
Abstract
Background:
In French Guiana, restrictions to control the spread of SARS-CoV-2 were put in place between March 2020 and March 2022. In vulnerable urban neighborhoods, during this period, requests for food assistance increased and fear of hunger overtook fear of being affected by COVID-19.
Objective:
The objective of this survey was to describe food security during the COVID-19 pandemic in French Guiana and to study the relationship between the socioeconomic conditions of the study households and household hunger.
Methods:
A multicenter survey was therefore conducted in mobile clinics and fixed structures providing care to at-risk urban populations. In a face-to-face interview, a community health worker asked participants questions about the sociodemographic and economic profile of the household, and about household food security (food consumption score, coping strategies in the face of food shortages, and household hunger index). Two hundred seventy-seven households were recruited in February 2021.
Results:
According to the household hunger scale, 42.6% of households experienced moderate hunger and 23.8% of households experienced severe hunger in the month preceding the survey. Lack of residence permit, lack of social support, water insecurity, small housing, and lack of access to an urban garden were determinants related to the risk of household hunger.
Conclusions:
Food insecurity has affected a large majority of the households in this survey, and the immediate consequences for children’s health were already apparent. These results draw attention to a neglected health problem in a socioeconomically vulnerable population during the COVID-19 pandemic.
Keywords
Introduction
Hunger or undernourishment is an uncomfortable or painful sensation caused by insufficient food energy consumption. 1 When people are hungry, they are food insecure—they cannot physically and economically access sufficient safe and nutritious food that meets their dietary needs and preferences for an active and healthy life. 1 An estimated 9.8% of the world’s population (8.6% of the population in Latin America and the Caribbean) was undernourished in 2021. The number of people affected by hunger in the world increased with an estimated additional 150 million more persons since 2019, prior to the COVID-19 pandemic. 1 Vulnerable populations have experienced the side effects of the health crisis in a deeper and more lasting way, exacerbating existing inequalities within countries. 1 -3 Strict restrictions of movements during lockdowns, loss of employment, loss of income, disruption of food supply chains, increased prices, poor sanitation, and limited access to clean water expose vulnerable populations to a significant risk of hunger. 4,5
The South American region only represents 5% of the world’s population, but by 2021, it already accounted for a quarter of the world’s deaths from COVID since the beginning of the pandemic. 6 With successive waves of COVID-19, social inequalities have increased, alarmingly increasing poverty, homelessness, and food insecurity in this region. 6 -8
French Guiana is a French territory in South America with a population of 285 133 as of January 1, 2020, and a very high average population growth rate (+2.1%). Half of the population is under 25 years of age and one-third is of foreign nationality. Inequalities in living standards are very pronounced. 9 The unemployment rate is estimated at 16.1% (compared to 8% for France as a whole) 9 and the regional gross domestic product (GDP) was among the lowest in France but the highest in Latin America. Prior to the COVID-19 pandemic, half of French Guiana’s population was materially and socially disadvantaged according to the European Statistics on Income and Living Conditions. 10 In 2018, the poverty rate was more than 3 times higher than in mainland France (50% and 14%, respectively). 10 Moreover, according to a recent study, French Guiana was highly dependent on French and European imports for food and agricultural products. 11 The lack of food self-sufficiency and the lack of local competitiveness of businesses result in a very high cost of living: prices were 11.6% higher in French Guiana than in metropolitan France in 2018. 10
This territory was affected by the first pandemic wave of COVID-19 from June to August 2020 and then by a second wave in January 2021 (at the time of this survey). 12 Thus, successive social distancing measures implemented to control the spread of SARS-CoV-2 unfolded for 12 months with a territory-wide lockdown from March to May 2020 and then partial lockdown in parts of the territory; curfews were enforced depending on the epidemiological situation. 12 These restrictions have had a strong socioeconomic impact on the population of French Guiana: 20% decline in economic activity, −4% impacts on GDP, 22% drop in household consumption, and financial deterioration of one-third of the poorest households. 13 Although food availability was maintained during the health crisis (national subsidies, continued imports, etc), food prices increased. According to the National Directorate of Food, Agriculture and Forestry, the price of fruits and vegetables has increased between 2019 and 2020 by an average of +10%. In some urban neighborhoods, requests for food aid have increased and the fear of hunger has overtaken the fear of being affected by COVID-19. 14
No studies on food behavior have yet been conducted in the general population in French Guiana. Thus, food security in French Guiana prior to the health crisis has been poorly documented. In 2018, 18.9% of French Guiana population had reported not having meals with protein at least 1 day out of 2. 10 In a study conducted in informal neighborhoods around Cayenne in 2019, 14.3% of respondents reported daily difficulties in obtaining food. 15
Therefore, in the particular context of the health crisis, this article presents the main results of a survey on food insecurity conducted in vulnerable urban neighborhoods located on the coast in February 2021 during the health crisis. The objective of this survey was to describe the situation and to study the relationship between the socioeconomic conditions of the households studied and food insecurity during the COVID-19 pandemic.
