
Abstract
There have been successful interventions fortifying staple foods to mobilize micronutrients as well as agricultural efforts to raise yields of staple foods to increase food availability. Zambia serves as an interesting case study because since 1961 there has been a notable decline in the availability of animal source foods (ASFs) and pulses and a significant increase in the supply of cassava and vegetable oils. The shift in food availability was partly attributed to the agricultural success in high-yielding and drought-resistant varieties that made cassava and oil crops more affordable and readily available. In this research, we explore another policy strategy that involves ASF as a mechanism to help remedy micronutrient inadequacies in a population. A scenario modeling analysis compares the changes in the nutrient profile of the Zambian diet through adding either staple plant source foods (PSFs) or ASFs. The scenarios under study involve the addition of (1) 18 fl oz of whole cow’s milk; (2) 60 g of beef, 30 g of chicken, and 5 g of beef liver; (3) milk plus meat; or (4) 83 g of maize flour, 123 g of cassava, and other staple PSF, that is, isocaloric to the “milk + meat” group. The findings alert program planners and policy makers to the value of increasing the availability, accessibility, and utilization of ASF to simultaneously address multiple nutrient deficiencies, as well as the nutrition challenges that remain when expanding the availability of plant-based staples.
Keywords
Introduction
Over the past 3 decades, production and consumption of cassava in Zambia have dramatically increased, 1 so have the supply and demand for edible oils. 2 On the other hand, concomitantly, the supply for human consumption of cereals, pulses, and foods of animal origin has declined. 3 Such a marked shift in the consumption pattern may be of concern from a nutritional point of view.
Designing an effective nutrition program requires a good understanding of the dietary profile and nutrition status of the target population. Unfortunately, national food consumption data at the individual level are seldom collected in low-income countries. 4 In Zambia, no nationwide food consumption and nutrition survey has been conducted since the national nutrition survey of 1970 to 1971 by Food and Agricultural Organization (FAO) Zambia, 3 nor have micronutrient deficiencies of the general population been extensively measured and updated for the past several decades. Although a recent study attempted to use the Zambian 2006 Living Conditions Monitoring Survey (LCMS) to fill this gap, this survey was not designed to measure micronutrient deficiencies (Note 1). 5,6 Existing evidence suggests that Zambians have multiple micronutrient deficiencies of iodine, iron, zinc, vitamin A, and vitamin B12, especially among children and women. 3,6,7 The prevalence of stunting, anemia, and deficiencies of iodine and subclinical vitamin A in Zambia is still high and persistent. 8 The national dietary energy supply (DES), though fulfilling over 75% of the population energy requirement estimated by FAO, is still insufficient. 3 The share of energy from protein (10%) is at the lower limit of the World Health Organization (WHO) recommendation (10%-15%). 9 This is consistent with the national statistics that 40% of Zambian children under the age of 5 are stunted and 6% are wasted, whereas 15% are underweight. 10
Biofortification and supplementation have traditionally been the key intervention strategies for controlling these micronutrient deficiencies resulting from inadequate intake among food insecure populations. 3,11 Salt has been iodized in Zambia since the 1970s. Significant progress has been reported toward the elimination of iodine deficiency, with the percentage of school children with low urinary iodine levels (<100 μg/L) considerably reduced from 72% in 1993 to 4% in 2002. 3
Margarine and sugar have been fortified with vitamin A since 1978 and 1998, respectively, whereas the vitamin A supplementation program for children and mothers also started in 1998. A follow-on study showed marked reduction in vitamin A deficiency due to direct supplementation and sugar fortification. 12 But subclinical vitamin A deficiency remains a severe public health problem, especially among young children, even though the prevalence of low serum retinol concentration (<0.70 μmol/L) declined from 66% in 1997 to 54% in 2003 among preschool children and 22% to 13% among women of childbearing age. 3 The issue of vitamin A deficiency remains an important policy objective as just recently HarvestPlus announced the release of vitamin A maize for the country. 13
In Zambia, antenatal supplementation of iron/folic acid has been provided by all health facilities. In 2013 to 14, over 90% of pregnant women were supplemented with iron, although only 59% took them for more than 90 days. 10 Between 1998 and 2003, the prevalence of anemia (hemoglobin concentration <11.0 g/dL) decreased from 65% to 53% in preschool children and 39% to 29% in nonpregnant women. 14 Despite this reduction, the prevalence of iron deficiency anemia remains high in Zambia. Data on the intake of other micronutrients in Zambia are less readily available. The estimated average intake of vitamin A, iron, and zinc in Zambia is highly inadequate, according to the study using Zambia’s 2006 LCMS data. 15 Adjusting for bioavailability, 87.2%, 73.1%, and 92.8% of the Zambian’s intake of vitamin A, iron, and zinc, respectively, fell below the estimated average requirements (EARs). A 2013 food consumption survey was carried out to assess the micronutrient intake of vitamin A, iron, zinc, and vitamin B12 among women and children in 2 provinces in Zambia. 16 Results showed that 15% and 87% of children under 5 were deficient in zinc and vitamin B12, respectively. For women, 95% were vitamin B12 deficient.
These studies suggest that despite efforts in mandatory biofortification and supplementation, there has been limited success in reducing the burden of vitamin A, B12, iron, and zinc deficiencies. Although short-term interventions such as supplementation and food fortification still need to be reinforced, the research in this article explores how food-based strategies might effectively combat micronutrient deficiencies in Zambia.
