
Abstract
Background:
In January 2015, the Alliance for International Medical Action and Bien Être de la Femme et de l’Enfant au Niger launched the 1000 Days Program in Mirriah District, Niger, to provide an integrated package of maternal and pediatric preventive and curative interventions. A new component of the package was the provision of small-quantity lipid-based nutritional supplements (SQ-LNS) for children 6 to 23 months.
Objective:
The objective of this study was to estimate the costs associated with providing the 1000 days package.
Methods:
Activity-based costing was used to estimate the total costs of the 10 activities included in the 1000 days package and also the incremental costs of new interventions, those beyond the standard of care.
Results:
The total cost of the 1000 Days Program was US$2.31 million for 9000 mother–child pairs. The average cost per pair was US$257 or US$103 per year. Incremental costs for new interventions accounted for 56% of program costs. Small-quantity lipid-based nutritional supplement represented 30% of incremental costs. A combination of efficiency measures could lower program costs by 15%.
Conclusions:
This study is the first to estimate the costs of an integrated, preventative–curative package of maternal–child health interventions with SQ-LNS. Implementing the 1000 days package across Niger will be challenging with only the country’s domestic health resources. Efficiency measures and creative financing arrangements, including support from external partners, should be explored. The approach and results described can inform future resource mobilization, financing, and budgeting efforts to scale the 1000 days or similar programs.
Keywords
Introduction
The first 1000 days, the length of pregnancy through the first 24 months of life, are decisive for a child’s physical health, cognitive development, and life expectancy. 1 Poor nutrition, inadequate access to health care, and recurrent infections during this period can lead to irreversible stunted growth, reduced performance at school and work, and heightened risk of early death. 2 -4
Mothers and children in Niger, especially in rural areas, face daunting nutrition and health challenges during these crucial 1000 days. The country’s health indicators are among the world’s worst. The maternal mortality ratio is estimated at 509 per 100 000 live births, 5 and neonatal and younger than 5 mortality rates are estimated at 25 and 84 per 1000 live births, respectively. 6 Malaria, diarrheal diseases, and respiratory tract infections are the top 3 causes of childhood death and disability, with malnutrition as the greatest risk factor. 7 Vaccine preventable diseases such as measles are common, 8 while the coverage of childhood vaccinations is low for most antigens. 9
A recent World Bank report found that more than half of the children in Niger do not have access to any of the determinants of good nutrition, such as adequate household food security, care and feeding practices, health services, or a healthy household environment. 10,11 The prevalence of wasting often exceeds the 15% World Health Organization (WHO) emergency threshold, and stunting affects 50% of children. 12 In all, 8% of children younger than 5 have concurrent wasting and stunting, 13 the highest prevalence worldwide, which is closely associated with an increased risk of death. 14 The Ministry of Health treats between 300 000 and 400 000 children for severe acute malnutrition (SAM) each year with support from international emergency aid organizations. 15 This places extreme pressure on an already fragile health system. On its current trajectory, Niger will not come close to meeting the Sustainable Development Goals (SDGs) for nutrition or maternal and child mortality. 16
The pediatric nutrition and health situation is most precarious in rural areas like the southeastern Zinder Region. Zinder routinely records some of the country’s highest malnutrition rates, with wasting and stunting among children 6 to 23 months in 2018 estimated at 30% and 63%, respectively. 17 The cost of a nutritious diet based on locally available foods is more than double the annual income available for food among poor families and more than triple the available income among very poor families, meaning that few households can afford a nutritious diet. 18 In the months before the harvest each year from June to November, families are further buffeted by a triple shock of (1) decreased household food quantity and quality as families exhaust their stores and food prices rise; (2) increased infectious diseases such as malaria and a spike in acute malnutrition; and (3) reduced time for childcare as a result of the demands of the agricultural season. In 2025, despite progress, the prevalence of wasting and stunting among children younger than 5 is projected to remain above 25% and 50%, respectively. To meet the WHO’s Global Nutrition Targets by 2025, there would need to be a more than 4-fold acceleration in the annualized rate of reduction for wasting and stunting prevalence. 19
To address this recurring nutrition and health emergency, in January 2015, the Alliance for International Medical Action (ALIMA) and its Nigerien medical partner, Bien Être de la Femme et de l’Enfant au Niger (BEFEN) introduced the 1000 Days Program in Zinder’s rural Mirriah District. The program provided a decentralized, integrated package of maternal and pediatric preventive and curative interventions with the objectives of reducing mortality, preventing malnutrition, and improving maternal and pediatric health. The interventions in the package included prenatal care, childbirth/delivery, postnatal consultations, child health and nutrition consultations and nutrition supplementation, the Expanded Program on Immunizations (EPI), malaria prevention, curative treatment for malnutrition, diarrhea, malaria, respiratory infections, and other diseases, personnel to provide these interventions, health systems strengthening, and administration and program management.
