
Abstract
The causes and risk factors of vitamin B12 deficiency are many and varied. Importantly, they vary considerably across the lifespan, from infancy to old age. The complexity of the physiology of vitamin B12 bespeaks the myriad of possible causes of deficiency and possible disruptions of its functional integrity. These lead ultimately to the pathobiological effects witnessed in deficiency of this fascinating micronutrient. This brief overview of the multiplicity of mechanisms that can result in vitamin B12 deficiency, and the panoply of its manifestations explores the underlying reasons for the protean presentations of the disease. As the human organism progresses through the chronology and milestones of age, various susceptibility factors arise resulting from the interplay of environmental and genetic factors. Acting independently and in concert, these factors produce the common denominator of vitamin B12 deficiency. However, the rate at which such deficiency develops and the way in which it presents clinically vary widely, subject to such influences as genetic variability, end-organ susceptibility, and concomitant micronutrient status. Some examples of unusual cases of vitamin B12 deficiency are described. Much has been learned about the last of the numbered vitamins in almost a century. Much yet remains to be discovered.
If you want to want the present to be different from the past, study the past
Much information has accumulated over almost 100 years since the landmark identification of a cure for pernicious anemia and the subsequent discovery of vitamin B12. The fascinating history covering this epoch of scientific discovery has been extensively reviewed. 1,2 Pernicious anemia carried a dismal prognosis before the Nobel Prize-winning discovery that a liver-derived substance was able to effect a cure. Figure 1 shows the Kaplan-Meier survival curve of the disease prior to this discovery. The median survival was less than 20 months. Mainly because of the emphasis on pernicious anemia as a cause of B12 deficiency, it was previously considered that B12 deficiency was mainly a disease of old age. However, B12 deficiency is certainly not confined to the elderly but can occur at any age and indeed may be a cause of severe morbidity among children and young adults, particularly in some parts of the world. 3,4
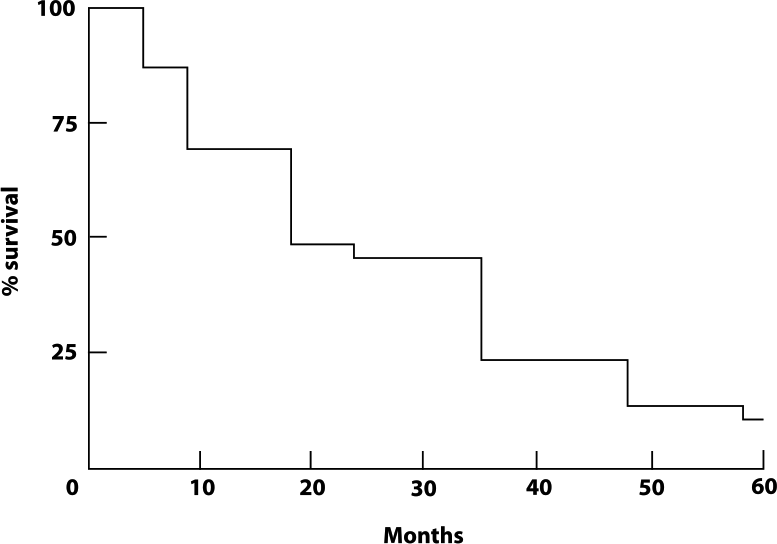
Kaplan-Meier survival curve of 321 patients with pernicious anemia, generated from the publication by Cabot (1908). 5 The median survival was less than 20 months and the 5-year survival less than 10 per cent.
Before getting into the central topic of my presentation, I want to pay a special tribute to one of the several scientists who were awarded Nobel Prizes for their work related to B12. Dorothy Crowfoot Hodgkin received the Nobel Prize for Chemistry in 1964 for elucidating the complex 3-dimensional structure of the B12 molecule using X-ray crystallography (Figure 2). The exciting story of her life and discovery is described in a fascinating biography. 6 At the age of 38, with a new baby and a blossoming research career, an infection triggered Hodgkin’s first attack of rheumatoid arthritis. She wrote: “I found I had great difficulty and pain in getting up and dressing. Every joint in my body seemed to be affected.” After a few weeks of treatment at a specialist clinic, Hodgkin returned to the lab. There, she found her hands had been so affected that she could no longer use the main switch of the X-ray equipment required for her experiments. Undeterred, she had a long lever made for the switch and carried on with her research. Max Perutz, another Nobel Laureate, wrote of her: “Her love for chemistry and her students was combined with a brilliant mind and an iron will to succeed regardless of her frail and later severely crippled body.”
