
Abstract
Background
Adequate fruit and vegetable (F&V) intake is important for health, yet populations globally are failing to meet recommendations.
Objective
A scoping review to summarize available evidence of evaluations of interventions to increase F&V intake globally, focusing on target populations, intervention strategies, research methods, and summarizing their evaluated impacts.
Methods
We searched PubMed and Web of Science in February 2023 for intervention studies in which dietary intake of fruit and/or vegetables were documented. Eligible studies included all age groups, excluding those targeting populations with specific disease-related conditions, such as cancer patients/survivors. Only articles published in English since 2012 were included in the review.
Results
We identified 6338 articles, with 226 meeting inclusion criteria, comprising 223 unique studies and 284 intervention comparisons. Most comparisons occurred in high-income countries (n = 192) compared to low- and middle-income countries (n = 92). Randomized controlled trials (RCTs; 37.3%) and cluster RCTs (52.5%) were predominant. Interventions primarily targeted adults (31.7%), school-aged children (18.0%), children under-five (14.4%), and adolescents (13.7%), lasting an average of 24 weeks (range: 2 weeks to 20 years). Food-frequency questionnaires (59.2%) and 24-h recalls (26.8%) were the most used dietary assessment method. Health and nutrition communication (75.9%) was the most common intervention, utilizing interpersonal communication, mass media, and information-communication technology, often in combinations. Positive impacts on fruit (43.9%), vegetable (40.2%), and combined F&V intake (53.0%) were observed in nearly half the intervention comparisons.
Conclusions
These findings highlight the predominance of health and nutrition communication interventions, predominantly in high-income countries, showing mixed success in improving F&V intake, emphasizing the need for context-specific strategies and standardized methodologies to design sustainable, cost-effective interventions for better diet quality and health outcomes.
Plain language title
A literature review assessing what we know and do not know about efforts to improve fruit and vegetable intake across the world.
Plain language summary
Eating enough fruit and vegetables is important to stay healthy, but most people do not eat enough diverse fruits and vegetables. Various strategies have been tried to increase fruit and vegetable intake; however, what worked, for whom, and in which context is not well understood. In this paper, we summarize the intervention strategies that have been implemented and their impact across different countries and age groups. Of the 226 published articles comprising 284 intervention comparisons included in this review, most intervention comparisons were from high-income countries (67.6%). Most intervention comparisons in which dietary intake of fruit and/or vegetables was documented focused on adults (31.7%), followed by school-aged children (5-9.9 years of age; 18.0%) and children under 5 years of age (14.4%). The interventions lasted an average of 24 weeks. Health and nutrition communication was the most commonly used component to encourage study participants to eat more fruit and vegetables. Different approaches were used, like talking to people in group settings and using mass media or technology. About one-half of studies found a positive impact on fruit intake, vegetable intake, and/or the intake of total fruit and vegetables. Few interventions have been implemented in low- and middle-income countries. The findings highlight the dominance of health and nutrition communication interventions, mainly in high-income countries, with mixed success in improving fruit and vegetable intake. Tailored, context-specific strategies are needed to enhance the intake of fruit and vegetables worldwide. Additionally, harmonizing study designs and methods is crucial for accurately evaluating intervention impact and strategies used. More research is needed to better understand how to improve fruit and vegetable intake in low- and middle-income countries and across different age groups.
Keywords
Introduction
Inadequate intake of fruit and vegetables (F&V) affects the health of populations globally.1,2 Despite the well-established health benefits of consuming sufficient F&V, many populations fail to meet the World Health Organization (WHO) recommendation of 5 servings (400 g) of F&V per day.3,4 The mean daily intake of F&V in low- and middle-income countries (LMICs) is 2.1 servings per day (1.8–2.4) compared to 5.4 servings per day (5.1–5.7) in high-income countries (HICs). 5 Generally, less than one-fifth of individuals aged 15 years and older in LMICs meet the WHO F&V recommendations. 6
Multiple factors influence the demand and consumption of F&V, including key factors such as availability (supply), accessibility, affordability, and desirability (individual preferences, perceptions, and food preparation). Additionally, food choices shaped by social context, cultural norms, and the broader food environment play a significant role in determining intake.7–10 Promoting increased F&V intake has the potential to significantly improve health outcomes and reduce the burden of chronic diseases, but it requires targeted action. 11 Interventions aimed at improving F&V intake include educational and promotional campaigns to address knowledge constraints and increase desirability, social protection (eg, subsidies for F&V, cash-based transfers) to address affordability constraints, improvements in supply chains to increase availability and access to fresh produce, school-based programs (eg, school gardens, school meals, and nutrition education), gender and women's empowerment to support self-efficacy, market integration and national health policies that encourage F&V intake through multiple channels. Each of these interventions may have a different impact depending on the duration, frequency, intensity, and content delivered, besides the potential influence of the context in which they are implemented.
Recent systematic and umbrella reviews have summarized strategies for improving F&V intake among various populations.8,12,13 A consistent finding is that most current research on consumer motivations, individual behavior and social norms regarding diets derives from HICs. A review by Savoie-Roskos et al 13 found that gardening interventions in HICs had a small but positive impact on children's F&V intake despite limitations such as small, convenient samples and short duration of interventions. Wolfenden et al 12 also found that intervention strategies within schools, childcare services, homes, workplaces, primary care, eHealth strategies, mass media campaigns, household food production strategies, and fiscal interventions can be effective. However, evidence was scarce on the impact of strategies targeting agricultural production practices, supply chains, and the broader food system. 12 A review by Lachat et al 14 in 2013, which analyzed national policies and national actions in LMICs, found that policy actions aiming to increase F&V intake described the need for production, storage and processing of local F&V along with nutrition education on the health benefits of F&V.
This scoping review was conducted as part of the Fruit and Vegetables for Sustainable Healthy Diets (FRESH) Initiative. FRESH is a multi-disciplinary and multi-partner research programme that is designing and testing end-to-end approaches including supply-side, demand-generation, and food environment interventions. The overall goal is to increase F&V intake and, in turn, improve diet quality, nutrition and health outcomes. 15 To understand the existing evidence of what works to increase F&V intake, the objective of this scoping review was to summarize the available evidence on intervention strategies and their impact on the intake of F&V in low-, middle-, and high-income countries. While previous reviews have often focused on specific population groups or regions, this review encompasses various age groups and countries, including HICs and LMICs. This broader scope offers a global perspective on the impact of intervention strategies on F&V intake and highlights critical areas for future research. The subsequent paper in this supplement will dive into the details to better understand the results of these trials by key intervention components and strategic approaches. 16 The overarching goal is to offer insights to inform stakeholders in their efforts to promote nutritious and healthy diets worldwide.
Methods
This scoping review was conducted using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Extension for Scoping Reviews (PRISMA-ScR) guidelines. 17 Our protocol has been published online, 18 and the PRISMA-ScR checklist that supports our approach is available in Supplemental Table 1.
Inclusion Criteria
Study Design
In this scoping review, the term “intervention comparisons” refers to any trial arm assessed against a valid and defined control group or a non-intervention group. These counterfactual groups were considered to allow isolation of the effect of an intervention or package of interventions on F&V intake. Therefore, the following types of intervention studies were considered: randomized controlled trials (RCTs), cluster-randomized controlled trials, controlled before–after studies, and feasibility and pilot studies. Solely qualitative studies, interrupted time series (without control), systematic reviews and meta-analyses were excluded. Articles not meeting the inclusion criteria described in this section were removed, and reasons for exclusion were documented. Conference reports, abstracts, opinions, editorials, commentaries, preprints, and other non-peer-reviewed articles were not included. Only articles published in English were eligible.
Populations of Interest
Studies among all population groups were considered eligible without imposing restrictions based on age, sex, gender, location, or country. However, we excluded studies that only targeted populations with pre-existing medical and health conditions (eg, cardiovascular disease, obesity, mental impairments, cancer patients or survivors, or diabetics). We also excluded studies focusing on specialized diets used in treating or managing diseases or meeting the dietary requirements of athletes. A minimum sample size of 50 in at least 1 of the intervention comparison groups was required for study inclusion.
Age groups were broadly based on WHO's World Standard Population categories. 19 The groups included in this review were children aged 6 months to 5 years (referred to as children under 5), school-aged children (5-9.9 years), adolescents (10-19.9 years), adults (20-59.9 years), and older adults (60 + years). When a study-defined age group did not align exactly with these cut-offs, we used the mean or median age to categorize the population. If neither the mean nor median was provided, we classified the population based on the closest corresponding age group reported in the study. Additionally, pregnant and/or lactating women, as well as caregiver–child dyads and family/ household units, were also considered as distinct and relevant target groups.
