
Abstract
Background:
The trend of unhealthy lifestyles is increasing among adolescents and has been associated with the rising burden of noncommunicable diseases (NCDs). However, specific determinants of unhealthy lifestyles among adolescents in low- and middle-income countries remain limited.
Objective:
To investigate the relationships of child-, parents-, and environment-associated determinants with diet quality, physical activity, and smoking habits among low-socioeconomic urban adolescents.
Methods:
A cross-sectional study involving 238 adolescents aged 11 to 17 years was conducted in Jakarta, Indonesia. Adolescents and their parents were interviewed to assess the determinants of healthy lifestyles that included diet quality, physical activity, and smoking habits. Diet and physical activity were quantified using the Diet Quality Index for Adolescents (DQI-A) and Physical Activity Questionnaire for Older Children (PAQ-C), respectively. Multiple regression was used to determine the β coefficients and odds ratios predictive of healthy lifestyles.
Results:
Mean scores of DQI-A and PAQ-C were considered low (33.5% ± 8.9% and 2.1 ± 0.5, respectively). Overall, 17.6% of adolescents were smokers, with 88% of these being males. Predictors of diet quality were child- (age, gender) and environment-associated (house size, access to a computer) determinants with β coefficients of −6.52 to 3.26. The PAQ-C score was associated with child- (female) and environment-associated (living area) determinants with β coefficients of −0.45 and 0.14, respectively. Younger adolescents and females were protective factors for smoking. Parents-associated determinants were not associated with any lifestyle indicators.
Conclusions:
Child- and environment-associated determinants were predictors of healthy lifestyles among adolescents. Thus, personal empowerment and environment transformation are needed to facilitate a healthy lifestyle and reduce the burden of NCDs among adolescents.
Introduction
Adolescents are a unique population and have become the focus of attention as a key to achieving Sustainable Development Goals. Adolescence is characterized by a strong tendency to experiment with new behavior, enabling them to be the drivers of change, including the potential transformation of the countries food system. 1,2 However, they also tend to be more adaptable to the current rapid transition of the food environment and susceptible to advertisements in the millennial era. 3 This transition has led to significant social and cultural changes, including the increased use of the Internet in various daily activities.
The massive introduction of online activities coincides with the rise of unhealthy and sedentary lifestyles, such as poor diet quality, less physical activity, and smoking among adolescents, especially in urban communities. The trends of child and adolescent obesity have accelerated in many Asian and African countries, 4 including Indonesia. According to the 2013 Indonesian National Health Research (as so called RISKESDAS) data, the rates of overweight or obesity among adolescents aged 13 to 15 years and 16 to 18 years were 10.8% and 7.3%, respectively. 5 Compared to the RISKESDAS data in 2010, there was an increase of 8.3% and 5.9% for these age-groups. 6 The trend over 3 years in Indonesia is comparable to the global trend of increased obesity in children and adolescents over 42 years, rising 4.9% percentage points in girls and 6.9% in boys. 4 The trend is projected to continue as Indonesian adolescents tend to have a high consumption of unhealthy foods (ie, western-style fast foods and convenience foods with excessive amounts of sodium). 7 In addition to poor diet quality, smoking habits also contribute to adolescents’ poor quality of life, as 19.4% of Indonesian teenagers are active tobacco smokers. 8 This is of added concern considering the rise in smoking among the general population in Indonesia compared to other Southeast Asia countries. 9 Lack of physical activity is also a problem in Indonesian youth, with 24.5% to 33.8% spending ≥ 3 hours per day on sedentary behaviors. 10 All these unhealthy lifestyles behaviors can increase the risk of noncommunicable disease (NCD) in adolescence, such as diabetes and cardiovascular diseases, and even cancer, and reduce the productivity of the young generation. 11,12 Long-term impacts may include lower economic performance during adulthood, adult-onset NCDs, and an estimated 70% of premature deaths. 13 -16
As adolescence is the transition phase to adulthood and includes growing capacity for decision-making, more diverse factors may influence changes in their lifestyle. Recently, a conceptual framework identifying factors contributing to NCDs among adolescents and later life has highlighted a comprehensive and integrated approach comprising the individual, family, peers, community, school, and societal determinants. 11 This aligned with the data from the previous studies that demonstrated various influences on healthy lifestyle behaviors among adolescents apart from child- or individual-associated (ie, gender) determinants, such as parental education, income status, living area, and media exposure. 17 -20 Although data in upper-middle and high-income countries are available to identify parents- and environment-associated determinants, studies in low- and middle-income countries are still lacking. Therefore, we investigated the relationship of child-, parents-, and environment-associated determinants with diet quality, physical activity, and smoking habits among urban adolescents in Jakarta, Indonesia, a setting relevant to urban centers and mega-cities in lower-middle-income countries.