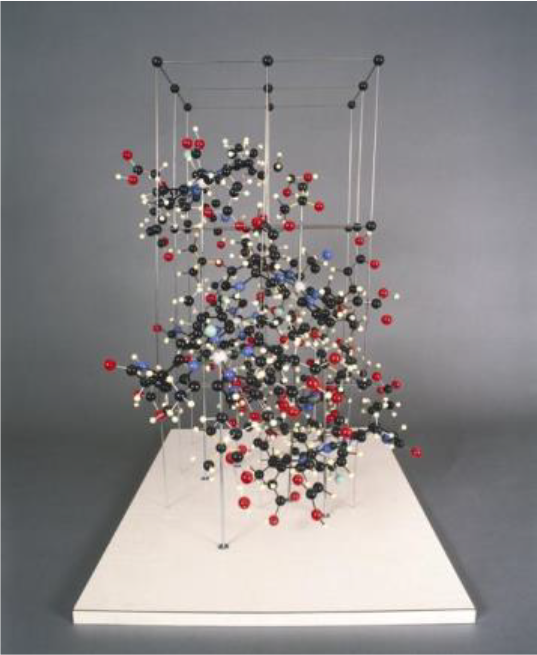
Three-dimensional model of the crystal structure of vitamin B12 (Image from the Science Museum Group ©).
There was, indeed, magic about her person. In 1989, at a symposium at Guy’s Hospital in London to commemorate the work of Sir Thomas Addison for his description of pernicious anemia, 7 I had the pleasure and privilege of meeting Dame Dorothy Hodgkin, who was the honorary president of the meeting. She was aged 89 and frail at the time, and my wife, Irene, and I, took her by each hand to help her cross a busy road from a reception at Lambeth Palace to a boat on the Thames. We were both struck by the fact that her hands were very gnarled by the disease that had afflicted her. Coincidentally, the following morning, Irene and I went to the Royal Academy on Piccadilly, where there was an exhibit of the works of Henry Moore.
On entering the exhibit, we were drawn to a sepia etching of deformed hands. Imagine our awe when we looked at the legend below this work that stated: “Hands of Dorothy Crowfoot Hodgkin” Figure 3 and https://www.tate-images.com/preview.asp?image=P02643]. The very hands that we had held the night before and the hands that manipulated the controls of the instrument that Hodgkin had used to decipher the structure of vitamin B12! We later learned that Henry Moore and Dorothy Hodgkin were good friends.

Hands of Dorothy Crowfoot Hodgkin—lithograph (Henry Moore, 1978). The Tate Gallery London.
We are here today to discuss that very molecule. Whether as scientists, health care providers, caregivers, or patients, our focus is on the many people who suffer from the deficiency of this molecule or perturbation of its handling in the body. Let’s examine the complexity of the mechanisms involved in capturing, protecting, conserving, and processing this precious micronutrient, an understanding of which is central to studying what can go wrong and result in B12 deficiency. The pathways for B12 absorption and metabolism are summarized in Figure 4. The detail behind this figure is described in the review from which it is taken. 4 The big picture is the complexity with which the body captures this precious micronutrient from the environment where it is present in very small quantities to satisfy the daily need for the vitamin through the help of various binding proteins in the gastrointestinal tract and the plasma, the specialized cellular receptors that serve as docking sites for the binding proteins, the intracellular chaperones for the trafficking of B12 and its delivery and conversion to its active forms.
