
Abstract
Background:
Household water security matters greatly for child nutrition outcomes in the global South. Water’s role in sanitation/hygiene, via diarrheal disease, is cited as a primary mechanism here. Yet, the relationship between Water along with Sanitation and Hygiene (WASH) and child stunting remains inconclusive. Water-related mechanisms outside of the traditional scope of WASH might assist with explaining this.
Objective:
We aim to test the mediating role of reduced dietary diversity as an additional potential mechanism in linking worse household water access to increased risk of early childhood stunting, separating its effects from sanitation and diarrhea among children (as a proxy for hygiene) and taking into account regional water availability.
Method:
We use nationally representative India Demographic and Health Survey (2015-16) data for 58 038 children aged 6 to 23 months, applying generalized structural equation modelling to estimate water’s direct and indirect effects (as mediated through dietary diversity and access to sanitation) on a child’s likelihood of being stunted.
Results:
Suboptimal water access is significantly associated with elevated likelihood of child stunting. More than 30% of the effect is indirect. In the context of low water access and availability, children’s dietary diversity alone mediates more than 20% of its total effect on child stunting.
Conclusion:
Beyond the WASH mechanisms, household water access affects child stunting indirectly, mediated through its impacts on children’s dietary diversity. These mediating effects are also moderated by regional water availability. Water interventions in low-water regions should help reduce children’s risk of nutrition-related stunting in households with lowest water access.
Introduction
The role of safe drinking water to promote childhood nutrition has long been established, 1 -3 especially the role of reducing nutrition-impairing diarrheal disease 4 through what is termed “the water, sanitation, and hygiene (WASH) mechanism.” 4 -6 Studies show a consistent positive association between access to clean water and improved child dietary intake and nutrition. 7 -12 But evidence on the relationship between safe, adequate water and child stunting outcomes is less conclusive. 13 -16 For example, Esrey 17 found that children in households with an improved water source had small benefits to height that were apparent only when household sanitation was also improved. Fink et al 18 made similar observations showing smaller effect of water access on child’s height as compared to that of sanitation. Recent randomized controlled trials in Bangladesh, Kenya, and Zimbabwe failed to identify any marked impact of WASH interventions on childhood diarrhea and stunting. 19 -21 These variations observed in impact of WASH on nutrition outcomes also underscore the role of context. Studies that document a positive association between better access to WASH and greater childhood height for age z-scores (HAZ) 22 also indicate that the association varies depending upon several factors such as child’s age, breastfeeding status, and maternal education, among others. 2,13,23,14,24
This observed heterogeneity in the impact of “the WASH mechanism” on different aspects of child nutrition is one reason underlying the call for broadening the conceptual structure of WASH—as an aspect of child nutrition and development interventions—beyond the sum of toilets, caregiver hand washing, and water purification. 22 The World Health Organization (WHO) and United Nations International Children’s Emergency Fund (UNICEF) 25 also underscore that the role of WASH should not only be seen in terms of health impact but should also focus on associated intermediate outcomes such as diarrhea, dietary diversity, and so on. Although WASH interventions are often described in terms of their role in preventing disease transmission, the benefits are not confined to health. 5 Thus, there is growing rationale for empirical testing of possible broader and more integrated pathways linking varied aspects of WASH with varied nutrition outcomes. 26,24
Water has established and potential linkages outside of WASH with nutrition through (a) health and hygiene, (b) household food security, and (c) care needs. 27 The role of household water access in affecting disease risk is one of the best studied. 28 -32,18,4 Water availability also has direct implications for overall food production and household food security, because it is needed to care for animals, grow crops, and prepare and cook food. 33 -36 At the household level, water access may affect nutrition outcomes by affecting people’s preference for growing and consuming less nutritional foods that require less water to produce or prepare. 37 -41 Paying for household water access competes with funds for households to acquire adequate, quality food. 5,42,43 The body also needs adequate water intake to absorb food nutrients effectively. 44 In the context of care needs, lack of access to water may also affect nutrition when it impacts the available time or other opportunities of caregivers. 27 These effects are mostly on mothers, who are managing household water tasks like fetching as well as childcare. 45 -48 Inadequate water access appears to reduce the diversity and quantity of complementary foods fed to children, for example, in low- and middle-income countries. 49
Here, we propose that the relationship of household water access to child’s dietary diversity is an additional pathway linking household water access to child nutrition outcomes like stunting. Drawing upon our recent work linking household water access and child’s dietary diversity in India 50 and taking into account regional variations in water availability, we test if household water access might affect child nutrition once separated from its simultaneous effect on drinking, sanitation, and hygiene. That is, outside of what is normally described as the WASH mechanism. To do this, we use a large nationally representative data set to test household water’s direct effects on child stunting and possible indirect effects via dietary diversity, and distinguish this from alternate—and better established—pathways via WASH (water along with sanitation and hygiene) effects.
This objective fits into the broader call from leading global health agencies and the academic community as discussed above, to clarify the complex pathways linking household water access and child nutrition outcomes. We focus on the effects of household water access on the likelihood of infants and young children meeting minimum dietary diversity as our index of early child feeding and nutritional status. But we also account for parallel indirect channels through which water access might impact child nutrition, for example, by affecting access to improved sanitation. Our specific proposition is that the association between suboptimal household water access and child nutrition outcomes is both direct (through biological water needs) and indirect as mediated through water’s effect on dietary diversity of infants and young children as well as on household access to sanitation.
Water, Diet, and Nutrition in India
As per the latest round of the India Demographic and Health Survey (2015-16), 37.3% of children aged below 5 are stunted. The proportion of children in India aged 6 to 23 months meeting minimum recommended levels of dietary diversity, as defined by WHO, 51 is very low, at 22%. 52 As per the assessment of India State-Level Disease Burden Initiative Malnutrition Collaborators, 53 malnutrition was the leading risk factor for death in children younger than 5 years in every state of India.
Collectively, lack of access to adequate and/or safe water and poor conditions of sanitation and hygiene have been considered key factors underlying the high incidence of child stunting in India. 54 -58,13,52,22 Generally, household access to improved water sources has been found to predict lower prevalence of both childhood diarrhea and stunting. 16,2
Although the WHO/UNICEF Joint Monitoring Report 59 estimates that 93% of India’s population has at least basic access to drinking water, only 63% have the access on their home premises and only 44% have access to piped water. Furthermore, only 32% of the rural population in India has access to piped water. Overall, more than 160 million people in India do not have access to clean water. 60 Achieving universal access to safe drinking water is likely to remain a huge challenge for all countries, 61 but more so for India, given low supply of piped water and severe regional water scarcity in the country.
With per capita availability of 1588 cu m/year, 62 India is a water stressed country as per the United Nations definition wherein water stress area is defined as such when annual water supply drops below 1700 cu m/person. Over half (54%) of India faces high to extremely high stress in terms of surface water. 63 Most regions of India suffer from water problems in terms of quality, quantity, or both. The majority of Northwest, Central, and South India are water stressed. South India in particular is subject to recurrent droughts leading to acute water scarcity. 64
This regional variation in water availability—distinct from household access to water—may have additional effect on children’s dietary diversity 50 and nutritional status. High water availability in the neighborhood can encourage better hygiene practices. At the same time, low water availability might affect the kinds of crops that are grown as well as limit overall crop production. Regions with limited surface water may offer limited access to fish, meat, and dairy, since they are water-intensive products, thus impacting household and child’s access to diversified diet. Though the market is able to supply foods imported into the local markets, poor people especially those in rural areas have low purchasing power and depend more upon locally grown foods than on available through the market.