Intervention Settings
Interventions from any settings globally were considered, including schools, households, communities, workplaces, and healthcare or clinical settings.
Outcome Measures
The outcomes considered included the intake of fruit, vegetables, total or combined F&V, specific F&V groups, or individual types of fruit and/or vegetables. Studies focusing solely on aspects such as F&V preferences, knowledge or attitudes, F&V purchases, or those limited to the consumption of F&V juices alone were excluded.
Dietary Assessment
We considered studies reporting on F&V intake in grams, portions, or servings, in terms of variety and diversity, and through frequency and percentage of intake. The included studies assessed these outcomes through various methods, such as food frequency questionnaires (FFQ), 24-h recalls (24HR), food diaries, and food records, through approaches such as photographs, food plate waste, and digital apps. Given the various types of FFQ and 24HR tools available, we categorized these into 2 types—quantitative and non-quantitative—regardless of the description provided by the authors. Quantitative FFQs involve not only tracking the frequency of food intake but also estimating the portion or serving sizes.20–22 Conversely, non-quantitative FFQs solely record the frequency of intake within a specified timeframe.20–22 Similarly, quantitative 24HR captures a detailed recall of all foods consumed in the previous 24 h, including the amount of each item,20,23,24 whereas non-quantitative 24HR tracks whether or not particular food items were consumed the previous day without detailing the amounts. 25
Intervention Strategy
A minimum intervention duration of ≥2 weeks was required for inclusion. Interventions that focused on F&V specifically and those targeting the broader health and food environment were included if the studies measured fruit and/or vegetable intake. As such, we organized included intervention types into 3 broad categories: (1) F&V specific, defined as those interventions designed with specific messaging or activities on F&V; (2) other diet interventions designed to increase food security and/ or dietary diversity without specific descriptions of F&V messaging, and (3) lifestyle, where interventions were designed for promotion of healthy lifestyles with activities that may have included physical activity, smoking cessation, and nutrition information. Within these interventions, multiple design and implementation strategies may have been applied. In this review, intervention strategy refers to the combination of intervention component and intervention approach, where the intervention component is defined as the specific elements of the intervention that are expected to drive change, and the intervention approach describes the method used to implement or deliver the intervention component. Briefly, intervention components identified in this scoping review were categorized as health/nutrition communication, social protection, nutrition-sensitive agriculture, and environmental restructuring, while intervention approaches were categorized as interpersonal communication (IPC), group-based approaches, mass communication, information and communication technology (ICT), community/social mobilization, and economic incentives/ in-kind transfers, as described in more detail in Supplemental Table 2.
Search Strategy
Comprehensive searches were conducted electronically in 2 online scientific databases: PubMed and Web of Science. The search strategy used a combination of keywords and MeSH terms related to F&V intake outcomes, interventions, and study designs (Supplemental Tables 3 and 4). The search was limited to studies published since 2012. The literature search was completed on February 13, 2023, using PubMed, and on February 17, 2023, using Web of Science.
Article Selection
The articles identified from the research databases were imported into Covidence (Veritas Health Innovation, Melbourne, Australia). Titles and abstracts were screened by 2 independent reviewers for assessment against the inclusion criteria. When necessary, a full-text review was performed to confirm eligibility for the present review. Any disagreements were resolved by a third reviewer.
Data Extraction, Summary, and Synthesis
Data from the eligible studies were extracted by a team of reviewers using a standardized Excel sheet. The data extraction form was piloted on a subset of included studies and underwent several iterations. Descriptive statistics (frequencies) were used to summarize key characteristics of the interventions identified from the included studies. The intervention characteristics reported encompass the country, target population group, study design, intervention details, type of comparison group, dietary assessment methods, and F&V outcomes. Significant impacts on F&V outcomes, as reported by the authors of the primary study, were summarized in overview tables distinguishing between fruit-only, vegetable-only, and combined F&V outcomes. We also described the intervention components and intervention approaches used in each intervention by population group to highlight the most common strategies used. The impact on fruit and vegetable outcomes was also summarized by categorizing intervention duration into 4 groups (<3 months, ≥ 3 to < 6 months, ≥ 6 to < 12 months, and ≥ 12 months) and intervention group sample sizes into 3 groups (<100, ≥ 100 to < 500, and ≥ 500). The cut-off points for these categorizations were selected arbitrarily based on the number of intervention comparisons in the respective categories of intervention durations and sample sizes. A cut-off based solely on intervention duration may be inherently arbitrary and risk excluding valuable insights from shorter yet impactful studies. In addition to duration, factors such as intervention intensity and design significantly influence outcomes.26,27 Shorter-duration interventions, particularly those employing high-intensity or innovative approaches, can yield meaningful evidence and measurable impacts. 28
Results
Search Results and Number of Articles Included
Our search identified 6338 articles from PubMed (n = 3738) and Web of Science (n = 2600). After removing 1292 duplicates, 5046 unique articles remained for screening (Figure 1). At the title and abstract screening stage, 4732 articles were excluded, leaving 314 for full-text review. A total of 226 articles met our inclusion criteria. These 226 articles reported on 223 unique studies, which included a total of 284 intervention comparisons, each consisting of 1 intervention group compared to the respective comparison, control or non-intervention group. An overview of the articles included, respective citations, and a brief description of the study design, intervention component, intervention approach, and outcome(s) assessed are provided in Supplemental Table 5.
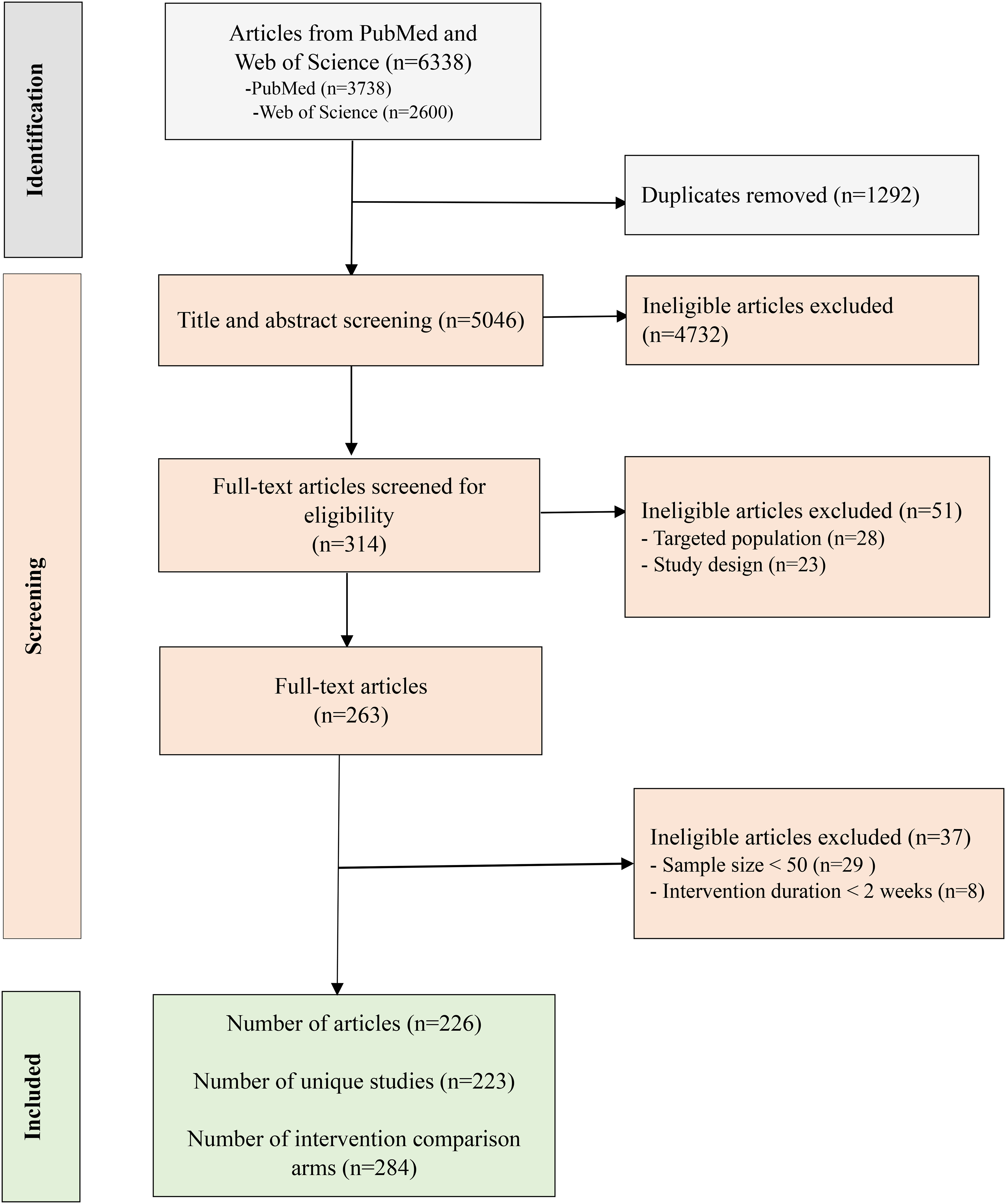
PRISMA flowchart of the screening process.
