
Abstract
Background:
Little is known about the sustained effects of nutrition- and gender-sensitive agricultural programs (NSAPs) after they end.
Objectives:
To examine the 4-year effects (2010-2014) of a 2-year NSAP (2010-2012) on women’s outcomes in rural Burkina Faso.
Methods:
We used baseline (2010) and endline (2012) data from a cluster-randomized controlled trial of Helen Keller International’s Enhanced Homestead Food Production (EHFP) program and baseline (2014) data from a new program. We included 134 women: 82 who participated in the 2-year EHFP program (treatment) and 52 who did not (control). We examined program (2010-2012), post-program (2012-2014), and overall 4-year effects (2010-2014) using difference-in-difference analysis (DID).
Results:
We found significant positive program effects (2010-2012) on women’s underweight prevalence (DID: 16.44 percentage points [pp]; P = .09) and on women’s knowledge about appropriate age to introduce liquids (DID: 28.40 pp; P = .01). Although there were no significant postprogram effects (2012-2014), differences found in 2012 between the treatment and control group were sustained resulting in an overall 4-year (2010-2014) reduction in women’s underweight prevalence (DID: 18.26 pp; P = .02) and an improvement in women’s knowledge about appropriate age to introduce liquids (DID: 31.29 pp; P = .02). We observed no postprogram or overall 4-year effects on women’s knowledge of child feeding and handwashing practices or women’s empowerment.
Conclusions:
Nutrition- and gender-sensitive agricultural programs demonstrate potential for sustained improvements in women’s nutritional status and nutritional knowledge. Postprogram assessments of NSAPs should be embedded in program evaluations to help further understand the potential of NSAPs to generate sustainable impacts on women’s outcomes.
Keywords
Introduction
There is ample evidence that nutrition- and gender-sensitive agricultural programs (NSAPs) have potential to increase production and consumption of nutrient-rich foods. 1 -5 NSAPs often include a combination of interventions such as agricultural inputs and training, women’s empowerment activities, and health and nutrition behavior change communication (BCC). Through these packages of complementary interventions, NSAPs provide opportunities to improve women and children’s nutritional status by increasing the availability of and access to micronutrient-rich foods; enhancing women’s health, nutrition and hygiene knowledge and practices; and boosting income (managed by women) from the sale of agricultural products. Evidence of the impact of NSAPs on women’s nutritional status is growing, with positive effects documented for dietary diversity, underweight, and anemia. 5 Similarly, NSAPs have been shown to improve women’s knowledge and practices related to child breastfeeding and complementary feeding, health seeking behaviors for prevention and treatment, and hygiene. 5
In addition to improving women’s outcomes during the program implementation period, NSAPs often seek to achieve sustainable, longer term changes that benefit target women and their current and future children. However, little is known about the medium- or long-term postprogram effects of NSAPs on women’s outcomes, with limited evidence coming primarily from Bangladesh. 5 Specifically, one home gardening and nutrition education intervention targeted to poor rural women in Bangladesh showed positive postprogram effects on women’s household decision-making power 3 years after the intervention ended. 6 Another home gardening and nutrition education program targeted to female smallholder farmers in Bangladesh also led to improved women’s nutritional knowledge and empowerment 3 years after it ended. 7 Still in Bangladesh, one study of improved home-gardening technologies delivered to women’s groups found significantly higher body mass index (BMI) among early adopters of improved home-gardening technologies 10 years after the program started. 8 In addition to these studies in Bangladesh, one study in South Africa showed improved knowledge of vitamin A-rich foods 1 year after an horticulture and nutrition education intervention targeted to households with children 1 to 5 years old ended. 9
In this article, we assessed the 2-year postprogram effects (2012-2014) and overall effects (2010-2014) on women’s outcomes of Helen Keller International’s (HKI) Enhanced Homestead Food Production (EHFP) program (a nutrition- and gender-sensitive agriculture program) implemented in Burkina Faso from 2010 to 2012. 10 Previously published findings showed that the 2-year EHFP program successfully reduced women’s underweight prevalence and improved women’s empowerment 11 and knowledge about hygiene and some infant and young child feeding (IYCF) practices. 12 One year after the EHFP program ended, a follow-up study assessed postprogram (2012-2013) and overall (2010-2013) effects on women’s IYCF and hygiene knowledge; however, effects on women’s underweight and empowerment were not examined. 13 Here, we used data from the cluster-randomized controlled trial (cRCT) evaluating the EHFP program (2010-2012) and baseline data (2014) from a new follow-on program to examine the postprogram (2012-2014) and overall 4-year effects (2010-2014) of the EHFP program in a subset of women who participated in both the original EHFP program or evaluation and the follow-on program. Postprogram (2012-2014) and overall 4-year effects (2010-2014) on women’s underweight, empowerment, and IYCF and hygiene knowledge have not been previously examined.
Methods
Program Description
A detailed description of HKI’s EHFP program is available elsewhere. 11,12 Briefly, HKI’s EHFP program was a 2-year NSAP implemented between 2010 and 2012 in 4 departments in the Gourma province in the eastern region of Burkina Faso. The program targeted women with children aged 3 to 12 months and aimed at improving women and children’s nutritional status. It included 2 primary components: agricultural production activities and a health and nutrition BCC strategy. The agricultural production activities consisted of provision of agricultural inputs (seeds, saplings, chickens, and small gardening tools) and training on best practices in homestead food production at village model farms. The village model farms were set-up and managed by 4 female village farm leaders and served as an on-going training and demonstration site throughout the 2-year project period. Targeted women were encouraged to establish their own home gardens and engage in small animal husbandry. The BCC strategy focused on improving health- and nutrition-related knowledge and practices. Targeted women received biweekly home visits delivered by older women leaders (OWL) or health committee (HC) members, where they learned about optimal health and nutrition practices and discussed facilitators and obstacles in adopting the promoted behaviors. The program was also gender-sensitive in that it explicitly targeted women and encouraged them to make independent decisions related to their home gardens and children’s health and nutrition.