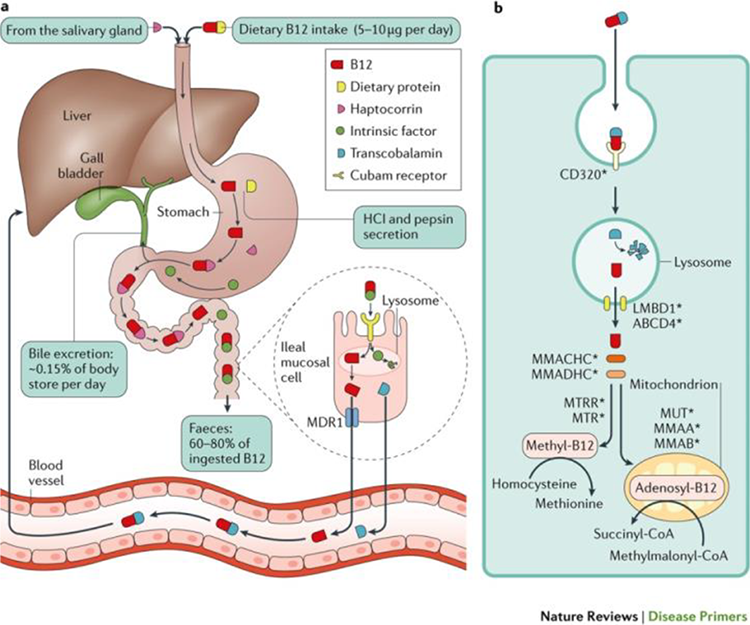
Absorption, enterohepatic circulation, and intracellular metabolism of vitamin B12. Green R, et al. 4
Remarkably, B12 is required as a cofactor for only 2 biochemical reactions in humans and other animals. One of these is the important methionine synthase reaction located in the cytoplasm in which the amino acid homocysteine is converted to methionine through methylation. This reaction requires folate in the form of methyltetrahydrofolate as a source of the methyl group, and the B12 in the form of methylcobalamin. The other reaction occurs in the mitochondria where the enzyme methylmalonyl Co-A mutase catalyzes the conversion of methylmalonyl-CoA to succinyl CoA and requires B12 in the form of adenosyl-cobalamin. In B12 deficiency, these reactions are impaired, increasing the levels of homocysteine and methylmalonate in the plasma. 4,8,9
Increased levels of homocysteine have been identified as a possible cause of vascular disease and are also associated with an increased risk of cognitive decline and incident dementia. 10,11 B12 deficiency is a leading cause of elevated homocysteine, particularly in an aging population consuming a folic acid-fortified diet. 12 Thus, an increase in homocysteine is one of the important metabolic consequences of B12 deficiency.