Methods
Study Design and Recruitment
InaCov project was a multicenter cross-sectional study. Participants were recruited between January 25, 2021, and February 26, 2021, from mobile health clinics of the French Red Cross and of Doctors of World as well as from hospitals with continuous access to health care services, which deliver free outpatient care to uninsured at-risk populations. These inclusion centers were located in vulnerable neighborhoods of the 2 main urban areas along the French Guiana coastline (around Cayenne and Saint-Laurent-du-Maroni). These priority neighborhoods were identified by the municipal authorities in charge of city policy in French Official Journal (JORF n°0106 of May 7, 2015). The study area included 29 urban priority areas in the city comprising, according to the latest estimates, nearly 40% of the total population of French Guiana. 16
The study focused on the populations living in these defined areas and the results were not intended to be inferred to populations living outside of these areas. The inclusion criteria were to be aged ≥18 years, to receive care and to have insufficient health insurance. The InaCov project was approved by the National Regulatory authority Commission Nationale Informatique et Libertés (CNIL) (Privacy Impact Assessment, PIA of 12/17/2020, CNIL receipt number 2215826, and registered in the Health Data Hub [number F20210108145245]). All participants were given individual and written information about the study and gave their nonobjection to participate, as required by French Law.
Data Collection in the InaCov Project
In a face-to-face interview, a community health worker asked participants questions about their household for 20 to 30 minutes in their language. A nurse was also asked to check the weight, height, of a household child aged 6 to 59 months, accompanying the participant. The questionnaire consisted of 4 sections (1) sociodemographic and economic profile of household; (2) indicators to assess household food security, which were: Food Consumption Score (FCS), 17 Reduced Coping Strategies Index (r-CSI), 18 and Household Hunger Scale (HHS) 19 ; (3) Request for household food aid; (4) children: a measure of height and weight. 20
The FCS is a composite score by the World Food Programme (WFP), based on dietary diversity, food frequency over a 7-day recall, and relative nutritional importance of different food groups. 17 Each food item is given a score of 0 to 7, depending on the number of days it was consumed by the household. There are a total of 9 food groups: (1) cereals, roots, and tubers; (2) beans, peas, groundnuts, and cashew nuts; (3) vegetables and leaves; (4) fruits; (5) meat, poultry, eggs, and fish; (6) milk and milk products; (7) sugar and sugar products; (8) oils, fats, and butter; and (9) condiments. Each food group is assigned a weight, reflecting its nutrient density. For each food group, the household consumption frequencies were multiplied by its specified weight. The FCS was calculated by adding all the weighted consumption frequencies. The FCS was compared with WFP’s pre-established thresholds that indicated the status of the household: poor food consumption (0-28), borderline food consumption (28.5-42), and acceptable food consumption (up to 42).
The r-CSI was based on a 7-day recall and composed of 5 questions related to households coping behaviors in the face of a food shortage. 18 These 5 questions focused on (1) using cheaper and less preferred foods, (2) getting help from friends or relatives, (3) limiting portion sizes at mealtime, (4) restricting adult’s consumption to allow young children to eat, and (5) reducing the number of meals eaten in a day. For each strategy of r-CSI, the frequency of use in the past 7 days was reported in number of days (0-7) and multiplied by the assigned severity weight. The household’s total score was calculated by adding-up the weighted scores. To calculate the categorical food insecurity indicator, the median was used as a cutoff value (> 21: high use of coping strategies in response of food shortages). The higher the r-CSI score was (0-56), the greater the food insecurity was in the household.
The HHS is a 30-day household hunger measure that has been specially developed and validated for cross-cultural use. 19 The HHS questions ask about (1) not having any food in the house, (2) going to sleep hungry because there was not enough food, and (3) going a whole day and night without eating. Each frequency of occurrence answer of HHS questions is coded by 0 (no), 1 (rarely or sometimes), or 2 (often, more than 10 times), and their sum yields a continuous score (0-6). To establish the categorical indicator of food insecurity, 2 cutoff values (> 1: moderate hunger in the household and > 3: severe hunger in the household) are applied to this HHS score.
Nutritional Status of Children Under 5 Years of Age
The weight-for-height indicator can be used to identify a child who is underweight for his or her height or who is overweight or obese. 20 According to the WHO Child Growth Standards classification, when the weight-for-height indicator Z-score is less than −2, the child has moderately acute malnutrition and when the weight-for-height indicator Z-score is greater than +2, the child is overweight.
Analysis
Descriptive analysis
Overall, the collected data were summarized using frequencies and percentages for categorical variables and median (interquartile range [IQR]) or mean (standard deviation [SD]) values for continuous variables.