Thus, there is ample basis to conceptualize that household water access as well regional water availability can affect child nutrition outcomes in multiple ways. Here, we propose that household water access and regional water availability can positively affect child nutrition by improving child access to dietary diversity as well as household access to sanitation. This effect is in addition to the direct effect that household access to water (along with sanitation and hygiene) is likely to have on child nutrition, as also the indirect effect that household water access can have on child nutrition by influencing access to sanitation and hygiene facilities.
Methods
Data and Variables
Data applied herein are from the most recent (2015-16) India Demographic and Health Survey (DHS), a nationally representative survey that provides comprehensive information on childcare, child feeding practices and relevant sociodemographic information on the household. The sample included in the analysis represents children aged 6 to 23 months (N = 58 038), nested in a relatively smaller number of households. Children were included in the analytic sample if they had complete data on the outcome, mediating, and predictor variables of interest.
Outcome variable
Our main outcome variable is whether the child is stunted or not, based on HAZ. This is calculated as the difference between the individual and the reference population median, divided by the standard deviation of the reference population. 65 A child with a z-score below 2 standard deviation is considered as stunted or too short for their age. 65
Mediating variable 1: child access to minimum dietary diversity
The dietary diversity of a child aged 6 to 23 months is our primary mediating variable. This is based on consumption of foods from 7 different food groups: grains, roots, and tubers; legumes and nuts; dairy products (milk, yogurt, cheese); flesh foods (meat, fish, poultry, and liver/organ meats); eggs; vitamin-A rich fruits and vegetable; and other fruits and vegetables. 51 To calculate the continuous score, a value of 1 is assigned for consumption of food from at least 1 of the 7 groups, so that the maximum dietary score of a child aged 6 to 23 months would be 7 and a minimum score would be 1. A child is classified as receiving minimum dietary diversity (MDD) if during the previous day, she or he was fed from at least 4 of the 7 food groups. 51
Mediating variables 2 and 3
Our proposition centers on explicating the indirect impacts that household water access can have on child stunting as mediated by child dietary diversity score. But we also account for possible mediation by household’s access to improved sanitation and hygiene. Access to hygiene manifests in child’s exposure to diarrhea among others. Accordingly, we have included household’s access to improved sanitation and child’s experience of diarrhea as the second and third mediating variables. According to WHO/UNICEF, 66 the following types of toilets are categorized as improved source of sanitation provided they are “unshared” between households—toilet flush to sewer system, septic tank, pit latrine to anywhere, pit latrine ventilated, pit latrine slab, and composting toilet. Our third mediating variable is whether or not the child experienced an episode of diarrhea in the last 2 weeks.
Key explanatory variables—household water access and regional water availability
We use household water access as the key dimension of water insecurity.
67,68
Reduced or inadequate household water access can be operationalized through varied measures, such as water source, quantity of water, time to fetch water, or the perceived degree to which household water needs are being met.
69,70
We use household water source as our key predictor variable through the question; “what is the main source of water used by your household for other purposes such as cooking and handwashing?” The response options include piped water, piped into dwelling, piped into yard/plot, bottled water, piped to neighbor, public tap, tube well water, tube well or borehole, protected well, protected spring, tanker truck, dug well, unprotected well, unprotected spring, river/dam, rainwater, and other. These were then coded into the following, based on WHO/UNICEF
71
access classifications Optimal access: piped water, piped into dwelling, piped into yard, bottled water. Among the available sources listed, these 4 sources are most likely to ensure water access in desirable quantity and quality meeting all consumption and hygiene needs in comfortable manner. Intermediate access: piped to neighbor, public tap, tube well water, tube well or borehole, protected well, protected spring, and tanker truck. These sources are more likely to assure that consumption needs are met and basic hygiene needs are likely to be met since even public sources are also protected. Basic or no access: dug well, unprotected well, unprotected spring, river/dam, rainwater, other. In these cases, we expect that consumption needs may be met with difficulty whereas minimum hygiene norms can hardly be assured.
Here, we have collapsed the “no access” and “basic access” categories to reflect “low access”, as the “no access” group had a very small sample size.
In addition, to account for the regional water context, we considered India’s spatial classification on the basis of a Surface Water Availability Index (“India Water Tool,” developed by World Business Council for Sustainable Development. Technical Note accessible from, www.indiawatertool.in/) developed to map India in terms of water availability. 50 The value of the indicator ranges from −1(low) to +1 (high) availability. The index classified India in 6 water availability regions, which have been recoded here in 3 categories (see Figure 1): Low water availability region (LWAR), medium water availability region (MWAR), and high water availability region (HWAR). Based on this scheme, HWAR included all northeastern Indian states (with the exception of Arunachal Pradesh), along with West Bengal, Himachal Pradesh, Punjab, Haryana, Uttarakhand, Kerala, and Goa. Medium water availability region includes Bihar, Jharkhand, Odisha, Andhra Pradesh, Tamil Nadu, Maharashtra, Karnataka, Jammu & Kashmir, and Gujarat come under of India. Finally, LWAR includes Telangana, Arunachal Pradesh, Rajasthan, Madhya Pradesh, Chhattisgarh, and Uttar Pradesh.