In 2014, two years after the EHFP program ended, HKI began the implementation of the “Creating Homestead Agriculture for Nutrition and Gender Equity” (CHANGE) program in the same area as the original EHFP program and targeted women with children <12 months of age. The program was implemented in the same area of Burkina Faso to allow former control villages to benefit from the successful program and to address questions related to the duration of program exposure. The CHANGE program built directly on the lessons learned from the EHFP program evaluation and was designed to optimize the impacts of the EHFP program, to address additional underlying causes of undernutrition, and to test the addition of new nutrition-sensitive and nutrition-specific program components and the benefits of longer term exposure to the program at the village level.
Study Design and Participants
Enhanced Homestead Food Production program
The EHFP program was evaluated using a longitudinal cRCT where 55 villages with access to water during the dry season, stratified by department and village size, were randomly assigned to 1 of 3 groups: (1) control group, with no program activities from HKI (25 control villages), (2) treatment group with EHFP program and BCC strategy implemented by OWLs (15 OWL villages), and (3) treatment group with EHFP program and BCC strategy implemented by HC members (15 HC villages). Within the selected villages, all women with children 3 to 12 months of age at baseline were invited to participate in the study. Women in OWL and HC villages were also invited to participate in the EHFP program. A total of 1767 households and 1882 women participated in the baseline survey conducted between February and May 2010. The endline survey was conducted between February and June 2012.
Creating Homestead Agriculture for Nutrition and Gender Equity program
The CHANGE program was also evaluated using a longitudinal cRCT where 60 villages were randomly assigned to 1 of 4 treatment groups. The 60 villages included the 55 villages which participated in the EHFP program and evaluation, and 5 additional villages that did not participate in either the EHFP program or its evaluation. The baseline survey was conducted between February and May 2014. A total of 2494 households participated in the baseline survey, which corresponded to all eligible households with children <15 months of age who agreed to participate in the study.
Measures
We examined indicators related to women’s knowledge about breastfeeding practices, age of introduction of complementary foods, and key handwashing times. Women’s weight and height were directly assessed by trained fieldworkers. Height was measured using a wooden height board (Shorr Productions), and weight was measured using an electronic scale. BMI was calculated as weight (kg) divided by height (m) squared, and underweight was defined as BMI <18.5 kg/m2. 14 Women’s empowerment was assessed on a 30-question survey. The now widely used Women’s Empowerment in Agriculture Index was not yet developed at the time of our baseline survey in 2010. 15 Using exploratory factor analysis on the full EHFP baseline sample of 1882 women, data were reduced into 7 empowerment domains: meeting with other women (range 0-5, Cronbach’s alpha = 0.90), spousal communication (range 0-14, Cronbach’s alpha = 0.87), social support (range 0-4, Cronbach’s alpha = 0.90), purchasing decisions (range 0-8, Cronbach’s alpha = 0.90), family planning decisions (range 0-2, Cronbach’s alpha = 0.65), health care decisions (range 0-2, Cronbach’s alpha = 0.58), and IYCF decisions (range 0-2, Cronbach’s alpha = 0.69). We calculated continuous individual scores for each domain and a continuous total empowerment score (range 0-37). Further details on the empowerment score have been previously published. 11
Analytic Sample
The analyses presented here used data on women who participated in both the EHFP evaluation and the CHANGE baseline survey (n = 134), and thus had a child aged 3 to 12 months in 2010 and a child aged <15 months in 2014. Of these 134 mothers, who represented approximately 7% of the 2010 EHFP baseline study sample, 82 lived in treatment villages, where the EHFP program was implemented, and 52 lived in control villages.
The EHFP evaluation sample size was based on power calculations to detect a minimum change of 0.25 in mean child length-for-age Z-score and weight-for-length Z-score, and 0.3 g/dL in mean child hemoglobin concentrations between the treatment and control groups. 12 Using the same type 1 error (α) of 0.05, power of 0.80, and the actual intracluster correlation for each indicator, we calculated that the sample size for the present analyses allowed us to detect a change of 14 to 16 percentage points (pp) in women’s underweight prevalence, 18 to 28 pp in women’s knowledge, and 1.9 to 2.3 points in total women’s empowerment score.
Statistical Analysis
We examined 3 types of effects in our sample of women for which data were available at all 3 time points (2010, 2012, 2014): program effects (2010-2012), postprogram effects (2012-2014), and overall 4-year effects (2010-2014). We estimated these effects using difference-in-difference (DID) estimates which examined the change over time in women’s outcomes between treatment and control villages, in line with the econometric approach used in previously published work on the EHFP program. 11 -13 All specifications controlled for baseline value of the outcome (thereby reducing the risk of regression to the mean), 16,17 household size, number of children <5 years of age (as a proxy for parity), housing quality score (calculated for the full EHFP baseline sample using principal components analysis), polygamy, household head gender, woman’s age, woman’s education, and child age. BMI and underweight estimates also controlled for the month the anthropometric measurement was taken. 11 Standard errors were clustered at the village level. All analyses were intent-to-treat. Estimates were considered marginally statistically significant at P < .10 and statistically significant at P < .05. All statistical analyses were performed in STATA 14.2. 18
The 2 EHFP treatment groups (HC and OWL) were pooled and compared to the control group for the analyses presented here. The EHFP study was designed to look at differential impacts on children’s nutritional status by BCC delivery platform. However, the BCC implementers were not considered to be of primary importance for secondary measures such as women’s outcomes. 11
Given the nonrandomized nature of our study sample, we tested for balance across the treatment and control groups in 2010. We compared household and women’s characteristics using t tests. Differences were considered statistically significant at P < .05.