Overall B12 adequacy is determined by size of the store and the daily requirement or loss are the major determinants of balance. From this, the time to develop B12 deficiency can be calculated by the simple quotient of the body store divided by the daily requirement. On the accrual side of the equation, the main components are the dietary intake and the functional integrity of the absorptive mechanism. 13 It is becoming increasingly clear that the microbiome plays an important role in the bioavailability of B12 and, hence, the body balance of the vitamin.
Causes
As shown in Figure 5, many causes of B12 deficiency occur throughout the lifespan. Broadly speaking, these can be divided into inadequate intake, malabsorption, and miscellaneous causes. 13 Inadequate intake occurs primarily but not exclusively in low and middle-income countries around the world, and it is largely due to inadequate intake of animal products foods out of unaffordability or out of choice. In the more socioeconomically advanced countries of the world, the practice of vegetarianism and veganism contributes to B12 deficiency, and that primarily affects children, adolescents, and pregnant women. 3,14,15 B12 deficiency can have many causes in the pediatric age-group. In addition to dietary insufficiency, there may be inherited disorders of cobalamin absorption, transport, and metabolism. These are extensively described in several reviews. 16,17
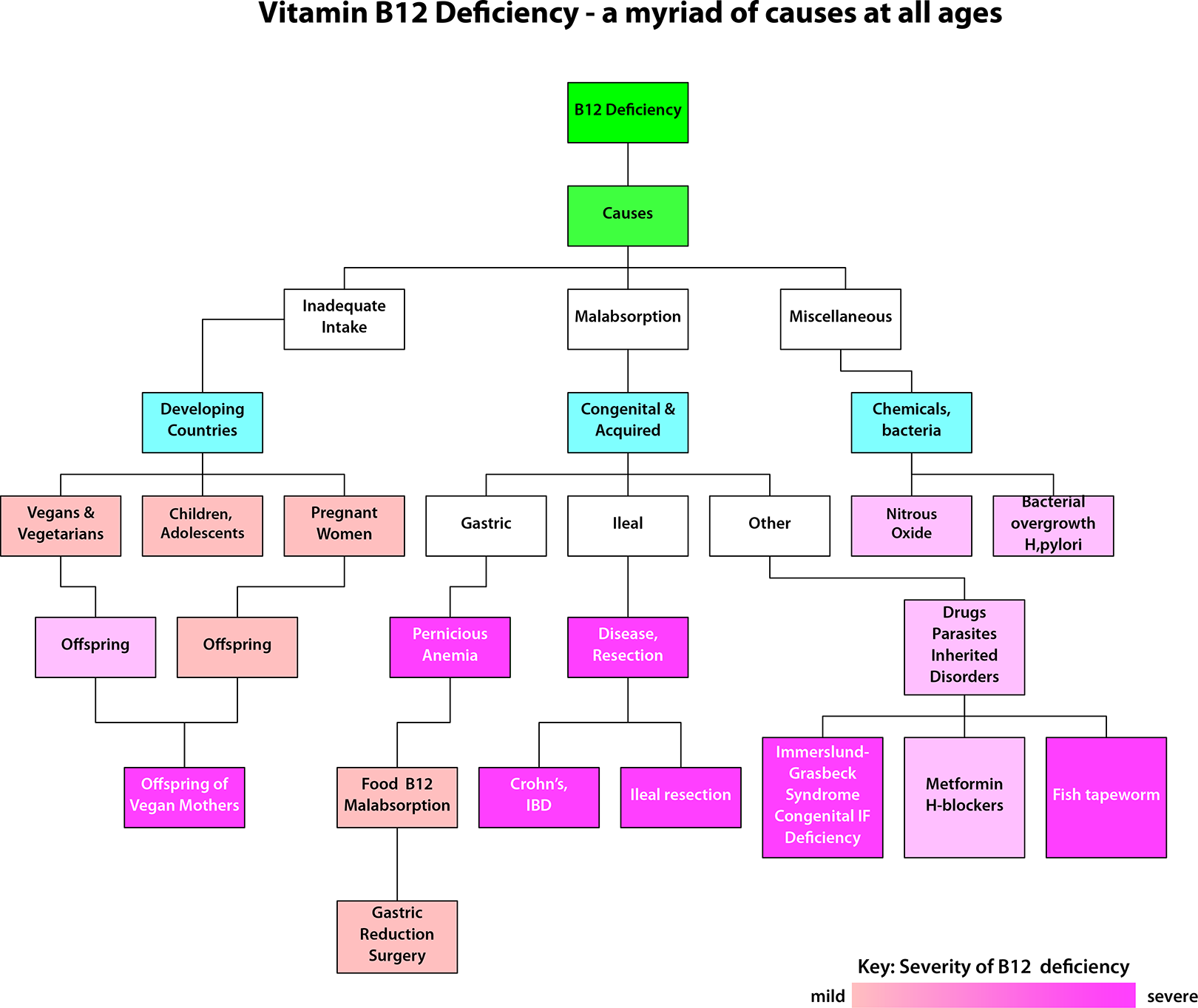
Vitamin B12 deficiency according to cause and severity.
