
Abstract
Multisystem inflammatory syndrome (MIS-C) is a new severe clinical condition that has emerged during the COVID-19 pandemic. MIS-C affects children and the young usually after a mild or asymptomatic COVID-19 infection. MIS-C has a high tropism for the cardiovascular system with need for inotropes and vasopressor support in 62% of cases. As of today a mortality from 1.5% to 1.9% related to MIS-C is reported. Hemoadsorption via the inflammatory mediator adsorber CytoSorb (CytoSorbents Europe, Berlin Germany) has been used as adjunctive therapy with the aim to restore the host response in septic shock and other hyper-inflammatory syndromes. We present the clinical experience of an adolescent boy with a refractory shock secondary to left ventricular dysfunction (LVD) in the context of MIS-C, treated with hemoadsorption, and continuous kidney replacement therapy (CKRT) in combination with immunomodulatory therapies. The therapeutic strategy resulted in hemodynamic and clinical stabilization as well as control of the hyperinflammatory response. Treatment appeared to be safe and feasible. Our findings are in line with previously published clinical cases on Cytosorb use in MIS-C showing the beneficial role of the hemoperfusion with Cytosorb in severe MIS-C to manage the cytokine storm. We provide an analysis and comparison of recent evidence on the use of hemoadsorption as an adjuvant therapy in critically ill children with severe forms of MIS-C, suggesting this blood purification strategy could be a therapeutic opportunity in severe LVD due to MIS-C, sparing the need for extracorporeal membrane oxygentation (ECMO) and other mechanical cardiocirculatory supports.
Keywords
Introduction
Multisystem inflammatory syndrome in children (MIS-C) is a clinically severe condition that was first described during the coronavirus 2019 (COVID-19) pandemic. This new phenomenon appears to be temporally, geographically, and epidemiologically related to the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection. 1 Most of the children affected have a positive SARS-CoV2 serology with a negative Reverse Transcription-Polymerase Chain Reaction (RT-PCR), indicating previous infection. It was hypothesized that a “cytokine storm” might be responsible for MIS-C, increased interferon signaling and high plasma levels of interleukin (IL)-6 and IL-10 were described by Cheung et al. 2 Diorio et al. 3 reported that the combination of IL-10 and TNF-alpha levels uniquely identifies MIS-C from severe COVID-19, while Consiglio et al. 4 observed that IL-6, IL-17A, and CXCL10 contributed the most to the cytokine storm.
The clinical picture in MIS-C is characterized by prolonged fever, nonspecific symptoms such as fatigue, headache, and mucocutaneous findings, with a high prevalence of gastrointestinal symptoms (71%) and cardiovascular dysfunction (82%). 1 Notably, cardiac involvement requiring inotropic support has been observed in 63% of cases and was the predominant reason for intensive care support (68%). Cardiovascular support is most common in cases where mechanical ventilation is required. 1 However, myocardial dysfunction improved in many cases with immune-modulatory drugs where the rate of Extracorporeal Membrane Oxygenation (ECMO) use (4%–6.3%) and mortality (1.5%–1.9%) are high.1,5 In particular, in their metanalysis Radia et al. reported that from the 12 children included in the study, 7 died while on ECMO. Given the severity of this condition, there is an urgent need to identify the best therapeutic strategies.
Increasingly more reports are appearing in the literature that describe the use of hemadsorption with Cytosorb as a supportive therapeutic intervention in critically ill children with cytokine storm-related multiple organ dysfunction, including cytokine release syndrome after chimeric antigen receptor (CAR)-T -cell infusion, and secondary hemophagocytic lymphohistiocytosis (HLH). 6 Indeed, CytoSorb is an extracorporeal adsorber which has been demonstrated to remove cytokines from the plasma, and it has been postulated that the use of hemoperfusion containing these highly biocompatible sorbents might potentially provide support to various organs in COVID-19 patients.7,8
We present a new clinical case of a 13 years old boy with severe myocardial dysfunction, with evidence of overlapping MIS-C and viral myocarditis and review and compare recent evidence and the potential role of hemoadsorption as an adjuvant therapeutic strategy in critically ill children with severe forms of MIS-C characterized by cardiogenic shock.