Since our sample was limited to women who participated in both the EHFP program evaluation and the CHANGE baseline survey, we also assessed whether sociodemographic characteristics of our subsample of women were different from those of the original EHFP study sample. We used t tests to compare household and women’s characteristics in 2010 for the subsample of women in our study and the remainder of women in the original EHFP study sample. Indicators were considered balanced between the subsample and the rest of the 2010 study sample at P > .05.
Ethical Approval and Consent
Trained fieldworkers provided information about each study and obtained oral informed consent from both the household head and target women. The protocols for both studies were approved by the Ministry of Health of Burkina Faso and the institutional review board of the International Food Policy Research Institute. The EHFP trial was registered with ClinicalTrials.gov, number NCT01825226, and the CHANGE trial was registered with number NCT02236468.
Results
Women in our study subsample were similar to women in the rest of the EHFP study sample in 2010, except that the former were significantly less likely to live in female-headed households (Supplementary Table 1). This difference held for both treatment groups. In addition, within the control group, women in our subsample were significantly less likely to have any formal education or to be underweight as compared to the rest of the EHFP study sample, whereas within the treatment group, women in our subsample were significantly less likely to live in households where the household head had any formal education as compared to women in the rest of the EHFP study sample (Supplemental Table 1).
Within the study subsample, some differences in household, household head, and women’s characteristics between the treatment and control groups in 2010 are of note (Table 1). Specifically, polygamy was less prevalent and dirt floors were more prevalent among treatment as compared to control households. Treatment households had higher housing quality score compared to control households. Moreover, more household heads in the treatment group had any formal education in 2010 as compared to the control group. However, none of these differences were statistically significant, likely due to lack of statistical power due to small sample sizes. With respect to women’s characteristics, women in the treatment group were significantly more likely to be underweight compared to women in the control group, which was characteristic of the full EHFP study sample, 11 albeit differences in our study subsample were larger. Likewise, women in the treatment group were significantly more likely to have any formal education compared to those in the control group.
Household and Women’s Characteristics of the Study Sample in 2010 by Treatment Group.
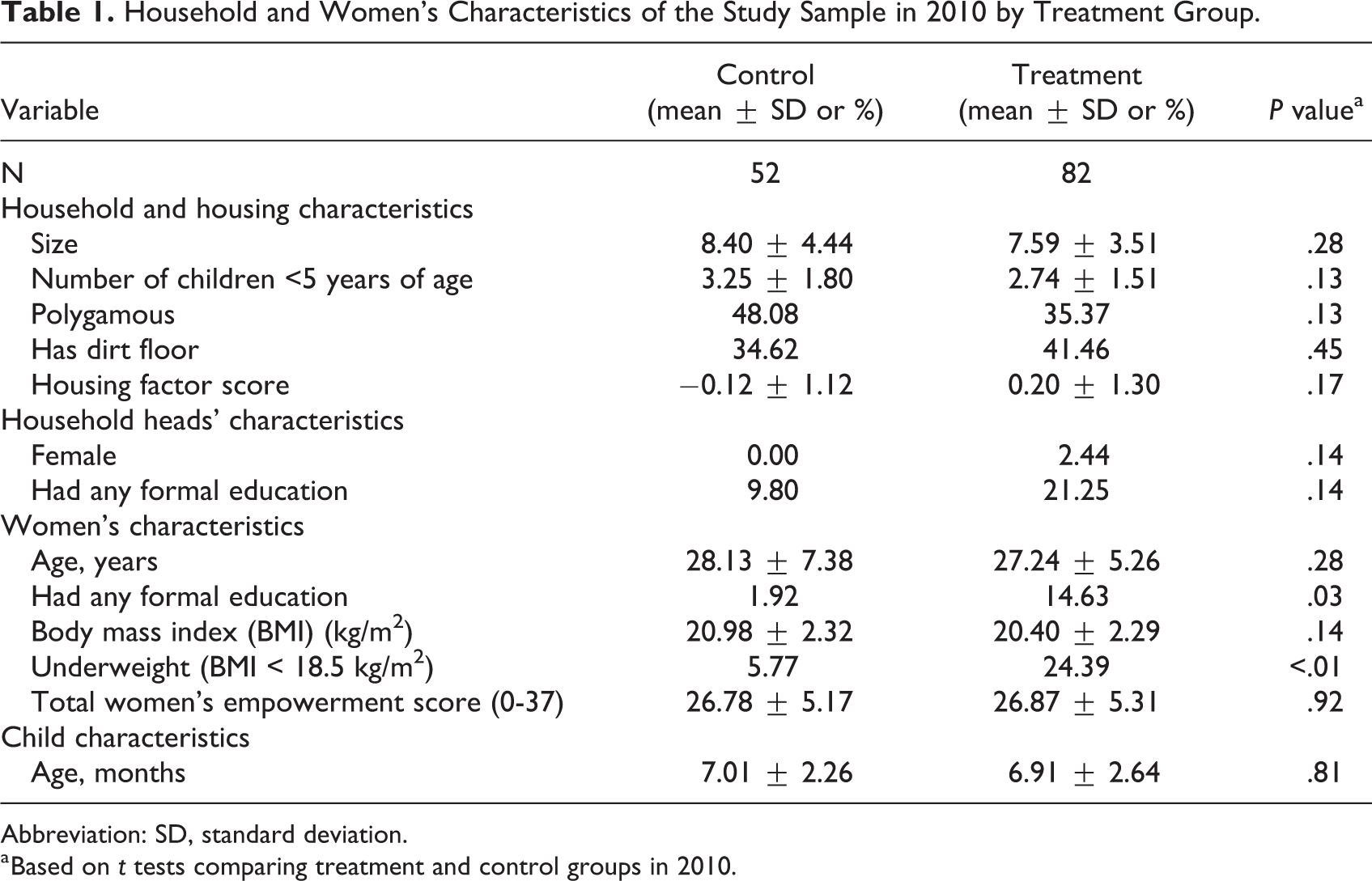
Abbreviation: SD, standard deviation.
a Based on t tests comparing treatment and control groups in 2010.