Geographical Distribution of the Intervention Comparisons
Most articles reported on studies implemented in HICs (n = 152/226 compared to LMICs (n = 74/226), which resulted in 192/284 (67.6%) intervention comparisons in HIC and 92/284 (32.4%) in LMICs. North America, particularly the United States (n = 72/284), had the highest number of intervention comparisons reporting on F&V intake (Figure 2). In Europe, Western countries dominated, with the Netherlands (n = 17/284), the United Kingdom (n = 16/284), and Spain (n = 12/284) contributing the most out of a total of 91/284 conducted in the region. Australia (n = 24/284) also contributed substantially to the literature. In Asia, Nepal and India led with 11 and 10 (out of 284) intervention comparisons, respectively, followed by China (n = 9/284) and Bangladesh (n = 4/284). South America had fewer intervention comparisons (n = 11/284), with most of them in Brazil (n = 9/284). A limited number of intervention comparisons were implemented in sub-Saharan Africa, with more in East Africa (n = 19/284) compared to West Africa (n = 7/284). In Southern Africa, only 2 eligible intervention comparisons were identified, both conducted in South Africa. Only 5 intervention comparisons were identified in North Africa and the Middle East, with none reported from the Caribbean. The number of interventions recorded for each country is provided in Supplemental Table 6.
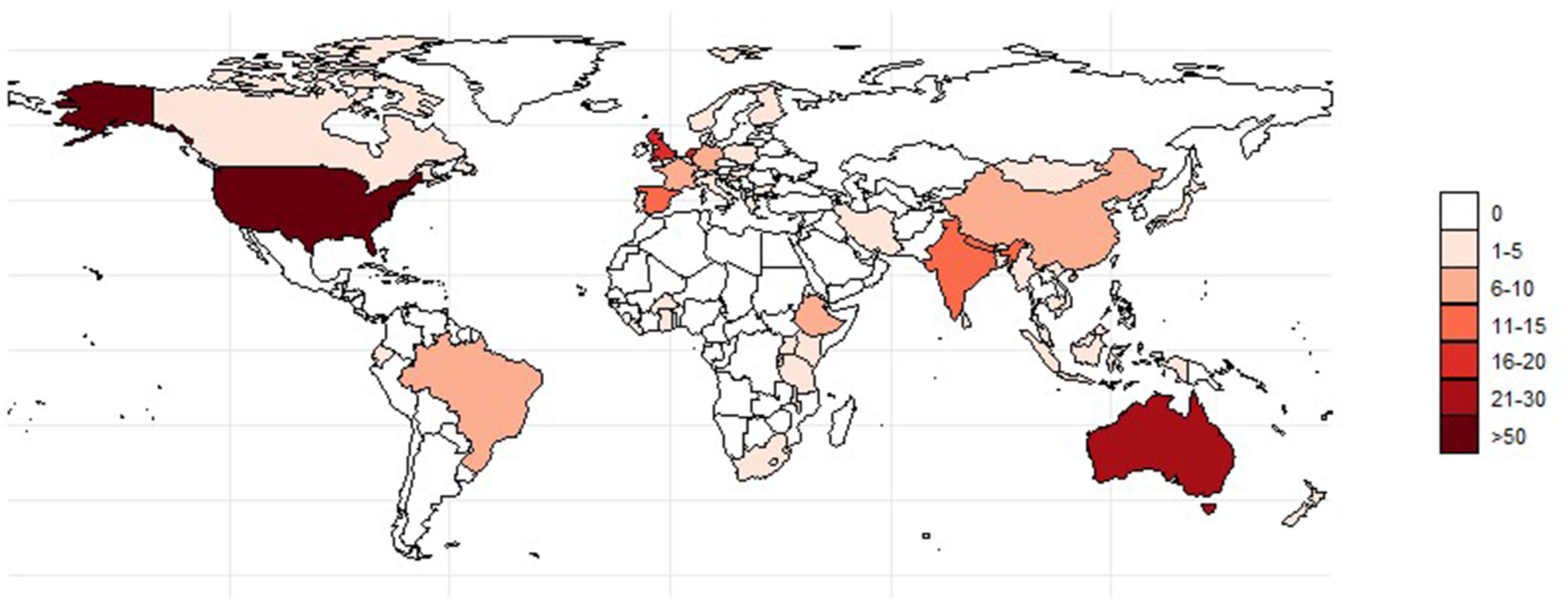
Global distribution of intervention comparisons aiming to improve fruit and vegetable intake.
Population Groups and Sample Size of Intervention Comparisons
The largest proportion (31.7%) of intervention comparisons targeted adults (Table 1). While 18% of intervention comparisons focused on 5–9.9-year-old school-aged children; about 14% of interventions targeted children under 5 years old and adolescents (10–19.9 years), respectively. About 10% of interventions involved caregiver–child dyads, with 5% or fewer targeting older people, pregnant and/or lactating women, or family/household units. Notably, 26.4% of intervention comparisons included populations consisting of more than 75% females. However, only 14.8% of interventions specifically targeted female participants, and 0.7% focused exclusively on males. The sample sizes ranged from 40 to 41012 participants for the intervention arms and 36 to 68120 for the comparison arms (Table 2). The median (IQR) sample size was 234 (127, 639) for the intervention arms and 228 (118, 603) for the comparison arms. Approximately half of the intervention groups included sample sizes between 100 and 500 individuals, while 29.2% enrolled ≥ 500 study participants. In contrast, 18.7% of the comparison groups had sample sizes with fewer than 100 participants.
Target Population, Participant Sex, and Study Setting of Intervention Comparisons (n = 284)a.
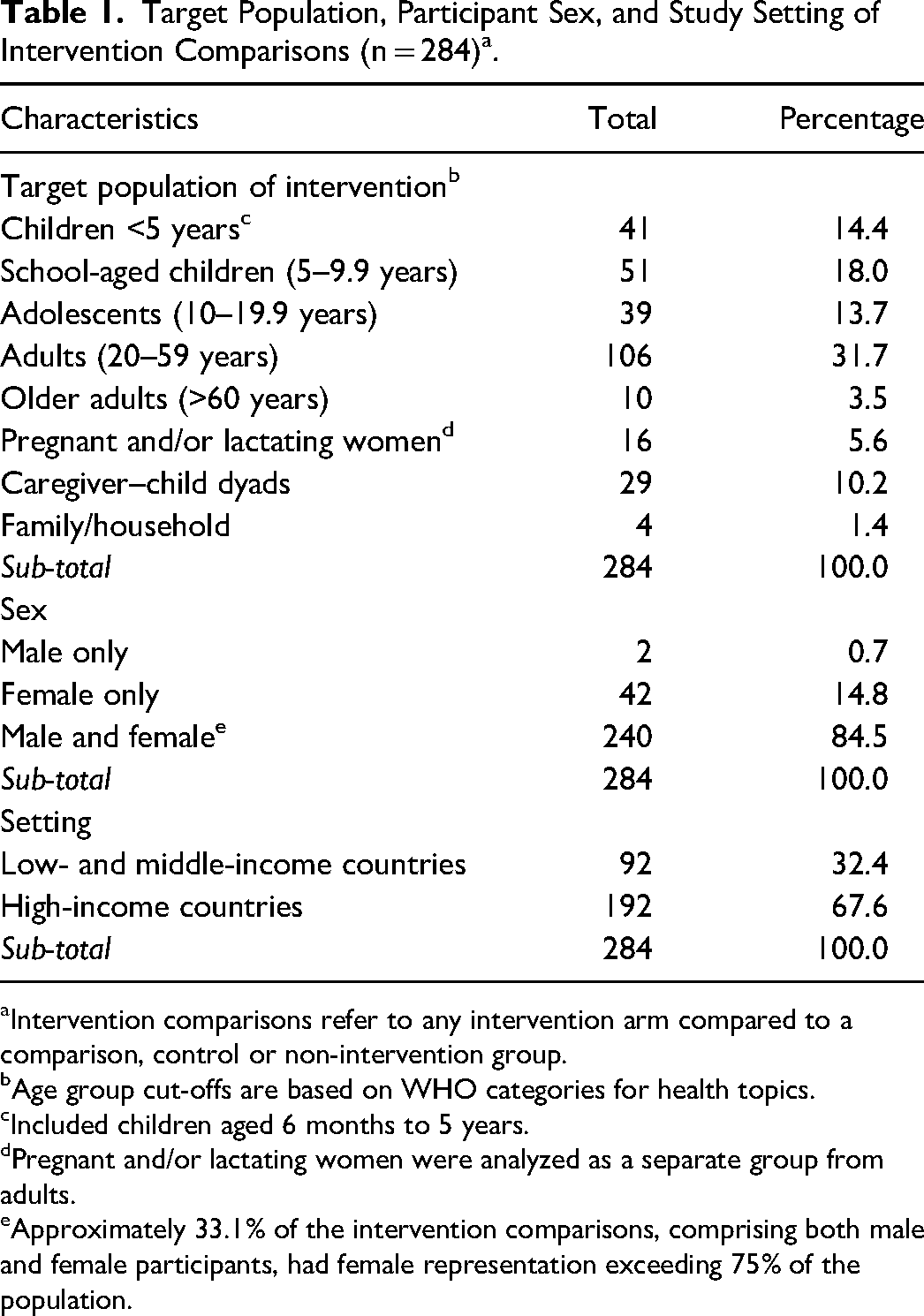
aIntervention comparisons refer to any intervention arm compared to a comparison, control or non-intervention group.