A key component to this package was the routine provision of small-quantity lipid-based nutritional supplements (SQ-LNS) for all children 6 to 23 months, financed by United States Agency for International Development (USAID’s) Food for Peace program. Lipid-based nutritional supplements are a class of ready-to-use food supplements that are highly nutrient-dense and fortified with vitamins and minerals at levels designed to treat and prevent acute malnutrition. Lipid-based nutritional supplements can be consumed directly from the package, do not require refrigeration, and are safe from bacterial contamination. They range in ration sizes based on their use to either treat or prevent acute malnutrition, with ready-to-use therapeutic (RUTF) or supplementary foods coming in 92- or 100-gram sachets, medium-quantity LNS in 50-gram sachets, and 20-gram sachets of SQ-LNS for home fortification of local diets to improve children’s complementary feeding.
A recent report on various maternal and child health interventions (including breastfeeding promotion and support, WASH, behavior change, micronutrient supplementation, and cash transfers) found that across a number of well-designed studies, food supplementation is the only intervention with sufficient evidence on effectiveness for preventing wasting. 20 In the past decade, a series of trials have looked at the impact of providing LNS in various quantities, including SQ-LNS. A recent Cochrane review found that compared to no intervention, LNS plus complementary feeding resulted in improved growth and reduced prevalence of moderate wasting, moderate underweight, moderate and severe stunting, and anemia among children. 21 The study showing that the largest impact was one in which SQ-LNS was provided in a package with testing and treatment for malaria and diarrhea. 22 A pooled analysis published after the Cochrane review found a 27% reduction in all-cause mortality among children receiving LNS across multiple low- and middle-income country contexts. 23 More recently, the PROMIS Mali study found a 30% reduction in the incidence of acute malnutrition among children receiving SQ-LNS for 12 months compared to the control group—including a 37% reduction in the incidence of SAM. 24
Although consensus surrounding the benefits of providing an integrated package of preventative–curative maternal–child interventions that include SQ-LNS is strong and growing, there is inadequate evidence to inform efforts to scale up these packages—especially a lack of documentation on the costs associated with implementing such comprehensive programs. As governments and donors set priorities for allocating funds across health and nutrition interventions at scale, improved estimates of the required costs of these programs will be needed for accurate budgeting and for developing investment plans to mobilize the required resources. Better cost information can also be used in studies of cost-effectiveness of different intervention strategies.
The objective of this study was to document the total costs and average cost per mother–child pair associated with providing the 1000 days package to 9000 mother–child pairs in Mirriah, Niger, and to estimate the incremental investments required to implement the program relative to the prevailing standard of care (SOC) in Niger. Possible sources of cost savings were also explored, including reducing the price of key cost drivers and adopting more efficient delivery strategies. The total costs of scaling up the program to the district, regional, and national level were analyzed and compared with current health spending in Niger in order to assess the affordability of such scale up and the need for mobilizing domestic and international resources.