Case report
The 13 years old boy (weight 60 kg, height 160 cm) presented with fever, rash, abdominal pain, and vomiting. Blood tests revealed elevated leukocytes with neutrophilia, high C-reactive protein (CRP) (29.31 mg/gL), procalcitonin (3.32 ng/mL), hyperferritinemia (1529 ng/mL). He had a positive history for SARS-CoV-2 infection 6 weeks previously with positive serology. Within 24 h he developed diarrhea, poor pallor, and hypotension. Cardiac markers were elevated, and 2D-echocardiogram showed left ventricular (LV) dysfunction (Ejection Fraction (EF) 35% calculated by Simpson biplane method). Supportive care with milrinone and dopamine was started and, as MIS-C was suspected, he received immunoglobulins and corticosteroids. The following day he deteriorated with an 2D-echocardiogram showing an EF of 25%, therefore he was referred to our pediatric intensive care unit (PICU) requiring endotracheal intubation and invasive mechanical ventilation (IMV) due to cardiogenic shock.
Given the increase in troponin I (high sensivity troponin, hs-TnI) levels from 75 to 1200 pg/ml in 12 h, infectious myocarditis was suspected and an endomyocardial biopsy (EMB) was performed. Considering the clinical picture of hyperinflammation associated severe shock due to the left ventricular dysfunction (LVD) and high lactate (7.9 mmol/l) with the need for high inotropic support (epinephrine 0.35 µ/kg/min, norepinephrine 0.06 µ/kg/min, Milrinone 0.5 µ/kg/min) hemoperfusion with Cytosorb was started in combination with continuous kidney replacement therapy (CKRT). The patient was placed on a citrate-calcium anticoagulation protocol.