Measures
The standardized monthly income for the purchase of food was calculated as self-reported household total net income for the purchase of food divided by the number of consumption units in the household. The number of consumption units was calculated using the modified equivalent scale (1.0 consumption unit for the first adult in the household, 0.5 for other household members aged 14 or older, and 0.3 for each child aged less than 14 years old) of the Organization for Economic Co-operation and Development.
Univariate and multivariate analysis
Household sociodemographic profile (independent variables) associated with moderate or severe hunger (dependent variable) were studied using univariate binary logistic regression models (crude odds ratios) and multivariate binary logistic regression models (adjusted odds ratios). The dependent variable could take 2 possible values: low or no hunger defined by a HHS less than 2 (coded as 0 in the models) and severe or moderate hunger defined by a HHS greater than or equal to 4 (coded as 1 in the models). 19 To fit the multivariate model, sociodemographic characteristics were selected when univariate Wald test P values were < .20. The independent variables with more than 10% of nonresponses were not included in the multivariable model. The best logistic model was selected with Akaike’s information criterion, Bayesian information criterion, and area under receiver operating characteristic (ROC) curve. The absence of interaction between the variables of the final model and the Hosmer-Lemeshow χ2 were checked. All tests were 2-sided and a P value < .05 was considered statistically significant. Analyses were carried out using STATA 16.
Results
A total of 277 interviews were conducted (184 in the Central Coast priority areas and 93 in the West Coast priority areas), representing 277 households with a total of 1221 members (642 adults and 579 children). The main languages of interviews were Haitian Creole (65.0%), French (23.1%), and Nengue or Maroon languages (7.2%). The nurses identified 70 children living in the participating households (53 in the Central Coast priority areas and 17 in the West Coast priority areas).
Household Profile
Of the 277 households surveyed, the majority (66.4%) resided on the central coast; one-third were large households of more than 5 people; 1 in 5 households had at least 1 pregnant or nursing mother and 20.2% of households had at least 1 child aged under 1 year. The majority of households (58.5%) traveled on foot or by public transportation, and the majority (62.3%) were adult foreigners without residence permits (Table 1).
Sociodemographic Characteristics, Financial Resources and Housing Characteristics of Participating Households Living in Vulnerable Urban Areas of French Guiana During the COVID-19 Pandemic in February 2021 (InaCov Study, n = 277).
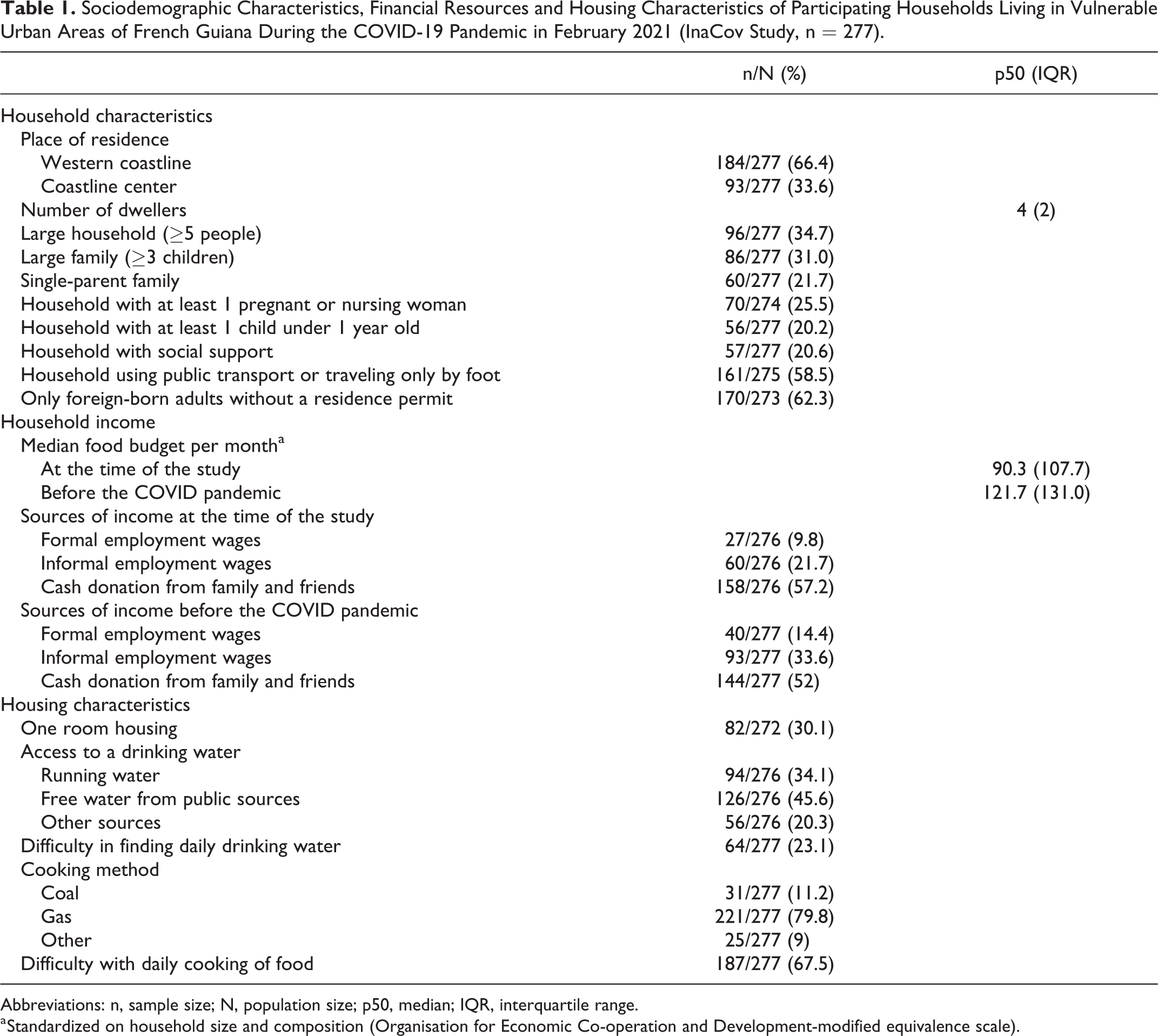
Abbreviations: n, sample size; N, population size; p50, median; IQR, interquartile range.