The severity of B12 deficiency can vary tremendously and, in the figure, this is roughly depicted in terms of shading, the darker shades representing the more severe forms of deficiency. For example, the offspring of vegan mothers can suffer severe B12 deficiency. Another general rule is that both the severity and the rate of onset of the deficiency depend on whether or not the normal absorptive pathway remains intact. This is because abrogation of the normal pathway disrupts not only the absorption of ingested B12 but also the considerable amounts of B12 in bile, normally absorbed through the enterohepatic circulation. 18,19
Numerous causes of malabsorption result from perturbation of the various phases of the complicated process of B12 absorption, from gastric to intestinal. These causes are shown in Figure 5. Diseases and surgical removal or modification of the stomach or ileum, as well as drugs and parasites, all fall under this category. They are described in greater detail in the review references. 4,9,12 Among the miscellaneous causes are the anesthetic gas, nitrous oxide, the use of which has spread as a result of recreational use of the drug. 18
Just as there are a myriad of causes of B12 deficiency, so there are a multitude of manifestations of B12 deficiency, as shown in Figure 6. Here, the degree of shading roughly reflects the frequency of how commonly these complications are seen. Intriguingly, there has been a notable shift in the frequency of manifestations of B12 deficiency from hematological to neurological. The manifestations of the anemia include weakness, fatigue, and pallor. Classically, the anemia is macrocytic but sometimes may be normocytic for several reasons, such as the coexistence of conditions that would tend to produce smaller red cells like iron deficiency and thalassemia. 20 Other blood cell types may also be affected, so bleeding and infection may occur because of low platelets or white cells. The neurological complications may be protean and affect the brain, the spinal cord, and nerves, even resulting in cognitive defects. The classic subacute combined degeneration of the spinal cord affects the long posterior and lateral columns to cause defects in proprioception and vibration sense and peripheral neuropathy. Shown in the center of Figure 6 are the other miscellaneous manifestations of B12 deficiency like skin hyperpigmentation, premature, graying, and a smooth tongue. Quite frequently, there are gastrointestinal manifestations, including anorexia, abdominal discomfort, and weight loss. These occasional nonhematological and non-neurological manifestations of B12 deficiency are described more fully in the source references. 4,9,13 Interestingly, B12 deficiency has also been identified as a cause of neural tube defect pregnancies.
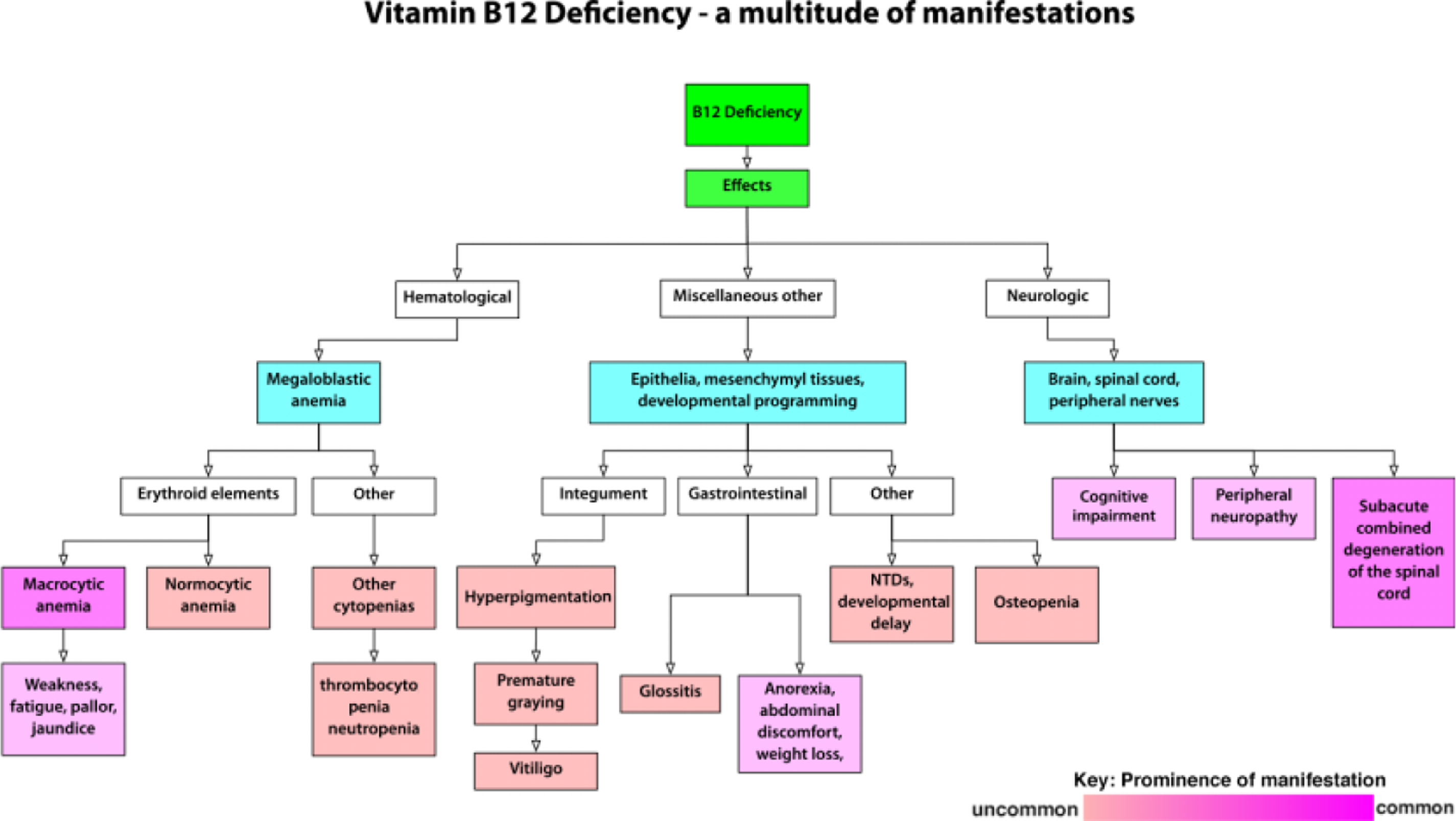
Complications of Vitamin B12 deficiency according to type and frequency.