Methods
Study Population and Design
This cross-sectional study was a population-based investigation of adolescents’ nutritional and lifestyle status (diet quality, physical activity, and smoking habits), carried out in 2 selected urban regions representing the nonflooding and flooding areas in East Jakarta, Indonesia, from January to March 2019. These areas represent distinct geographical characteristics of Jakarta province and encompass different risk factors. The current study was conducted as a part of the 10-year follow-up study of a randomized, double-blind controlled trial of probiotics and calcium supplementation during childhood, as described elsewhere. 21,22 Data were collected from 238 adolescents aged 11 to 17 years and their parents. Adolescents were excluded if they did not complete all questionnaires or had communication difficulties (ie, special needs).
All participating adolescents, including their parents, were interviewed to assess the child- (eg, age, gender), parents- (eg, parental education, financial distress), and environment-associated (eg, living area, having access to a computer) determinants of healthy lifestyles. Financial distress as one of the parent-associated determinants was evaluated by using open-ended questions. It is defined as a condition where the monthly spending is larger than the income. 23 Data on family and house sizes and access to a computer at home were obtained from the Abbreviated Early Adolescent Home Observation and Measurement of the Environment ((EA-HOME-A) Inventory. Diet quality was assessed using the Diet Quality Index for Adolescents (DQI-A) based on 2 nonconsecutive 24-hour dietary recalls. Physical activity was quantified using the Physical Activity Questionnaire for Older Children (PAQ-C).
Data Collection
Trained field enumerators interviewed each participant for sociodemographic characteristics, PAQ-C, and 24-hour recall. In addition, we used 2 nonconsecutive 24-hour recalls to assess dietary intake representing the food intake on weekdays and weekends. Food models and a book displaying the portion size of foods were used to visualize and aid in estimating portion sizes.
Diet Quality Index for Adolescents
The DQI-A assessment was based on food-based dietary guidelines for adolescents, which put forward 3 basic principles for a healthy and balanced diet comprised of dietary quality, dietary diversity, and dietary equilibrium. 24 The DQI-A scoring utilized 9 recommended food groups consisting of (1) water; (2) bread and cereals; (3) grains and potatoes; (4) vegetables; (5) fruit; (6) milk products (7); cheese; (8) meat, fish, eggs, and substitutes; and (9) fat and oils.
Dietary quality calculated from the DQI-A assessment implied whether the adolescent made the optimal food quality choices within a food group. It was represented by a “preference group” (eg, cereal/brown bread, fresh fruit, fish) with a score of 1 for each food, an “intermediate group” (eg, white bread, minced meat) with a score of 0, and a “low-nutrient, energy-dense group” (eg, soft drinks, sweet snacks, chicken nuggets) with a score of −1. The dietary diversity described the degree of variation in the diet. This diversity component was obtained by giving points ranging from 0 to 9 when at least one food serving in a recommended food group was consumed. Finally, dietary equilibrium was scored by calculating the difference between the dietary adequacy (the percentage of the minimum recommended intake for each of the main food groups, truncated to 1) and the dietary excess (the percentage of intake exceeding the upper level of the recommendation, truncated to 1 if larger than 1 and truncated to 0 when below 0).
The total score of DQI-A and each component’s scores were represented as percentages. The dietary quality component ranged from −100% to 100%, while dietary diversity and dietary equilibrium ranged from 0% to 100%. To compute the DQI-A score, the mean of these components was calculated. The DQI-A score ranged from −33% to 100%, with a higher score reflecting a better diet quality. The score was calculated for each day, and a mean of the daily scores was taken as a total index score of the individual.
Physical Activity Questionnaire for Older Children
The PAQ-C is a 9-item, 7-day recall of activity designed for elementary and middle school children’s physical activity assessment in a field-based setting. 25 The children were asked to recall their participation in the activities in the last 7 days. Their responses were scored between 1 and 5, based on a rubric, for each of the 9 items obtained. The mean of these 9 items was calculated as the final PAQ-C score, in which a higher score implies a more physically active adolescent. A 10th item, which was not included in calculating the activity score, clarified whether the adolescent was sick or otherwise prevented from engaging in regular physical activity. These conditions might alter the daily physical activities of the participant, and the questionnaire would then be repeated in the next week.
Ethical approval
Ethical permission for this study was obtained from the Ethics Committee of the Faculty of Medicine, Universitas Indonesia (No. 18-10-1170). Separated permission was also obtained from the Jakarta provincial government and health office. In addition, all of the study participants and their parents provided written, signed informed consent before the data collection process. The protocol was registered with clinicaltrials.gov as NCT04046289.
