
Abstract
Background:
Pernicious anemia (PA) is a type of macrocytic anemia caused by autoimmune gastritis. To facilitate timely diagnosis and treatment of PA there is a pressing need for improved understanding among Healthcare providers of the condition’s symptoms and diagnostic criteria.
Objective:
This systematic review aims to extend existing clinical knowledge on the presentation of PA by determining which symptoms and clinical complications are reported in published adult case studies.
Methods:
Relevant studies were identified through electronic searches of PsycINFO, Embase, and MEDLINE, via OvidSP. During data extraction symptoms were categorized according to the International Classification of Diseases and were grouped based on frequency.
Results:
Symptoms were documented for 103 adults with a diagnosis of PA; the most frequent symptoms were fatigue (55%), loss of sensation in limbs (32%), excessive weight loss (27%), and a sore tongue (23%).
Conclusions:
This review highlights the diverse symptomology of adults who are diagnosed with PA. Most symptoms documented in case studies are consistent with the core signs of B12 and folate deficiencies. Research is needed to identify if there are common clusters of PA symptoms that can be used as prompts for diagnostic testing in patients with suspected B12 deficiency.
Plain language title
A Review of Symptoms of Pernicious Anemia
Plain language summary
This study reviewed case studies that have been written about adults with pernicious anemia, it has documented the frequency of the core symptoms and the impact these have on health.
Background
Pernicious anemia (PA) is an autoimmune disease that can cause Vitamin B12 deficiency by malabsorption. Initially, PA was considered as a form of macrocytic anemia. 1 However, as anemia is not always present, the diagnosis now relies on identifying diminished levels of Vitamin B12, raised concentrations of methylmalonic acid (MMA) and/or homocysteine, and the presence of intrinsic factor or parietal cells antibodies. 2 Globally, PA is a common cause of Vitamin B12 deficiency and is implicated in approximately 20% to 50% of adult cases worldwide. 3 Although the disease predominantly affects older adults, with a prevalence of around 1.9% within this demographic 4 ; there is significant underdiagnosis and undertreatment of the disease particularly among individuals below the age of 60. 5
Pernicious anemia is challenging to diagnose in clinical practice. 6 The symptoms are nonspecific and insidious, making it difficult for patients and their healthcare providers to recognize disease early. Individuals who present to primary care with characteristic signs and symptoms of the condition can experience lengthy diagnostic journeys and it is not uncommon for symptoms to be initially misdiagnosed as anxiety or depression. 7 Patients report that the most commonly experienced symptoms are unrelenting fatigue, memory loss, and difficulty maintaining concentration. 8 These symptoms are consistent with the core signs documented in guidelines for diagnosing B12 and folate deficiencies. 9 However, PA case studies within clinical literature often describe a complex heterogenous disease that has a broad spectrum of symptoms; these include gastrointestinal manifestations neurological and cognitive impairment. 10
Many patients with PA describe their experiences of receiving a diagnosis as a “battle,” and it is common for patients to report experiencing diagnostic delays of up to 5 years. 7,8 In the United Kingdom the need for improved management of PA has been identified by the National Institute for Health and Care Excellence who are due to publish their first treatment and diagnosis guideline for B12 deficiencies in 2023. 11 To facilitate changes which enable timely diagnosis and treatment, healthcare providers must be aware of both biomedical markers of the disease and the varied ways in which PA can present. This systematic review aims to extend existing clinical knowledge by identifying the frequency of PA symptoms and their clinical complications in adult cases. The review focuses on published case studies that have documented diagnosis in adults and will contribute rigorous insight into the heterogeneity of PA symptoms This, in turn, can inform the development of diagnostic tools to facilitate accurate and timely diagnosis.
Methods
Protocol and Registration
This systematic review was prepared according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (PRISMA). 12 The review protocol was registered on the International Prospective Register of Systematic Reviews (PROSPERO) database (ID: CRD42022335508). 13
Search Strategy
Relevant studies were identified through electronic searches of PsycINFO, Embase, and MEDLINE, via OvidSP databases. Publication type was restricted to peer-reviewed journal articles written in English or translated into English and published up until May 30, 2022. The search was completed using the following free text and Medical Subject Headings pernicious anemia, macrocytic anemia, megaloblastic anemia, vitamin B12 deficiency, autoimmune atrophic gastritis, atrophic gastritis, autoimmune gastritis, parietal cell antibodies, anti-parietal cell antibodies symptom* lived experience, patient journey.