bAge group cut-offs are based on WHO categories for health topics.
cIncluded children aged 6 months to 5 years.
dPregnant and/or lactating women were analyzed as a separate group from adults.
eApproximately 33.1% of the intervention comparisons, comprising both male and female participants, had female representation exceeding 75% of the population.
Study Design, Duration, Sample Size, Assessment Time Points and Type of Comparison Group for Intervention Comparisons (n = 284)a.
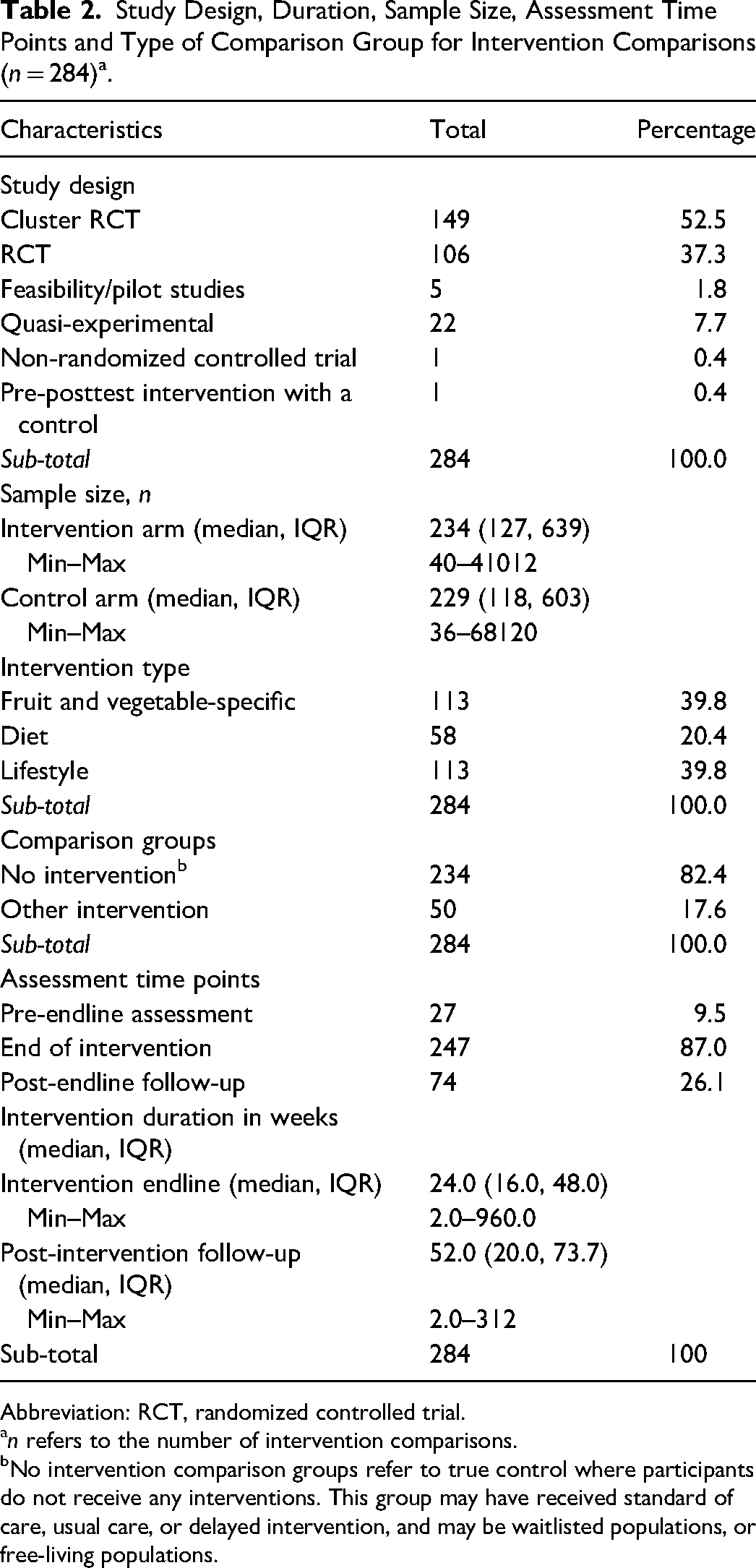
Abbreviation: RCT, randomized controlled trial.
an refers to the number of intervention comparisons.
bNo intervention comparison groups refer to true control where participants do not receive any interventions. This group may have received standard of care, usual care, or delayed intervention, and may be waitlisted populations, or free-living populations.
Overview of Intervention Characteristics
Of the 284 intervention comparisons included, most were either from cluster RCTs (52.5%) or RCTs (37.3%), respectively (Table 2). Approximately 40% of the intervention comparisons employed a fruit- and/or vegetable-specific intervention, an additional 40% utilized diet-related interventions, and 20% used lifestyle-focused interventions. The majority of intervention comparisons (82.4%) employed a free-living comparison arm in which either no intervention or a standard of care/practice was provided. Approximately one-fifth (17.6%) of the comparison groups received an alternative intervention.
Most intervention comparisons (87.0%) evaluated outcomes at the end of the intervention, but about a quarter (26.1%) also assessed outcomes at a post-intervention follow-up. A small percentage (9.5%) also reported on pre-endline assessment of the outcomes. The median (IQR) duration of interventions was 24.0 (16.0, 48.0) weeks. The shortest eligible intervention lasted approximately 2 weeks, and the longest extended up to 20 years. Post-intervention follow-up periods also showed a broad range, with a median (IQR) of 52.0 (20.0, 73.7) weeks. Of the intervention comparisons, 19.4% had a duration of less than 3 months, 13.0% spanned 3–6 months, 30.6% lasted 6–12 months, and 37.0% extended beyond 12 months.
Dietary Assessment Methods
FFQ was the most frequently used dietary assessment method (59.2%; Table 3). Of the FFQ, almost two-thirds were quantitative (63.7%), while 36.3% were non-quantitative assessing only the frequency of intake. The second most frequently used assessment method was 24HR (26.8%), of which more than half were quantitative (57.9%) and 42.1% were non-quantitative. Food records (10.6%) and food diaries (2.5%) were less common.
Overview of Dietary Assessment Methods Used in the Included Intervention Comparisons (n = 284).
