
Abstract
Viral infections are a common cause of acute myocarditis. However, vaccines including influenza and smallpox have also been rarely implicated. Recently, the coronavirus disease 2019 (COVID-19) vaccines have been associated with acute myocarditis. We describe a case of acute myocarditis in a 19-year-old male 2 days after the initial dose of the COVID-19 mRNA-1273 vaccine. He presented with chest pain radiating to his left arm and bilateral shoulders. COVID, influenza, coxsackie, respiratory syncytial virus polymerase chain reaction (PCR) tests were negative. Electrocardiogram revealed diffuse ST-segment elevation. Initial Troponin was 15.7 ng/mL. A coronary angiogram revealed patent coronary arteries and no wall motion abnormality. A transthoracic echocardiogram showed diffuse hypokinesis with an ejection fraction of 49%. Cardiac magnetic resonance scan was aborted after 2 attempts due to severe claustrophobia. His chest pain resolved following initiation of aspirin, tylenol, colchicine, lisinopril, and metoprolol.
Introduction
Acute myocarditis refers to an inflammatory injury to the myocardium without the presence of ischemia.1-6 Viral infections including influenza, respiratory syncytial virus (RSV), severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), and coxsackie are leading causes of acute myocarditis. 5 In addition, vaccine exposures (particularly influenza and smallpox) have also been rarely implicated in the development of acute myocarditis.3,5 Recently, the coronavirus disease 2019 (COVID-19) vaccine-associated-myocarditis has been documented as an adverse event in previously healthy young adult populations1-6; although at a much lower prevalence than viral myocarditis. 3 Symptoms typically occur 4 days after the second dose of the vaccine.2-6 Most cases have been mild and self-limiting with a hospital length of stay of approximately 2 to 3 days. 6 Here, we present a case of a previously healthy male who presented with acute myocarditis after the initial dose of the mRNA-1273 vaccine.
Case Presentation