We found no effect of the EHFP program on women’s BMI in our subsample (Figure 1, Panel A, Supplemental Table 2), results consistent with those in the full EHFP sample, 11 and no significant postprogram or overall effects. With respect to women’s underweight, we found a positive effect of the EHFP program on women’s underweight prevalence of 16.44 pp (Figure 1, Panel B, Supplemental Table 2), which was larger than the 8.7 pp in the full EHFP sample. 11 Although we found no significant postprogram effects, differences were sustained in the postprogram period, resulting in an overall 18.26 pp decrease in underweight prevalence from 2010 to 2014 among women living in treatment compared to control villages (Supplemental Table 2).
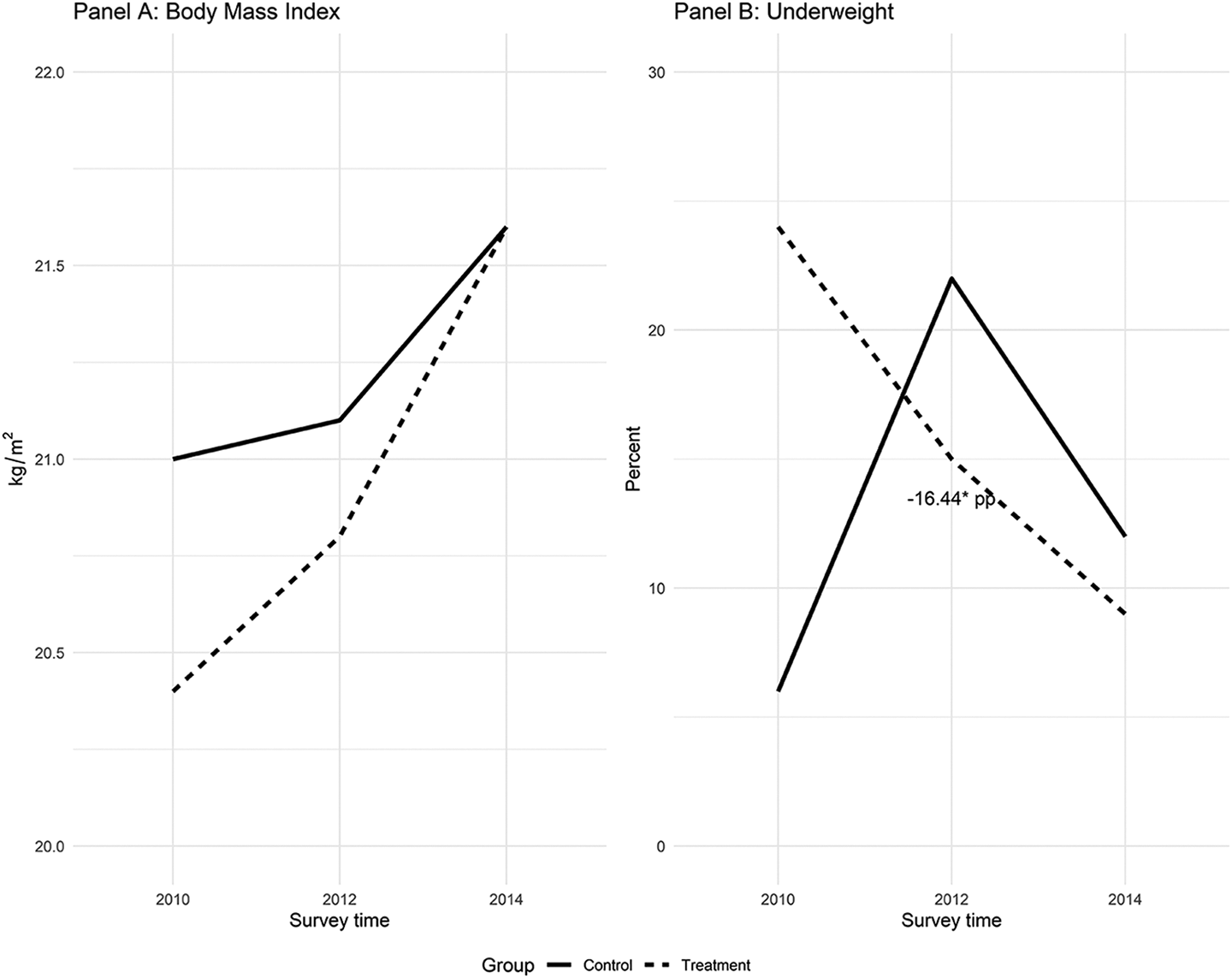
Sustained effects on the nutritional status of women targeted by the Enhanced Homestead Food Production Program or not, treatment and control, respectively. Values are mean ± SD or percentages. Coefficients ± SE or percentage points (pp) from statistically significant difference-in-difference (DID) estimates comparing treatment and control groups are labeled. Significance level for differences between treatment groups based on one-sided t tests: * P < .10, ** P < .05. SD indicates standard deviation; SE indicates standard error.
