had higher rates of successful recovery. 33 Customized-implants for maxillofacial-defects’ treatment or customized models for preoperative evaluation can significantly enhance treatment effectiveness.
This is the first study that compared additive-manufacturing-methodologies with CT and CBCT data from dry-human-mandible.
Conclusion
The current study demonstrates that CBCT generates substantially more accurate data than CT for producing mandibular-models those are closest to reality in terms of lengths between certain anatomical-landmarks. The ranking of machine accuracy is as follows (higher to lower): BJ (Z-Corp), PJ (Stratasys), FDM2 (Raise-pro), SLA (Formlabs), and FDM1 (Sindoh). 3D-Printer evaluations from the highest to the lowest in terms of trueness in productions generated from CBCT-data are, BJ, SLA, FDM1, PJ, FDM2; for CT-data, from higher to lower BJ, PJ, FDM2, SLA, FDM1. With both tomographic techniques, BJ-technology produced the greatest results. The trueness of the models derived from CBCT-data was significantly greater. BJ is the technology of preference for manufacturing human mandibles, while SLA is the technology of second-choice. However, in today’s technology, ease of production and low-cost of SLA-technology could be an efficient option.
The method in which data of the production is obtained and the 3D-printer-technology directly affect the dimensional-measurements of the 3D-model to a greater or lesser extent.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.