Given that multiple rather than single micronutrient deficiencies are present, food-based dietary diversification approaches are believed to be more sustainable and culturally acceptable than is supplementation or fortification in alleviating malnutrition under conditions of food insecurity. 17,18 Increasing evidence suggests that promoting livestock production in food-insecure communities may effectively and sustainably diversify and improve dietary quality, nutrient status, and overall health. 19 -24 A positive association has been observed between consumption of animal source foods (ASFs) and dietary quality, micronutrient intake, and health of the poor. 25 -31 Livestock intervention can directly increase animal production, which provides more animal products for household consumption. 32 -34 Indirectly, income from animal product sales can also be used to purchase an even wider variety of nutritious food, as well as more or better quality healthcare services or other household products. 35 -37 Milk consumption among dairy cow producers and neighbors, and meat intake among goat producers, increases as do household incomes through the sale of animal products. 38 Similar results were found in Rwanda where dairy cow raising significantly increased milk consumption, dietary diversity score, and child nutritional outcomes. 39 Evidence from randomized controlled trials and quasi-experiments show that direct ASF supplementation is effective not only in improving diet quality 40 and nutritional status 41 -44 but also in promoting various health outcomes including growth, 26,45 -50 cognitive function, 27,51,52 physical activity, 53 and school performance, 54,55 as well as reducing morbidity and mortality 56,57 of children in developing countries.
Compared to plant source foods (PSFs), ASF is regarded to have higher nutritional value. 58,59 Animal source foods are not only a nutritionally dense source of energy and readily digested protein but are also a compact and efficient source of an array of bioavailable micronutrients that are difficult to obtain in adequate quantities from foods of plant origin alone. 58,60 These micronutrients include iron, zinc, calcium, retinol (preformed vitamin A), vitamin B12, riboflavin, and folic acid, which are of the greatest concern worldwide when addressing malnutrition associated with food insecurity. Proteins from animal products generally more closely match the amino acid requirements of humans than do PSFs and tend to have 20% to 30% higher digestibility and thus are easier to absorb and be utilized by the body. 61 Also, many minerals and vitamins, especially lipid-soluble vitamins, are provided primarily by foods of animal origin. Animal source foods are the almost exclusive dietary sources of dietary vitamin B12, 62 highly bioavailable iron, 63 and preformed vitamin A. 64 The zinc content of beef is more than twice that of maize and beans, and it is up to 10 times as absorbable. 65 When consumed with foods of plant origin, ASF can enhance the absorption of minerals and vitamins in plant foods, such as nonheme iron and zinc. 66 An animal-based diet simultaneously provides multiple nutrients without the risk of antagonistic interactions or nutrient overload, which can be more effective than single-nutrient supplements in alleviating poor micronutrient status. 67 Therefore, increasing ASF intake has the potential to significantly improve the overall nutrition status of the vulnerable populations in Zambia and other developing countries having multiple micronutrient malnutrition associated with food insecurity.
In sum, because food-based dietary diversification approaches may more effectively address multiple micronutrient deficiencies, and there exists evidence supporting the link between ASF and micronutrient intake, the objectives of this study are to (1) track the dietary transition and assess the current food consumption pattern in Zambia relative to recommendations for a healthy life; (2) evaluate the macronutrient and micronutrient profile of the current Zambian diet in order to identify the key nutrients likely to be inadequate in the diet of the Zambian population; and (3) estimate the nutritional improvements through interventions with moderate amounts of ASFs.
Methods
To accomplish our objectives, we adopt an approach based on nutrient density profiles derived from the FAO Food Balance Sheet (FBS) data because nationwide food consumption data at the individual level are not readily available. 68 We use scenario modeling analysis to explore the impact of moderate increases in ASF on average energy, protein, and micronutrient intake in Zambia.
The FAO FBS annually contains estimates, with regular updates, of national food supplies for 95 food commodities across more than 170 countries worldwide. It has been widely used for monitoring global, regional, and country-specific food consumption patterns and trends of nutrition status. The formal and universally accepted data collection methods, comprehensive country panel, and long historical span allow for cross-country comparisons and time series analyses of foods available for human consumption and the nutrient status given a diet based on all these foods. 69 The data though represent aggregate per capita availability of food for human and not actual consumption. Thus, we recognize that the use of these data does involve quality tradeoffs in terms of the level of data aggregation but are valid for a nutritional study such as ours. 70 In the remainder of this article, the terms “food consumption” or “food intake” should be read as “food available for consumption.”
Our study compiles data on the estimated average amount of various food items available for Zambian consumption using the FAO FBS covering the period 1961 to 2013. Per capita daily supply of ASF for Zambian consumption was also compared to those for United States, China, and the Mediterranean countries. The baseline food consumption pattern was based on data for the years 2005 to 2007.
All single food items were further classified into one of the 5 main food groups (grains, lean meat and beans, milk, vegetables, and fruits) following the 2005 US Dietary Guidelines. We use the US guidelines because Zambia has not yet developed a national food-based dietary guideline. Quantity of food available for per capita consumption was then referenced to the dietary guideline. The recommended daily amounts needed for each food group are 8 oz equivalent of grains, 6.5 oz equivalent of lean meat and beans, 3 cups of milk, 3 cups of vegetables, and 2 cups of fruit.
The nutrient profiles for the foods available for Zambian consumption were calculated using the WorldFood Dietary Assessment System, version 2. 71 This program was developed primarily for dietary research projects in developing countries. The database contains a list of over 1800 foods reported from 6 countries, including 2 African countries, Kenya and Senegal. A unique feature of the software is the calculation of an individual’s probability of deficiency for each nutrient based on the estimated distribution of the nutrient requirements. The probabilistic approach, as opposed to statements as to discrete recommended intake levels, is regarded to be superior for dietary comparisons.
Additionally, the WorldFood Dietary Assessment System also estimates bioavailable nutrient content by taking into account protein bioavailability (amino acid scores); dietary fiber intake; iron (ascorbic acid); meat–fish–poultry protein intake; tannin-containing coffee or tea intake; and bio-available zinc (phytate, calcium, and animal protein intake).