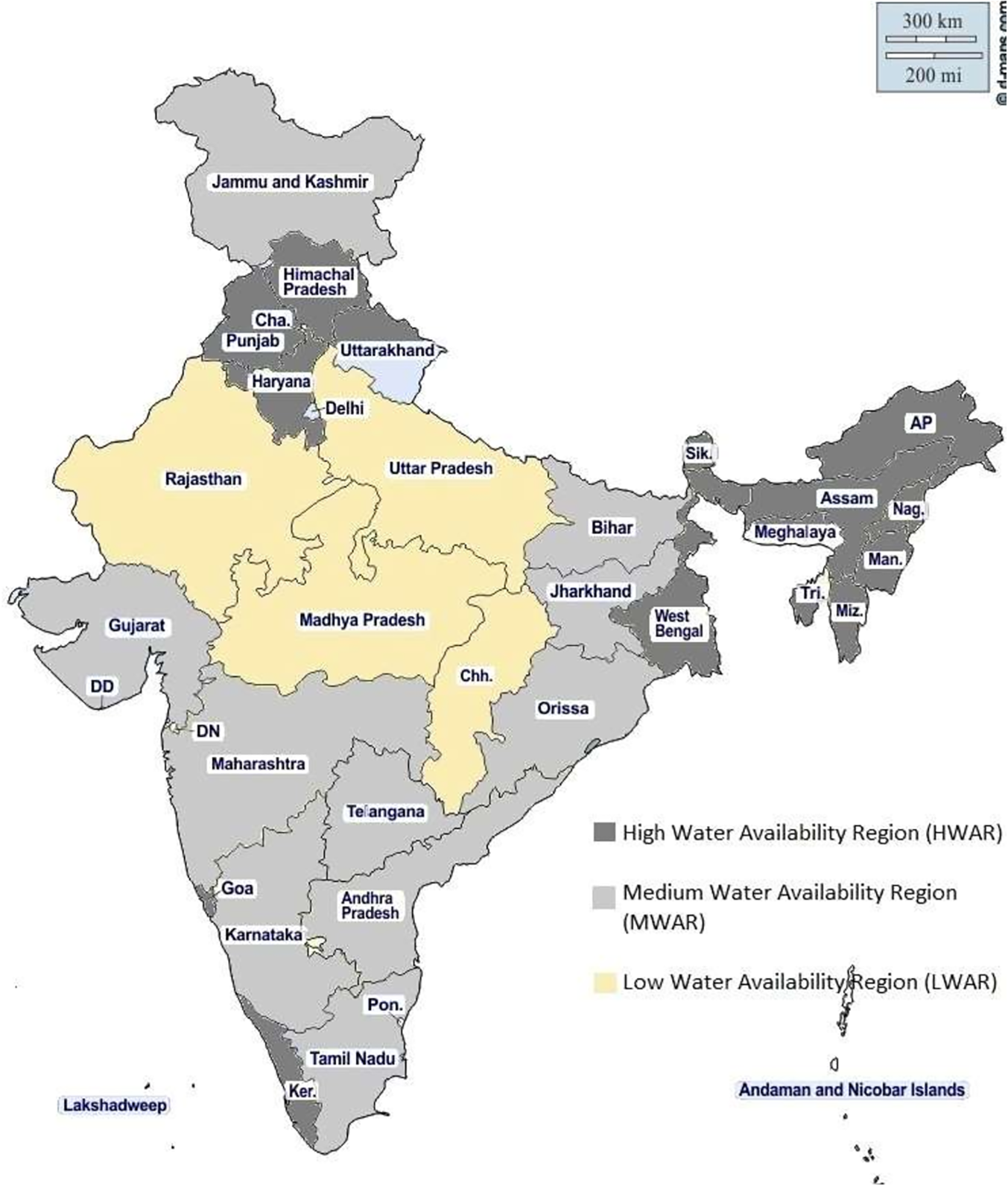
Classification of India based on water availability index.
Other covariates
To take relative household material wealth into account in the models, we constructed a physical asset index using the methodology similar to the standard DHS-constructed household wealth index. 72,73 This is because the DHS wealth index includes the variables on source of water, which is our key explanatory variable. We derive the physical asset index using a smaller set of variables that represent physical asset. These variables include housing characteristics, cooking fuel type, and ownership of specific consumer goods. We also do not include toilet facilities in the index since we control for sanitation as separate variable in our model. We then construct 4 household asset classes by dividing the n-ranked distribution into 4 quartiles based on the absolute scores for the entire country sample (Table 1).
Sociodemographic Characteristics of Infants and Young Children Aged 6 to 23 Months Included in the Analysis.
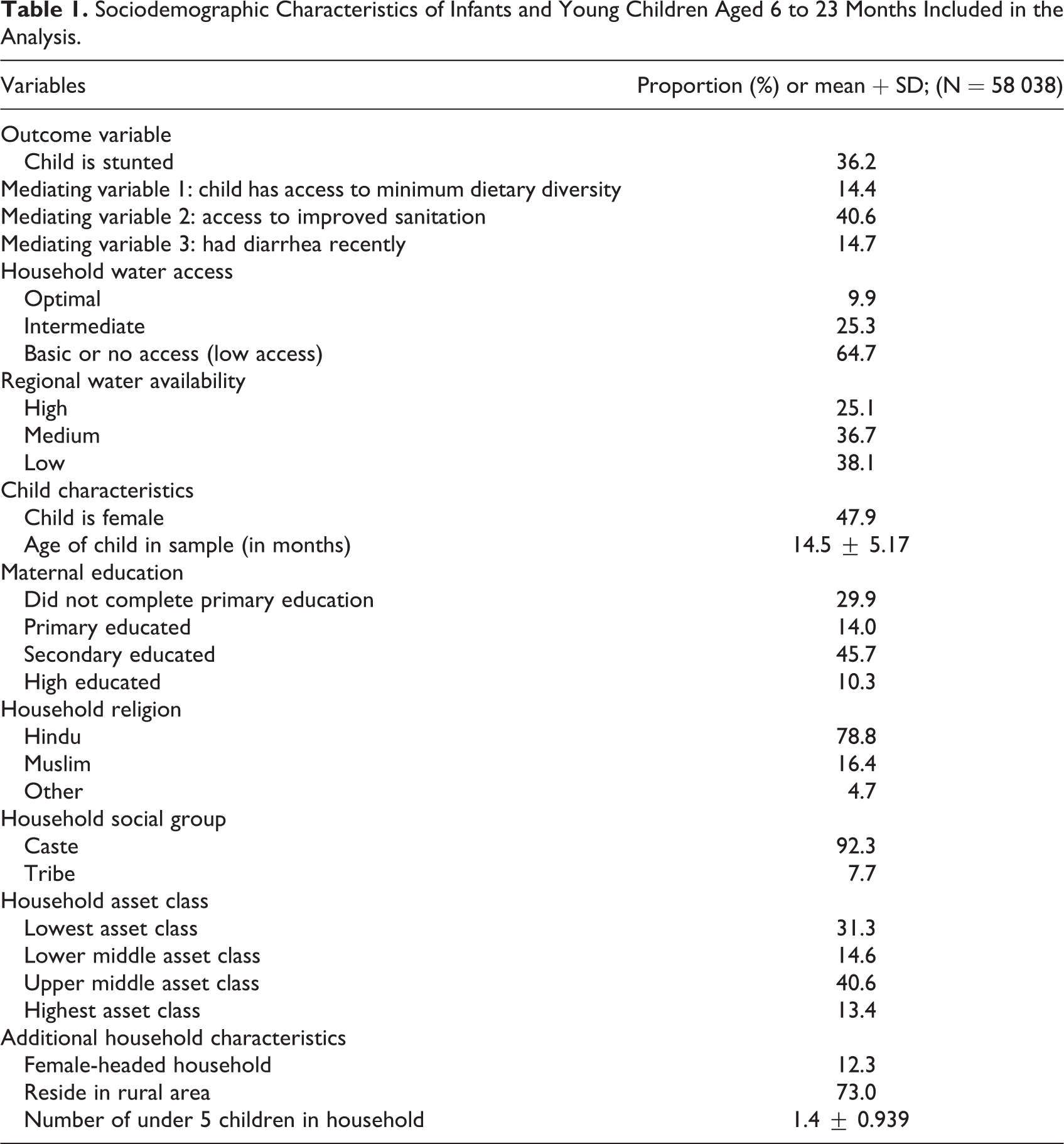
We include maternal education in our model since it together with awareness and knowledge affect child nutrition positively by improving care behavior and child feeding practices. We also tested the role of female versus male household head, given the relative social and economic vulnerability of the former compared to the latter.