With respect to knowledge about IYCF practices, we observed positive effects of the EHFP program of 28.40 pp on women’s knowledge that liquids should be introduced at 6 months of age (Figure 2, Panel B, Supplemental Table 3), in line with results in the full EHFP sample. 12 We observed no significant postprogram effect; however, differences between treatment and control were sustained, resulting in an overall 4-year increase in the proportion of women knowing that liquids should be introduced at 6 months of age (DID: 31.29 pp; P = .02). In contrast to the full EHFP sample where positive effects on knowledge about breastfeeding within the first hour of birth and that semisolid foods should be introduced at 6 months of age were also observed, 12 we found no program, postprogram, or overall effects on these outcomes in the subsample (Figure 2, Panels A and C, Supplemental Table 3).
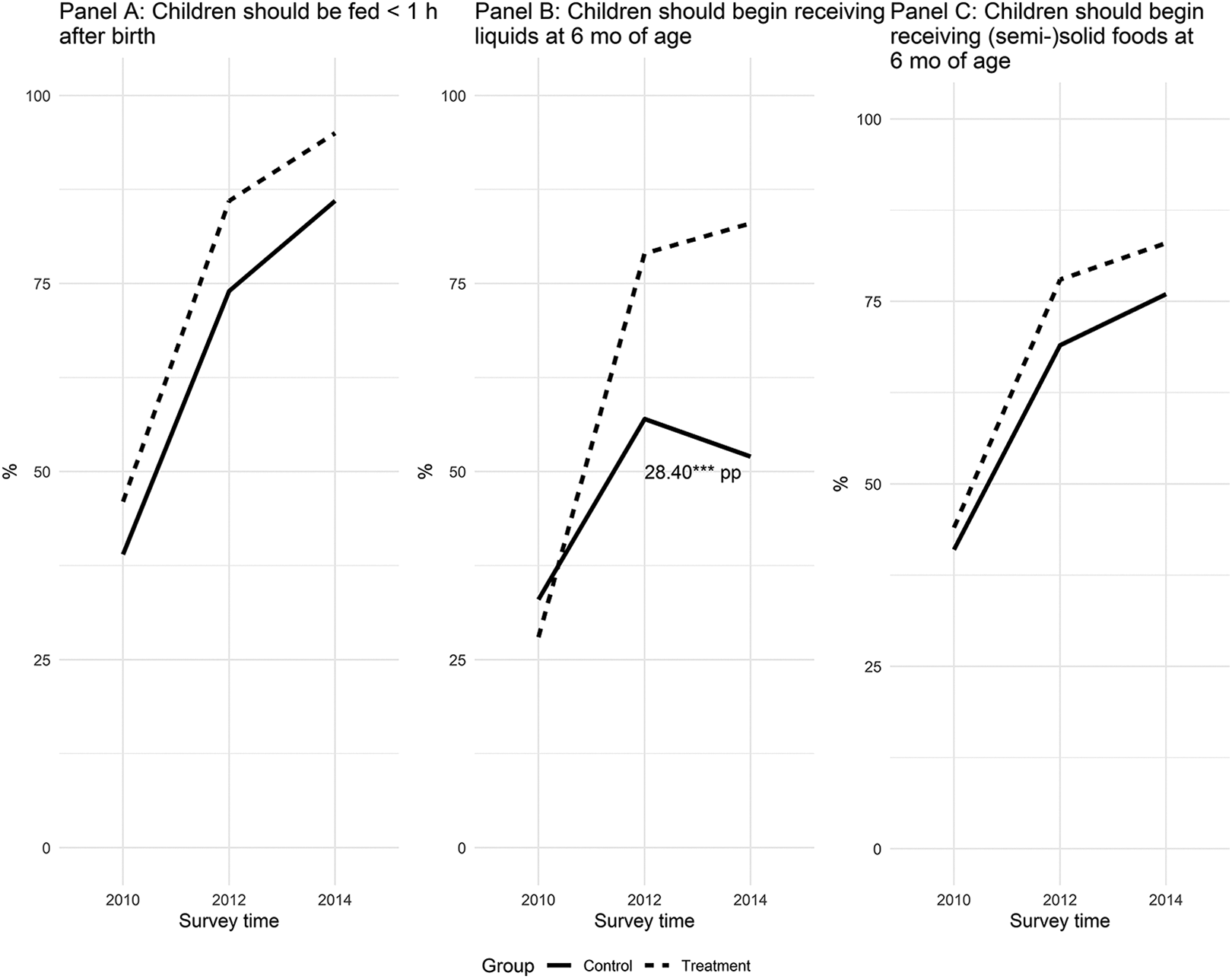
Sustained effects on the knowledge about infant and young child practices of women targeted by the Enhanced Homestead Food Production Program between 2010 and 2012 and those that were not, treatment and control, respectively. Values are mean ± SD or percentages. Coefficients ± SE or percentage points (pp) from statistically significant difference-in-difference (DID) estimates comparing treatment and control groups are labeled. Significance level for differences between treatment groups based on one-sided t tests: * P < .10, ** P < .05. SD indicates standard deviation; SE indicates standard error.
Likewise, we found no effect of the EHFP program on women’s knowledge about washing hands before feeding a child (Figure 3, Panel A, Supplemental Table 3), despite a positive effect being observed in the full EHFP sample. 12 In the postprogram period, we observed a decline in the proportion of women knowing this key handwashing moment in the control group, resulting in a 5.87 pp difference between treatment and control; however, this estimate did not reach statistical significance due to small sample sizes and related lack of statistical power. As a result, we also observed no significant overall effects. With respect to knowledge about washing hands after cleaning a child who has defecated, we observed a similar difference between groups as the one observed in the full EHFP sample between 2010 and 2012; however, our estimates in the subsample did not reach statistical significance (Figure 3, Panel B, Supplemental Table 3). These results remained unchanged in the postprogram period, leading to no significant overall effect.