A 19-year-old male with a history of childhood asthma presented to the emergency department with a 1-day history of chest pain. The pain was described as a severe pin-like sensation, radiating to the left arm and bilateral shoulders. Pain improved with laying down. He denied any prior similar episodes. He further denied any recent viral illnesses, fever, or cough. He further denied any gastric symptoms including nausea or vomiting. He appeared anxious but denied shortness of breath. He had no family or personal history of heart disease. He admitted to occasional marijuana use but denied alcohol, tobacco, or other illicit drug use. Of note, he reportedly received the first dose of the mRNA-1273 COVID vaccine 2 days prior to symptoms onset.
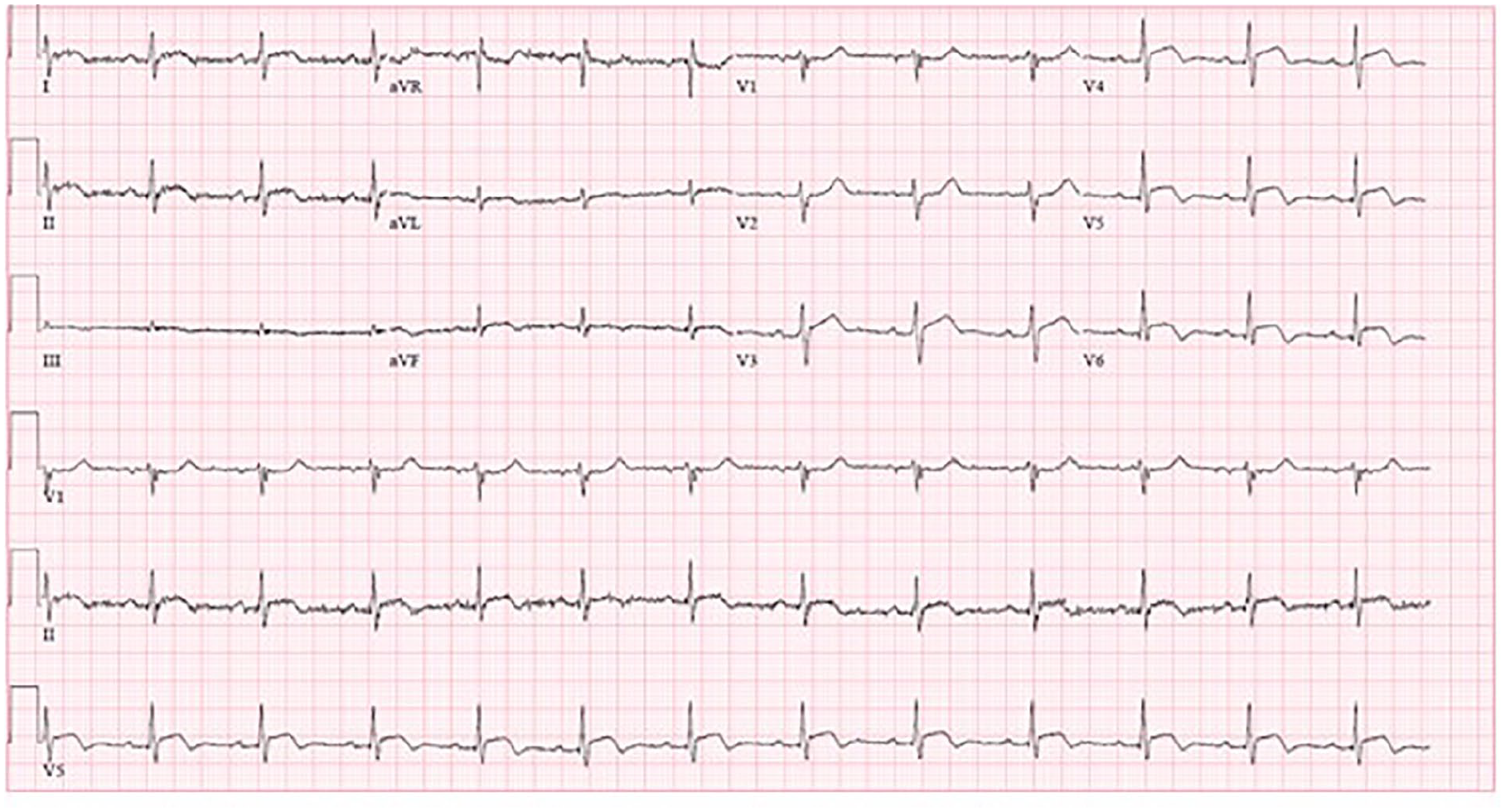
On arrival, vital signs were remarkable for sinus tachycardia of 105 beats per minute. Initial troponin was significantly elevated at 15.7 ng/mL and up trended to 24.8 ng/mL. Complete blood count and comprehensive metabolic panel were within normal limits. Urine drug screen was positive for marijuana. COVID, influenza, coxsackie, and RSV PCR tests were all negative. Chest X-ray was unremarkable, without evidence of pulmonary infiltrate, and normal cardiac border (Figure 1). Electrocardiogram (EKG) was significant for diffuse ST-segment elevation (Figure 2). Owing to concerns for ST-segment myocardial infarction, he emergently underwent cardiac catheterization. This however, revealed patent coronary arteries. The left heart ventriculography was unremarkable for Takotsubo cardiomyopathy (Figure 3). A transthoracic echocardiogram was obtained which showed mild diffuse hypokinesis and left ventricular ejection fraction of 49% (video in Supplementary File). At this time, we were concerned about acute myopericarditis; aspirin, tylenol, and colchicine were initiated. Repeat troponin on hospitalization Day 2 had downtrended to 17.2 ng/mL. Repeat EKG showed normal sinus rhythm, with interval decreased magnitude of ST-segment elevations (Figure 4). Low-dose lisinopril and metoprolol were initiated.

Chest X-ray showing clear lung fields and normal heart borders without evidence of cardiomegaly or acute disease.

Initial electrocardiogram with diffuse ST-segment elevation in limb and precordial leads.

Coronary catheterization revealing angiographically normal coronary arteries.
Electrocardiogram on hospital day 2 showing interval decrease in ST-segment elevation.