Other variables included are place of residence (rural or urban), child age and gender, number of under 5 children in the household, religion, and social group. In India, households are constitutionally classified (India is traditionally a caste stratified society. In support of affirmative action, the Indian constitution defines certain population groups as scheduled caste and schedule tribes, based on their social and economic status) into various social groups in terms of caste. Here, we consider households as either caste or tribal group since dietary preferences are usually more variable between castes and tribes than within castes. 74
The Estimation: Generalized Structural Equation Modelling
We estimate an SEM to test the relationships since we have multiple mediations at the same time. SEM is particularly useful in case of linked regression style equations involving endogenous explanatory variables. 75 Here, we employ generalized structural equation modelling (GSEM) to estimate the relationship since our outcome and mediating variables are dichotomous requiring a nonlinear approach.
In our model, water availability and access (Xi) has direct effect on stunting (Ya) as well as an indirect effect through its effect on minimum dietary diversity (Yb), household access to improved sanitation (Yc), and child experience of diarrhea (Yd). To estimate the mediated or indirect effects of water on child stunting, we followed the method proposed by Buis, 76 which is a generalized version of Erikson et al 77 and decomposes total effects into direct and indirect (mediated) effects for each of 3 nonlinear relationships as well as the combined effect of the variables. The mediation estimate is done using the ldecomp command in STATA.
In addition, since our central focus is on the role of child’s dietary diversity in mediating the effect of water insecurity on child nutrition, we ran a separate SEM wherein child’s HAZ score and child’s dietary diversity score are continuous outcome and mediating variables.
All the analyses have been done in STATA version 16 after accounting for survey characteristics of DHS data using the svy command.
Results
Table 1 gives information on socioeconomic and demographic characteristics of the sample. In our sample, nearly 10% of households had optimal water access, 25% had intermediate water access, and around 65% had low water access (Table 1). Around 38% of our sample came from LWAR, 36.72% from MWAR, and 25% from HWAR. Around 41% of our sample had access to improved sanitation as per this definition.
Nearly 31% of the sample belonged to the lowest asset class, around 55% belonged to the middle asset class, and the remaining 30% belonged to the highest asset class. The majority of our sample belonged to the Hindu religion (79%), followed by Islam (16.5%), and 73% resided in rural areas. In our sample, around 30% of mothers had no formal schooling, 14% had completed primary school, 46% completed secondary school, and around 10% attained higher education (Table 1).
In our sample, 36.2% of children aged 6 to 23 months were stunted and only 14.4% of children achieved MDD (Table 1). A total of 14.7% of the children had at least 1 episode of diarrhea in last 2 weeks. Mean HAZ of children aged 6 to 23 months was −1.35 ± .0105 and mean dietary diversity score was 1.85 ± .0109.
Table 2 gives the percentage incidence of stunting and access to MDD as also average HAZ and dietary diversity scores of children aged 6 to 23 months by household water access and regional water availability. Proportions of stunted children were 30.5%, 35.0%, and 38.7% in households with optimal, intermediate, and low water access, respectively. Average HAZ among children in these households is −1.09, −1.30, and −1.49, respectively. Proportions of children achieving MDD were 18.1%, 14.9%, and 13.3% in households with optimal, intermediate, and low water access. Average dietary diversity scores for children in these households were 2.08, 1.88, and 1.79, respectively. Proportions of stunted children were the highest in LWAR at 38.4% and is the lowest in HWAR at 30.8%. Corresponding values for children achieving MDD were 7.5% and 19.8%. Average HAZ were −1.17, −1.30, and −1.48, respectively, in households located in HWAR, MWAR, and LWAR. Average dietary diversity scores among children of these households were 2.14, 1.96, and 1.58, respectively.
Summary of Nutrition Indicators for Children Aged (6-23 months), by Household Water Access and Regional Water Availability.
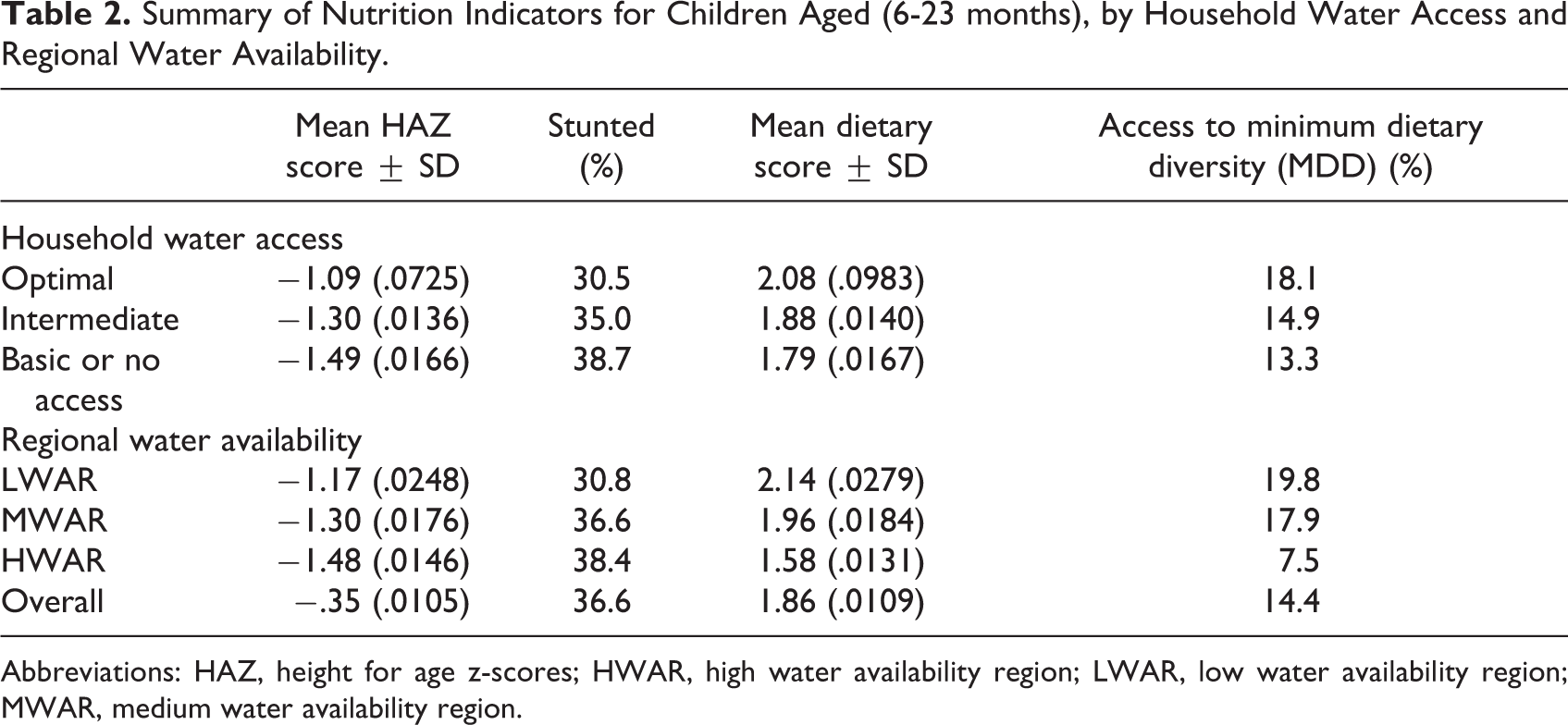
Abbreviations: HAZ, height for age z-scores; HWAR, high water availability region; LWAR, low water availability region; MWAR, medium water availability region.