EMB histology showed diffuse infiltration of lymphocytes and monocytes (CD3+++, CD4, CD8++, TIA-1+, Granzime B+, CD20+/−, and MUM1−) with myocyte fragmentation and necrosis (Figure 1) Nested PCR and RT-PCR for the detection viruses showed the presence of Parvovirus B19 (PVB19), but did not detect SarS-CoV-2 RNA in the myocardium. Serological test for PVB19 returned positive for IgG and negative for IgM.
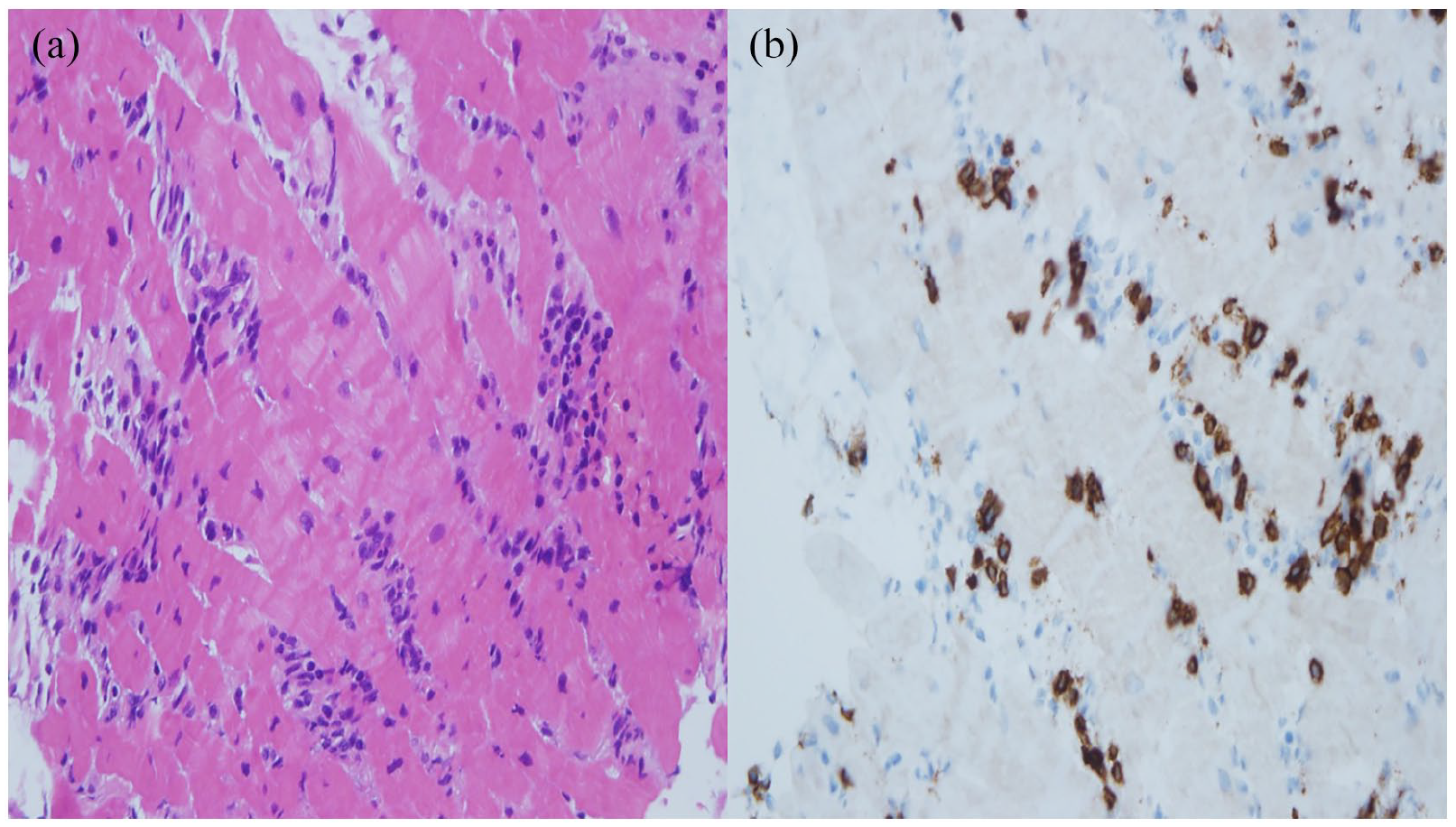
(a) Endomyocardial biopsy (EMB) histology shows a mononuclear, predominantly lymphocytic, inflammatory infiltrate, and myocardial injury with necrosis (HE, 40×). (b) Immunohistochemistry with anti-CD3 revealed a rich T-lymphocytic component (CD3, 40×).
PVB19 is a frequent causative agent of myocarditis that commonly induces cardiac dysfunction but also gastrointestinal symptoms. Of note, even though the patient fulfilled the diagnostic criteria of MIS-C, we cannot completely rule out the development of fulminant myocarditis due to PVB19 after suffering from COVID-19.
Due to PVB19 positivity, corticosteroids were withheld and immunoglobulin and anakinra were maintained. Blood purification continued for 72 h (the sorbent was changed every 12 h in the first 24 h, then every 24 h). We already observed an improvement in the LV-EF. after the first 24 h of hemoperfusion and CKRT. Inflammatory and cardiac markers reduced and inotropes were progressively tapered off (Figures 2 and 3). The most of laboratory tests improved in the same time (Figure 4). CKRT was discontinued at the same time of hemoperfusion after 72 h (day 3), and there were no adverse events noted. He was weaned off invasive mechanical ventilation on day 6 and discharged from the PICU on day 8.