a Standardized on household size and composition (Organisation for Economic Co-operation and Development-modified equivalence scale).
Regarding household financial resources, the median food budget per month (standardized on household size and composition) at the time of the study and before the COVID pandemic were significantly different (90.3 vs 121.7; Wilcoxon signed-rank test P values < .000). The main source of household income was cash donations from family and friends (Table 1). In terms of housing characteristics, few households had tap water (34.1% vs 85% for French Guiana as a whole) and the majority (79.8%) used gas for cooking (Table 1).
Household Food Security
On the day before the interview, 42.2% of households with adults and 27.1% of households with children had eaten 1 meal or less. During the month preceding the survey, a quarter of households (25.6%) had requested food aid.
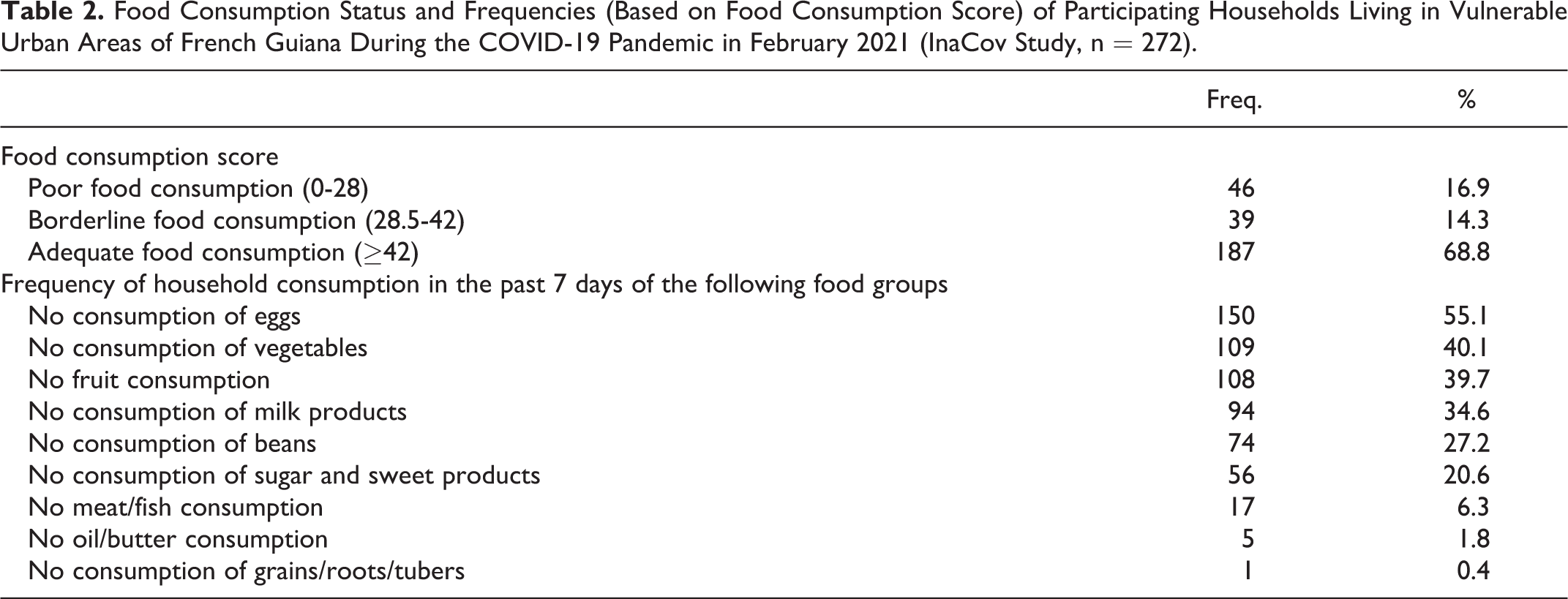
Household food consumption was inadequate and insufficient (poor and borderline food consumption) for 31.2% of the study households. Of the 277 households surveyed, 39.7% and 40.1% had not consumed any fruit or vegetables, respectively, in the 7 days preceding the survey (Table 2).