The search strategy for each individual database is presented in the Online Supplementary Material (Supplmentary Materials Figure 1).
Study Selection
Publications were included in this review if they reported symptoms experienced by an adult diagnosed with PA. Eligible study designs included case study reports, case series, case–control studies, and cohort studies. There were no restrictions on the study or sample size. Editorial or narrative reviews and grey literature, books, book chapters, and editorials were excluded. Only studies that reported PA as the primary medical condition were included in the review. Studies reporting Vitamin B12 deficiency as secondary to another acute or chronic condition were excluded. Studies that primarily reported the symptoms of PA in infant or pediatric patients were excluded. Where a case study reported on symptoms of multiple patients with B12 deficiency, only patients whose symptoms were attributed to PA were recorded.
Study Quality and Data Extraction
Titles and abstracts of all retrieved records were screened for duplication and to assess if they met the inclusion criteria. Two authors (CHS and AB) screened full texts of all potentially relevant studies to determine their inclusion, with any discrepancies being resolved by discussion and consensus. The following data were extracted from eligible articles and tabulated: bibliographic details of the study (title, authors, study type, publication year, country), population characteristics (age, gender, clinical diagnosis), and clinical outcomes (symptoms, serum B12 levels, hemoglobin levels, and diagnostic tests). As all the featured studies were case study reports, only descriptive analysis was possible. Symptoms were categorized into symptom groups, using the International Classification of Diseases (ICD). 