Effect of Household Water Access and Regional Water Availability on Child Stunting and Mediating Variables
Table 3 gives odds ratio obtained from GSEM for our dependent variable child stunting and the 3 mediating variables. The odds ratios for all covariates are given only for the outcome and the main mediating variable, that is, child’s achievement of MDD. For the other 2 mediating variables (household’s access to sanitation and child’s experience of diarrhea), odds ratio of only our key explanatory variables (household water access and regional water availability) are presented.
Generalized Structural Equation Modeling Estimates for Overall Model (Figure 2) Predicting Key Nutrition Outcome of Child Stunting and Mediating Factors of Access to MDD, Experience of Diarrhea, and Access to Improved Sanitation.
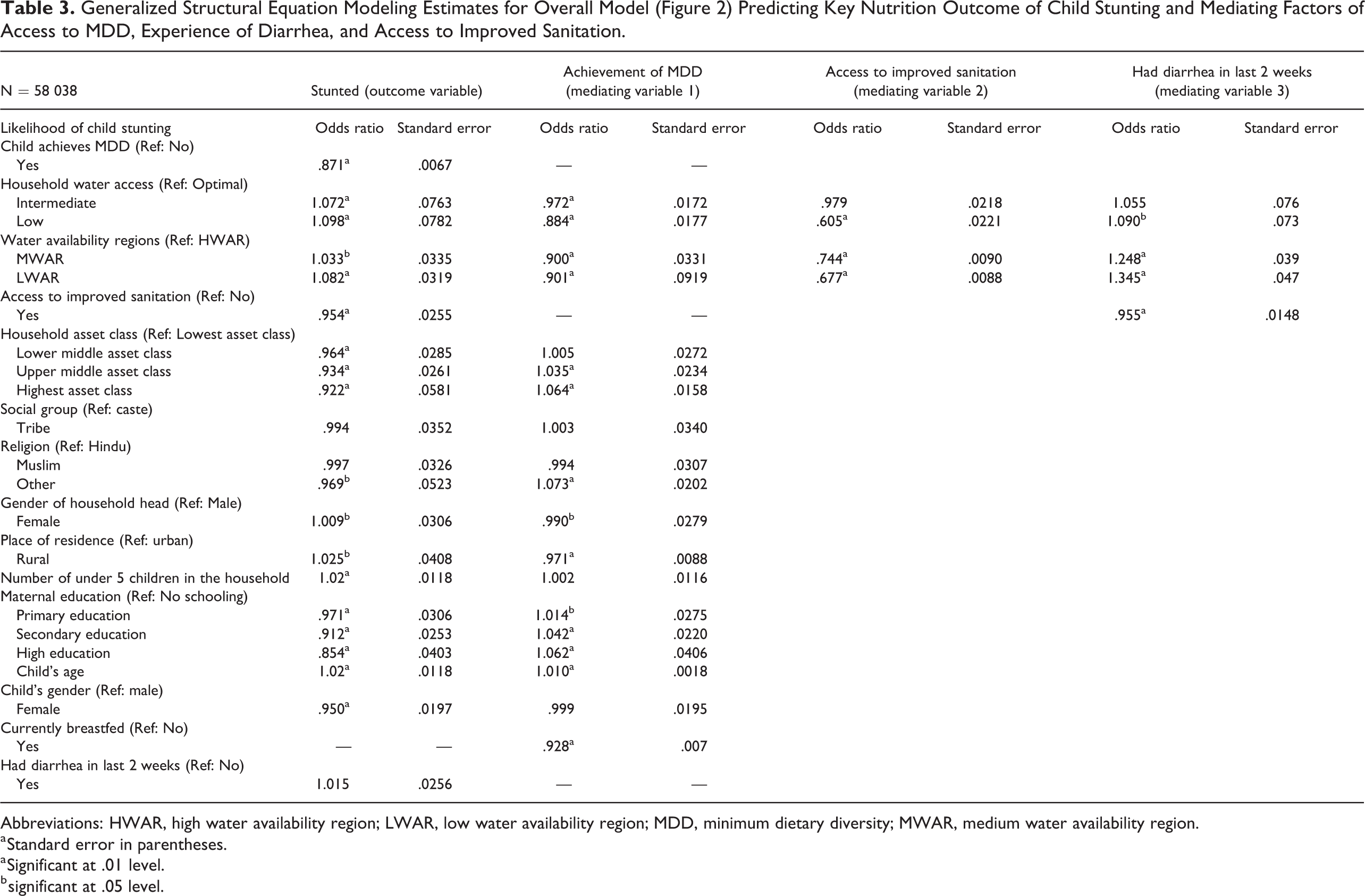
Abbreviations: HWAR, high water availability region; LWAR, low water availability region; MDD, minimum dietary diversity; MWAR, medium water availability region.
a Standard error in parentheses.
a Significant at .01 level.
b significant at .05 level.
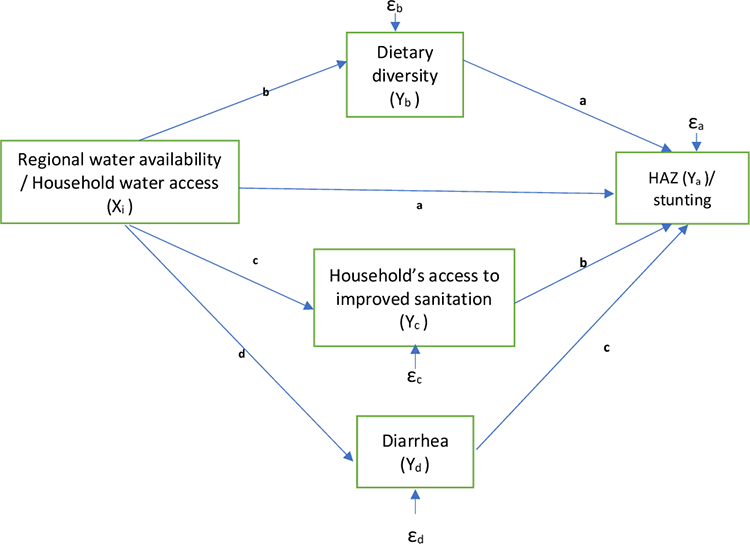
Proposed mediation pathways between water availability and access, and children’s Height for age. z-scores or stunting outcomes.
Our key explanatory variables—household’s access and regional water availability appear as statistically significant. As compared to a child in a household with optimal access to water, a child in a household with low access to water was nearly 10% more likely to be stunted, and a child in a household with intermediate water access was more likely to be stunted by approximately 7%. Furthermore, a child from LWAR was more likely to be stunted by around 8% than a child from HWAR, and a child from MWAR was more likely to be stunted by around 3%.
Child stunting was also significantly associated with our main mediating variable, that is, child achievement of MDD. A child who had achieved MDD was around 13% less likely to be stunted than a child having suboptimal diet. Furthermore, child achievement of MDD was also significantly associated with household water access as well as regional water availability. A child in household with intermediate water and low water access was less likely to achieve MDD by nearly 3% and 12%, respectively, than a child in household with optimal water access. A child from MWAR and LWAR was less likely to achieve MDD by 3% and 9%, respectively, compared to a child from HWAR.