Food Consumption Status and Frequencies (Based on Food Consumption Score) of Participating Households Living in Vulnerable Urban Areas of French Guiana During the COVID-19 Pandemic in February 2021 (InaCov Study, n = 272).
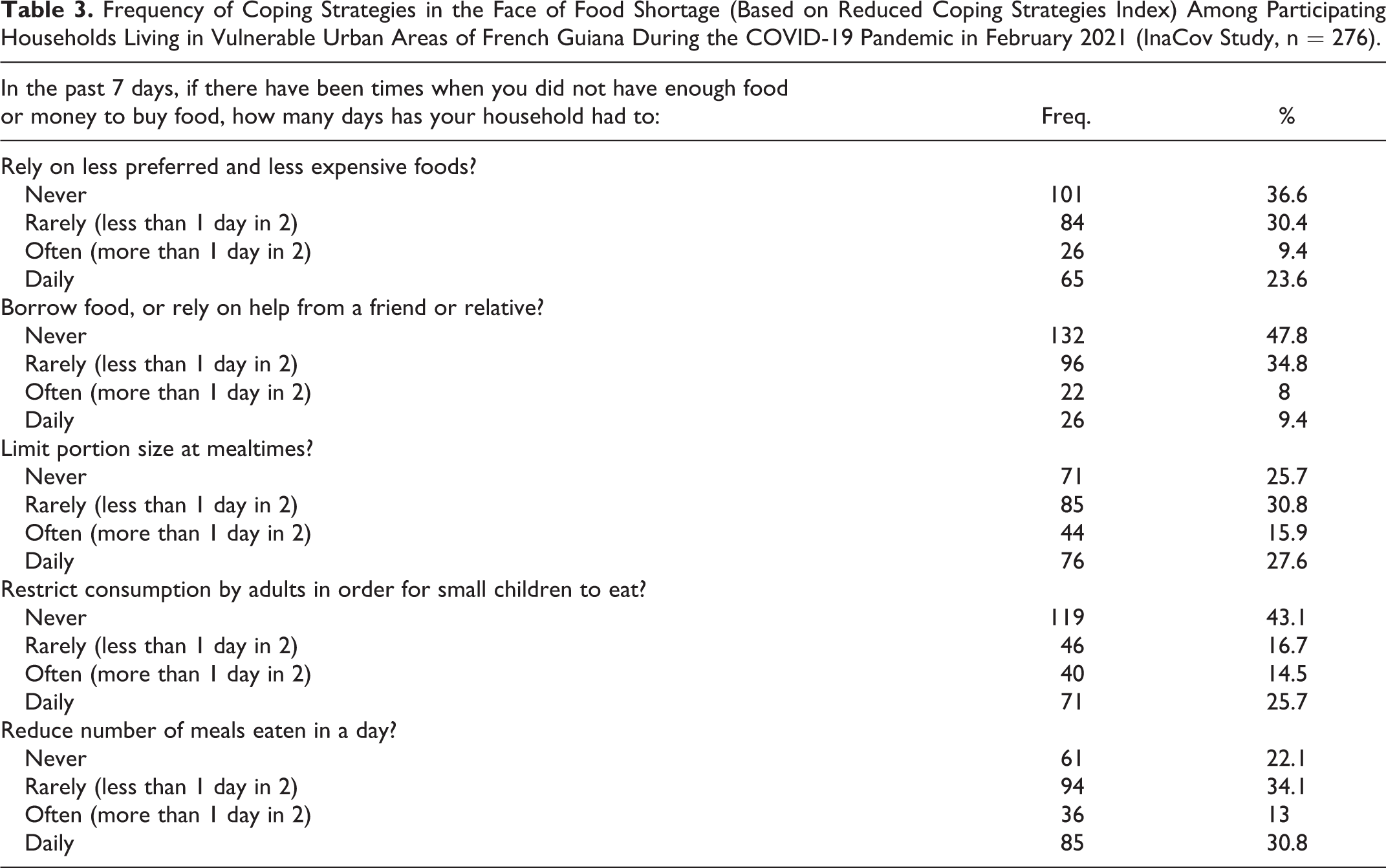
With respect to coping strategies in the face of food shortages (Table 3), the most common strategies at the time of the study were reducing the number of meals per day (77.9% of households having used it at least 1 day in the past 7 days) and limiting portion sizes at meals (74.3% of households having used it at least 1 day in the past 7 days).