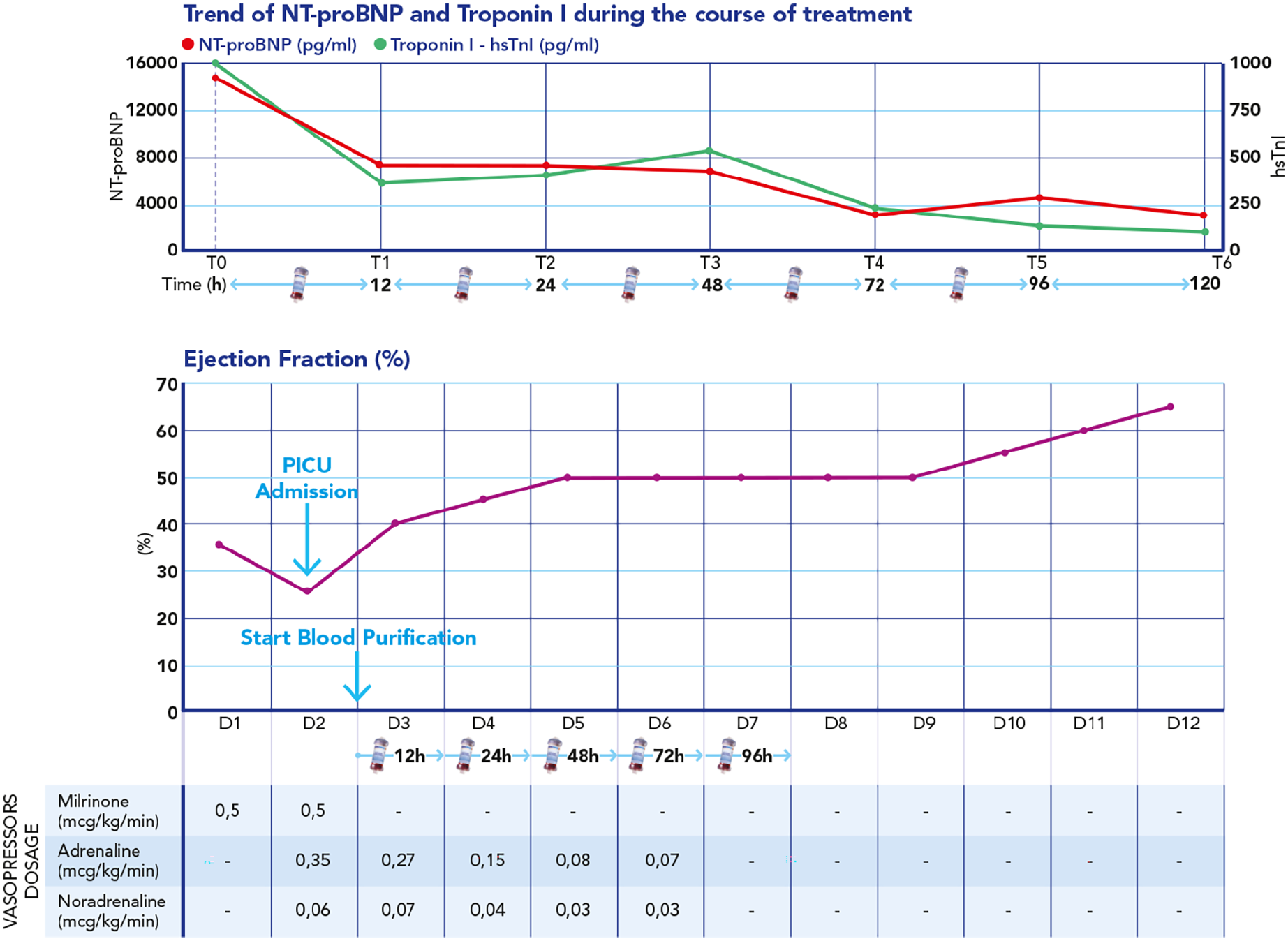
Upper section: time course of N-terminal (NT)-pro hormone brain natriuretic peptide (BNP) (NT-proBNP) and Troponin I (high sensivity troponin hs-TnI) during extracorporeal blood purification treatment (EBPT). Lower section: time course of the ejection fraction during EBPT.