Statistical analysis
All analyses were performed using Statistical Package for the Social Sciences version 20.0. Descriptive characteristics were obtained by calculating means and standard deviations (SDs) for continuous variables and percentages for categorical variables. Multiple linear regression was used to analyze the association between the child-, parents-, and environment-associated determinants with DQI-A and PAQ-C scores of the participants. Effect sizes were calculated by dividing the β coefficient by the pooled SD of the outcomes. To evaluate the association of the determinants with smoking status, we used the multiple logistic regression with simultaneous entry method and presented the odds ratio (OR).
Results
The sociodemographic characteristics of the participants are presented in Table 1. Participants were equally distributed by gender. About one-third of the adolescents were from households wherein parents had less than 9 years of parental education. Although this study was conducted in low-socioeconomic communities with only 34% of participants living in a better nonflooding area, most participants (79.8%) had no financial distress.
General Sociodemographic Characteristics of Adolescents Living in Low Socioeconomic Urban Areas of East Jakarta.a
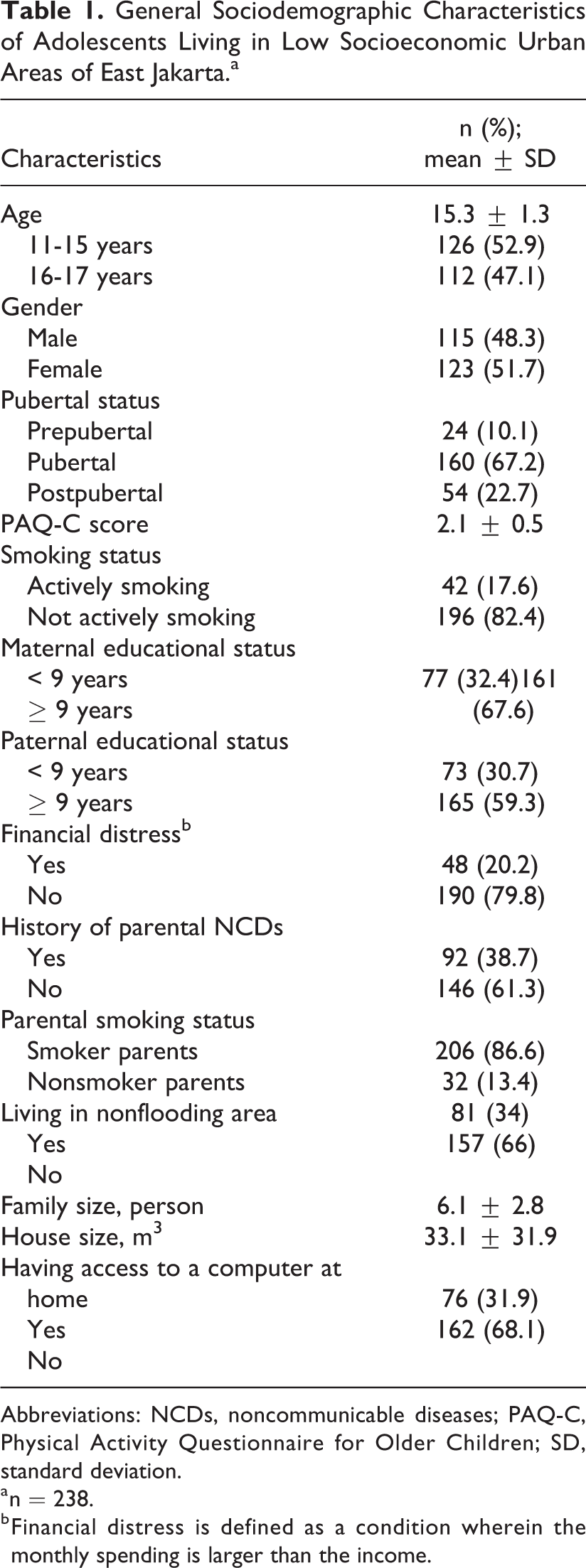
Abbreviations: NCDs, noncommunicable diseases; PAQ-C, Physical Activity Questionnaire for Older Children; SD, standard deviation.
a n = 238.
b Financial distress is defined as a condition wherein the monthly spending is larger than the income.
Based on the dietary assessment, only 27.7% of the adolescents consumed fruits, 17.6% consumed milk products, and 7.9% consumed cheese regardless of the amount in at least 1 of the 24-hour recalls. Nonetheless, we found 73.1% of adolescents who consumed vegetables in at least one recall. The mean DQI-A score in our adolescents was 33.5% ± 8.9%. As seen in Table 2, the mean dietary quality and diversity scores were 31.7% ± 17.7% and 57.4% ± 8.7%, respectively. Meanwhile, the mean dietary adequacy, excess, and equilibrium scores were 41.8% ± 6.4%, 24.6% ± 16.8%, 11.2% ± 15.6%, respectively. The mean PAQ-C score among participants was 2.1 ± 0.5, lower than 2.73 as the cutoff point to discriminate > 60 minutes of moderate-to-vigorous physical activity (MVPA) as recommended for adolescents (Table 1). Of 238 participants, 17.6% of the adolescents were smokers, and 88.1% of these smokers were males.