Frequency of Coping Strategies in the Face of Food Shortage (Based on Reduced Coping Strategies Index) Among Participating Households Living in Vulnerable Urban Areas of French Guiana During the COVID-19 Pandemic in February 2021 (InaCov Study, n = 276).
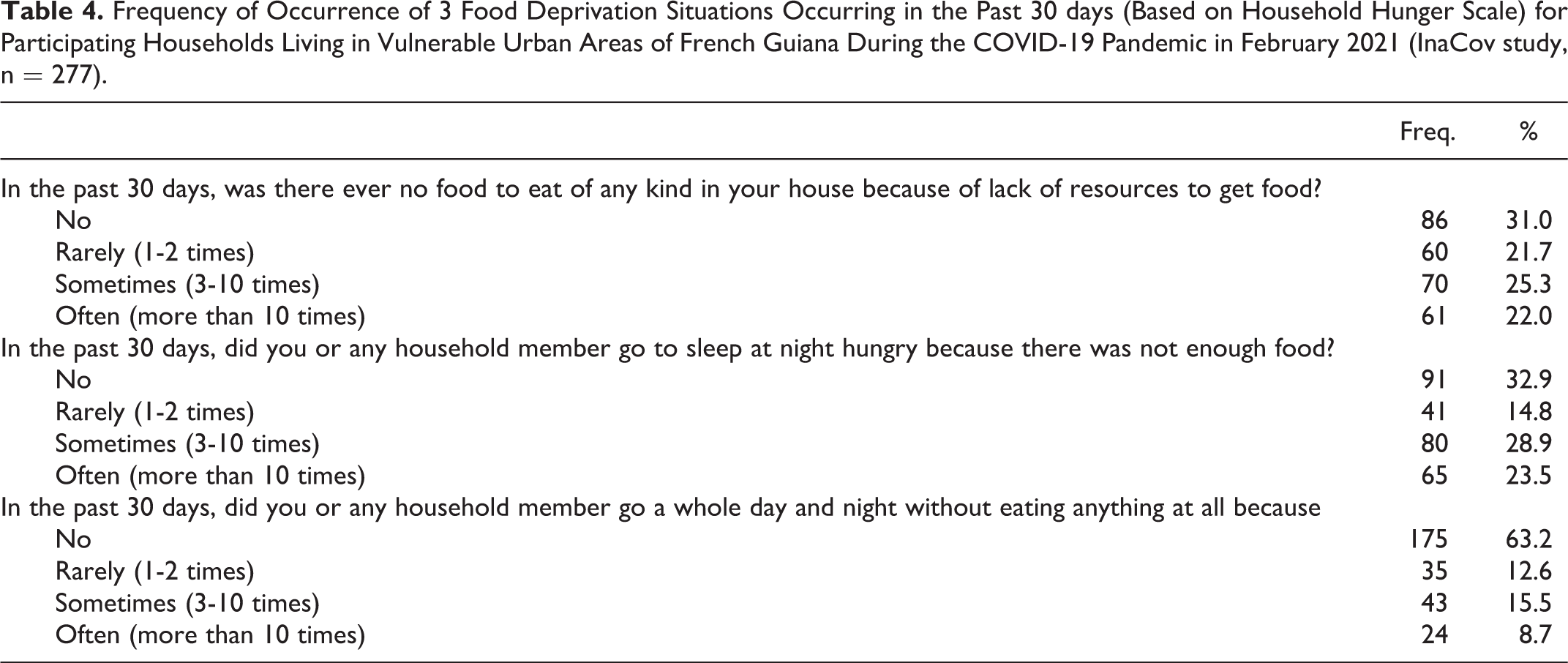
According to the household hunger scale, 23.8% of households had experienced severe hunger, 42.6% moderate hunger, and 33.6% little or no hunger in the month prior to the study. More than 1 in 3 households (36.8%) had gone at least 1 full day and night without food in the past 30 days (Table 4).
Frequency of Occurrence of 3 Food Deprivation Situations Occurring in the Past 30 days (Based on Household Hunger Scale) for Participating Households Living in Vulnerable Urban Areas of French Guiana During the COVID-19 Pandemic in February 2021 (InaCov study, n = 277).
Nutritional Status of Children Under 5 Years of Age
Among the 70 participating children, 61.4% were at least 24 months of age. The majority of children had been breastfed (82.9%). Half of them had been exclusively breastfed for the first 4 or 6 months of life. In 60.6% of cases, children had abnormal weight for height and age. In this study, 5 children (7.5%) suffered from wasting (95% CI: 2.5%-16.8%). There was no pre-COVID-19 data for comparison.
Sociodemographic Profile of Households With Moderate to Severe Hunger
Table 5 presents crude and adjusted logistic regression models of sociodemographic factors within the household experiencing moderate to severe hunger within the past month. After adjustment, households that were highly affected by hunger had a significantly higher probability of living in a single room dwelling, in a house without running water, were composed of immigrants without a residence permit, had no social support, and had no access to an urban garden.