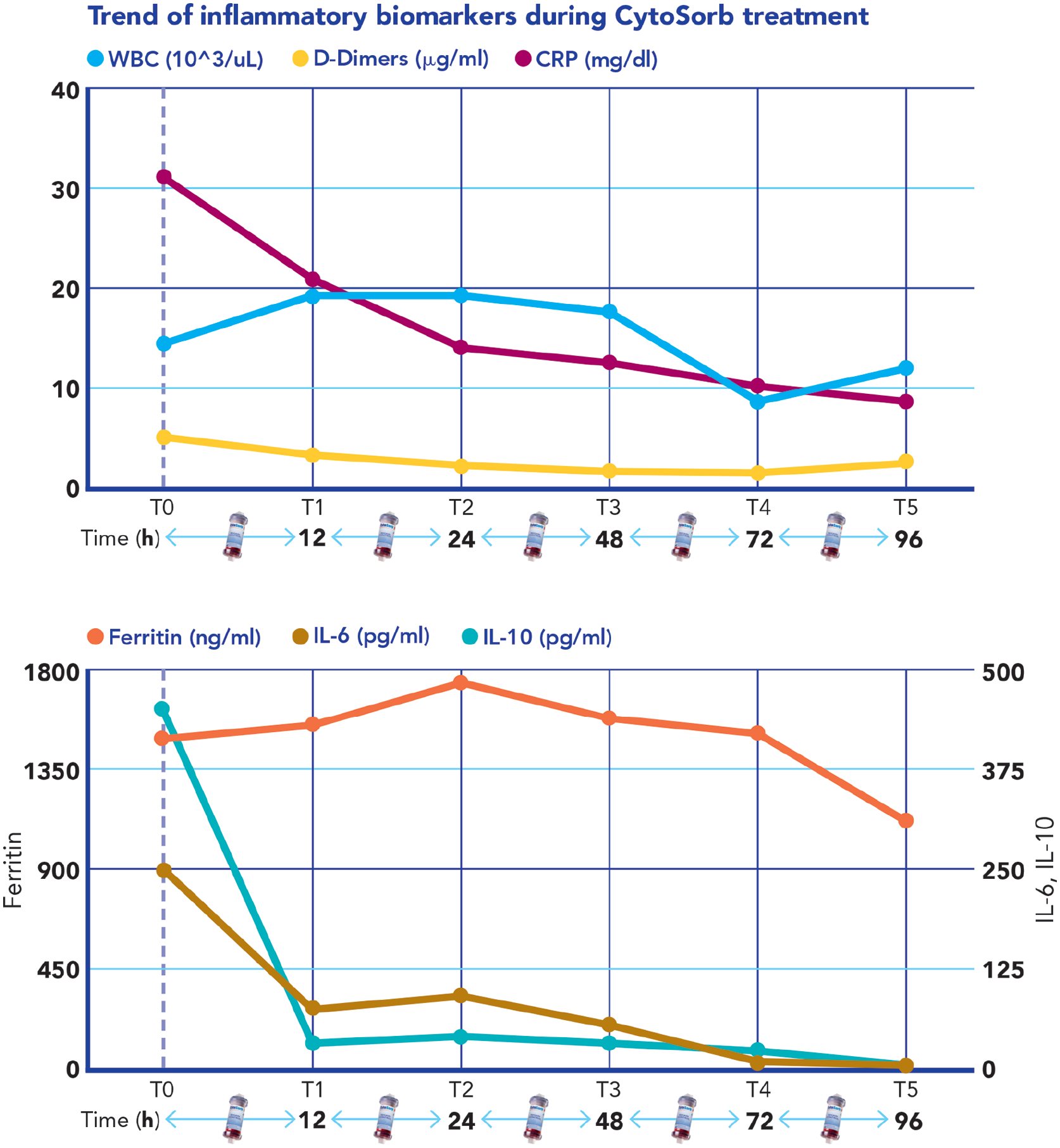
Upper section: time course of White Blood Cells (WBC), D-dimers, and C-reactive protein (CRP) during extracorporeal blood purification treatment (EBPT). Lower section time course of Ferritin, Interleukin 6, Interleukin 10 during EPBT.