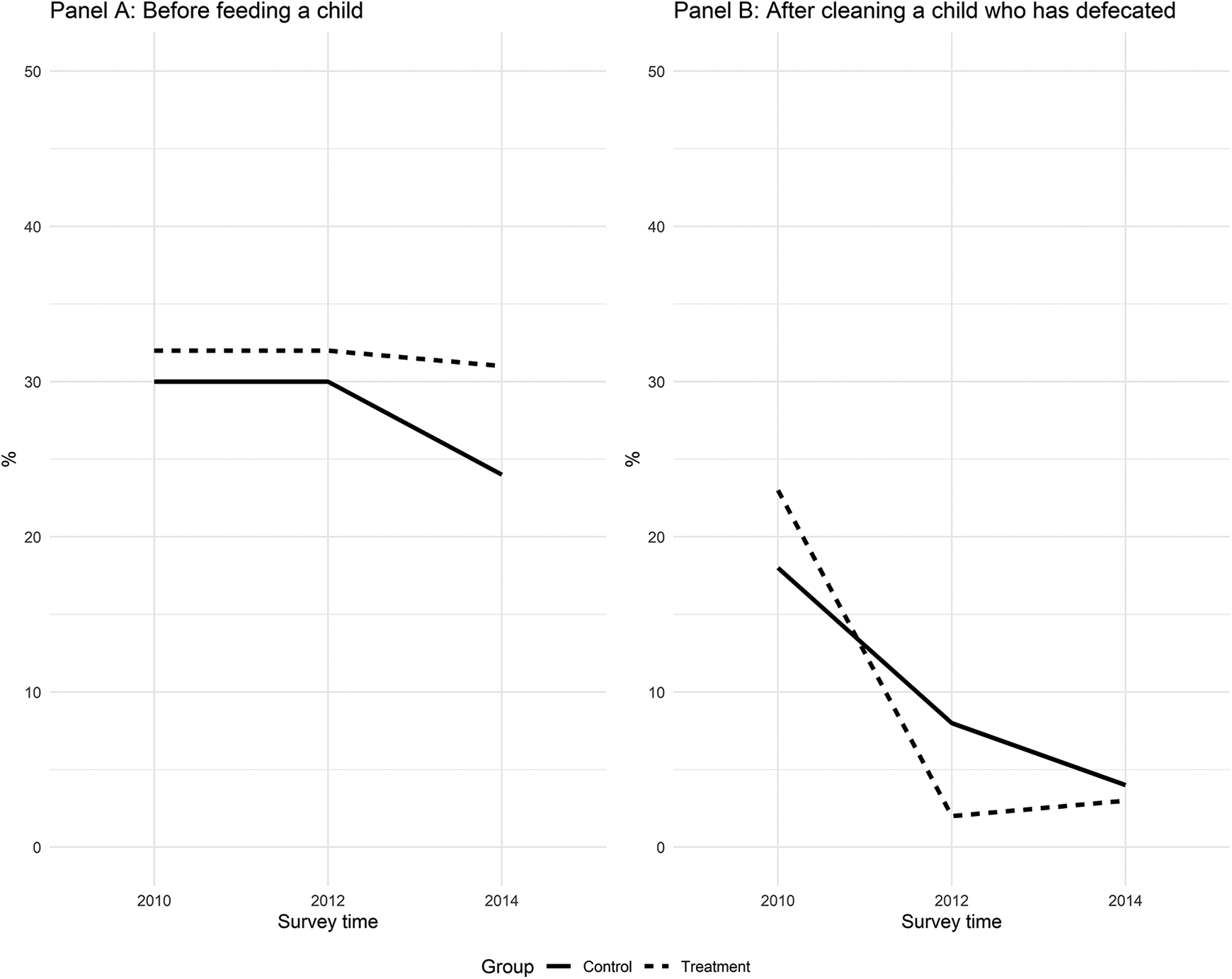
Sustained effects on the knowledge about handwashing practices of women targeted by the Enhanced Homestead Food Production Program between 2010 and 2012 and those that were not, treatment and control, respectively. Values are percentages. Percentage points (pp) from statistically significant difference-in-difference (DID) estimates comparing treatment and control groups are labeled. Significance level for differences between treatment groups based on one-sided t tests: * P < .10, ** P < .05.
Finally, we examined effects on women’s empowerment (Figure 4, Supplemental Table 4). Although Olney et al showed positive effects of the EHFP program on meeting with other women, health care decisions, and total empowerment score, 11 we observed no program effects, nor any postprogram or overall program effects in our subsample. In fact, we observed a small negative postprogram effect on meeting with other women (DID: −1.17 ± 0.53, P = .03) which appeared to be due to women in control villages catching up with women in treatment villages. With respect to purchasing decisions, health care decisions, and total empowerment, we also observed no postprogram or overall effects.