Diet Quality Index for Adolescents Living in Low Socioeconomic Urban Areas of East Jakarta.a
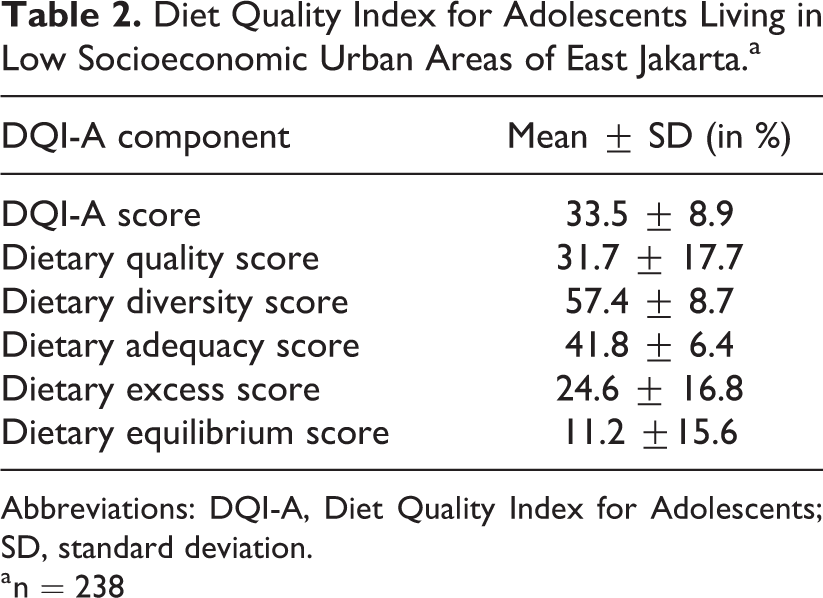
Abbreviations: DQI-A, Diet Quality Index for Adolescents; SD, standard deviation.
a n = 238
Table 3 shows the results from multivariable linear regressions including the β coefficient of each determinant with its 95% CI. Various diet quality components of DQI-A were associated with child- and environment-associated determinants. Age, gender, house size, and access to a computer were significant determinants of diet quality. The dietary quality score of female adolescents was 6.52% or 0.37 SD lower than males. Although the dietary diversity score was inversely associated with house size, the β coefficient was extremely small (0.04%). Older adolescents and adolescents with access to a computer had a score of 0.71% and 3.26% higher in dietary adequacy scores, respectively.
Multiple Regression Model of Determinants Predicting Each Diet Quality Component among Adolescents Living in Low Socioeconomic Urban Areas of East Jakarta.a
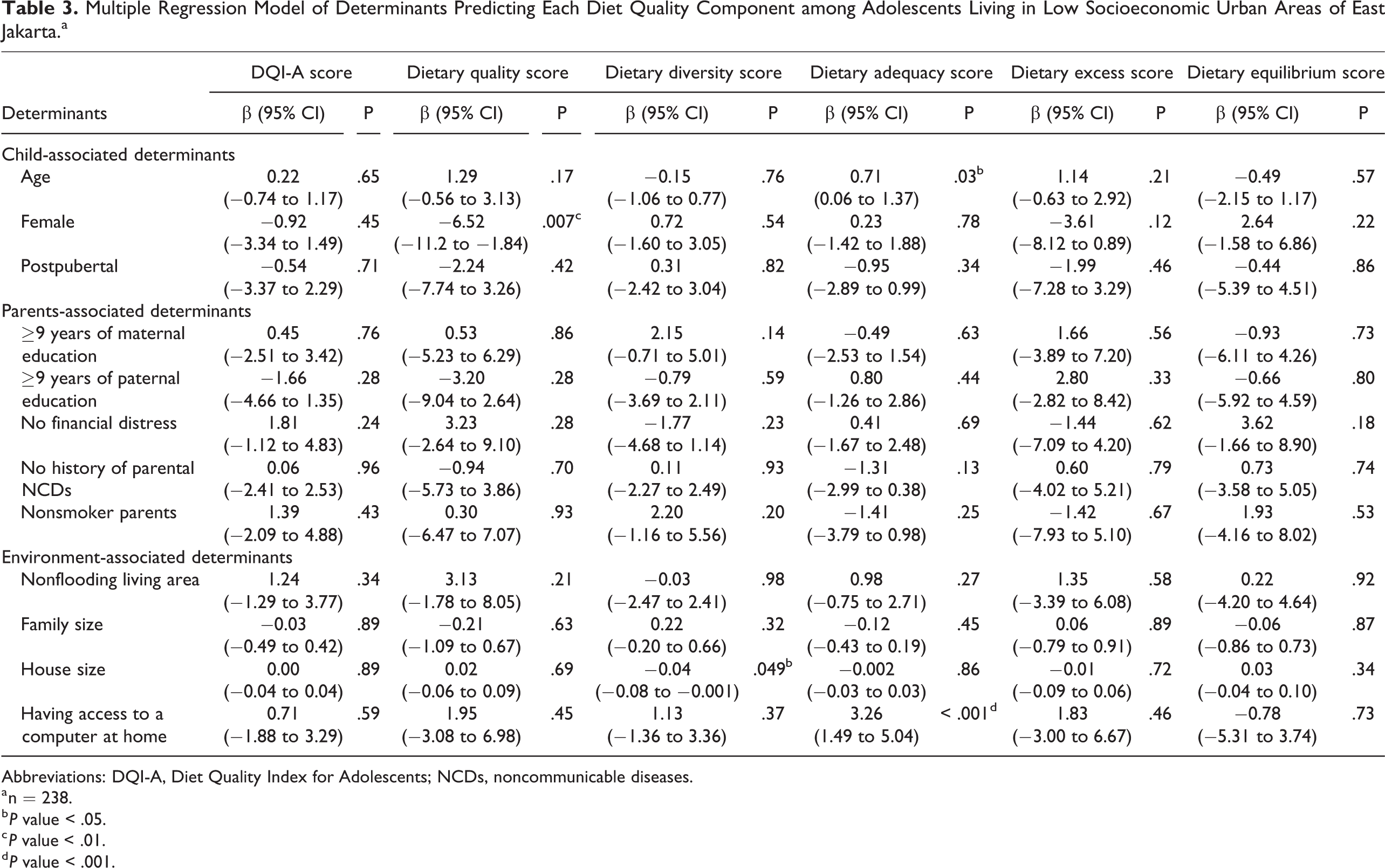
Abbreviations: DQI-A, Diet Quality Index for Adolescents; NCDs, noncommunicable diseases.
a n = 238.
b P value < .05.
c P value < .01.
d P value < .001.