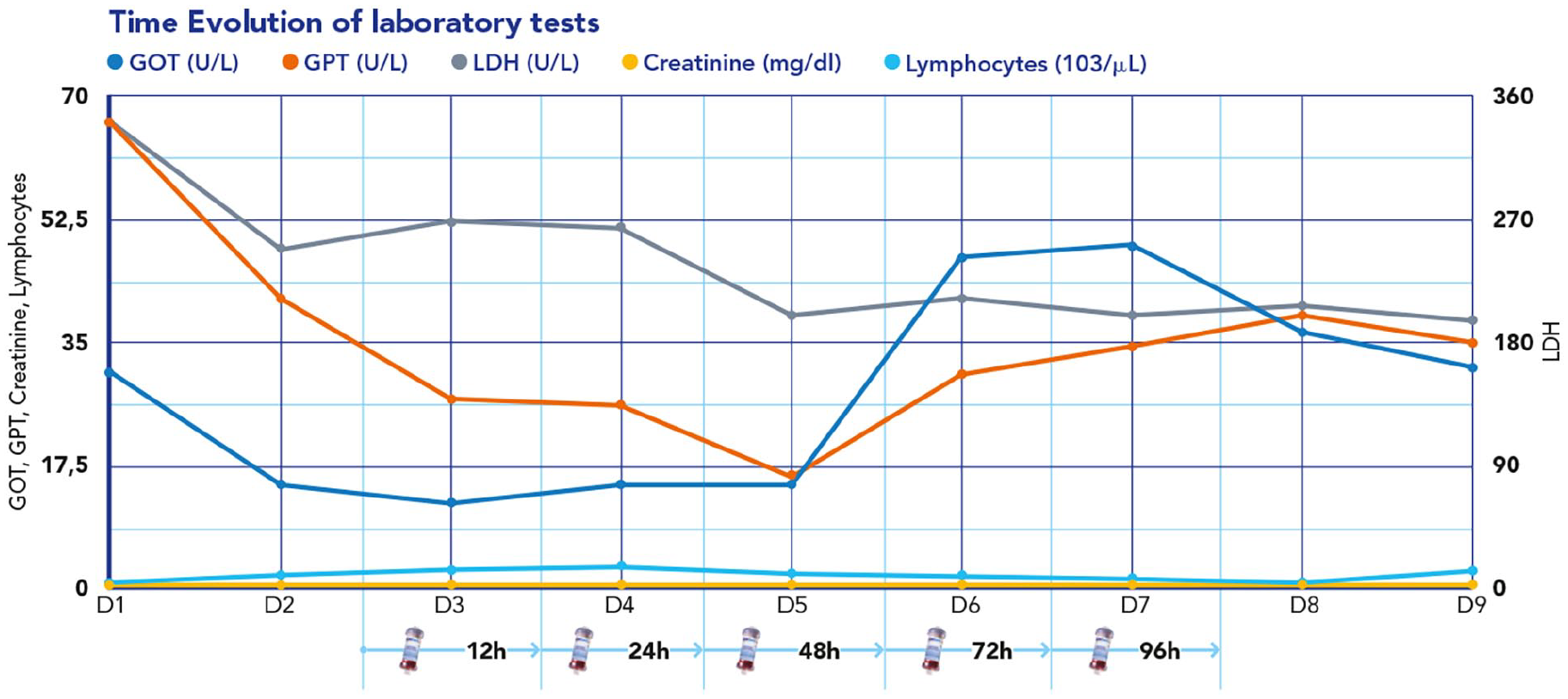
Time course of Lymphocytes, Lactate Dehydrogenase (LDH), Creatinine, aspartate aminotransferase AST, alanine aminotransferase ALT during Extracorporeal Blood Purification Treatment (EBPT).
After 2 weeks his cardiac function had completely restored and the patient was discharged from the hospital on day 20 requiring only spironolactone.
Discussion
The exact mechanism of myocardial dysfunction in MIS-C is still poorly understood. Due to the fact that EMB is rarely performed, diagnosis is largely based on clinical symptoms, laboratory results and findings from imaging. SARS-CoV-2 can infect macrophages and also myocytes, but the virus is in most cases not cytolytic. 9 It is likely that SARS-CoV-2 rather induces an inflammatory response by cytokine release, thus resulting in indirect cytotoxic myocardial injury. 10
Our patient fulfilled the diagnostic criteria of MIS-C: looking at the CDC criteria which confirm the diagnosis of MIS-C in contrast to other infections, and we concluded that the child had overlapping MIS-C and viral myocarditis, both of which probably contributed to the myocardial dysfunction. 11
In this adolescent with refractory shock secondary to LV dysfunction in the context of MIS-C, treatment with hemoadsorption in combination with immunomodulatory therapies resulted in hemodynamic and clinical stabilization as well as control of the hyperinflammatory response. Treatment appeared safe and feasible.