14 Symptoms that were experienced by only one individual were not clustered in terms of frequency. The quality of case reports was assessed using the Joanna Briggs Institute critical appraisal checklist for case reports. 15 This tool considers the clarity of the description of (1) patient demographics, (2) patient history, (3) clinical condition, (4) diagnostic tests and methods, (5) treatments, (6) post intervention condition, (7) adverse events, and (8) key lessons.
Results
A total of 4216 articles were returned from the searches of which 132 full-text publications were included based on the title and abstract (see Figure 1 for overview). Papers excluded during full-text review (n = 57) reported cases where PA was secondary to the presenting diagnosis (n = 44) or was diagnosed in infants (n = 13). Seventy-five case studies were included in the full review, representing the experiences of a total of 103 patients. Case studies were published between 1978 and 2021.
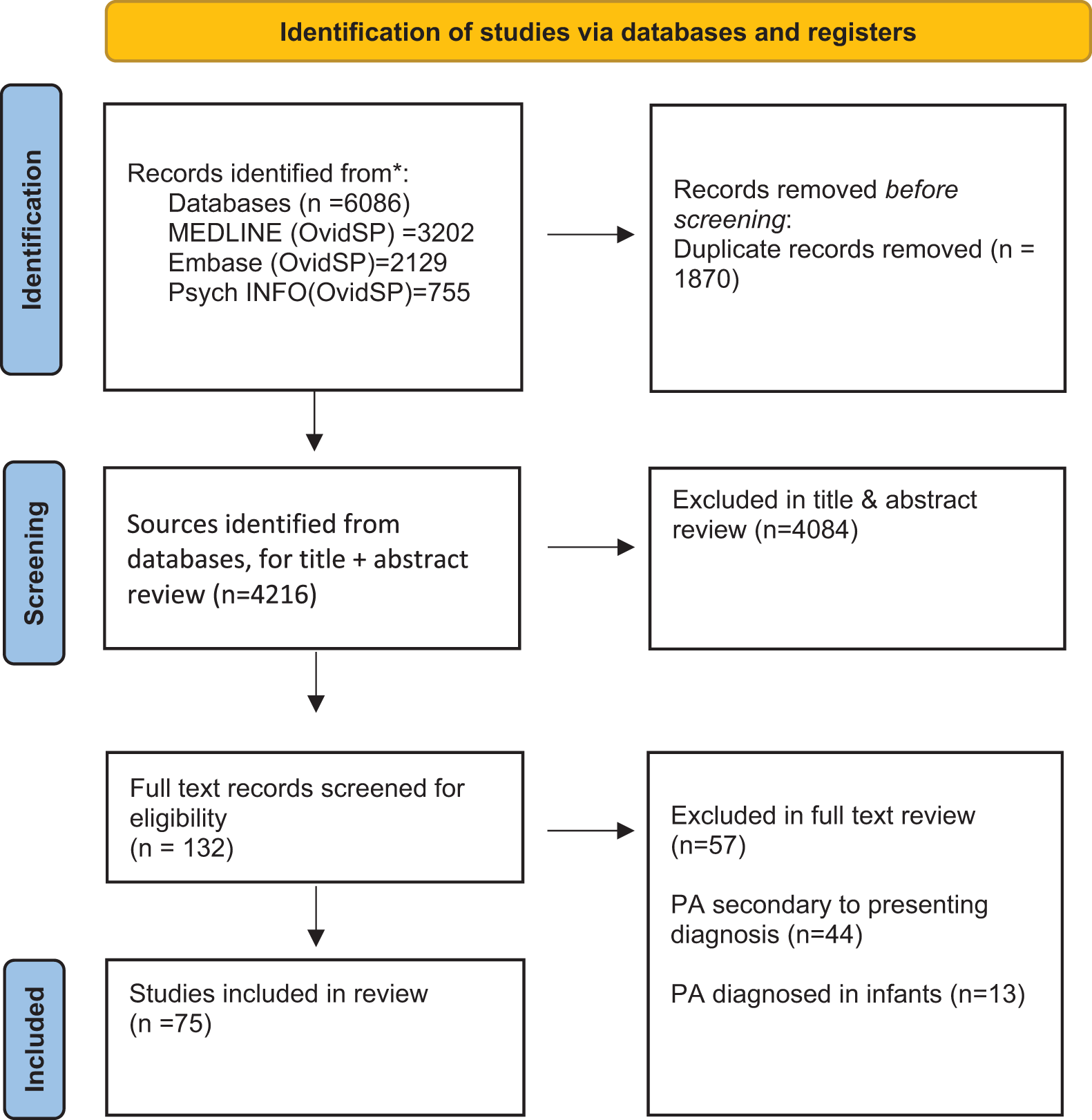
PRISMA 2020 flow diagram for new systematic reviews which included searches of databases and registers only.
Pernicious anemia symptoms documented in patients’ case study notes were extracted and tabulated (Table 1). Table 2 presents an overview of patient demographics, clinical characteristics, and treatment settings; the case studies described the symptoms of 66 females and 37 males whose ages ranged from 16 to 90 years. Ethnicity was not reported for 70% of the cases; where an individual’s ethnicity was stated, most patients were categorized as black. Pernicious anemia is typically diagnosed and treated within primary care settings. Some case studies described patients who were treated as inpatients within a secondary healthcare setting (e.g., emergency departments, neurology, and general medicine) and only a small number of patients had been referred to an outpatient clinic via their primary care practitioner (<5%).