Our second mediating variable, household access to improved sanitation, was also significantly associated with child likelihood of being stunted and reduced a child’s odds of being stunted by nearly 5%. Access to improved sanitation was significantly though partially associated with household water access (Table 3). Compared to household with optimal water access, a household with low water access was 39% less likely to have access to improved sanitation. Similarly, households located in HWAR were around 25% and 33% more likely to have access to improved sanitation than those in MWAR and LWAR.
Our third mediating variable, child experience of diarrhea in the last 2 weeks, was significantly associated with the likelihood of stunting among children, but the size of effect was very small (1%). Low household access to water was significantly associated with 9% increase in child’s experience of diarrhea, as compared to household’s optimal access to water. Household’s location in MWAR and LWAR was associated with 25% and 34% increase in child’s likelihood of experiencing diarrhea compared to in households located in HWAR. Household’s access to improved sanitation was associated with reduction in child’s likelihood of experiencing diarrhea by 5%.
Among other covariates, household asset class was positively and significantly associated with both stunting and MDD. A child in a household from the lower middle, upper middle, and highest asset class was less likely to be stunted by 4%, 7%, and 8%, respectively, than a child in a lowest asset household. A child in upper middle and highest asset class households was 3.5% and 6.4% more likely to achieve MDD. Maternal education was significantly associated with child stunting as well as achievement of MDD. As compared to non-educated mothers, maternal education of primary, secondary and higher level was associated with a decrease in child’s likelihood of being stunted by 3%, 9%, and 15%, respectively, and increase in child’s likelihood of achieving MDD by 1.4%, 4.2%, and 6.2%, respectively. Likelihood of achieving MDD was around 8% lower among currently breastfed children compared with those who had been fully weaned.
Among demographic variables, child’s age, rural residence, and number of under-5 children in household were significantly associated with incidence of stunting and MDD among children. There was no significant difference between a child’s likelihood of being stunted and of achieving MDD, across caste or tribe. Religion did not have a significant association with a child’s likelihood of being stunted but was associated with likelihood of achieving MDD, which was around 7% higher among children belonging to “other” religious groups compared to the Hindus.
Water Insecurity Affects Child Stunting Through Multiple Mediating Pathways Including Dietary Diversity
Table 4 gives direct effect of household water access and regional water availability on a child’s likelihood of stunting. It also gives the indirect effect of household water access and regional water availability on likelihood of child stunting, as mediated by a child’s achievement of MDD, experience of diarrhea, and access to improved sanitation, separately as well as simultaneously. The coefficients are given as log of odds ratio. Here it is suffice to notice that the direct effect of household water access on a child’s likelihood of stunting was significant at .01 level of significance. The direct effect of low regional water availability as compared to high regional water availability on a child’s likelihood of being stunted was not significant statistically, though the indirect effect was significant. This implies that the effect of low regional water availability on a child’s likelihood of stunting was primarily mediated by other variables.
Direct and Indirect Effects of Household Water Access and Regional Water Availability on Child’s Likelihood of Stunting as Mediated by MDD, Access to Improved Sanitation, and Experience of Diarrhea.a
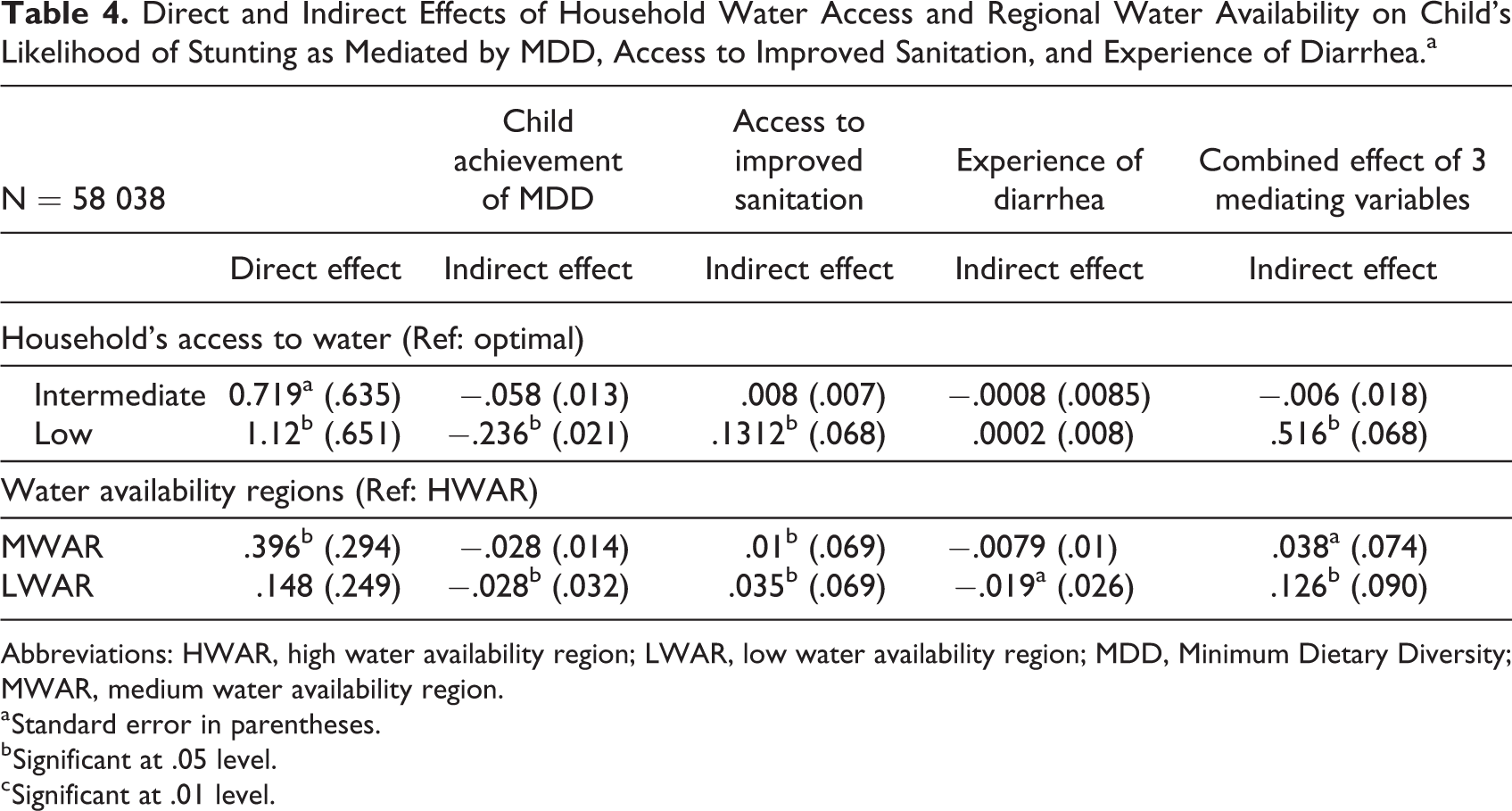
Abbreviations: HWAR, high water availability region; LWAR, low water availability region; MDD, Minimum Dietary Diversity; MWAR, medium water availability region.
a Standard error in parentheses.
b Significant at .05 level.
c Significant at .01 level.