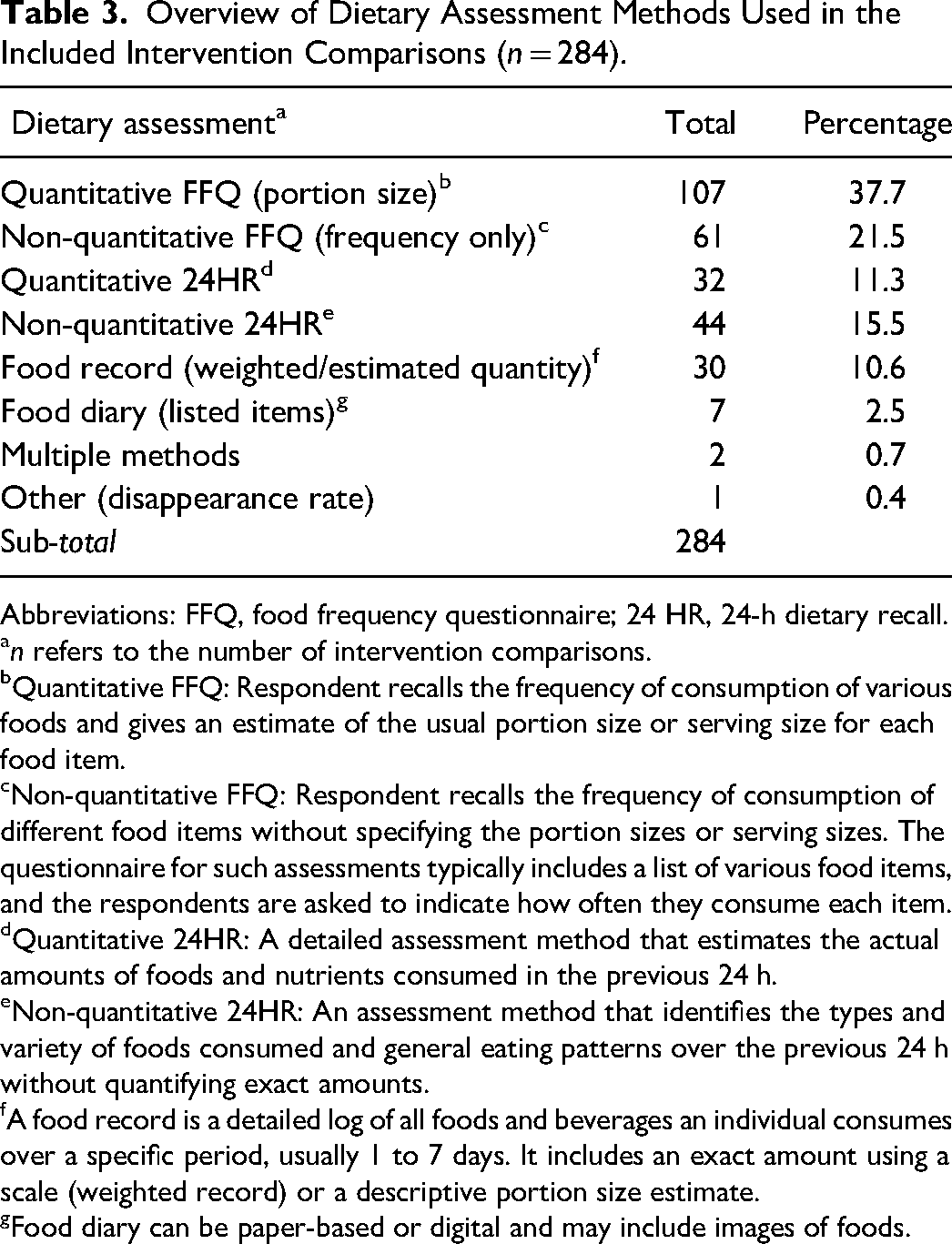
Abbreviations: FFQ, food frequency questionnaire; 24 HR, 24-h dietary recall.
n refers to the number of intervention comparisons.
Quantitative FFQ: Respondent recalls the frequency of consumption of various foods and gives an estimate of the usual portion size or serving size for each food item.
Non-quantitative FFQ: Respondent recalls the frequency of consumption of different food items without specifying the portion sizes or serving sizes. The questionnaire for such assessments typically includes a list of various food items, and the respondents are asked to indicate how often they consume each item.
Quantitative 24HR: A detailed assessment method that estimates the actual amounts of foods and nutrients consumed in the previous 24 h.
Non-quantitative 24HR: An assessment method that identifies the types and variety of foods consumed and general eating patterns over the previous 24 h without quantifying exact amounts.
A food record is a detailed log of all foods and beverages an individual consumes over a specific period, usually 1 to 7 days. It includes an exact amount using a scale (weighted record) or a descriptive portion size estimate.
Food diary can be paper-based or digital and may include images of foods.
Intervention Components
Health and nutrition communication emerged as the most prevalent intervention component used in 75.9% of the intervention comparisons reporting on F&V intake (Table 4). This intervention component was most implemented among adults (n = 87/240) and least commonly used among older people (n = 10/240) and households (n = 1/240). In contrast, social protection (4.7%), environmental restructuring (1.2%), and nutrition-sensitive agriculture (1.2%) interventions were the least common intervention components included in the present review. Some intervention strategies included 2 intervention components (15.5%), while 1.6% were more complex, involving 3 or more components.
Distribution of Intervention Components and Intervention Approaches Used in Studies Documenting Fruit and Vegetable Intake Across Different Population Groups.
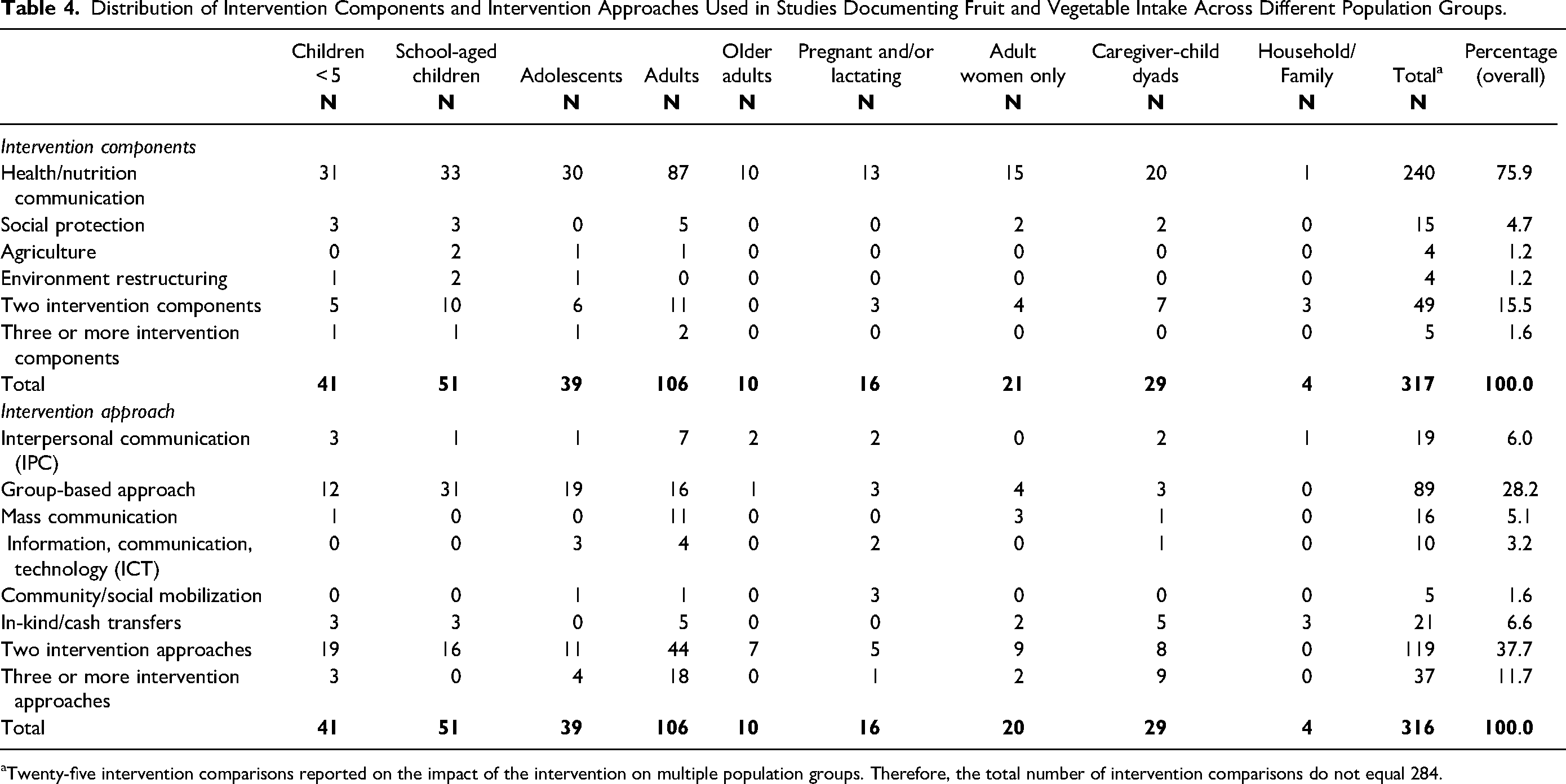
Twenty-five intervention comparisons reported on the impact of the intervention on multiple population groups. Therefore, the total number of intervention comparisons do not equal 284.