Methods
Program and Study Setting
The health system in Niger is organized at 3 levels of health care delivery—a hospital in each district, one health center per health zone, and decentralized community-based health posts throughout the health zone. The posts are for the most part nonoperational due to limited operating budget resources. Currently, only 39% of people live within 1-hour’s walking distance (approximately 5 km) of a health post in the dry season, with this percentage decreasing to 24% during the rainy season when the population is further dispersed. 25
The 1000 Days Program was implemented in Niger’s rural Zinder region, where SMART surveys routinely show the prevalence of acute malnutrition (both moderate and SAM) to be between 20% and 30% among children 6 to 23 months and the prevalence of SAM to be between 4% and 8%. 26,27 The prevalence of stunting among children 6 to 23 months is 50% to 60%. 26,27
The 1000 Days Program
In collaboration with the Ministry of Health, ALIMA/BEFEN has been delivering maternal and pediatric health care in Niger’s Zinder Region since 2010, including varying levels of support to health centers in up to 24 health zones near the town of Mirriah and full support of the maternal and pediatric wards at the Mirriah District Hospital.
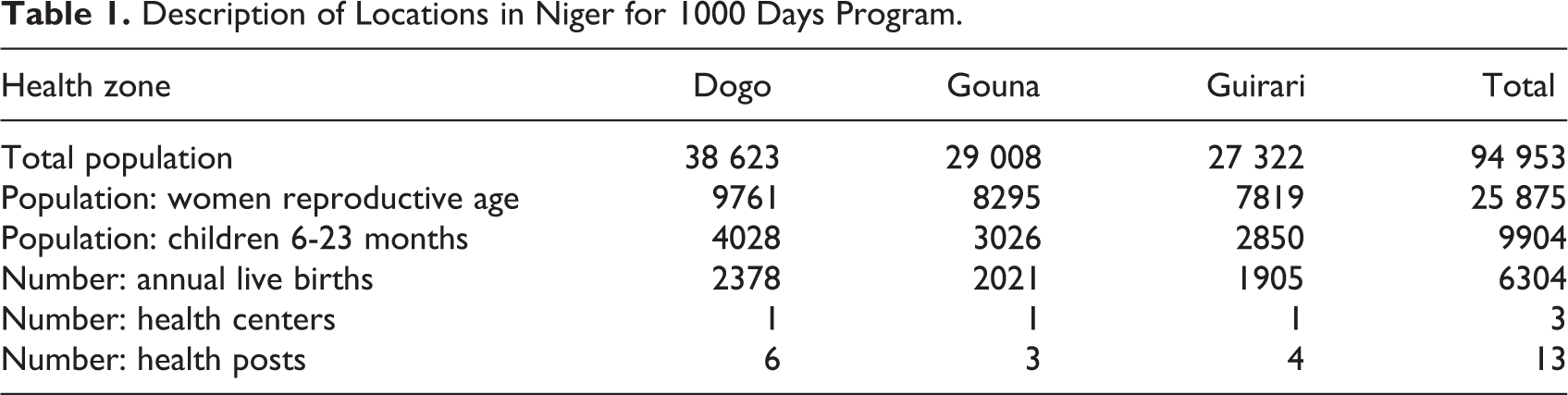
The 1000 Days Program was implemented in 3 of Mirriah District’s health zones—Dogo, Gouna, and Guirari—with activities conducted in 3 health centers and in 13 decentralized community health posts across these zones. Table 1 shows the population size and number of health system facilities served by the 1000 Days Program in each of the zones.
Description of Locations in Niger for 1000 Days Program.
The integrated package supported by ALIMA involved 7 preventive and curative interventions for mothers and children, as well as 3 cross-cutting support activities. Preventative and curative activities included: (1) prenatal care for pregnant women; (2) availability of skilled birth attendance for childbirth/delivery (used by approximately 40% of mothers); (3) postnatal consultations for mothers within 42 hours post-delivery; (4) 8 pediatric consultations for growth monitoring, clinical checkups, and nutrition supplementation for children 6 to 23 months (30 sachets of SQ-LNS per month); SQ-LNS was distributed monthly without a scheduled clinic visit in addition to the 8 pediatric consultations; (5) vaccination for children according to the EPI schedule; (6) seasonal malaria chemoprophylaxis (SMC) for children; and (7) outpatient curative treatment for mothers and children and inpatient care for children when needed, for example, for malaria, diarrhea, respiratory tract infections, SAM, and so on. The support activities included (1) medical personnel staffing, (2) health systems strengthening, and (3) administration and program management. Table 2 describes these activities in more detail.
Description of Standard of Care and New Interventions in 1000 Days Program.