We have previously described the successful treatment of severe MIS-C in a 14-year old girl with CytoSorb hemoadsorption plus CKRT and immunomodulatory drugs (described as patient B in Table 1). 12 Ruiz Rodriguez et al. recently also reported the use of hemadsorption as part of the supportive treatment in a 17-year old boy with severe MIS-C (described as patient C in Table 1). 13 Including our present case (described as patient A in Table 1), these three patients all developed shock secondary to severe myocardial dysfunction requiring inotropic support and IMV (Table 1).
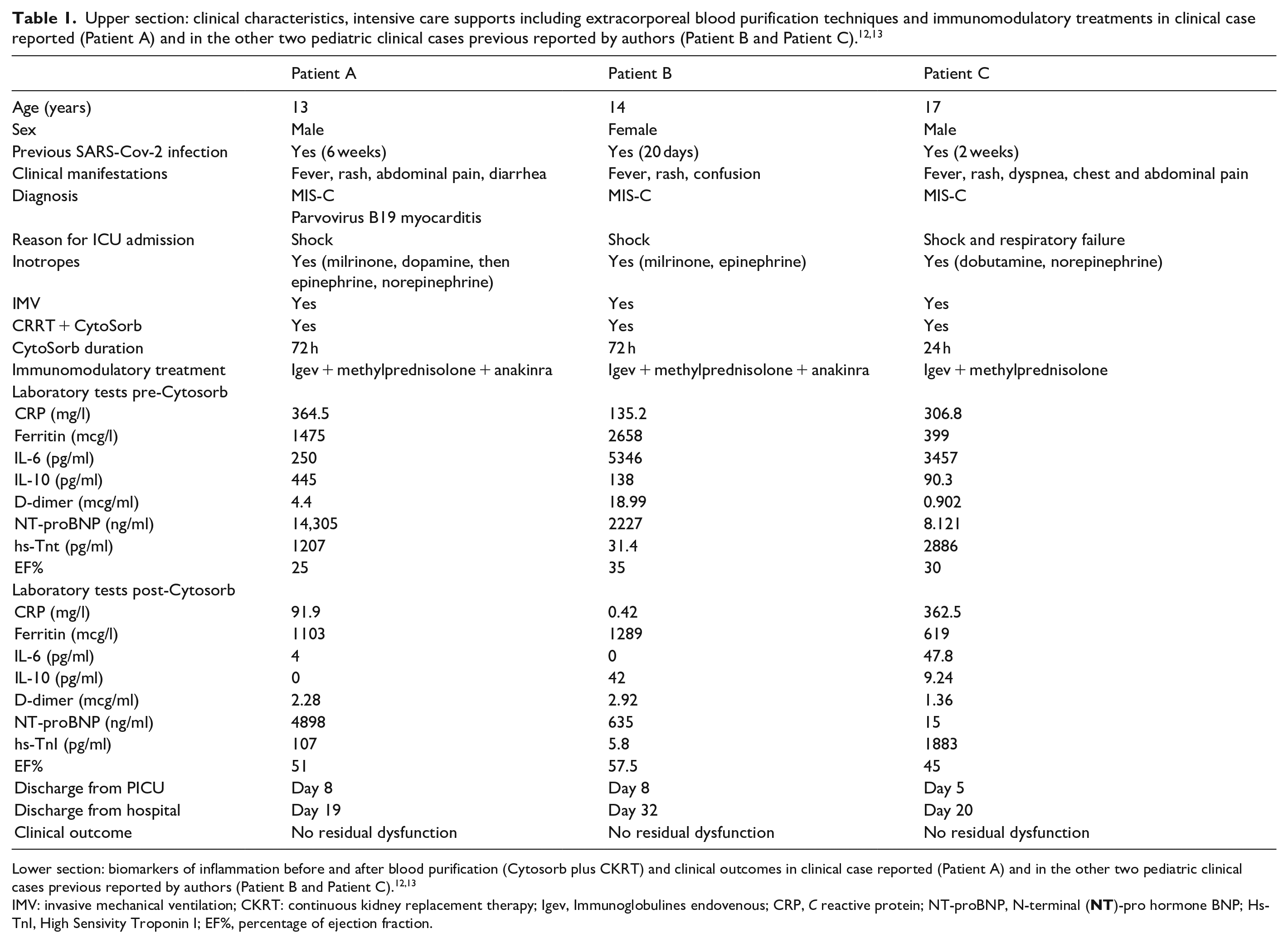
Lower section: biomarkers of inflammation before and after blood purification (Cytosorb plus CKRT) and clinical outcomes in clinical case reported (Patient A) and in the other two pediatric clinical cases previous reported by authors (Patient B and Patient C).12,13
IMV: invasive mechanical ventilation; CKRT: continuous kidney replacement therapy; Igev, Immunoglobulines endovenous; CRP, C reactive protein; NT-proBNP, N-terminal (NT)-pro hormone BNP; Hs-TnI, High Sensivity Troponin I; EF%, percentage of ejection fraction.
Patient A and Patient B required IMV due to cardiogenic shock, Patient C required IMV not only for hemodynamic reasons but also for a concomitant clinical picture of bilateral pneumonia. The time lapse in the three cases to receive blood purification support from the onset of the low cardiac output syndrome ranged between 24 and 48 h. High levels of inflammatory biomarkers are reported in all cases, in particular IL-6 values were significantly higher than 100 pg/ml (Table 1). The duration of blood purification ranged from 24 to 72 h. In the two patients treated at our center, the first two CytoSorb cartridge columns were changed every 12 h in the first 24 h.6,12,14 The patients also received immunomodulatory treatments (Table 1). All three patients responded with a prompt improvement in their myocardial function (within the first 24 h) following the start of hemadsorption. A dramatic decrease in inflammatory cytokines (IL-6 and IL-10) was observed, as well as a reduction in inflammatory markers (CRP, ferritin, D-dimers) (Table 1). As a treatment option for cytokine storm, CytoSorb has been applied by clinicians in MIS-C, however