Frequency of Symptoms Reported in Patients.a
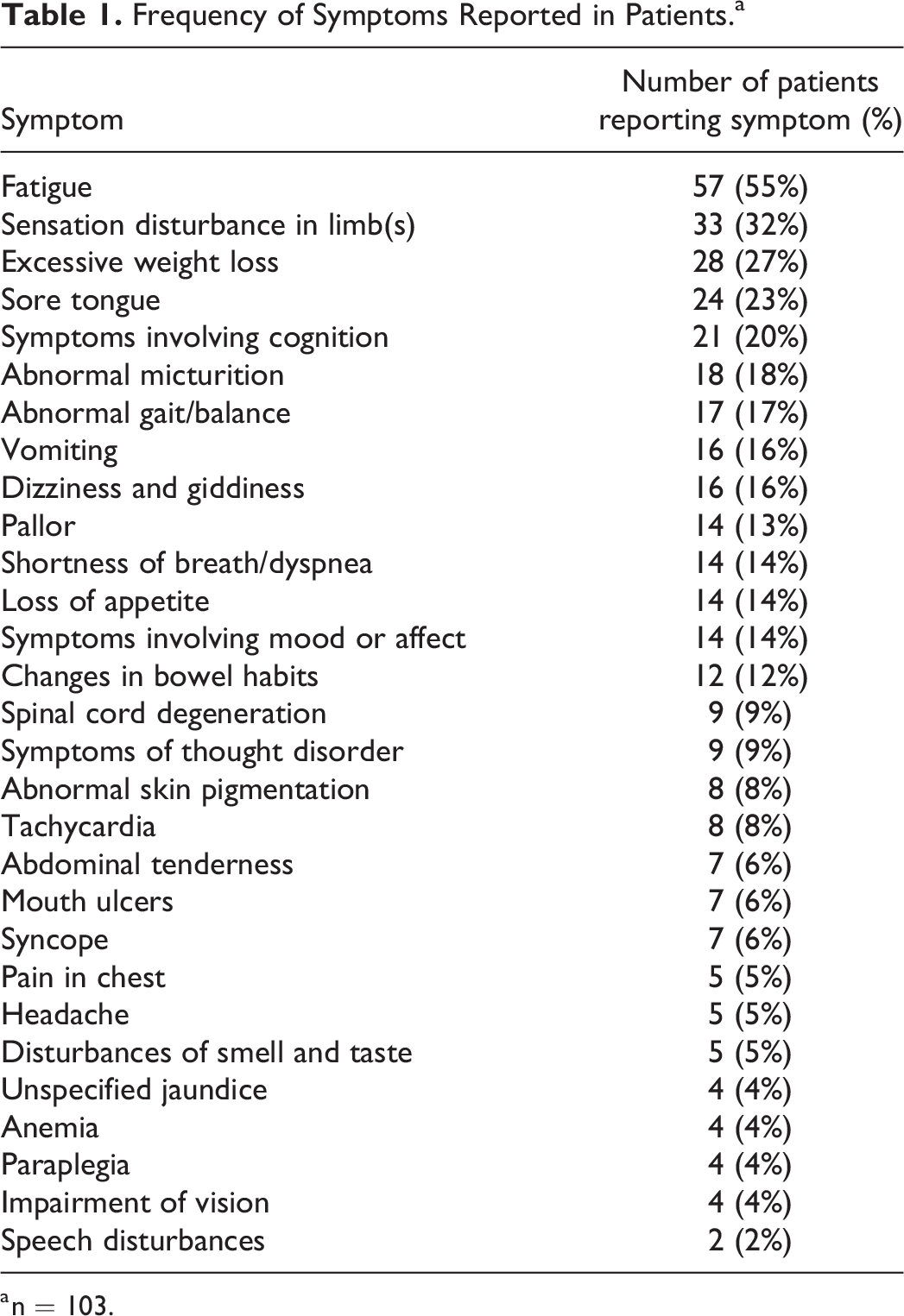
a n = 103.
Demographic and Clinical Characteristics of Patients.a
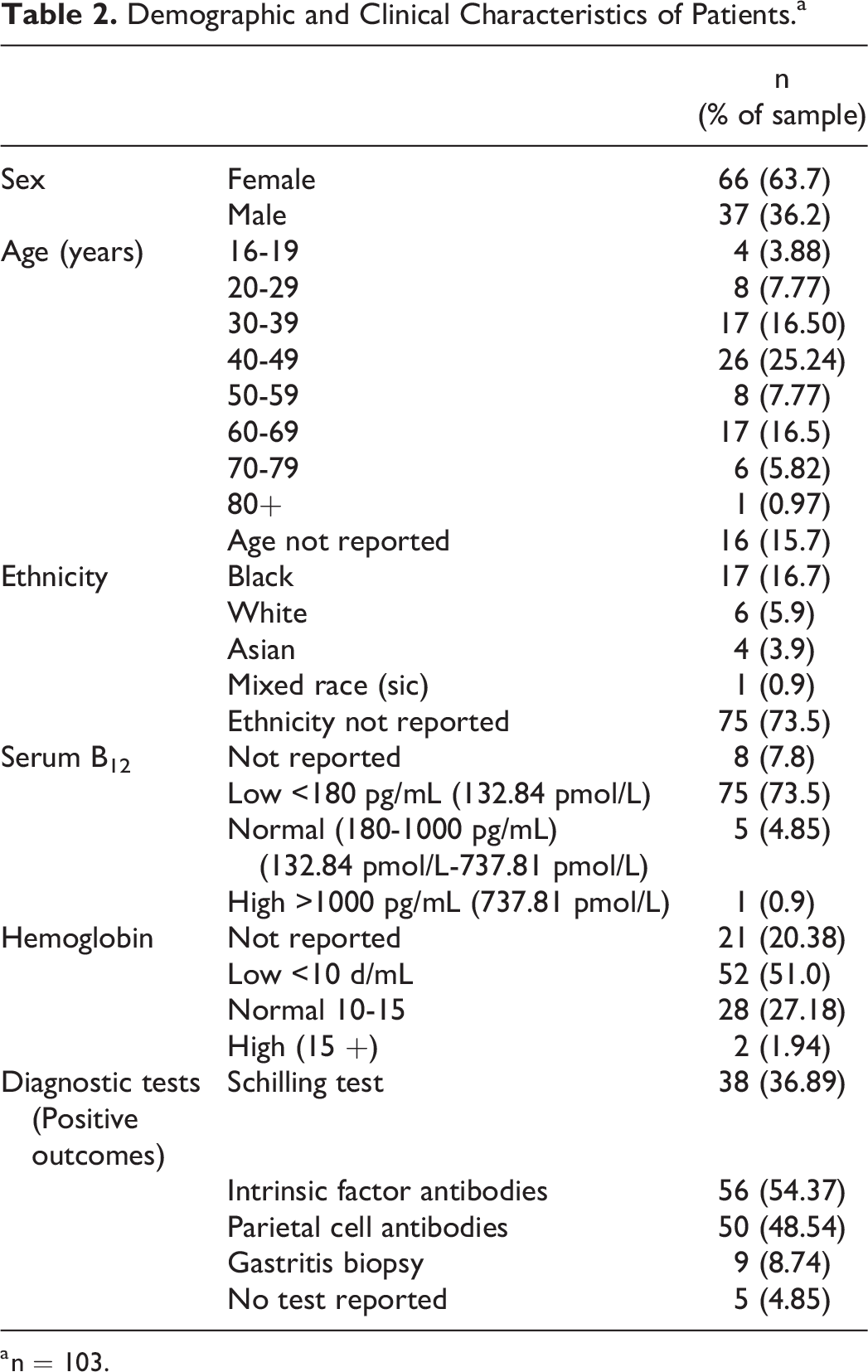
a n = 103.
Although PA diagnosis can be confirmed by histopathology, this was rarely performed and most of the case studies relied on biomarkers such as low serum vitamin B12 for diagnosis. For most patients, a diagnosis of PA was attributed to testing positive for intrinsic factor antibodies with/without parietal cell antibodies. Some patients had diagnoses confirmed by the Schilling test (n = 38); however, these tended to be older case studies published in the 1960s or 1970s. Nine individuals had atrophic gastritis confirmed via biopsy. Five of the case studies did not report which laboratory tests were used to confirm diagnosis. Serum B12 levels prior to treatment were reported in 95 patients; almost all individuals were described as deficient in B12 and had serum B12 levels which were <180 pg/mL (132.84 pmol/L). In 5 case studies, patients were described as having B12 levels that were within normal ranges; however, these patients were diagnosed with a functional B12 deficiency as evidenced by elevated MMA and homocysteine values. Hematological abnormalities indicating low hemoglobin were found in two thirds of cases.
Across the case studies there were 94 different symptoms recorded (Table 1); case notes documented between 1 and 11 symptoms, with the mean number of symptoms reported for each patient being 4 (standard deviation = 2.53). The symptoms were categorized by the ICD into 29 symptom groups which are