Table 4 shows the β coefficient of each determinant associated with the PAQ-C score and the ORs of determinants with smoking based on the multiple regression models. Similar to the results for diet quality, we found that child- and environment-associated determinants were significantly associated with physical activity and smoking habits. Females had a lower score of PAQ-C by 0.45 points as compared to male adolescents. Participants who lived in the nonflooding area scored 0.14 points higher in PAQ-C than adolescents in the flooding area. We found that being male and older adolescents were associated with smoking habits. Female adolescents were associated with the habits of not smoking (OR 17.4), and age was inversely associated with the habits of not smoking (OR 0.46).
Multiple Regression Model of Each Determinant Predicting Physical Activity and Smoking Habits among Adolescents Living in Low Socioeconomic Urban Areas of East Jakarta.a
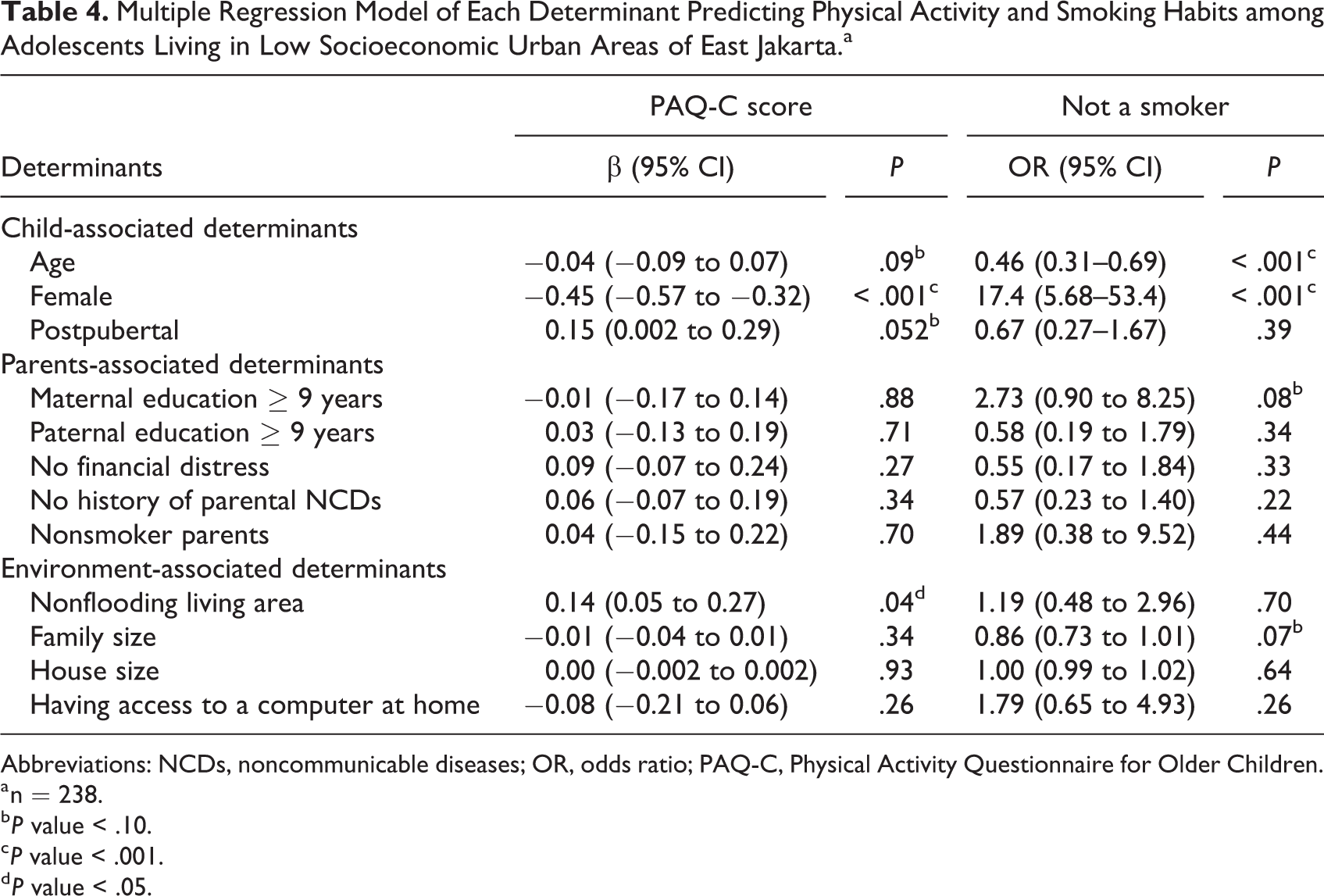
Abbreviations: NCDs, noncommunicable diseases; OR, odds ratio; PAQ-C, Physical Activity Questionnaire for Older Children.
a n = 238.
b P value < .10.
c P value < .001.
d P value < .05.
Based on Table 4 and Figure 1, the gender of the participants was consistently associated with all of the healthy lifestyle indicators and had the largest effect size on physical activity and the highest ORs with regard to smoking habits. The determinant with the largest effect size on diet quality was access to a computer. This study found no apparent association between parents-associated determinants and any healthy lifestyle indicators among adolescents.