Crude and Adjusted Logistic Regression Model of Sociodemographic Factors Associated With the Household Experience of Moderate to Severe Hunger Within Month, During the COVID-19 Pandemic in Vulnerable Urban Areas of French Guiana (InaCov Study, February 2021).
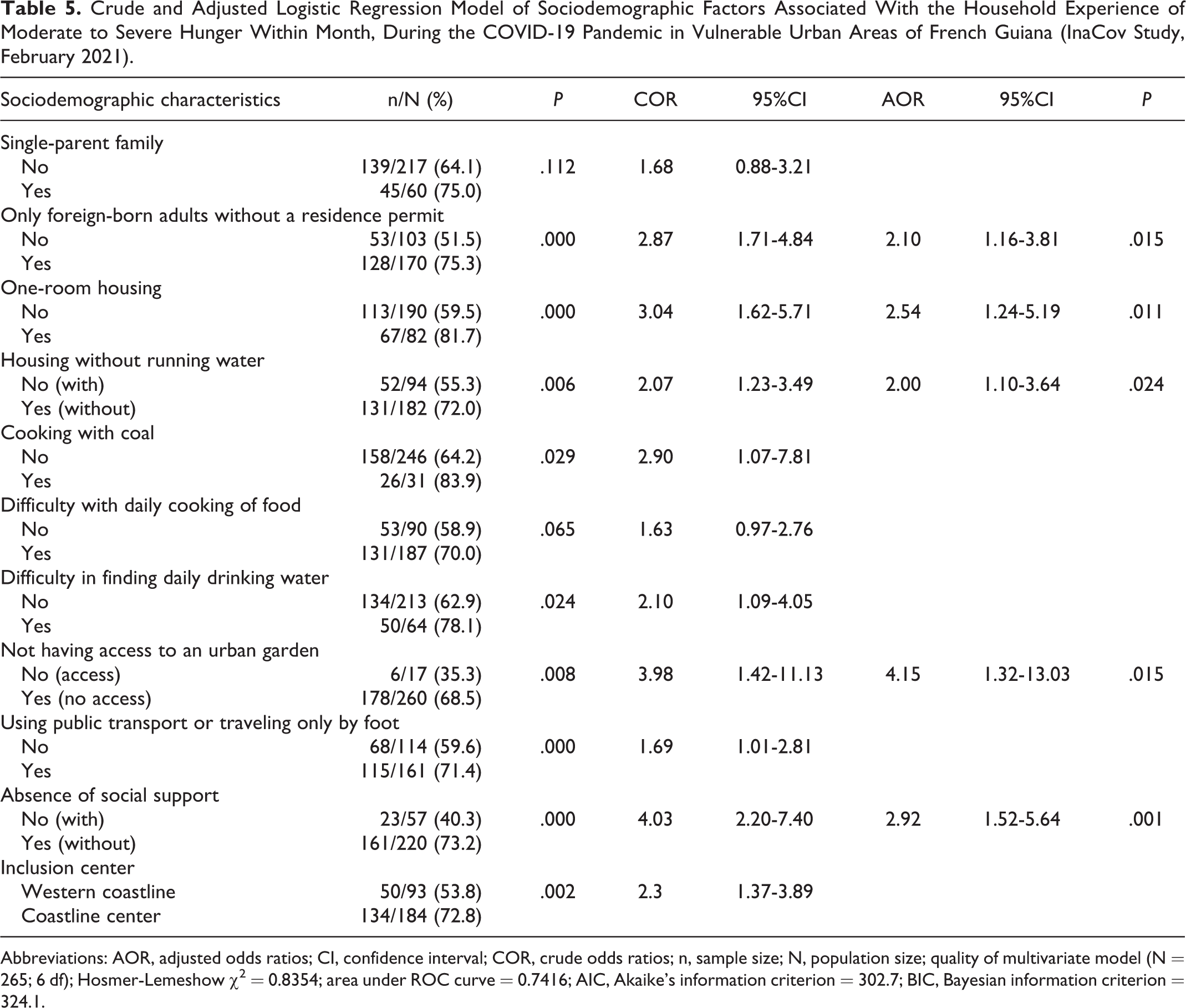
Abbreviations: AOR, adjusted odds ratios; CI, confidence interval; COR, crude odds ratios; n, sample size; N, population size; quality of multivariate model (N = 265; 6 df); Hosmer-Lemeshow χ2 = 0.8354; area under ROC curve = 0.7416; AIC, Akaike’s information criterion = 302.7; BIC, Bayesian information criterion = 324.1.
Household composition, household food budget, children’s enrollment, and time since arrival in French Guiana were not significantly associated with household hunger.