outlined in terms of frequency in Table 1. Four symptoms could not be classified using the ICD (i.e., coldness, grey hair, scaly skin, and Lhermitte phenomenon). Fatigue was the most frequently reported symptom and noted in just over half of the cases. It was also common for patients to experience changed sensation in their limbs or extremities, this included numbness, tingling or burning pains in hands, feet, and legs. Where such symptoms were present prior to diagnosis patients received a neurological assessment to confirm pathology. Rapid weight loss was common and documented in over a quarter of the case studies with the patient experiencing weight reductions upward of 20 kg. Although cognitive symptoms were common (20%), most symptoms of this nature were self-reported (e.g., memory loss, aphasia, confusion, and difficulty concentrating) and few patients received cognitive assessments to confirm impairment. Where clinical assessment of cognitive performance had been made, there was documentation of impairment in executive functioning and global cognitive decline. A lower percentage of patient notes recorded general mood changes such as increased irritability, depression, anxiety, and apathy (12%). Around a third of the case studies described neurological symptoms such as loss of feeling in limbs or extremities and 10% of the sample had spinal cord degeneration. Several rare complications of PA were documented which had high clinical significance due to their potential for disability or mortality. For example, spinal cord degeneration had caused disability in 9 patients, a similar number of patients had been admitted as psychiatric inpatients after experiencing serious mental health symptoms (i.e., psychosis, hallucinations, and paranoid delusions) caused by undiagnosed PA.