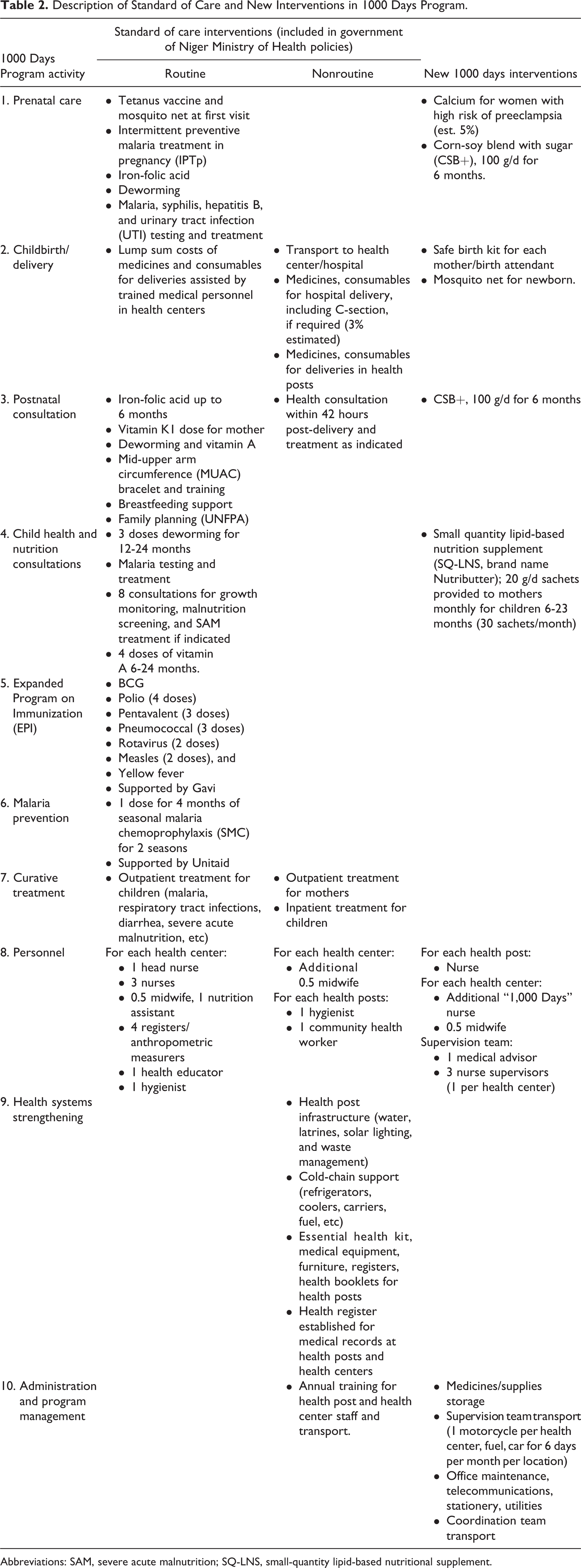
Abbreviations: SAM, severe acute malnutrition; SQ-LNS, small-quantity lipid-based nutritional supplement.
A prospective cohort study following more than 1700 pregnant mothers and children up to 2 years of age was embedded in the program from January 2015 to December 2018. Results will be reported elsewhere. Because previous research in a similar region of Niger showed a reduced incidence of acute malnutrition from routine provision of LNS, no control group was used in either the overall 1000 Days Program or the smaller study cohort. 28 -30
Standard of Care Versus 1000 Days Program
The 1000 Days Program was composed of both SOC interventions and an expanded set of new interventions. Standard of care interventions included those that are routinely implemented by the Ministry of Health (either financed by the government or by international donors and nongovernmental organizations), and those called for in government guidelines and plans but not routinely implemented due to constrained resources. These 2 sets of interventions are described as “routine” and “nonroutine” SOC interventions. For the 1000 Days Program, these nonroutine SOC interventions were financed by ALIMA/BEFEN via its donors, principally USAID’s Office of Foreign Disaster Assistance and the European Civil Protection and Humanitarian Aid Operations, with support from United Nations Children’s Emergency Fund (UNICEF) and World Food Program. “New” interventions were those not considered part of the SOC in Niger and introduced for the first time as part of the 1000 Days Program. The ALIMA/BEFEN and its donors also paid for these new interventions. Table 2 shows that 1000 days interventions were part of the SOC package, delivered routinely by the Ministry of Health or not, and which components were new interventions, including SQ-LNS, birth kits, maternal supplementation, and additional medical personnel.