Food interactions within the same meal also affect nutrient bioavailability. But FBS data reflect the aggregate national daily food supply, thus limits separate meal data analysis. Therefore, the analysis reflected in this research assumes that all the foods are consumed in the same meal.
Bioavailable iron at the level of preventing anemia, as measured by clinically detectable signs, was calculated as well. For vitamin A and zinc, 2 levels of availability were estimated: for persons with basal status, negligible stores but no functional impairment and for those with normative status, maintenance of a reserve adaptive capacity.
For example, Zn-basal is the amount of zinc needed to prevent clinically detectable signs of functional impairment. Zn-normative is the amount of zinc needed for the prevention of functional impairment and also for the generation and maintenance of a reserve storage of the nutrient. The concept of zinc for basal and normative status is still accepted according to the most recent update by the FAO/WHO/International Atomic Energy Agency (IAEA) committee (2004). The International Zinc Nutrition Consultative Group (IZiNCG), in their first technical document, compares the estimated physiologic requirements for absorbed/available zinc developed by 3 expert committees: the FAO/WHO/IAEA, the US Food and Nutrition Board/Institute of Medicine (FNB/IOM), and IZiNCG. 72 The WorldFood Dietary Assessment System we use in this research uses estimates of zinc by the FAO/WHO/IAEA committee (1996). 73 The estimated physiologic requirements for available zinc are relatively higher by IZiNCG compared to the WorldFood program. Similarly, the revised recommended dietary allowance (RDA) for total zinc by IZiNCG is higher than that recommended by the US FNB/IOM. Thus, the FAO/WHO/IAEA are the most conservative estimates among the 3 of the physiologic requirements of available zinc. For detailed information on the definition and calculation of usable protein and all the bioavailable minerals, readers can refer to the user’s guide for the WorldFood 2 Dietary Assessment System program. 73
Following standard practice, we compare Zambian intake for each individual nutrient with the intakes recommended by the IOM’s Dietary Reference Intake reports. We use both the RDA and the EAR for a healthy male 19 to 50 years of age, weighing 79 kg, with moderate physical activity. The EAR is the daily dietary intake level of a nutrient expected to satisfy the needs of 50% of healthy individuals, whereas the RDA considers the level of a nutrient sufficient to meet the requirements of 97.5% of the people. We use the RDA in this study because the recommendation assures a greater percentage of the population will receive adequate nutrition. For parsimony, we report only the RDA results, as they were quite comparable to the EAR results. We also focus our analysis on males 19 to 50 years of age, as a category, because other age and sex groupings generally have higher requirements for nutrients to be considered potentially inadequate. Therefore, our analysis identifies nutrient deficiencies that are applicable to other age and gender groups.
The 4 scenarios, in addition to the baseline, involve intervening with the following: A moderate amount of milk (18 fl oz of whole cow milk). This level reflects a return to the levels of milk consumption per capita found in Zambia in the 1970s. Meat (60 g of beef, 30 g of chicken, and 5 g of beef liver). The addition of this level and diversity of meat, when combined with the milk, meets the estimated energy requirement of 2479 kcal. Milk plus meat. A baseline diet plus extra plant-based staples (123 g of cassava, 83 g of maize flour, 7 g of wheat, 1 g of sweet potato, 1.2 g of sugar, 5 g of palm oil, 0.5 g of sunflower seed oil, and 0.5 g of cottonseed oil). These additions reflect a mix of locally available PSF that when combined with the baseline are isocaloric to the milk plus meat diet.
Results
The main food groups in terms of quantity in grams available for Zambian consumption are cereals and starch roots as staples, followed by alcoholic beverages, fruits and vegetables, and animal products (Table 1). Although the per capita supply of cereals has declined steadily since the 1978 to 1983 period, the supply of starchy roots, which is comprised mainly of cassava, has been increasing. Concomitantly, the availability of pulses and ASF has dropped since the 1970s and remains at a relatively low level. On the other hand, the per capita supply of vegetable oils and oil crops has increased dramatically in recent years. Alcoholic beverages available for Zambian consumption have dramatically declined from 314 g/per capita/day in 1961 to 1965 to 79 g/per capita/day in 2008 to 2013 but still reflect a large component of Zambian national food availability. The total protein supply fell from 67 g/capita/day in 1977 to 45 g/capita/day in 2007, whereas fat supply has grown steadily from 29 g/capita/day in 1991 to 42 g/capita/day in 2013. In fast developing countries such as China, per capita supply of ASF has been dramatically increasing, approaching the level for Mediterranean countries (778 kcal/capita/day) and the United States (995 kcal/capita/day; Figure 1). The per capita supply of total animal products in Zambia though has declined after the mid-1970s, from an already very low level (164 kcal/capita/day).