Discussion
This review is the first to systematically document symptoms that are associated with PA. Most patients described in the case studies had severe disease that appeared to have been present but undiagnosed for a considerable time; across these cases there was a broad range of symptoms which varied in intensity and frequency. The symptoms attributed to PA overlap with those experienced by patients who have other causes of vitamin B12 deficiency (e.g., medication, low dietary intake, gastric surgery) suggesting that there are no disease-specific markers for PA. 10 A recent paper exploring the lived experience of PA diagnosis indicates that “extreme or unrelenting fatigue” is a common reason why individuals decided to visit their healthcare provider. 16 Surprisingly, this systematic review found that only 50% of case studies noted that the patient had been experiencing fatigue. Discordance between patient self-reported symptoms and case notes have been found in other chronic conditions. 17 It is important to acknowledge that the psychological or emotional impact of PA symptoms such as fatigue may be underrecognized within case notes.
The case reports included in this review provide high quality descriptions of the clinical condition and diagnostic process; however, many did not provide information on key patient demographics such as ethnicity (73%) or age (15%). Some of the case studies included limited information on patients’ medical histories, which makes it difficult to establish how long patients had been experiencing symptoms or if symptoms could be attributed to other comorbid conditions. It is imperative to get a clear picture of patients’ clinical history, as PA is associated with an increased risk of other autoimmune disorders that may have overlapping symptoms. 18 When synthesizing the evidence from this review, we must acknowledge that there is a potential of publication bias within case reports. It is often the most interesting/surprising cases that are presented as case studies in published literature. This bias could be overcome by reviewing the results of cohort studies where medical records have been checked over a specific period. However, no such studies were retrieved during the literature search.
In summary, this review highlights that the symptomology of PA is diverse. However, there are several groups of symptoms identified that could function as indicators for healthcare providers that further diagnostic testing is required. Many case studies in this review described patients who had experienced significant weight loss, alongside unexplained fatigue and changed sensation in their limbs. Further research should establish whether there are core symptom patterns that distinguish PA from other forms of B12 deficiency. The knowledge gained from this review can support the development of patient-reported outcome measures to support healthcare providers to monitor how the PA symptoms impact daily function. The findings derived from this review can aid healthcare professionals to recognize the heterogeneous spectrum of PA symptoms and instigate prompt treatment to prevent irreversible disease progression resulting from delayed diagnosis.
Supplemental Material
Supplemental Material, sj-pdf-1-fnb-10.1177_03795721241227016 - A Systematic Review of Symptoms of Pernicious Anemia
Supplemental Material, sj-pdf-1-fnb-10.1177_03795721241227016 for A Systematic Review of Symptoms of Pernicious Anemia by Catherine Heidi Seage, Alexis Bennett, Nicola Ward, Lenira Semedo, Clara H. M. Plattel, Kim I. M. Suijker, Jolande Y. Vis and Delyth H. James in Food and Nutrition Bulletin
Supplemental Material
Supplemental Material, sj-pdf-2-fnb-10.1177_03795721241227016 - A Systematic Review of Symptoms of Pernicious Anemia
Supplemental Material, sj-pdf-2-fnb-10.1177_03795721241227016 for A Systematic Review of Symptoms of Pernicious Anemia by Catherine Heidi Seage, Alexis Bennett, Nicola Ward, Lenira Semedo, Clara H. M. Plattel, Kim I. M. Suijker, Jolande Y. Vis and Delyth H. James in Food and Nutrition Bulletin
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.