the use of the device in the US is not FDA approved for the pediatric population, and thus the providers need to obtain authorization for compassionate use. 14 Therefore, caution is advised with the use of these systems.8,15 On the other hand, the presented clinical experiences suggest that hemoadsorption may be a promising rescue therapy in patients with refractory shock secondary to severe left ventricular dysfunction (LVD) in MIS-C, potentially avoiding the need for ECMO and/or other mechanical cardiocirculatory support, if it is started as early as possible. Sparing ECMO in critically ill children with severe myocardial dysfunction due MIS-C is a stimulating therapeutic opportunity considering morbidity and mortality ECMO-related in these patients.1,5,16,17 Indeed blood purification is for technical reasons less invasive and allow the use of regional anticoagulation with citrate. On the other hand, these preliminary experiences should be confirmed with more evidences.
Furthermore, CytoSorb does not appear to interfere with the most common immunomodulatory therapies used currently in MIS-C.
Conclusions
MIS-C is a complex clinical syndrome that can induce severe myocardial dysfunction secondary to massive cytokine release. Evidence shows that mortality is significant and that there is a need for ECMO or other mechanical cardiocirculatory support. The potential beneficial role of an extracorporeal blood purification treatment based on hemoperfusion and CRRT is suggested by our report and by previous experience described in 2021. From this point of view hemoperfusion could be considered a therapeutic opportunity in this clinical setting, but further evidence is needed to confirm these clinical experiences.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Gabriella Bottari received honoraria as a speaker for CytoSorbents.
Ricard Ferrer Roca received honoraria as a speaker for CytoSorbents.
Juan Carlos Ruiz-Rodriguez received fees for the Advisory Board Palex.
Ethical statement
Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin. Written informed consent was obtained from the minor(s)’ legal guardian/next of kin for the publication of any potentially identifiable images or data included in this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.