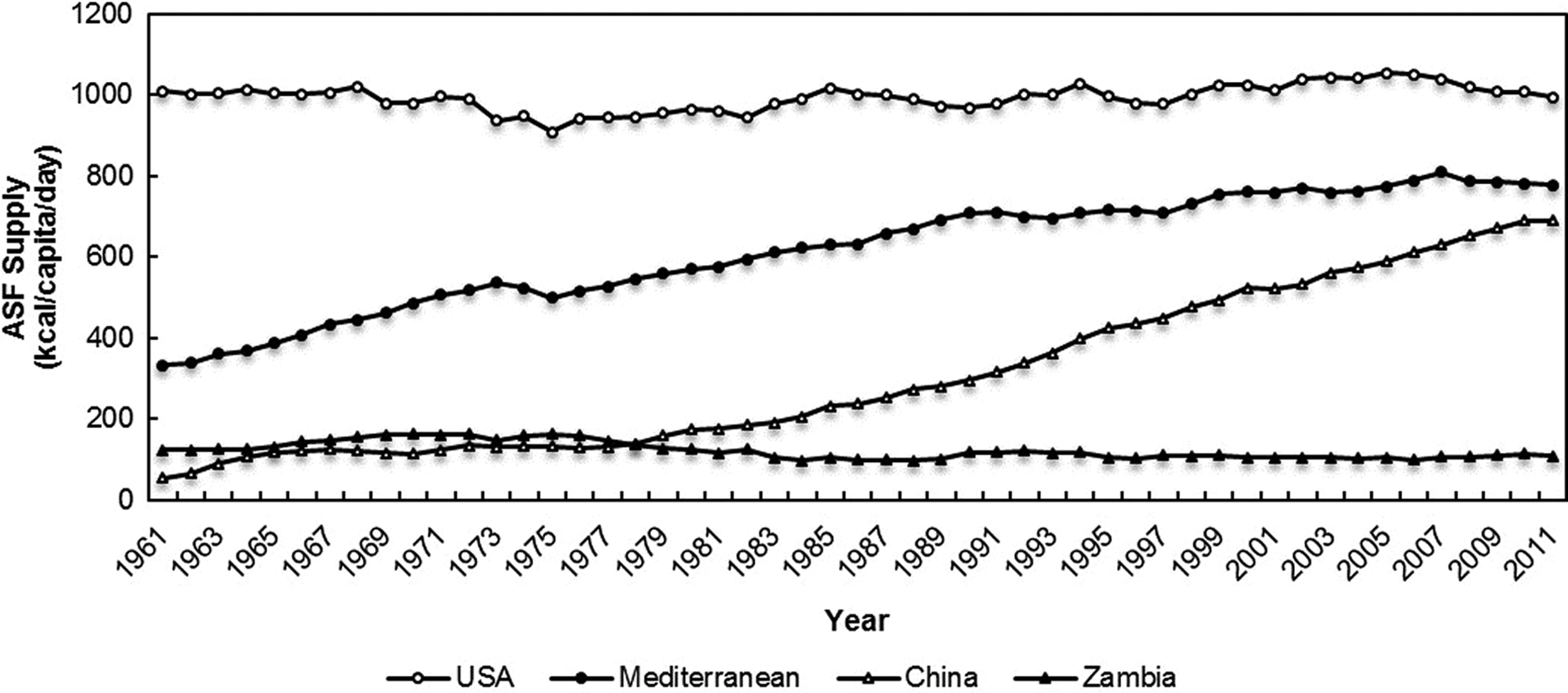
Changes in annual supply of animal source foods (ASF), 1961 to 2011 (kcal/capita/day). Note: The Mediterranean supply is based on the average of Italy, Portugal, Spain, Morocco, Greece, Cyprus, and Croatia.
Trends in Per Capita Supply of Major Food Groups for Zambian Consumption (g/capita/day).
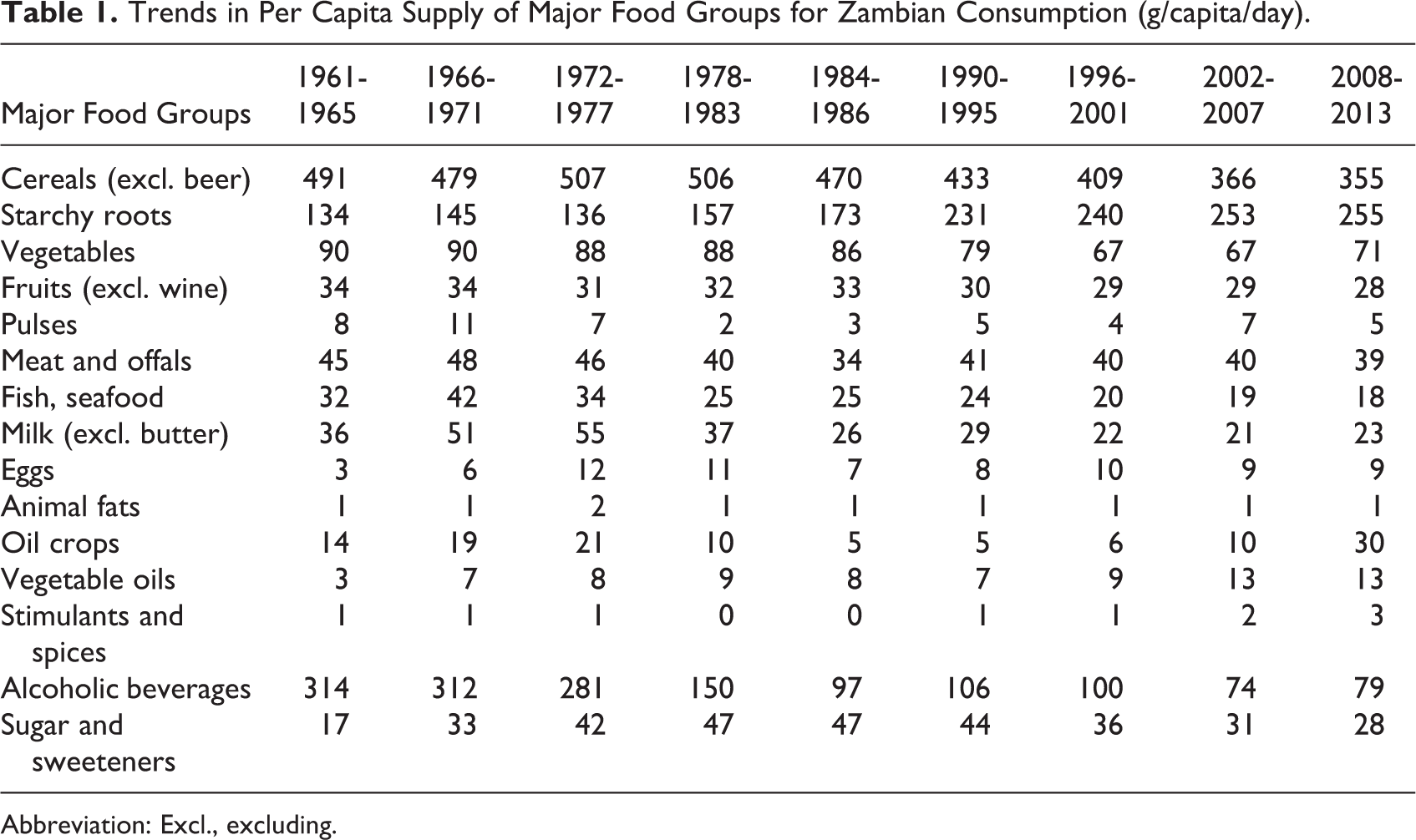
Abbreviation: Excl., excluding.