Intervention Approaches
A diverse range of intervention approaches were used (Table 4). Approximately 37.7% of intervention comparisons employed a combination of 2 approaches, frequently integrating IPC with ICT or combining group-based communication with IPC or ICT. This multi-approach strategy was particularly common in interventions targeting adults (n = 44/118). Group-based communication alone was also frequently used (28.2%), most commonly in interventions focused on school-aged children (n = 31/89), adolescents (n = 19/89), and adults (n = 16/89). Interventions that utilized 3 or more approaches represented 11.7%, predominantly those targeting adults (n = 18/37). In-kind or cash transfers (n = 21/316), mass communication (16/318), ICT (15/318), and community/social mobilization (n = 5/316) were the least employed approaches; when used, they were primarily implemented in interventions aimed at pregnant and/or lactating women, caregiver–child dyads and households/families.
Outcomes Assessed
Out of 284 intervention comparisons, the most frequently reported outcomes were vegetable intake (63.0%) and fruit intake (60.2%; Table 5). Combined F&V intake was reported in 47.2% of intervention comparisons. About 12.7% of the intervention comparisons presented all 3 outcomes, ie, fruit, vegetables, and combined F&V intake.
Number of Intervention Comparisons Reporting on Fruit and Vegetable (F&V) Outcomes Assessed and the Impact of Intervention Comparisons on F&V Intake.
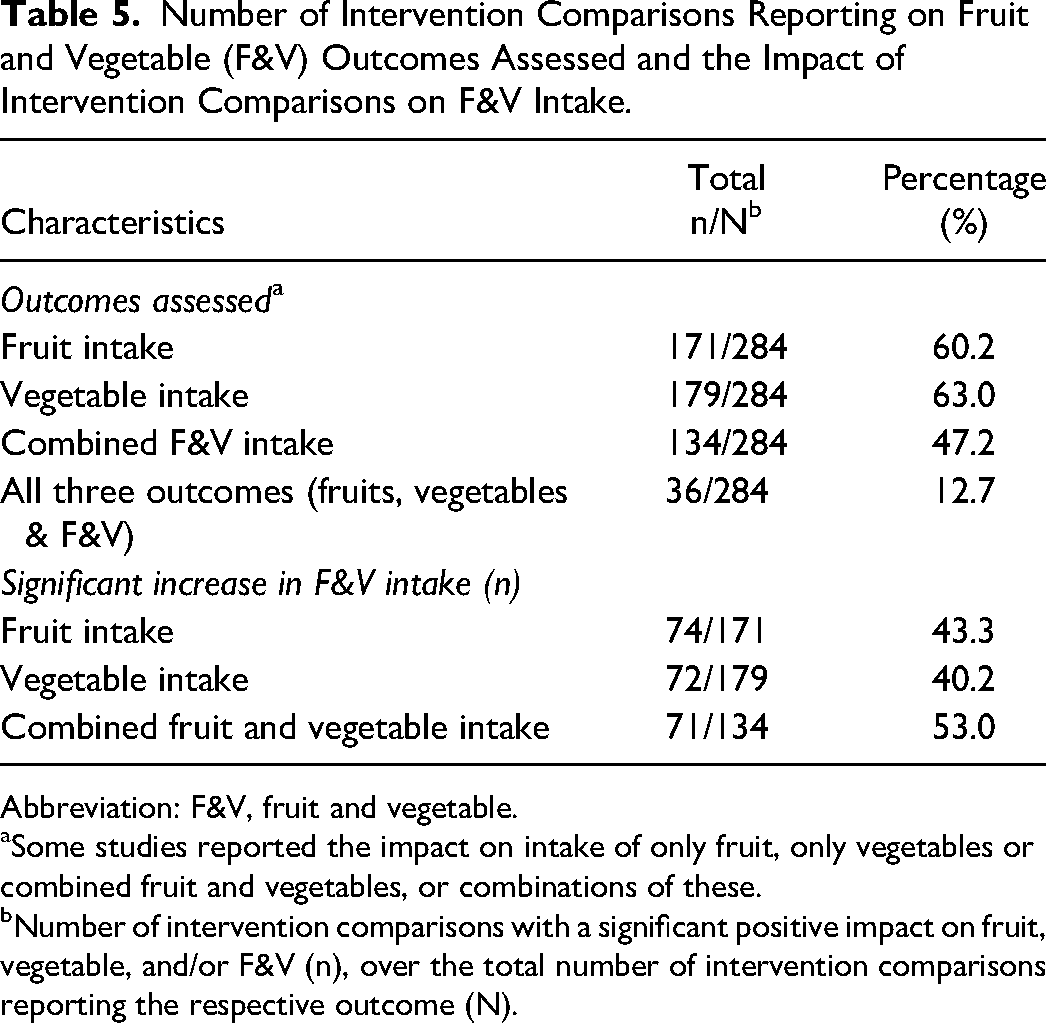
Abbreviation: F&V, fruit and vegetable.
Some studies reported the impact on intake of only fruit, only vegetables or combined fruit and vegetables, or combinations of these.
Number of intervention comparisons with a significant positive impact on fruit, vegetable, and/or F&V (n), over the total number of intervention comparisons reporting the respective outcome (N).
Effect of Intervention on Intake
Among intervention comparisons that assessed combined F&V intake, approximately one-half demonstrated a statistically significant positive impact (n = 71/134, 53.0%; Table 5). However, less than half of intervention comparisons reported a statistically significant positive impact when fruit and vegetable intake were analyzed separately. For vegetable intake, 72 out of 179 comparisons (40.2%) showed a positive impact, while 74 out of 171 comparisons (43.3%) found a positive impact on fruit intake. When exploring the impact of intervention strategies by duration categories (Figure 3), we found a decreasing trend in the proportion of intervention comparisons with a significant positive impact on F&V, ie a smaller proportion of intervention comparisons showed an impact on F&V intake in the higher duration categories. For fruit and vegetable intake specifically, the proportion of intervention comparisons demonstrating a positive impact declined between 3 and 6 months, increased for interventions lasting 6–12 months, and then declined again for those exceeding 12 months.
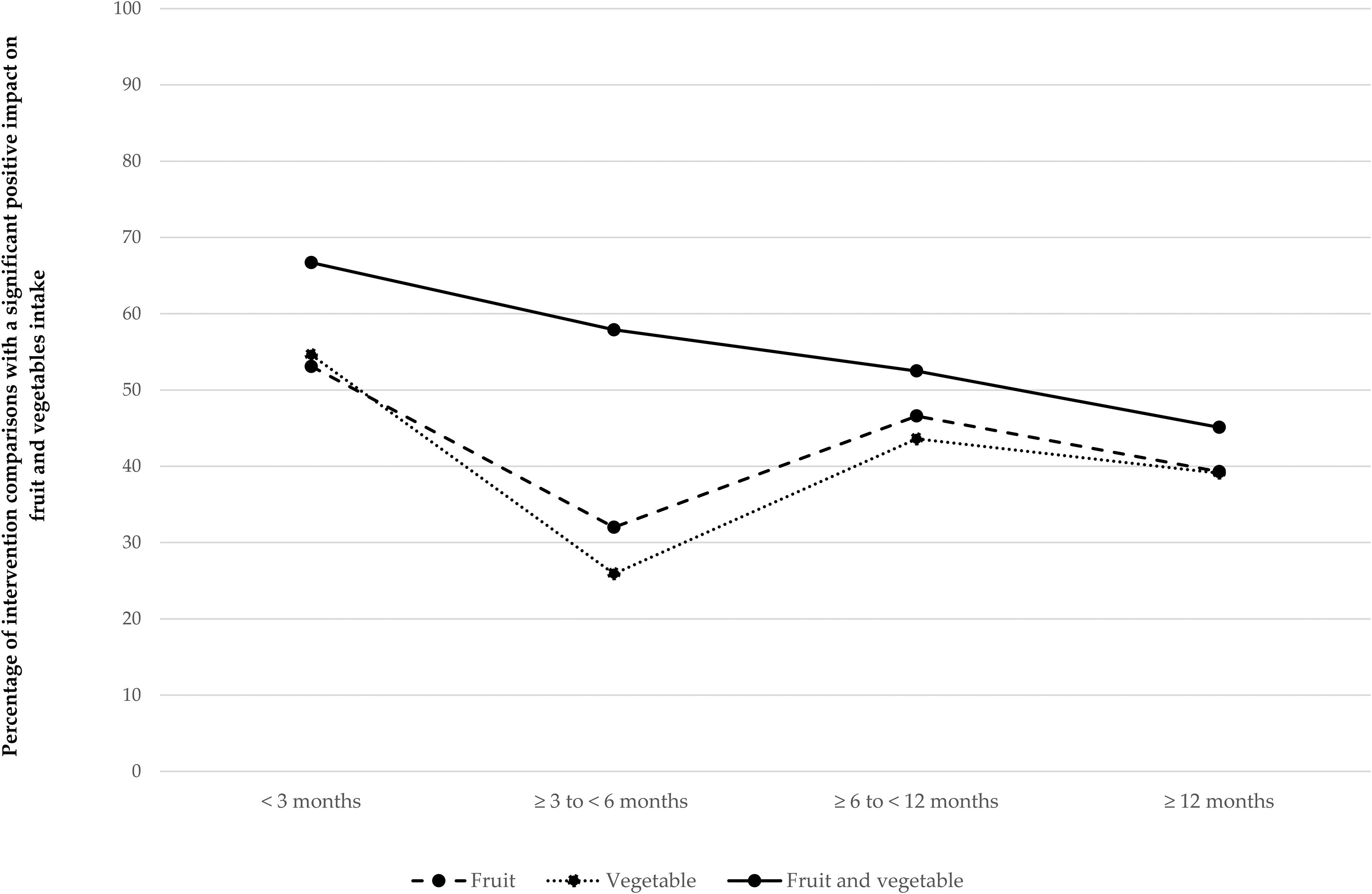
Percentage of intervention comparisons with a significant positive impact on fruit and vegetables intake.