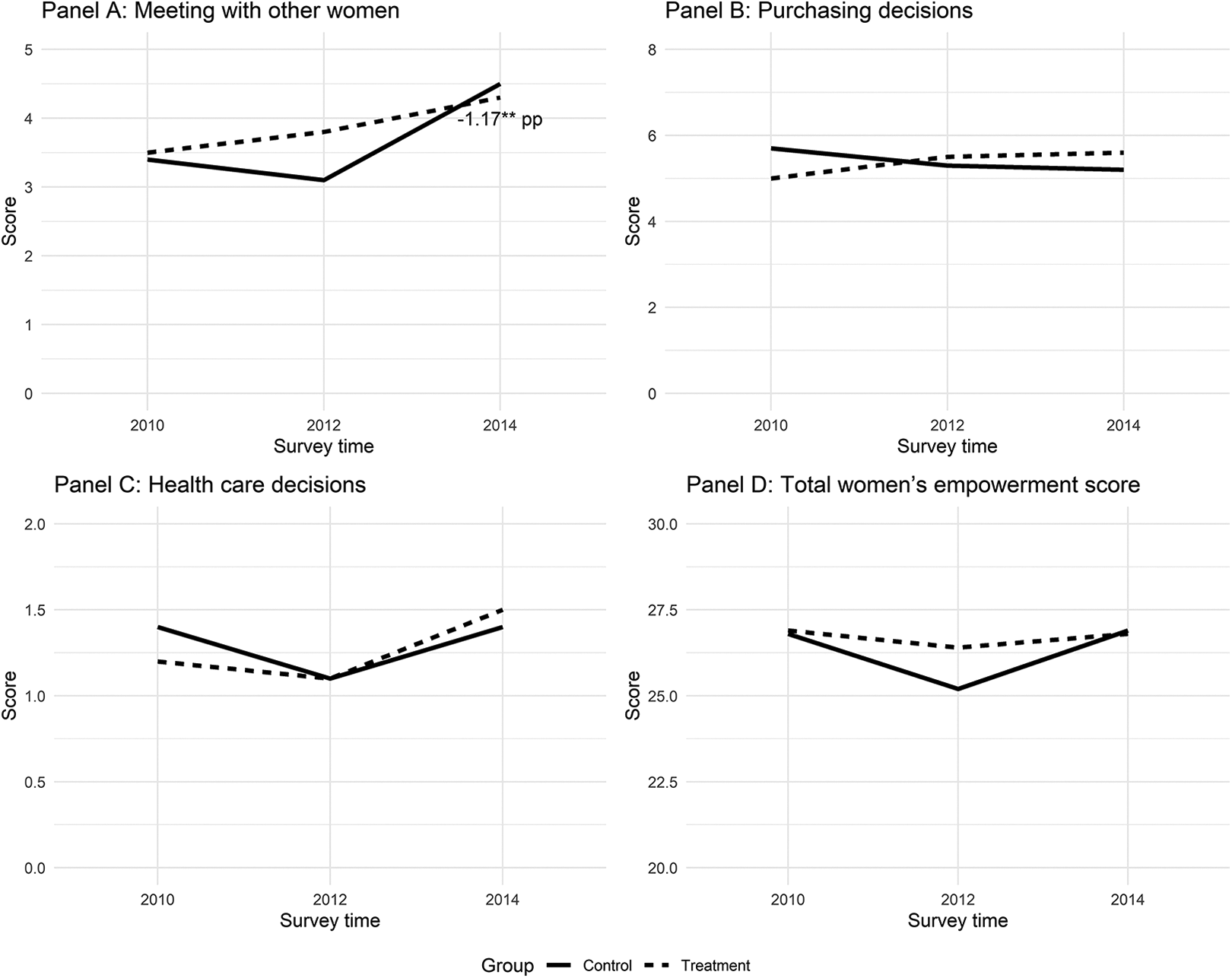
Sustained effects on the empowerment of women targeted by the Enhanced Homestead Food Production Program between 2010 and 2012 and those that were not, treatment and control, respectively. Values are mean ± SD. Coefficients ± SE from statistically significant difference-in-difference (DID) estimates comparing treatment and control groups are labeled. Significance level for differences between treatment groups based on one-sided t tests: * P < .10, ** P < .05. SD indicates standard deviation; SE indicates standard error.
Discussion
In this study, we examined the program, postprogram, and overall 4-year effects of HKI’s EHFP program in Burkina Faso among a subset of women who received the program for 2 years (between 2010 and 2012). Although we found no significant postprogram effects, we observed positive overall 4-year effects on women’s underweight and knowledge about some IYCF practices. Our results support the potential of NSAPs to contribute to sustained changes in women’s underweight status and nutritional knowledge. Previously published results showed that the EHFP program reduced underweight by 8.7 pp among targeted women during the 2-year implementation period. 11 In this article, we show that, within our subsample of women, the 16.44 pp reduction in women’s underweight generated during the EHFP program implementation period was sustained 2 years after the program ended leading to an overall 4-year reduction in women’s underweight of 18.26 pp. This reduction in women’s underweight is at least partially supported by previously demonstrated positive impacts of the EHFP program on household calorie consumption. 19 The much larger effect size we observed is likely due to women in our control group being significantly less likely to be underweight compared to women in the rest of the EHFP control group in 2010. Of note is that underweight prevalence in the control group also declined between 2012 and 2014, potentially indicating socioeconomic improvements in the area. Our findings are consistent with the only other study we are aware of that assessed the long-term impact of a NSAP on women’s nutritional status and showed that early adopters of improved home-gardening technologies in Bangladesh had 0.54 kg/m 2 significantly higher BMI 10 years after the start of the program. 8 Although we did not observe an effect on BMI, previously published results from the full EHFP sample showed a significant increase in BMI among women who were underweight at baseline, indicating the program benefited the most vulnerable women. 11 Given the small sample size in the current analysis, we did not conduct a similar subgroup analysis which would have been underpowered.
Our results also highlight the potential of BCC strategies to generate long-term positive effects, which may benefit future children. We found significant sustained 4-year improvements in women’s knowledge that liquids should be introduced at 6 months of age. Results also suggested potential sustained 4-year improvements in women’s knowledge that children should be breastfed within the first hour after birth and that semisolid foods should be introduced at 6 months of age. However, these were substantially smaller than those observed in the full 2010 EHFP sample 12 and smaller than the differences we were powered to detect with our small sample size. Of note is that women in the treatment group were significantly more likely to have any formal education than women in the control group (albeit the proportion was still low at 15%), which may help explain the large sustained effects on knowledge of certain IYCF practices we found. Nevertheless, these findings suggest that BCC strategies may have the potential to generate long-term sustained improvements in women’s knowledge about some IYCF practices even in the absence of repeat messaging. However, we did not observe any sustained effects on handwashing knowledge in our study subsample, consistent with results from the full EHFP sample 1 year-after the program ended. 13 This could be due to several reasons such as the relative emphasis of the BCC on IYCF compared to hygiene messages, the perceived relevance of the messages for the participants, and/or their potentially limited ability to apply knowledge due to lack of resources. Increasing the relative frequency and/or addressing resource constraints (eg, water, soap, handwashing stations) could help increase the impact of this type of program on handwashing knowledge in the short- and long-term.