A baseline diet, based on all the foods available for Zambian consumption in 2005 to 2007 period, is found to be predominantly cereal based, exceeding the recommended daily intake of 8 oz grains by over 100% (Figure 2). It includes little ASF and very few fresh fruits and vegetables. Only 3%, 22%, 5%, and 40% of the recommended daily intake level of 3 cups of milk, 6.5 oz of meat and beans, 2 cups of fruits, and 3 cups of vegetables are met, respectively. The DES in the baseline diet was about 1892 kcal/per capita/day, which was insufficient to meet the population’s average dietary energy requirement (ADER) of 2099 kcal/per capita/day estimated by FAO and the estimated energy requirement (EER) of 2479 kcal per capita/day by the IOM (Table 2). The protein supply of 48.1 g meets 86% of the RDA level, but it is of low quality with only 9.5 g of animal protein and insufficient lysine. Multiple micronutrients were found to be inadequate, including calcium, zinc, and vitamins A, B2, B12, and D. Although the supply of total iron (15 mg) exceeds the RDA, only 0.6 mg of it is bioavailable. People consuming the baseline diet have a relatively high risk of inadequacy for utilizable protein intake (65%) and all forms of vitamins and minerals (Figure 3). The probability of nutrient inadequacy was highest for calcium (100%) and available Zn-normative (100%), followed by available Zn-basal (99%), available iron (99%), vitamin A-normative (98%), vitamin B12 (97%), and available Fe to prevent anemia (81%).
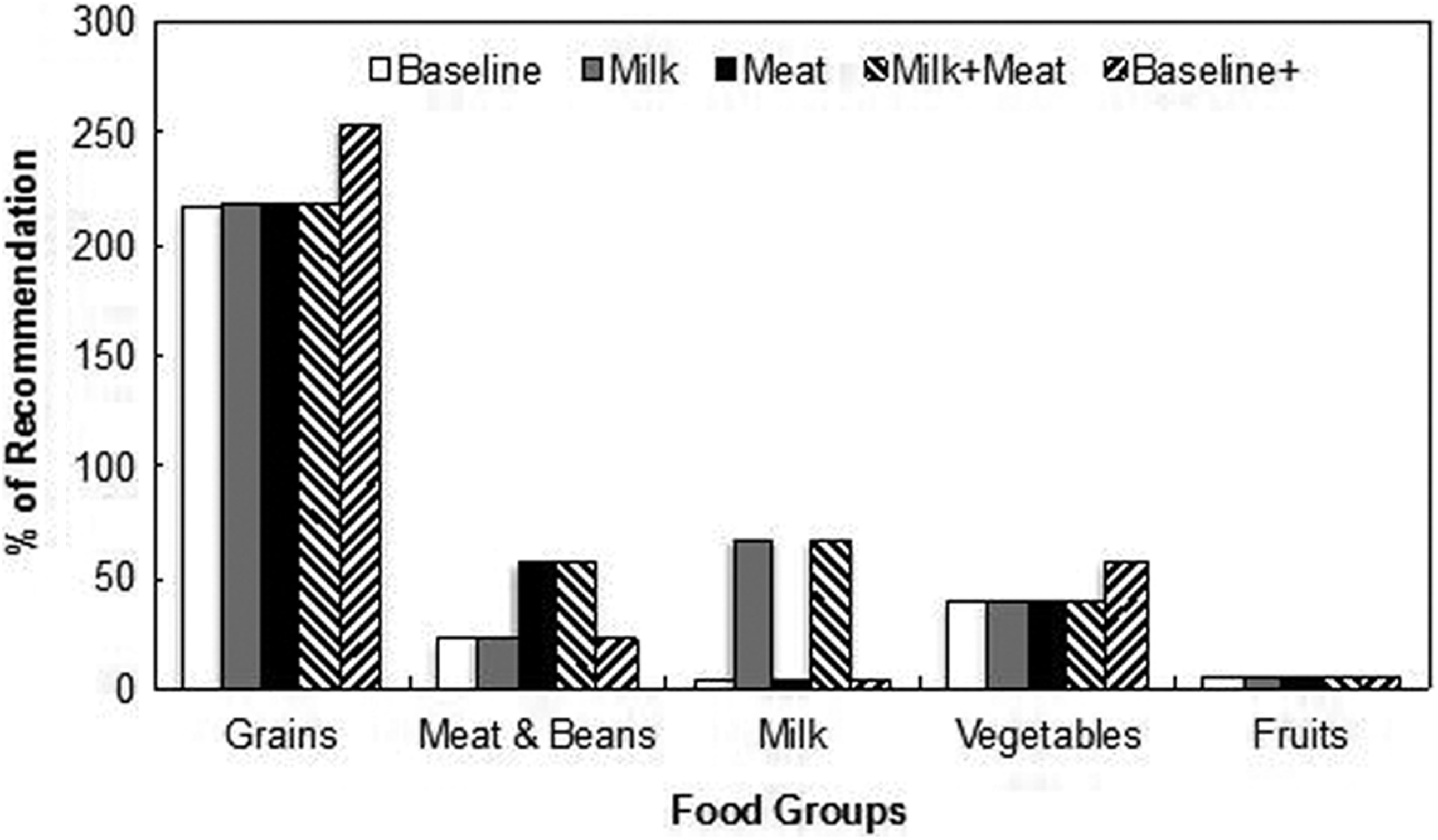
Distribution of food groups in the food supply of Zambia.