Two attempts were made to obtain a cardiac magnetic resonance imaging scan to confirm the diagnosis and characterize the extent of acute myopericarditis. However, these were unsuccessful due to significant claustrophobia, despite multiple doses of Benadryl, Ativan, and intravenous metoprolol. The patient was discharged home on hospital day 2, with instructions to continue a 1-month course of colchicine, a slow taper of aspirin, as well as lisinopril and metoprolol.
Discussion
This patient’s presentation of chest pain without shortness of breath, in the setting of a negative COVID-19, influenza, coxsackie, and RSV PCR tests, along with a significantly elevated troponin, ST-segment elevation in the inferior, lateral leads, diffuse wall hypokinesis with EF of 49% on echocardiogram, the absence of significant coronary artery disease, and Takotsubo cardiomyopathy on LHC and ventriculography, respectively, following the first dose of the mRNA-1273 vaccine makes his presentation a probable case of vaccine-associated myocarditis according to the center for disease control (CDC). 1 Cardiac magnetic resonance imaging (MRI) to evaluate for signs of myocarditis could not be completed due to persistent claustrophobia despite multiple anxiolytics.
A significant number of COVID-19 vaccine-associated myocarditis cases have been described in the young adult population between ages 16 to 30, most of whom had no significant morbidities.2-6 Male patients have been predominantly affected, mostly after receiving the second dose of the mRNA vaccine,2-6 with a reported incidence of 5.8 cases per million after second doses compared to 0.8 per million after the first dose. 6 Therefore, our patient represents one of the very few cases of myocarditis after the first vaccine dose.
Although acute myocarditis was reported as a rare adverse effect of the smallpox and influenza vaccines, 7 it was not reported as an adverse event in both mRNA vaccine clinical trials.8,9 Only 0.1% of the trial vaccine group had an adverse cardiac event of any kind which was reportedly not higher than the placebo group. 5 This could be due to the very few numbers of trial participants (20 000 for each) compared to the vast millions of fully vaccinated individuals since the emergency use authorization of both vaccines.
It is postulated that mRNA COVID-19 vaccine-associated myocarditis is likely due to a hypersensitivity reaction. 5 This is thought to be because most cases have been reported following the second dose of the vaccine. 5 However, our patient’s presentation after just the first dose seems to be an exception to this theory. Although he denied a history of symptomatic COVID-19 infection, a previous asymptomatic COVID-19 exposure and/or asthma allergen could have sensitized his immune system to his myopericardium via the mechanism molecular mimicry.
Owing to his mild symptoms and a quick improvement with colchicine and aspirin, an endomyocardial biopsy was deferred. Colchicine and aspirin were administered due to concerns for pericardial involvement. While the use of nonsteroidal anti-inflammatory drugs (NSAIDs) in myocarditis remains controversial, our decision to add aspirin was guided by the absence of adequate in-human studies that recommend against NSAIDs use and case reports that demonstrated improvement symptoms with the use of NSAIDs.10,11
Other differential diagnoses that were considered include coronary vasospasm, sarcoidosis, giant cell myocarditis, and autoimmune causes such as systemic lupus erythematosus and Takayasu arteritis. However, his presentation was not typical for any of these. In addition, he did not have any physical exam and echocardiographic findings of autoimmune diseases; and his symptoms resolve without the use of immunosuppressive medications.12-14 Furthermore, in coronary vasospasm, chest pain usually occurs at rest, the ST changes on ECG are transient and normalize with the resolution of chest pain. 15
Conclusion
We present a probable case of acute myocarditis 2 days after the first dose of the mRNA-1273 COVID-19 vaccine. It is important to be aware of this exceedingly rare adverse effect due to the increase in the COVID-19 vaccinations rate globally and symptoms resolution with supportive care in many reported cases. Notably, there is no substantial evidence proving a direct causal effect between COVID-19 vaccination and acute myocarditis. Therefore, the very rare temporary association of vaccination with myocarditis should not preclude vaccination as the benefits exceedingly outweigh the risks.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.