The indirect effect of household water access as mediated through MDD was statistically significant for households with low water access when compared to those with optimal water access but not for households with intermediate water access. Similarly, the indirect effect through MDD was statistically significant only for children in households located in LWAR as compared to households located in HWAR. Indirect effect of regional water availability and household water access as mediated through household access to sanitation was also significant. Indirect effect as mediated through child experience of diarrhea was insignificant except in case of LWAR. The combined indirect effect of MDD, sanitation, and diarrhea was significant for all levels of regional water availability but only for low level of household water access.
Figure 3 demonstrates the relative contribution of indirect or mediated effect of household water access and regional water availability on child’s likelihood of stunting. Around 9% of the effect of intermediate water access compared to optimal water access on a child’s likelihood of stunting was mediated by child achievement of MDD. Very low proportion of this effect was mediated by sanitation or experience of diarrhea. This indirect effect was considerably greater for a household’s low water access compared to optimal water access. Child achievement of MDD alone mediated nearly 27% of total effect of low water access whereas access to improved sanitation mediated 10.5% of the effect. The indirect effect of MWAR as compared to HWAR through child’s achievement of MDD was 7.6% and through sanitation was nearly 3%. The indirect effect of LWAR as compared to HWAR was highest through MDD, which mediated 23.3% of the total effect. Household access to sanitation accounted for 19% of the effect that being located in LWAR had on child stunting as compared to in HWAR. Diarrhea also mediated considerable proportion (around 15%) of the effect of LWAR versus HWAR, on child’s likelihood of being stunted. Overall, around 30% of the total effect of household water access on a child’s likelihood of being stunted is indirect and mediated, primarily through child achievement of MDD and household access to sanitation and to a small extent by child experience of diarrhea.
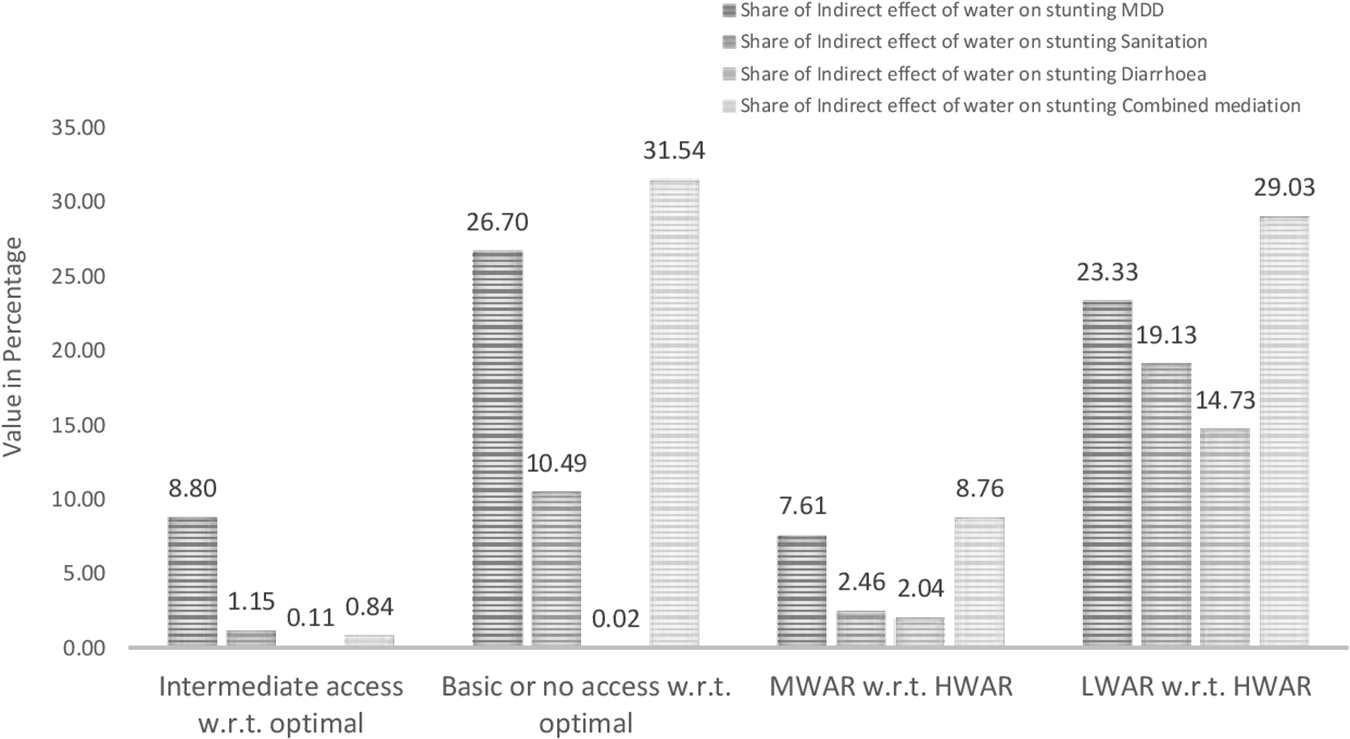
Share of indirect effect of relative water access and regional water availability on child stunting as mediated by child’s achievement of MDD, experience of diarrhea, and household’s access to improved sanitation.
As described in the methodology section, we ran a separate SEM wherein child HAZ score and child dietary diversity score are continuous outcome and mediating variables. Based on the SEM results, Figure 4 shows predicted values of child’s HAZ score with and without mediation by child’s dietary diversity score by household water access and across regional water availability. The divergence in behavior of the 2 predicting lines reflects moderating effect of water availability context on dietary score’s mediation of the effect of household water access on child’s HAZ.
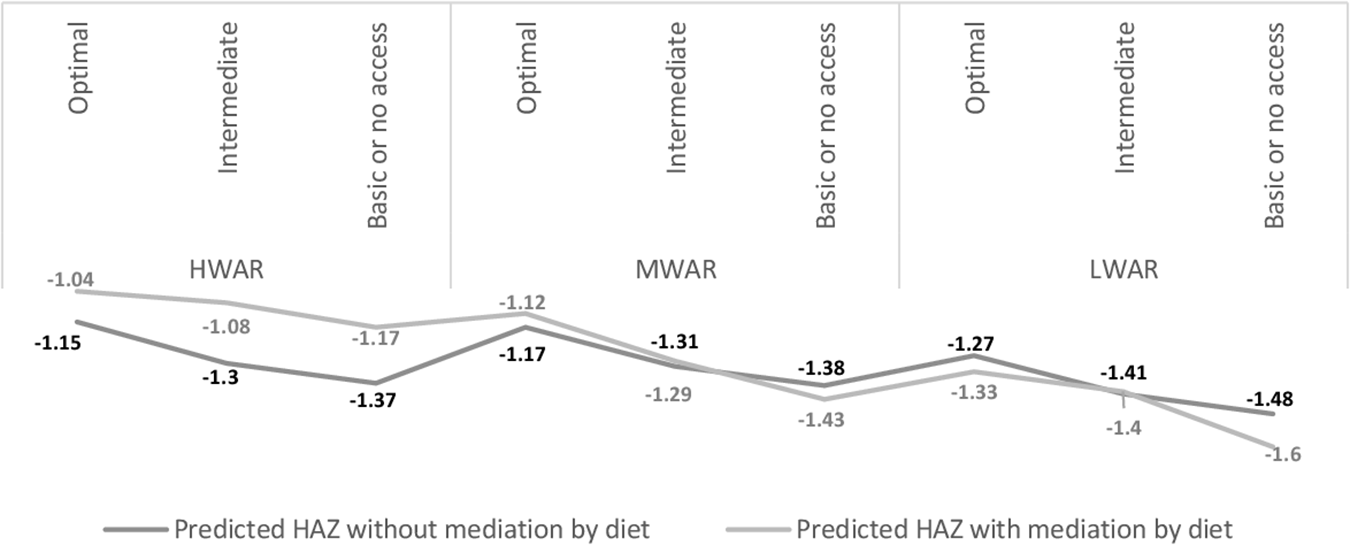
Predicted values of child’s height-age z-score (HAZ) without and with mediation by child’s dietary diversity score by household water access and across water availability regions.