Change of Key Nutrient Supplies by Supplementation With ASF as Compared to Adding More PSF.
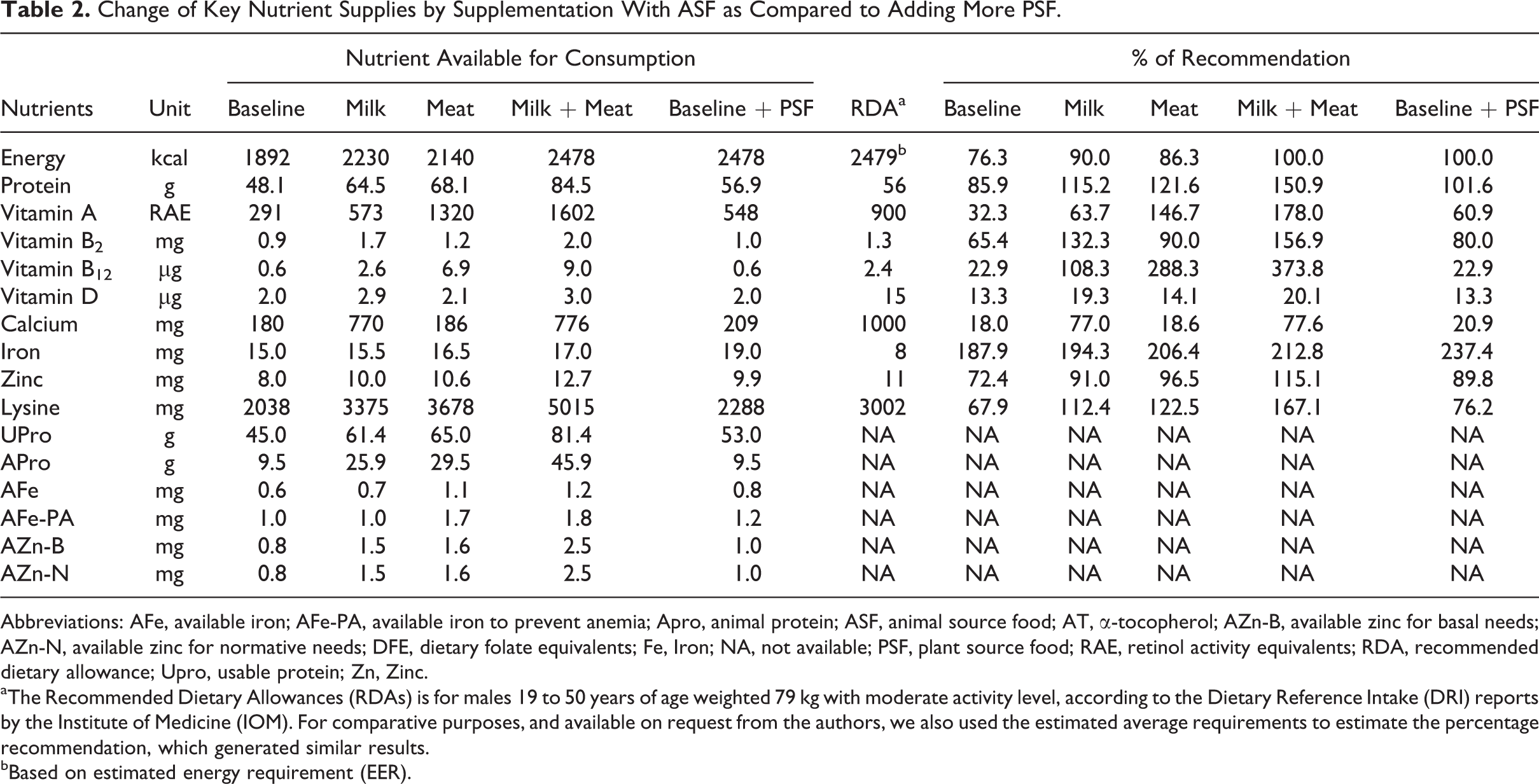
Abbreviations: AFe, available iron; AFe-PA, available iron to prevent anemia; Apro, animal protein; ASF, animal source food; AT, α-tocopherol; AZn-B, available zinc for basal needs; AZn-N, available zinc for normative needs; DFE, dietary folate equivalents; Fe, Iron; NA, not available; PSF, plant source food; RAE, retinol activity equivalents; RDA, recommended dietary allowance; Upro, usable protein; Zn, Zinc.
aThe Recommended Dietary Allowances (RDAs) is for males 19 to 50 years of age weighted 79 kg with moderate activity level, according to the Dietary Reference Intake (DRI) reports by the Institute of Medicine (IOM). For comparative purposes, and available on request from the authors, we also used the estimated average requirements to estimate the percentage recommendation, which generated similar results.
bBased on estimated energy requirement (EER).