Purpose
This analysis was conducted to estimate the costs of the 1000 Days Program to inform future decision-making on resource mobilization, financing, and budgeting for integrated packages of maternal child health preventative and curative interventions, and as an input to future cost-effectiveness analyses.
Costing Perspective
The costing was conducted from a payer perspective. All financial costs incurred for both routine and nonroutine SOC interventions and new interventions were estimated. The total costs of the program for the first 9000 mother–child pairs were calculated based on 13 months of enrolling pregnant women (typically at around the end of the first trimester of pregnancy) from January 2015 to March 2016 and by following their children up to 24 months of age, for a total of 30 months or 1000 days per mother–child pair. The last enrollee in March 2016 received the full package until the child reached 24 months in September 2018. Therefore, incremental personnel and other cross-cutting monthly costs covered 45 months in total, from January 2015 to September 2018. All care was provided free at the point of service to mothers and children. No user fees were required from participants. Any costs to the households, such as transport and the opportunity costs of participating, were excluded from the study. Future savings for health providers and households from the averted disease were not calculated.
Approach
A mix of top-down and bottom-up approaches 31 was used to estimate the costs for delivering the 7 direct and 3 support activities (personnel, health systems strengthening, and administration and program management) for the program years 2015 to 2018. These interventions are outlined in Table 2. Annual program costs were calculated by dividing total costs by 3.75 years (45 months). Costs were calculated based on normative guidance for each activity using guidelines, actual program design documents, budgets, and accompanying unit cost data. 31 The input costs for each activity are described in Supplementary Table S1.
The average cost of the full package and of each activity was derived by dividing total costs by the 9000-participating mother–child pairs enrolled in the program. Annual costs per mother–child pair were calculated by dividing the total average cost per mother–child pair by 2.5 years (30 months).
Intervention and cross-cutting costs were further analyzed across 4 categories of inputs, including: (1) medical and nonmedical supplies and materials, (2) supplementary food, (3) personnel salaries, and (4) infrastructure and logistical support (Supplementary Table S2). Medical and nonmedical supplies and materials were subdivided into (1a) drugs and medicines and (1b) consumables and equipment excluding drugs and medicines. Infrastructure and logistical support was subdivided into (4a) transport and (4b) buildings.
Costs are presented in 2019 US dollars. Euro and Central African Franc input prices from 2015 were adjusted for inflation. Cumulative inflation of the Euro from 2015 to 2019 was 4.98%. 32 Costs were then converted to US dollars using an exchange rate of 1.0 Euro = US$1.1 and 1.0 Euro = 655.96 West African CFA Francs, based on the average rates for 2019.
Data Sources and Assumptions
All unit costs and other assumptions were drawn from ALIMA/BEFEN budget records in planning for the 1000 Days Program. Unit costs for medicines, consumables, and equipment were referenced from the MSF Supply List, last updated December 31, 2015. Vaccines were procured by UNICEF using the UNICEF Vaccine Price List. Personnel costs were based on the Ministry of Health Salary Schedule. Supplementary Table S1 gives individual unit costs. Unit costs were compared to other sources for validation, when possible. Budget records were also validated against program results and programmatic data records. This costing exercise assumed that each mother–child pair received the complete package, but program records suggested some gaps in delivery. For example, coverage for maternal supplementation was low in this program because of repeated stockouts and financing shortages for this activity.