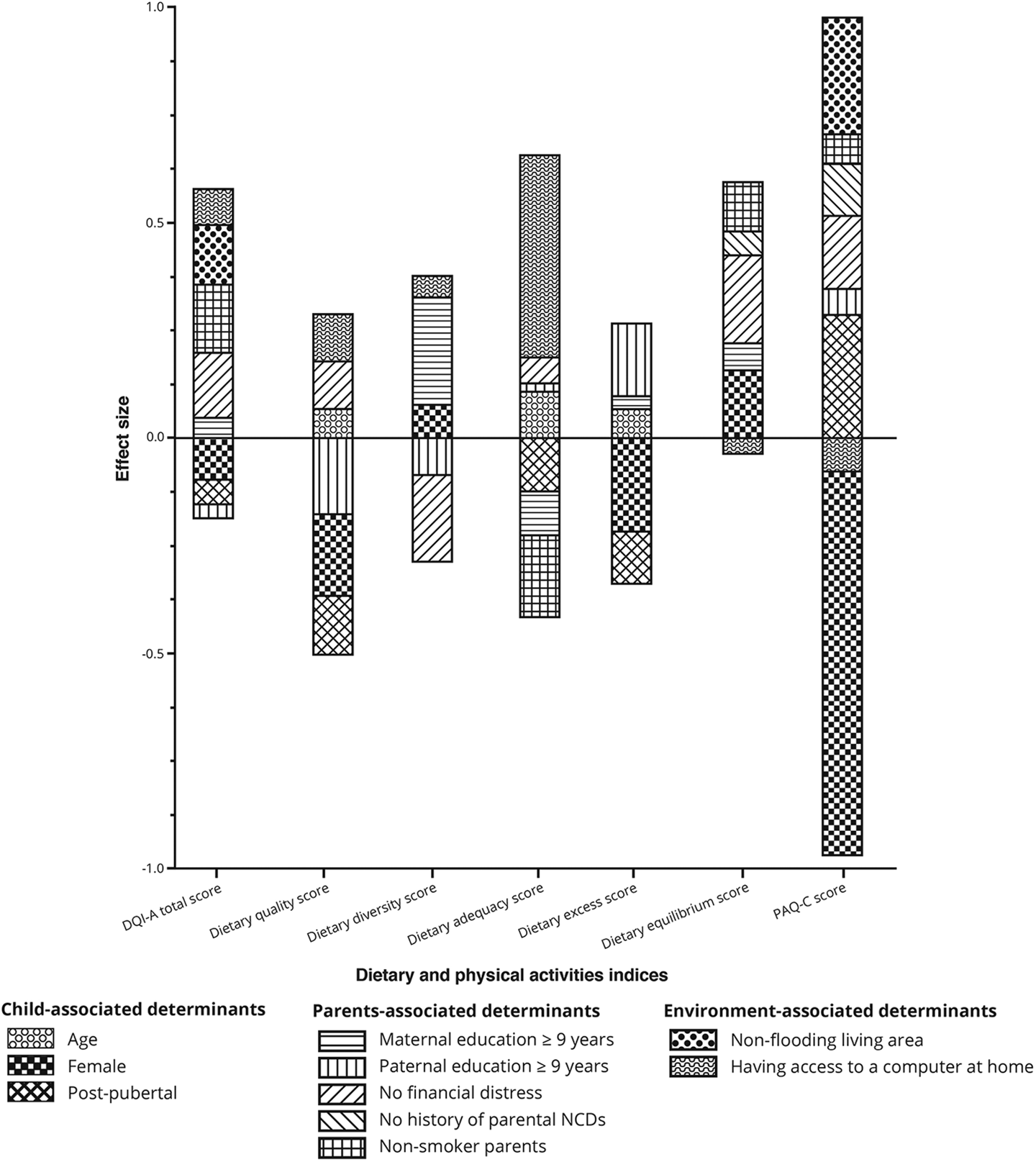
Effect Sizes of Each Determinant as the Predictors of Diet Quality and Physical Activity among Adolescents Living in Low Socioeconomic Urban Areas of East Jakarta. Effect sizes with a value less than 0.05 SD were not presented. DQI-A indicates Diet Quality Index for Adolescents; NCDs, noncommunicable diseases; PAQ-C, Physical Activity Questionnaire for Older Children; SD, standard deviation.
Discussion
The present study indicated that the Indonesian adolescent population in East Jakarta tended to have a low diet quality and less physical activity with 17.6% prevalence of cigarette smoking. Both child-associated determinants and environmental-associated determinants were found to be significant predictors of healthy lifestyles (dietary quality, physical activities and smoking habits) in adolescents. There was no apparent association between parent-associated determinants with any healthy lifestyle indicators.
Although this study was undertaken as a part of a follow-up study of a clinical trial of probiotics and calcium supplementation during childhood, a random sampling method was applied in the previous clinical trial to obtain representative samples. Diet quality was assessed by 2 nonconsecutive 24-hour recalls, which were representative for dietary intake on weekdays and weekends. More importantly, this study described various determinants of adolescents’ healthy lifestyles in low-socioeconomic urban communities. Thus, the results are essential to accelerate the implementation of health promotion in these communities.
Diet quality assessment was used to capture the complex combinations of nutrients, which might account for the synergistic effects across food groups, rather than assessing a single nutrient. 26 A previous study conducted among adolescent girls in West Java, Indonesia, found a higher score of the DQI-A by nearly 10% compared to our study, 27 but this score would still be considered low. Another study in Brazil found a lower DQI-A score compared to our findings. 28 Unfortunately, data on the DQI-A score among other middle-income countries are lacking. Two other studies assessing the diet quality of adolescents with higher DQI-A scores were conducted in high-income countries. 29,30 The mean PAQ-C score in this study was also lower than the recommended score for MVPA. 31 The combination of low diet quality and physical activity in this study may increase the risk of NCDs among adolescents. Additionally, 17.6% of adolescents were smokers, highlighting the urge to promote cardiovascular disease awareness at a younger age.