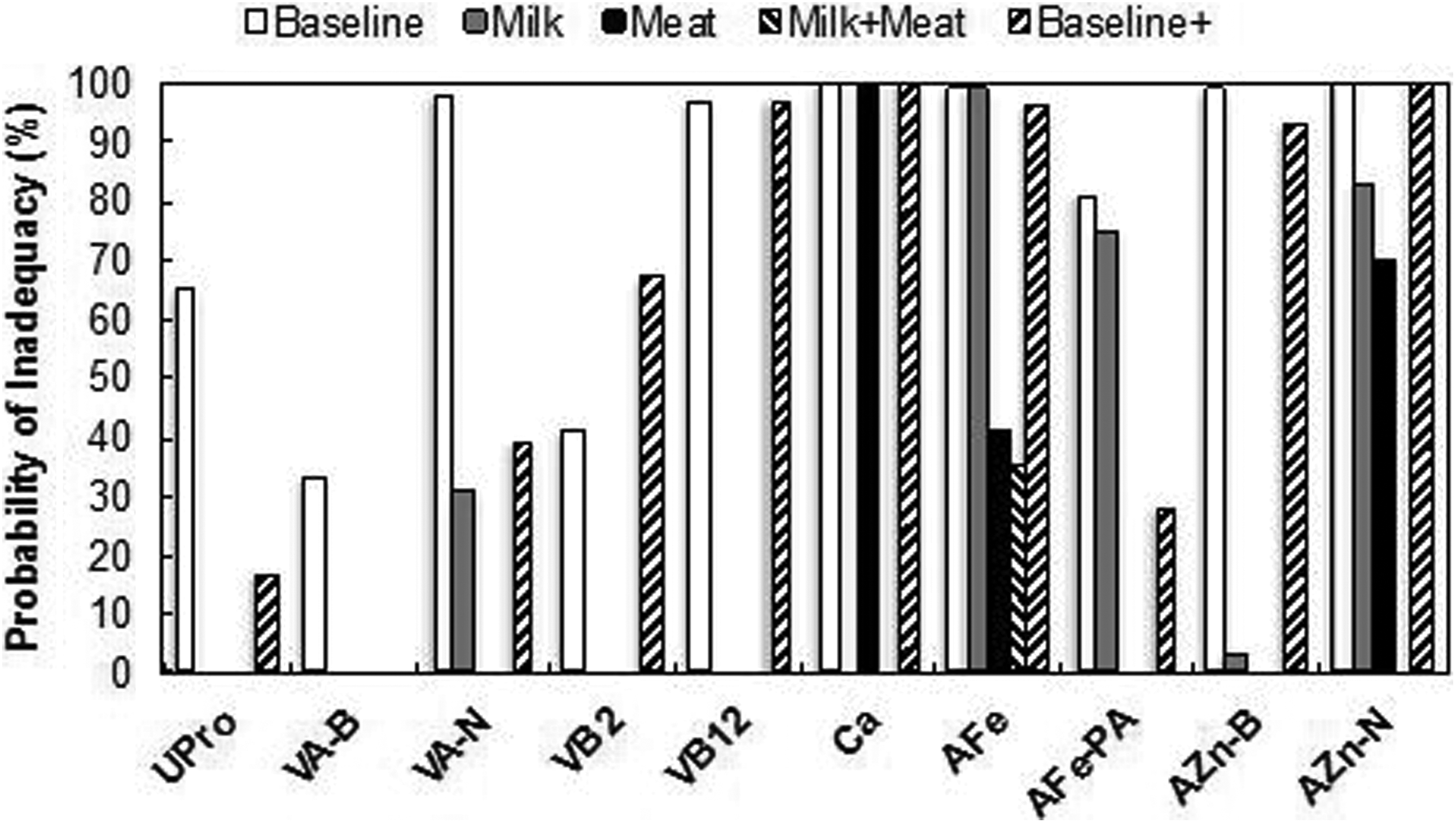
The probability of micronutrient inadequacy under 4 nutrition scenarios. AFe indicates available iron; AFe-PA, available iron to prevent anemia; AZn-B, available zinc for basal needs; AZn-N, available zinc for normative needs; Ca, calcium; Upro indicates utilizable protein; VA-B, vitamin A for basal needs; VA-N, vitamin A for normative needs; VB2, vitamin B2; VB12, vitamin B12.
By adding 18 fl oz of whole cow’s milk to the baseline diet in scenario 1 allows consumers to meet 67% of the recommended quantity of milk and milk products, up from a current level of 3% (Figure 2). We regard this amount of milk (18 fl oz) added as relatively small. There are few other dairy products, such as cheese or yogurt, available for Zambian consumption. All consumed milk-based products together still reach less than 70% of the recommendation, even when adding 18 fl oz of whole cow’s milk to the baseline diet. Under scenario 1, the dietary caloric supply (2230 kcal) becomes sufficient for the population’s ADER and fulfills 90% of the EER (Table 2). Protein supply becomes adequate, satisfying 115% of recommendation. Dietary quality improves by 173%, 36%, and 66% in terms of animal protein, utilizable protein and lysine, respectively. The supply of calcium and vitamin B12 increases more than 3-fold and vitamin A and B2 almost double. Vitamin D, zinc, and iron increase 45%, 26%, and 3%, respectively. Adding 18 fl oz of whole cow milk lowers the probability of inadequacy for all of these nutrients to below 30%, except for available iron and zinc, which remain at 75% (Figure 3). Therefore, adding milk alone is not sufficient for reducing the inadequacy of these 2 key micronutrients.
Similarly, adding 60 g of beef, 30 g of chicken, and 5 g of beef liver to the baseline diet in scenario 2 increases the supply of “meat and beans” group to 56% of the consumption recommendation (Figure 2). The dietary caloric intake (2140 kcal) becomes sufficient for the population’s ADER and fulfills 86% of the EER. Protein supply becomes sufficient, satisfying 122% of the recommendation. Dietary quality also improves, as there is a 210%, 44%, and 80% increase in animal protein, utilizable protein, and lysine, respectively. The supply of vitamin A and vitamin B12 increases more than 3.5-fold and that of vitamin B2 and zinc increases over 33%. Total iron, vitamin D, and calcium increase 10%, 6%, and 3%, respectively. Adding this small amount of meat reduces the risk of inadequacy for available zinc for normative needs by 30% and available iron by 60%. Adding small amounts of meat eliminates the risk of inadequacy for all other nutrients except for calcium, which does not change. Therefore, adding meat alone was not effective in reducing the risk of calcium deficiency.