Sensitivity Analyses
Sensitivity analysis was conducted to consider how program costs might change if certain efficiency measures were introduced or as the program was scaled. The key unit cost examined was SQ-LNS given that it was the largest cost-driver among new interventions. The market for SQ-LNS is still in its infancy, and other analyses have suggested that future price reductions in SQ-LNS may occur as demand expands through economies of scale, entrance of additional local manufacturers, introduction of competitive tenders by purchasers, and advocacy for removal of value-added taxes (VAT). When UNICEF Supply Division introduced tenders for RUTF, which is also an LNS product, prices dropped by 27%. 33 One cost model on SQ-LNS suggests that the removal of VAT for products produced in Niger or France could reduce costs by 24%. 34 For the 1000 Days Program, ALIMA/BEFEN received SQ-LNS from Edesia with financing provided by USAID’s Food for Peace program. From 2008 to 2015, the Nutriset average price for RUTF dropped by more than 30% as the market grew. 33 As part of sensitivity analysis, the impact on program costs for an SQ-LNS price reduction of 25% was assessed.
Efficiencies in program delivery of the program may be achieved in 2 different ways. First, the length of SQ-LNS supplementation could be reduced from 18 to 12 months. Substantial benefits have been observed with 12 months of supplementation for each child (from 6 to 18 months) when there is high population coverage among 6- to 8-month olds. 35 This is likely because, for infants 6 to 8 months, SQ-LNS provides approximately half of needed caloric input from foods complementary to breastfeeding, and all nutritional requirements for iron, calcium, and zinc. 36 Second, the 1000 Days Program could become more integrated into the Ministry of Health. This integration would reduce the number of extra personnel employed by ALIMA/BEFEN, including medical supervision staff and the 1000 days nurse in the health centers whose duties could be performed by existing Ministry of Health workers. This type of integration would also allow the costs of the remaining incremental personnel to be more easily absorbed into Ministry of Health budgets to reduce the financial burden of implementing the 1000 Days Program.
The costs and economies of scale for bringing the program to the district, regional, and national level were calculated for 2 years of consecutive enrollment of pregnant women since at scale the program will have to outlay costs for both children in year 1 and year 2 of the program. According to Government Statistics, the Mirriah district had a population of 643 000 people in 2018, while the Zinder region had a population of 3.5 million. 37,38 Over 2 years, it was estimated the 1000 Days Program would serve over 62 000 mother–child pairs across all of Mirriah, 388 000 mother–child pairs in Zinder region, and 1.7 million mother–child pairs across the entire country. 38,39 Program costs were scaled based on the number of mother–child pairs for the 7 health interventions and based on the number of health facilities for the 3 supporting activities. The number of health facilities in Mirriah district, Zinder region, and the entire country are shown in Supplementary Table S4. All unit costs were considered fixed per mother–child pair given the lack of additional data for costs of implementation across different settings. Economies of scale were expected from the fixed programmatic management and administration costs.
Results
Total Costs of the 1000 Days Program
The total cost for a cohort of 9000 mother–children to receive the full 1000 Days package of interventions over a period of 45 months was estimated at US$2.31 million. The average program cost per mother–child pair was US$257. The most expensive activity was medical personnel staffing at US$707 069, 31% of total costs, followed by child health and nutrition consultations at US$395 161 or 17% of total costs. The least costly activities were curative treatment and malaria prevention at US$52 481 (2%) and US$22 451 (1%), respectively.
All SOC activities, both routine and nonroutine, were estimated to cost US$1.01 million. SOC interventions routinely implemented by the government totaled US$818 258 or 35% of total costs. Standard of care interventions not routinely implemented but financed by ALIMA/BEFEN’s donors required the remaining US$190 581 or 8% of total program costs. New program costs required US$1.30 million, 56% of program costs (see Table 3). The average incremental cost per mother–child pair was US$145 or US$58 annually for new interventions.
Costs of Standard of Care and New Interventions in the 1000 Days Program for 9000 Mother–Child Pairs.