Various combinations of features may occur, including neurologic complications, with or without anemia, smooth tongue, hyperpigmentation, and gastrointestinal symptoms. These can occur in no particular order, which is why there should be a high index of suspicion for B12 deficiency to make the diagnosis, with appropriate laboratory testing for low plasma B12, with or without the raised plasma metabolite levels, of methylmalonate and homocysteine.
The features of B12 deficiency may be atypical, as in the following examples, which have been described in more detail elsewhere. 21
A 64-year-old man of African origin with a 4-month history of leg weakness, tingling, and numbness with intervals of mental confusion was confined to a wheelchair. He had a history of refractory normocytic anemia, which had been treated with iron. He was anemic with an MCV of 87, a high RDW, and hypersegmented neutrophils. Serum B12 was less than 100 pg/mL and serum intrinsic factor antibody positive. He was treated with B12, his anemia resolved and his MCV fell from 87 to 75. He had 2 gene deletion alpha thalassemia, which is very common in people of African origin. 20 After B12 treatment, his neurological deficits improved, but he was left with some residual lower extremity weakness. The diagnosis in this patient was missed at first, simply because his anemia was normocytic. His B12 deficiency went unrecognized, and this resulted in profound neurological damage that was not completely reversible.
Another remarkable case is that of a 56-year-old apparently healthy male hospital employee who volunteered to establish normal ranges for methylmalonic acid and homocysteine in our laboratory. We were puzzled to find that he had a plasma homocysteine of 78 mmol/L and a methylmalonic acid of 1440 nmol/L, both considerably higher than the normal range for these metabolites. We checked and found that he had a low serum B12 but a normal blood count, blood smear, and apparently normal neurological examination conducted by a consultant neurologist. However, he did have serum antibodies to gastric parietal cells and intrinsic factor.
Following intramuscular B12 treatment, his serum homocysteine and methylmalonic acid levels became normal. Months later, on close questioning, he shared that in his job as a phlebotomist, he would frequently ride in the elevators to draw blood on different floors in the hospital. He was always puzzled that he could not appreciate the Braille elevator buttons through touch with his eyes closed. However, following his B12 replacement, he reported that he could feel the raised dots. The sensation of stereognosis, the ability to perceive the form of objects by tactile recognition, recovered, and he could again appreciate subtle shape differences. This modality of sensation is related to proprioception, or position sense, and requires intact functioning of the dorsal columns of the spinal cord.
These 2 cases illustrate the remarkable heterogeneity of clinical presentations of B12 deficiency. Other examples are given in a fuller description of these cases that can be found in the cited reference. 21 Patients may present with clinical pictures that may be mistaken for Alzheimer’s dementia, multiple sclerosis, or obscured by other coexistent hematological disorders like iron deficiency, thalassemia, or leukemia. More examples may be found in the excellent review by Wolffenbuttel et al. 22
Conclusion
The basic conclusion that we can draw is that B12 deficiency is a master of disguises at all ages and in many clinical situations, so it is prudent to have a high index of suspicion and to rule out B12 deficiency.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.