The addition of both milk and meat in scenario 3 meets 67% and 56%, respectively, of the consumption recommendation (Figure 2). This is in contrast to scenario 4 where PSF additions to the baseline diet meet 255% and 57% of the recommendation for the grains and vegetables groups, respectively. Both scenario 3 and scenario 4 intervention diets have the same dietary caloric intake (2478 kcal) and are adequate for the EER (Table 2). The protein supplies are both sufficient. The diet quality reflected by lysine and utilizable protein levels is elevated to 119% in scenario 3 and only 54% for scenario 4. The “milk + meat” intervention (3) raises all essential nutrients to the RDA levels, except for calcium and vitamin D that meet 78% and 20% of the recommendations, respectively. Note that the RDA value for vitamin D is based on minimal sun exposure. The milk and meat combination eliminates all nutrient inadequacy risk except for a 35% probability of an iron deficiency (Figure 3). The “baseline + PSF” intervention (4) diet maintains all micronutrient levels below RDA levels, except for vitamin A. The PSF-enhanced diet only eliminates the risk of vitamin A inadequacy in basal form and leaves all other nutrients at some risk for inadequacy. These results suggest that adding more plant-based staples to the baseline diet will not be as effective in improving the level of micronutrient sufficiency in the diet as with the addition of ASF.
Discussion
Our analysis of the trend in food supply in Zambia since 1961 highlights a notable decline in the availability of ASF and pulses for Zambian consumption and a significant increase in supply of cassava and vegetable oils. It is consistent with the observed falling supply of total protein since 1977 and the steady increase in the supply of fat in the diet since the 1990s. Zambian food consumption is predominantly cereal based and often includes little or no ASF, with few fresh fruits and vegetables. It is not only insufficient in food quantity but also poor in dietary quality because the supply of utilizable protein, animal protein, and lysine is low. Multiple micronutrients were identified to be highly deficient, including calcium, zinc, available iron, vitamin A, B2, B12, and D. However, a variety of food is needed to provide the many nutrients required to maintain human health. Future food policy needs to balance the costs and benefits of elevating supplies of starchy staples with expanding the supply of nutrient-dense foods, such as ASF. Improving diet diversity and diet quality by promoting the availability, accessibility, and utilization of ASF in Zambia through agricultural, nutrition, and health policy may prove beneficial.
Our scenario modeling analysis shows that interventions involving ASF have a greater potential than PSF to tackle the multiple micronutrient deficiencies present in Zambia. Encouraging additional milk and meat consumption, even marginally, could potentially remove the risk of most nutrient inadequacy.
The present study adapts a method of nutrition assessment based on the FAO FBS data, and these data enabled our understanding of the changes in food consumption patterns and the current nutrition status of the Zambian general population. Results of the present analyses can be used to provide a reference for future development of intervention programs to control micronutrient deficiencies in Zambia and countries in similar situations. The analysis also can inform nutrition, health, and agricultural policy makers as to alternative approaches to achieve improved nutrition outcomes.
Nevertheless, there are a number of limitations that need to be recognized. First, the FBS data measure the amount of all foods available for human consumption at the national level and tend to overestimate the quantities of food actually consumed due to wastage and losses during storage, preparation, and cooking. This means the true micronutrient status in Zambia may be worse than what is estimated in the present study. However, this would not affect our results because if FBS data show that even a diet based on all the foods available for human consumption is insufficient for the nutrient needs, then the actual consumption should be regarded as “not adequate” as well.
Second, the estimated per capita food supply is applicable only at the aggregate national level, and therefore, important differences among geographic, ethnic, and socioeconomic strata remain hidden. It is unlikely, as is the case with the uneven distribution of income, that the average nutrient accessibility, which our study uses, reflects the median or modal levels, nor the state of the population having extreme deficiencies. There are great variations in micronutrient intake across regions, 6 which is consistent with the assumption that nutrient availability and intake are unevenly distributed.
Third, it is important to bear in mind that we only present results comparing to the dietary recommendation level for a healthy male 19 to 50 years of age, weighing 79 kg, with moderate physical activity. This may lead to an overestimation of the true nutrition status in Zambia because this age and gender group generally has lower nutrient requirements. For example, children and pregnant or lactating women often have higher nutritional needs to maintain health. In food-insecure communities where disease incidence is high, dietary requirements are recommended to be elevated over that needed by healthy individuals in order to improve disease resistance and treatment efficacy. 74,75 This is especially important for a country like Zambia with relatively high infection levels of HIV/AIDS, malaria, tuberculosis, and other diseases. Therefore, the nutrient deficiencies identified in the present article may also be applicable to other age and gender groups in Zambia.
In conclusion, Zambia has experienced a substantial increase in the supply of cassava and (more recently) vegetable oils and a corresponding decrease in that of ASF, pulses, and cereals during the past several decades. A diet based on all the foods currently available for Zambian consumption is predominantly cereal based and includes very little ASF and few fresh fruits and vegetables. It is unbalanced, poor in quality, and lacks of dietary diversity. Multiple micronutrient deficiencies were identified, including protein, lysine, calcium, zinc, available iron, vitamin A, B2, B12, and D. Supplementation with small amount of milk and meat dramatically improves the supply of these nutrients and reduces their probability of inadequacy, whereas adding more plant-based foods only marginally changes the nutrient profile. Program planners and policy makers should appreciate the nutritional advantages of increasing ASF intake in Zambia, and other low-income countries, and the potential for nutritional improvements by increasing availability, accessibility, and utilization of ASF. Zambia is also in urgent need to develop its own food-based dietary guidelines to educate its people on how to secure a balanced, diversified, and nutritious diet for better health.
Footnotes
Note
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.