Lastly, we found no significant postprogram or overall 4-year effects on women’s empowerment in our subset of women, possibly due to the fact that women in the control group improved postintervention and seemed to have caught up with women in the treatment group. Improvements in the control group could be due to socioeconomic improvements in the area, spillover effects from neighboring treatment villages, or gender-sensitive interventions in the control areas. However, we lacked data to confirm these hypotheses. The program effect (2010-2012) on women’s total empowerment score in the sample used for this analysis was substantially smaller than the impact observed in the full EHFP sample 11 and our sample size was smaller, resulting in a nonstatistically significant difference.
Although promising, our findings should be interpreted with caution for 2 main reasons. First, our sample for the postintervention and overall effects was small, so our analyses lacked the statistical power to detect small differences in the outcomes we examined. Second, the postprogram and overall 4-year effects presented here cannot be causally interpreted as longer term effects of the EHFP program because we used a subsample of the original households in our 2014 analysis. The subsample included households who met the targeting criteria of having a child <15 months of age in 2014 and had been in the 2010 sample (having a child 3-12 months of age at the time). In effect, our sample excluded primiparous women and was therefore different from the original EHFP sample for which parity was not a targeting criteria in 2010. In fact, we did find some important differences between our study subsample and the rest of the 2010 EHFP sample at baseline. Specifically, women in the rest of the EHFP sample were significantly more likely to come from female-headed households, which could help explain their lower probability of having another eligible child in 2014 and hence lower probability of being part of our subsample. It is likely that female-headed households have very specific characteristics, and our findings might not be generalizable to this population (6.7% of the full 2010 EHFP sample and 8% of the full 2014 sample). Nevertheless, given that our subsample was similar to the rest of the 2010 EHFP sample for several other characteristics and that our findings were generally consistent with previously published findings on the EHFP program and postprogram impacts, 11 -13 it is plausible that the overall effects we found were due to the EHFP program. However, purposively designed evaluations to assess the sustained effects of EHFP programs are needed to support and strengthen the encouraging results presented here.
Despite these limitations, our study showed significant positive 4-year effects of HKI’s EHFP program on women’s nutritional status and knowledge about some IYCF practices 2 years after the program ended. Additionally, our findings suggest that the positive effects on other knowledge indicators observed during the program implementation period were generally sustained among women in the treatment groups. Our study findings imply that nutrition- and gender-sensitive programs like HKI’s EHFP program can improve women’s nutritional status and child feeding knowledge over a period of 2 years, and that some of these effects may be sustained in the absence of programmatic activities. Although no sustained effects were found on indicators of women’s empowerment, the sustained effects on women’s knowledge are by themselves an important aspect of empowerment, especially for women who have other children beyond the life of a project. Achieving sustained impacts on other dimensions of women’s empowerment may require continued engagement in the communities to achieve sustainable transformational change. A key lesson from our study is that assessment of sustainability of impacts should be an explicit goal of program evaluation plans and should be developed, along with a sustainability plan, at early stages of design and program planning.
Supplemental Material
Supplemental Material, sj-pdf-1-fnb-10.1177_03795721221090380 - Four-Year Effects of a 2-Year Nutrition and Gender Sensitive Agricultural Program on Women’s Nutritional Status, Knowledge, and Empowerment in Rural Burkina Faso
Supplemental Material, sj-pdf-1-fnb-10.1177_03795721221090380 for Four-Year Effects of a 2-Year Nutrition and Gender Sensitive Agricultural Program on Women’s Nutritional Status, Knowledge, and Empowerment in Rural Burkina Faso by Lilia Bliznashka, Elodie Becquey, Marie T. Ruel and Deanna K. Olney in Food and Nutrition Bulletin
Footnotes
Authors’ Note
DKO and MTR designed the EHFP evaluation; DKO, EB, and MTR designed the CHANGE evaluation; DKO led the EHFP data collection activities; DKO and EB led the CHANGE data collection activities; LB and DKO conceptualized the current study, led the data analyses, and drafted the manuscript; LB had final responsibility for submitting this article for publication; all authors contributed to interpreting the results, had full access to the data, and read and approved the final version of the article.
Acknowledgments
The authors would like to thank Helen Keller International (HKI), the HKI Burkina Faso Office, HKI’s West Africa Office, the EHFP program team in Burkina Faso, and specifically Marcellin Ouedraogo and Abdoulaye Pedehoumbga. The authors would also like to extend their gratitude to Andrew Dillon for his role in the design and implementation of the EHFP study, Ousmane Birba for his help in fieldwork preparation and data collection activities, Agnes Quisumbing for her help in interpreting the results, and Daniel Gilligan for his support with the statistical analyses.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by United States Agency for International Development (USAID)/Office if Foreign Disaster Assistance (OFDA) through Helen Keller International (HKI), the Bill and Melinda Gates Foundation through the Gender, Agriculture and Assets Project (GAAP), Global Affairs Canada, and the Consultative Group for International Agricultural Research (CGIAR) Research Program on Agriculture for Nutrition and Health (A4NH) led by IFPRI.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.