Effect of Interventions by Dietary Assessment Method and Sample Size
Because dietary assessment methods have different strengths and weaknesses that may affect the findings, we also explored the results of the included studies by dietary assessment method (Table S7). However, no single dietary assessment stood out, and no clear pattern emerged.
No clear trend was observed on the impact of interventions on fruit, vegetable, and combined F&V intake by sample size categories (Table S8). In other words, intervention comparisons with larger sample sizes did not seem more likely to find a significant impact than smaller studies.
Discussion
This scoping review summarizes the available evidence on interventions and their impact on F&V intake in different population groups in low-, middle-, and high-income countries, regardless of whether F&V intake was the primary focus of the intervention. There is a significant gap in the geographical distribution of intervention studies that focus on F&V intake as an outcome; interventions implemented in HICs dominate the research landscape. This imbalance is consistent with a prior scoping review 29 and an analysis of F&V intake in LMICs. 30 This underscores a disparity in research efforts and resource allocation, indicating that LMICs may be underserved in intervention studies that could potentially provide insights into how best to improve diets and associated nutrition and health outcomes of people living in LMICs. The evidence gap in LMICs is partly due to limited investment in research and development from key stakeholders, including the public sector, academia, the private sector, and development partners.31,32 However, our review suggests countries such as Brazil, India, China, and Nepal have made notable investments in F&V intake research. The Global Burden of Disease Study 1 also highlighted that a disproportionate number of dietary intervention trials were implemented in HICs. Similarly, the Food and Agriculture Organization (FAO) also concluded that there is a scarcity of studies on the effectiveness of interventions to improve F&V intake in LMICs. 33 Addressing this disparity is vital for more inclusive and equitable food systems and global health strategies that adequately address the diverse dietary needs and challenges across population groups globally.
Within LMICs, the variation in the number of intervention studies across continents and countries points to differing levels of research activity in general and on F&V. A relatively higher number of interventions were implemented in Asia, particularly in India, Nepal, and China. Conversely, fewer intervention studies were implemented in sub-Saharan Africa and South America. Limited funding, infrastructure and research capacity, as well as logistical challenges, are well-known barriers to research efforts in LMICs, which, along with varying public health priorities, may contribute to the geographical disparities in dietary intervention research.31,32 A deep dive to better understand the causes of these disparities is important to overcome inequity.
In this scoping review, about one-third of intervention comparisons focused on adults aged 20–59. This focus likely reflects the critical role of diet in preventing and managing non-communicable, chronic diseases, which are a significant concern in this age group.34,35 However, this concentration on adults may overlook the long-term benefit of improved F&V intake among other population groups. Besides adults, school-aged children, children <5 years of age and adolescents were the next 3 most commonly targeted groups for the studies included in this review. This is of concern as early childhood is a critical period for physical and cognitive development and an opportunity for establishing lifelong healthy eating habits. 36 Similarly, the relatively low proportion of intervention studies aimed at adolescents is concerning, given that this is a formative period for developing independent dietary habits that can persist into adulthood.37–39 Moreover, the lack of focus on families/households suggests a potential area for future research and an entry point for dietary interventions. Since household dynamics often influence the dietary habits of all family members,40,41 family-based interventions could be particularly beneficial because household members may support each other and reinforce some of the knowledge gained through interventions. The focus on adults may also explain the limited impact observed in some studies, as behavior change in adulthood can be more challenging. Established habits and routines become deeply ingrained, making breaking old patterns and adopting new behaviors more difficult. 42
Sex distribution in the included studies also presents interesting findings. Almost one-third of the intervention studies enrolled more than 75% female participants. A systematic review and meta-analysis among young adults 43 indicated that females were more frequently targeted in dietary interventions. This may be because women are often responsible for meal preparation and food purchasing, making them key participants in interventions aimed at influencing dietary habits. The meta-analysis, as mentioned above, also demonstrated a significant increase in F&V intake in sex-specific interventions compared to sex-neutral interventions. 43 However, this finding was limited by the small number of sex-specific studies specifically addressing F&V intake.
The variability in sample sizes, ranging from 40 to over 41000 participants, underscores the diversity in study designs and the scale of intervention implemented. Although our inclusion criteria required a minimum sample size of 50 participants for intervention comparisons, some studies with multiple comparison arms included group(s) with fewer than 50 participants, explaining the observed range. Consistent with these observations, a systematic review by Savoie-Roskos et al 13 on F&V intake among children and adolescents aged 2–15 years in HICs highlighted that many studies are limited by small sample sizes. Consequently, it is possible that some of the included studies failed to detect a significant difference due to limited statistical power. However, contrary to our expectations, we did not find an obvious trend when comparing the impact of intervenion comparisons by sample size categories.
The decreasing trend in the proportion of intervention comparisons reporting positive impacts at longer durations for combined F&V intake suggests that there may be challenges in sustaining participant engagement or adherence over time. For fruit and vegetable intake, the drop in positive impact from 3 to 6 months might indicate that the initial excitement has faded or that challenges persist. On the other hand, the increase at 6–12 months suggests a delayed impact on behavior change, potentially due to the time needed for habit formation. 44 However, the decline beyond 12 months underscores the need for strategies like booster sessions or systemic changes to sustain long-term behavior change. 45 Short-term interventions may benefit from initial enthusiasm and novelty, but longer interventions may struggle to maintain momentum due to diminishing motivation, competing priorities, or intervention fatigue. However, due to the nature of this analysis, we cannot attribute causality to the association between the intervention duration and the study impact. It is possible that some of the methodological characteristics of the studies, such as smaller sample sizes, different countries/contexts, seasonality impacting F&V availability and/or less intense intervention strategies, may also have affected study outcomes. Nevertheless, this finding highlights the importance of developing dynamic and adaptable strategies that evolve throughout the duration of the program. Implementing periodic reinforcement and personalized support may effectively sustain interest and compliance and eventually lead to the desired long-term behavior change. From a research perspective, studies comparing different durations would be useful to better understand the factors contributing to declining impact and identify specific challenges that require targeted solutions.