Discussion
With the highest GDP per capita in Latin America, French Guiana represents for many immigrants the hope of a better life and a gateway to Europe. However, once in French Guiana, access to this better life is elusive and subject to many conditions. The survey was conducted in vulnerable urban areas among households with multidimensional precariousness. The level of food insecurity and hunger among these households surveyed during the COVID-19 pandemic was very high (24% severe hunger and 43% moderate hunger). Housing conditions, administrative status, lack of social support, and lack of access to an urban garden were household profiles at higher risk of hunger. In the face of a crisis situation, this study reveals the persistence of pockets of extreme poverty in a rich territory traditionally endowed with extensive social protection.
The majority of adults in this study were foreign-born. In the literature, the rate of food insecurity among immigrants (between 40% and 71%) was higher than in the general population. 21 With the COVID-19 crisis, the loss of informal jobs and the suspension of administrative services resulted in loss of income without Safety Nets for those awaiting status regularization. 22,23
Compounding the problem, water insecurity was significantly associated with household food insecurity. 24 Lack of clean water can limit food choices or cooking methods 25 and make food unsafe. 26 In the surveyed neighborhoods households without safe tap water were forced to walk to public water sources. Fecal contamination of food may be due to food preparation practices, especially when water is scarce, with a higher incidence of diarrhea and malnutrition among children. 26
In French Guiana, housing is the number one expense of households, representing 19.2% of their budget. 27 Families often have difficulties accessing suitable housing in terms of space or comfort for financial reasons (expensive rent or noncreditworthy household). Moreover, household overcrowding plays an independent role in predicting COVID-19 mortality. 28
Developing urban agriculture in these priority neighborhoods may be a useful strategy for improving household food availability. 29 Indeed, it allows easy access to fresh food rich in vitamins and micronutrients (fruits, vegetables, roots…) and thus improves the quality and diversity of household diet. In this study, nearly one-third of households had inadequate energy intake and 7.5% of children measured by the nurse were emaciated. The latter result is based on a small sample and there was no pre-COVID-19 estimate, so caution should be exercised in its interpretation. Nevertheless, this observation is of concern. The nutritional consequences of poor and undiversified diets in children can compromise their physical, cognitive, and socioemotional well-being and affect their school performance. 30,31
Finally, the use of social support may be part of a coping strategy for hunger stress at the household, neighborhood, or community level. 32,33 The restrictive measures during the COVID-19 pandemic have limited these social network based strategies by isolating individuals and by displacing vulnerable populations further out on the margins of society. 32 The focus on the vital and concrete aspect of food, while essential, should not obscure the subjective dimension of these populations—socially isolated, hungry, and fearful of deportation and disease—and the mental health issues associated with exacerbating these stressors that affect the core of their lives. 34
This study has some limitations. The results focused on households attending mobile clinics and continuing care hospitals and may not be extrapolated to all households in urban slums in French Guiana. In addition, due to the lack of prior data, it is not possible to know whether food insecurity was acute or chronic.
In conclusion, it would be an illusion to think that the COVID-19 pandemic affected every population in similar ways. Since the present survey, systematic reviews have confirmed the impact of COVID-19 on food security both in low- and middle-income countries, and on high-income countries. 35,36 In French Guiana, migrant populations in vulnerable urban neighborhoods did not perceive the pandemic as a health crisis but as a social crisis. 37,38 The present study conducted in a relatively rich French territory showed a high level of food insecurity in the urban informal areas close to that of low-income countries. 1 Access to a varied and adapted diet corresponds to basic needs that condition immediate and future well-being. Fighting against food insecurity of at-risk populations must go beyond simple nutritional education. In practice, the present study lends support for targeted interventions such as the creation of urban gardens, improved housing equipment, and comfort and initiatives increasing social links in the priority urban areas of French Guiana’s coastline.
Footnotes
Authors’ Note
CB, OD, FH, LO, AVM, MS, and MN contributed to study design, data analysis, and/or writing the manuscript. COM, AM, AG, AT, LC, CB, PMC, VD, and LT contributed to data collection or to conception. AA and MN supervised this research. All authors have drafted, read, and approved the manuscript. The InaCov project was approved by the National Regulatory authority CNIL (PIA of 12/17/2020, CNIL receipt number 2215826, and registered in the Health Data Hub [number F20210108145245]). All participants were given individual and written information about the study and gave their nonobjection to participate, as required by French Law.
Acknowledgments
We thank the households that participated in this study. We acknowledge the partners who worked to make the study possible. Special thank to Camille Agostini, Néia Barbosa da Silva, Théo Blaise, Noémie Bleher, Clarisse da Silva, Marie Cornouiller, Olivier Pedro Desruisseau, Henry Joseph, Hélène Hilderal, François Lair, Catherine Oliviero, Olivier Morel, Etiennise Tooy, Benoit Renollet, Félicien Salvi, Myrna Sansouci, and Anne Viaud. This work was supported by Regional Health Agency and Prefecture of French Guiana. The funding agencies had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study received public funding from Regional Health Agency (Order n°FIR/ARS/2020/91 of December 21, 2020) and the Prefecture of French Guiana (Order n°168/DGCP/PSPI of November 27, 2020).