In HWAR, predicted HAZ with mediation by dietary diversity score is higher than predicted HAZ without mediation, while in LWAR predicted HAZ with mediation is lower than predicted HAZ without mediation. The effect of mediation by dietary diversity score in predicting child HAZ is relatively narrow in MWAR, as also seen in Figure 3. In HWAR, the association between household water access and child HAZ is positively mediated by dietary diversity score. However, in LWAR, the mediation by dietary score is negative. This implies that in context of greater overall water availability, dietary diversity score reinforces an increase in child HAZ and in limited water availability context, dietary diversity score has dampening effect on child HAZ. This is because child dietary diversity score itself is significantly and positively associated with household water access and regional water availability (Table 3).
Discussion
Our analysis explicates an additional pathway linking household water access and child stunting, by identifying and estimating the potential mediating effect of child dietary diversity. The more often explored “WASH mechanism” encompasses improved nutrition through reduction in diarrheal disease due to decline in fecal contamination of the environment, reduced exposure to enteric infections, reduced prevalence of anemia, and reduced time spent fetching water and caring for sick children, among others. 24 However, our analysis unfolds that household water access can have a parallel pathway to affect child stunting through affecting a child’s access to dietary diversity, a crucial component of child nutrition, even after controlling for the role of sanitation in the estimation model. Our analysis reveals that not only does water (along with sanitation and hygiene as WASH) affects child nutrition, but water through sanitation and hygiene has additional effects on nutrition. This is because optimal access to water or proximity to source of water may allow for more hygienic use of a toilet facility, for example, pour flushing, cleaning, post-defecation handwashing, and may improve the frequency of hygiene behavior such as handwashing before cooking. 78 -80 This ultimately has positive effect on child nutrition.
Our findings thus confirm that household’s suboptimal access to water can affect child stunting (as a marker of the outcomes of complex nutritional processes) through multiple parallel pathways. In fact, the association between water and child HAZ (stunting) is more of an indirect nature, mediated through child dietary diversity as well as access to sanitation. This finding aligns with the existing literature that gives an inconsistent but intriguing picture on significant association between access to water and stunting 23 and has fueled a fresh debate mulling over the relevance of huge water (sanitation and hygiene) or WASH interventions for gains in child nutrition (WHO Position Paper). Our analysis partly explains this apparent inconsistency by showing that the role of water toward child HAZ/stunting is more indirect, which is often not accounted for in existing literature that only focuses on direct mechanisms. Since water access itself affects access to sanitation and hygiene, it is likely that the simultaneous presence of the 3 variables (WASH) in models may suppress the contribution of water, the impact of which is channelized also through sanitation and hygiene.
Furthermore, when mediation is accommodated in the model, household water access and regional water availability have a direct significant association with child stunting. However, in the context of low water access and availability, it is the indirect effect mediating particularly through child’s achievement of MDD that becomes significantly predominant. This is likely because lack of adequate water is found to constraint the preparation of minimum diversified food for children, especially if it has high water content or requires longer boiling time. 81,82 Insufficient water availability has been qualitatively linked with a decrease in the quantities and types of foods prepared for the household 42,83 and has been reported to lead women toward increased instances of breastfeeding when water to prepare complementary foods is unavailable. 49 Since it is usually women who are responsible for both child care and household water management, suboptimal water access can negatively affect dietary diversity by diverting the caregiver’s time away from child care and feeding activities. 49 Collectively, these mechanisms deserve further attention to unravel the relationship between breastfeeding, dietary diversity, and caregiver time in the context of water insecurity.
Additional findings reveal that the mediating role of dietary diversity in the association between household water access and child’s HAZ score was also moderated by regional water availability contexts. In HWAR, mediation by dietary diversity reinforced the positive effect of household water access on a child’s HAZ score. However, in the context of LWAR, mediation by dietary diversity further accentuated the negative effect of suboptimal water access on child HAZ. This also explains relatively higher predicted HAZ score of a child in HWAR than in MWAR and LWAR. In HWAR, a child’s dietary diversity could be higher due to a household’s relatively higher access to diversified food facilitated by water-intensive agricultural and allied activities—for example, through diversification and multicropping involving water-rich food and vegetables such as soybean, groundnut, maize, and so on. 38 Such agricultural and allied practices have been found to improve child’s anthropometry in the context of Malawi. 84 Greater availability of surface water in the neighborhood raises the likelihood of people having water-based animal product in their diet such as freshwater fish, which are among the most water-intensive consumption products. 85 Moreover, regions with greater water availability are likely to make these products relatively easily accessible even to low asset households, thus raising the probability of child’s receiving minimum dietary diversity and lowering the probability of such outcomes as stunting.
Our finding has policy implications. Improvement in household water access can have a direct and significant effect on reducing a child’s likelihood of stunting, even when the direct association between water (along with sanitation and hygiene) may be statistically insignificant on average. 19,20 This direct effect on stunting might come from access to safe drinking water, which has immediately positive effect on child health. But these findings suggest improvements in water access—whether hard solutions like digging wells and putting in pipes or soft solutions like improved community water governance—also affects child stunting through improvements in children’s dietary diversity. This provides additional points of intervention for nutrition and child growth interventions in water-insecure households or communities. It also suggests that including water impacts on children’s diets might broaden the conceptual structure of WASH, 22 wherein dietary diversity could be additional pathway to children’s improved well-being.
Limitations
Our measure of household water access is based on sources of water, which does not account for water quality parameters. The cross-sectional nature of the data is another limitation that constraints inter-temporal prediction of the relationships being tested. The DHS for India does not give data on who in the household is responsible for fetching water or how is the time allocated across activities such as household water management or childcare activities; this limits our understanding of how intra-household arrangements are implicated in the studied mechanisms. Finally, we would have liked to include behavioral data to reflect household- and child-specific practices related to water, sanitation, and hygiene; we hope future studies will include these.
Conclusion
Household water status consistently associates with many aspects of child nutritional status, and this is often explained in relation to sanitation/hygiene mechanisms that increase diarrheal loss of nutrients. The patterning is less clear with stunting, as a longer term marker of nutritional well-being. Using data from a nationally representative sample from India, we demonstrate that low water access can have additional indirect effects on a child’s height for age Z-scores outside of sanitation/hygiene mechanisms, mediated by the suppressive effect on child dietary diversity created by suboptimal household water access. Our novel analysis supports the suggestion that water-based interventions should improve children’s longer term nutritional outcomes in water-insecure households and in water-scarce regions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.