Among child-associated determinants, diet quality was associated with the age and gender of adolescents. Female adolescents had lower dietary quality scores, reflecting suboptimal food quality choices within a food group. These scores were also associated with small effect sizes in regression analysis. In contrast, several other studies found better dietary quality in females compared to males. 24,32,33 Nonetheless, a cross-sectional survey in Tunisia observed that women consumed more sweets but less red meat and soft drinks and had a higher mean moderation subscore but lower variety and adequacy. 34 A national study in Taiwan demonstrated an association between poor dietary quality with emotional disturbance in adolescent girls but not in boys. 35 This finding may hint at the need to take psychosocial factors into account to identify the most prominent child-associated determinants in dietary quality. We also found that younger adolescents were associated with lower dietary adequacy scores implying early interventions may help adolescents reach the recommended intakes for each of the main food groups. This finding was similar to another study that showed younger individuals were more vulnerable to low-quality diet. 36
House size and having access to a computer at home were significant predictors of diet quality. Although house size was inversely associated with dietary diversity, the effect size was small. On the other hand, having access to a computer at home was significantly associated with dietary adequacy score with a moderate effect size. This finding might exhibit the importance of Internet access to providing nutrition literacy among adolescents. 37
The age and gender of the participants were found to be significant predictors of physical activity and smoking habits among adolescents. Although physical activity was substantially lower in female adolescents, they were less likely to be smokers. These gender differences might be due to several factors that influence the decision-making process of a healthy lifestyle, such as the competition/ego, appearance, physical condition, mastery subscales, cues (eg, food/alcohol consumption), and other ties to social context. 38,39 In this study, younger adolescents had lower odds of being a smoker. Despite this finding, another study observed the association between earlier initiation of smoking with subsequent regular smoking. 40 Thus, the prevention of smoking habits at an earlier age should not be underestimated.
We also found a significant, albeit small, association between the characteristic of the living area (ie, nonflooding) and physical activity. Cleanliness of public open spaces (POS) and beautiful sceneries were crucial factors supporting adolescents’ physical activity in POS. 41 Nonetheless, various factors that were not evaluated in this study might be linked to our findings, such as the availability of accessible sports facilities, walkability, and destinations within walking distance. 42,43
Although no parent-associated determinants were significantly associated with healthy lifestyles among adolescents in this study, certain aspects should be highlighted to interpret these findings adequately. Several parent-associated determinants were not assessed in this study, such as parental occupational status and the home food environment involving parents (parenting style/feeding practices, food rules, parents’ perceptions of food costs). 44 Previous studies have found that the home food environment influenced children’s eating behaviors. 44,45 A study in European adolescents demonstrated a significant association between adolescents’ parental occupational status and diet quality. 46 These findings underscore the critical point of assessing parent-associated determinants beyond educational and economic status. However, it is worth mentioning that social and cultural factors influencing diet quality in everyday life are country-specific. 47 More importantly, adolescence depicts a transition phase, which might be dominantly influenced by the peer rather than the parents through modeling. 48,49
This study highlights the importance of environmental transformation to promote adolescents’ healthy lifestyles, especially those living in low socioeconomic areas. Our research highlighted that ensuring the optimum environment for supporting healthy lifestyles among adolescents is essential through the policy reform for expanded environmental context. Considering the high mobility of adolescents, aside from the home environment, schools and urban planning should be focuses of improvement. Besides hygiene practices implemented in several government programs, better access to good quality and a sustainable healthy diet and encouraging POS for physical activity are warranted. Furthermore, this study found significant associations between age and gender with particular healthy lifestyle indicators. This confirms the need to define specific target populations in promoting healthy lifestyles among Indonesian adolescents. Larger studies in low socioeconomic communities in Indonesia and other countries are needed to confirm our findings on the determinants of adolescents’ healthy lifestyles.
Conclusion
Child- and environmental-associated determinants had strong associations with healthy lifestyles among urban adolescents. Therefore, interactive and innovative interventions, such as digital platforms of personal empowerment and environment transformation, are warranted to facilitate a healthy lifestyle and reduce the burden of NCDs among adolescents.
Footnotes
Author’s Note
The study is registered with ![]() as NCT04046289. Rina Agustina, Davrina Rianda, and Evania Astella Setiawan designed and conducted the study, analyzed the data, and drafted the article. Rina Agustina and Davrina Rianda wrote the grant. Rina Agustina had primary responsibility for the final content. All authors read and approved the final manuscript.
as NCT04046289. Rina Agustina, Davrina Rianda, and Evania Astella Setiawan designed and conducted the study, analyzed the data, and drafted the article. Rina Agustina and Davrina Rianda wrote the grant. Rina Agustina had primary responsibility for the final content. All authors read and approved the final manuscript.
Acknowledgments
We thank all of the adolescents and their families, cadres, and enumerators involved in the study. We highly appreciate Dr. Anuraj Shankar for helping us in finalizing the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:This study was financially supported by a grant from the Ministry of Research, Technology, and Higher Education of the Republic of Indonesia [grant numbers NKB-1886/UN2.R3.1/HKP.05.00/2019] awarded to Rina Agustina in 2018.