Nearly 80% of the intervention comparisons included in this scoping review implemented nutrition communication alone or as part of the intervention strategy, while only 7% included social protection, nutrition-sensitive agriculture or environmental restructuring intervention alone. About 17% of intervention comparisons included 2 or more intervention components (nutrition and/or health communication, social protection, agricultural programs, environmental restructuring). The idea behind multifaceted interventions is that they can simultaneously help address multiple barriers to F&V intake. Within nutrition communication interventions, combined implementation approaches were frequently used, such as group-based approaches, IPC, mass media, and ICT. One systematic review found no evidence that multifaceted strategies are more effective than single-strategy interventions. 46 Further research is needed to compare the impact of single- and multi-component interventions on increasing F&V intake. A detailed review of the impact of interventions by component and implementation method is provided in an accompanying article by Koyratty et al. 17
Some interventions specifically assessed the intake of only fruit or vegetables, indicating a targeted approach in certain studies. Interestingly, a substantial proportion of the interventions evaluated only the combined intake of F&V, while few researchers also reported all 3 outcomes (fruit, vegetables, and combined F&V). While it is important to determine the intake of various fruit and vegetable groups to understand specific consumption patterns, evaluating and reporting the combined intake of F&V is equally useful to assess adherence to WHO and country-specific recommendations. Therefore, we would like to encourage researchers of studies on F&V intake to evaluate the quantitative intake of all 3 outcomes: fruit, vegetables, and the combined F&V.
Accurate dietary assessment methods are essential for understanding dietary intake and patterns, which are critical for informing recommendations. However, a range of methods were employed to assess F&V intake across the included studies, complicating direct comparisons between intervention arms. Hence, efforts to improve and standardize dietary assessment methods are crucial. Consistent with a prior systematic review on physical activity and dietary behavior, 47 FFQs were the most widely used dietary assessment method in the included studies. However, FFQs rely heavily on memory, making it challenging to quantify portion sizes accurately, and they are prone to higher rates of misreporting compared to a 24HR.48,49 In contrast, 24HR methods collect more detailed information about foods and beverages consumed in the past 24 h, but these methods also depend on remembering details of foods and estimating quantities consumed, making them prone to reporting bias.48,49 Importantly, our brains are better at remembering emotional or surprising experiences rather than routine activities, like daily food intake. 50 Nonetheless, FFQs and 24HRs are valid methods for assessing dietary intake and dietary patterns.48,49 In the present review, we explored whether certain dietary assessment methods may be more likely to bias the study findings but could not identify a clear pattern. This may imply that there is no difference in positive impact by dietary method, or more likely, that we could not identify a difference due to the large variety in methods used and outcomes reported, resulting in small numbers of studies for this comparison.
Overall, about one-quarter of the intervention comparisons that met the inclusion criteria conducted follow-up assessments to determine if the impacts on F&V intake were sustained after the intervention ended. To better understand the long-term effectiveness and sustainability of these interventions, future research should incorporate follow-up evaluations across short-, medium-, and long-term periods, providing valuable insights into the lasting impact of interventions on F&V intake. The importance of long-term evaluation in F&V interventions has been underscored in previous work, including a systematic review by Savoie-Roskos et al, 13 which emphasized the need for assessments over a year to better understand how F&V interventions impact dietary changes.
Because our goal was to review the available evidence on interventions that may increase the dietary intake of F&V, a key characteristic of this scoping review is that only studies reporting dietary intake of fruit, vegetables, or combined F&V intake were eligible for inclusion. As a result of these strict inclusion criteria, studies that did not assess F&V intake were excluded. Hence, we did not focus on determining all the evidence on a specific intervention but instead explored the evidence available on any intervention assessing dietary intake of F&V. Consequently, we included and reviewed a heterogeneous set of studies across all countries, all population age groups, using any type of intervention and any type of dietary assessment method. Because of this heterogeneity, it was challenging to systematically assess the magnitude of statistically significant increases in reported results, which hindered direct comparisons of the varying outcome measures, such as mean differences in grams/day, cups/day, portions/day, and percentages meeting WHO recommendations. We were, therefore, unable to ascertain whether the statistically significant increases in F&V intake may have any public health relevance or are biologically plausible. These limitations underscore the need for standardized dietary metrics and frameworks in future research to enable more consistent evaluations.
Since this was a scoping review, we did not undertake a quality or transparency appraisal of the included studies. A key strength of this approach is that it offers an overview of the landscape of F&V intake interventions, highlighting trends, gaps, and diverse methodologies. This inclusivity allows for the identification of areas where more focused, high-quality research is needed, particularly in underrepresented regions and populations. Limiting our inclusion criteria to studies published in English may have resulted in the exclusion of relevant research published in other languages, particularly French and Spanish, from LMICs, where these are official languages.
Conclusions
This scoping review found significant disparities in the geographical distribution of F&V intake intervention studies. Data were especially limited from Southeast Asia, South America, the Caribbean and sub-Saharan Africa. Expanding research and interventions in LMICs and underrepresented regions could contribute to more comprehensive and effective global health strategies, improving dietary habits and health outcomes worldwide. Additionally, broadening the focus of interventions to underrepresented groups, such as pregnant and lactating women, older adults, adult men and families/households, may enhance the relevance and efficacy of these interventions. There is also a clear need for harmonization of study designs and methods to assess the impact of various intervention strategies more accurately. Specifically, quantitative dietary assessment methods should be prioritized to compare the F&V intake in the study population with the daily amount of F&V recommended. Lastly, the majority of interventions used 1 or more approaches to provide nutrition and health communication, but only a few studies used multiple intervention components to address several barriers to adequate F&V intake simultaneously. More research is needed using multi-disciplinary, multi-component interventions recognizing that F&V intake is often inadequate due to limited availability, accessibility, affordability, and desirability.
Supplemental Material
sj-docx-1-fnb-10.1177_03795721251314141 - Supplemental material for Interventions on Fruit and Vegetable Intake in Low-, Middle-, and High-Income Countries: A Scoping Review of Evidence and Knowledge Gaps
Supplemental material, sj-docx-1-fnb-10.1177_03795721251314141 for Interventions on Fruit and Vegetable Intake in Low-, Middle-, and High-Income Countries: A Scoping Review of Evidence and Knowledge Gaps by Fusta Azupogo, Nadia Koyratty, Taryn J. Smith, Guy-Marino Hinnouho, Manisha Tharaney, Lilia Bliznashka, Dorcas A. Amunga, Imelda Angeles-Agdeppa, Eva Goyena, Frederick Grant, Joyce Kinabo, Irene Medeme Mitchodigni, Renuka Silva, Hasara Sitisekara, Deanna K. Olney and Sonja Y. Hess in Food and Nutrition Bulletin
Supplemental Material
sj-xlsx-2-fnb-10.1177_03795721251314141 - Supplemental material for Interventions on Fruit and Vegetable Intake in Low-, Middle-, and High-Income Countries: A Scoping Review of Evidence and Knowledge Gaps
Supplemental material, sj-xlsx-2-fnb-10.1177_03795721251314141 for Interventions on Fruit and Vegetable Intake in Low-, Middle-, and High-Income Countries: A Scoping Review of Evidence and Knowledge Gaps by Fusta Azupogo, Nadia Koyratty, Taryn J. Smith, Guy-Marino Hinnouho, Manisha Tharaney, Lilia Bliznashka, Dorcas A. Amunga, Imelda Angeles-Agdeppa, Eva Goyena, Frederick Grant, Joyce Kinabo, Irene Medeme Mitchodigni, Renuka Silva, Hasara Sitisekara, Deanna K. Olney and Sonja Y. Hess in Food and Nutrition Bulletin
Supplemental Material
sj-docx-3-fnb-10.1177_03795721251314141 - Supplemental material for Interventions on Fruit and Vegetable Intake in Low-, Middle-, and High-Income Countries: A Scoping Review of Evidence and Knowledge Gaps
Supplemental material, sj-docx-3-fnb-10.1177_03795721251314141 for Interventions on Fruit and Vegetable Intake in Low-, Middle-, and High-Income Countries: A Scoping Review of Evidence and Knowledge Gaps by Fusta Azupogo, Nadia Koyratty, Taryn J. Smith, Guy-Marino Hinnouho, Manisha Tharaney, Lilia Bliznashka, Dorcas A. Amunga, Imelda Angeles-Agdeppa, Eva Goyena, Frederick Grant, Joyce Kinabo, Irene Medeme Mitchodigni, Renuka Silva, Hasara Sitisekara, Deanna K. Olney and Sonja Y. Hess in Food and Nutrition Bulletin
Footnotes
Author Contributions
Conceived and designed the study: TJS, NK, FA, LB, GMH, DKO, and SYH. Literature search: TJS and FA. Screening and data extraction: FA, TJS, NK, GMH, SYH, and LB. Writing the first draft of the manuscript: FA, TJS, NK, GMH, and SYH. Contributed to the editing of the manuscript: MT, LB, DAA, IAA, EG, FG, JK, IMM, RS, HS, and DKO. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the CGIAR Trust Fund: https://www.cgiar.org/funders.
Ethical Considerations
This scoping review did not involve human subjects.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.