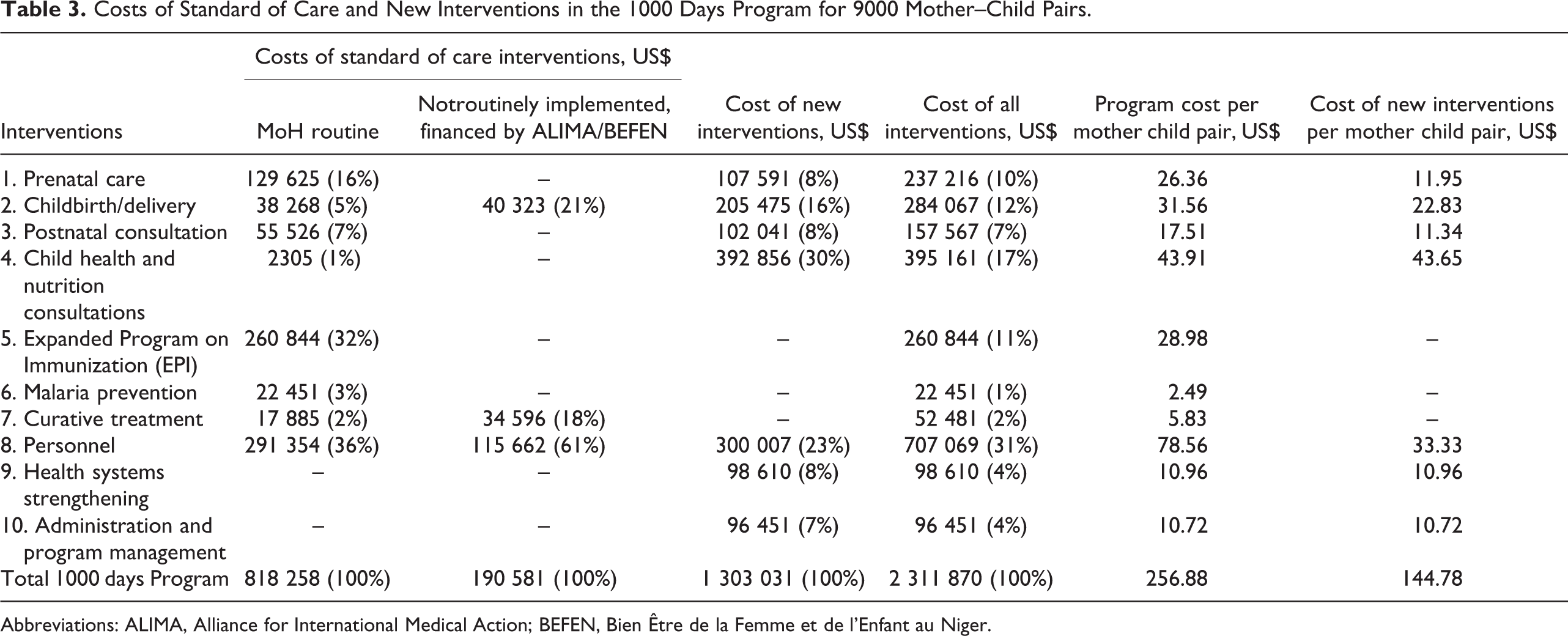
Abbreviations: ALIMA, Alliance for International Medical Action; BEFEN, Bien Être de la Femme et de l’Enfant au Niger.
Breakdown of Costs by Cost Input Categories
Among cost input categories, medical supplies and materials represented the greatest cost driver at 37% of total costs, broken down into drugs and medicine at 24% (US$561 282) and consumables and equipment at 13% (US$310 647). The next largest cost input category was medical staff salaries at 31% (US$707 958). Therapeutic food and supplements accounted for 25% of total costs, with SQ-LNS during child health and nutrition visits absorbing two-thirds of this amount alone (US$392 856). Infrastructure and logistical support represented 6% of total costs. Supplementary Table S2 shows the full breakdown of activities by the cost input category and subcategories.
Incremental Costs
Of all incremental costs (Figure 1), the new costs relative to the SOC, SQ-LNS supplementation accounted for 30% at US$44 per mother–child pair or US$2.43 per child per month for the 18 months of SQ-LNS delivery. Medical personnel (ie, staff at health posts, health centers, and medical supervision team) absorbed 23% of the incremental costs. Other new costs included routine supplementation to pregnant and lactating women with corn-soy blend with sugar (CSB+; 100 g/d) at 15% of incremental costs, drugs, and medicines such as calcium supplementation and safe birth kits (14%), consumables such as mosquito nets and supplies for health posts (8%), renovations for health posts (6%), and transport for patients and the supervision teams (4%).
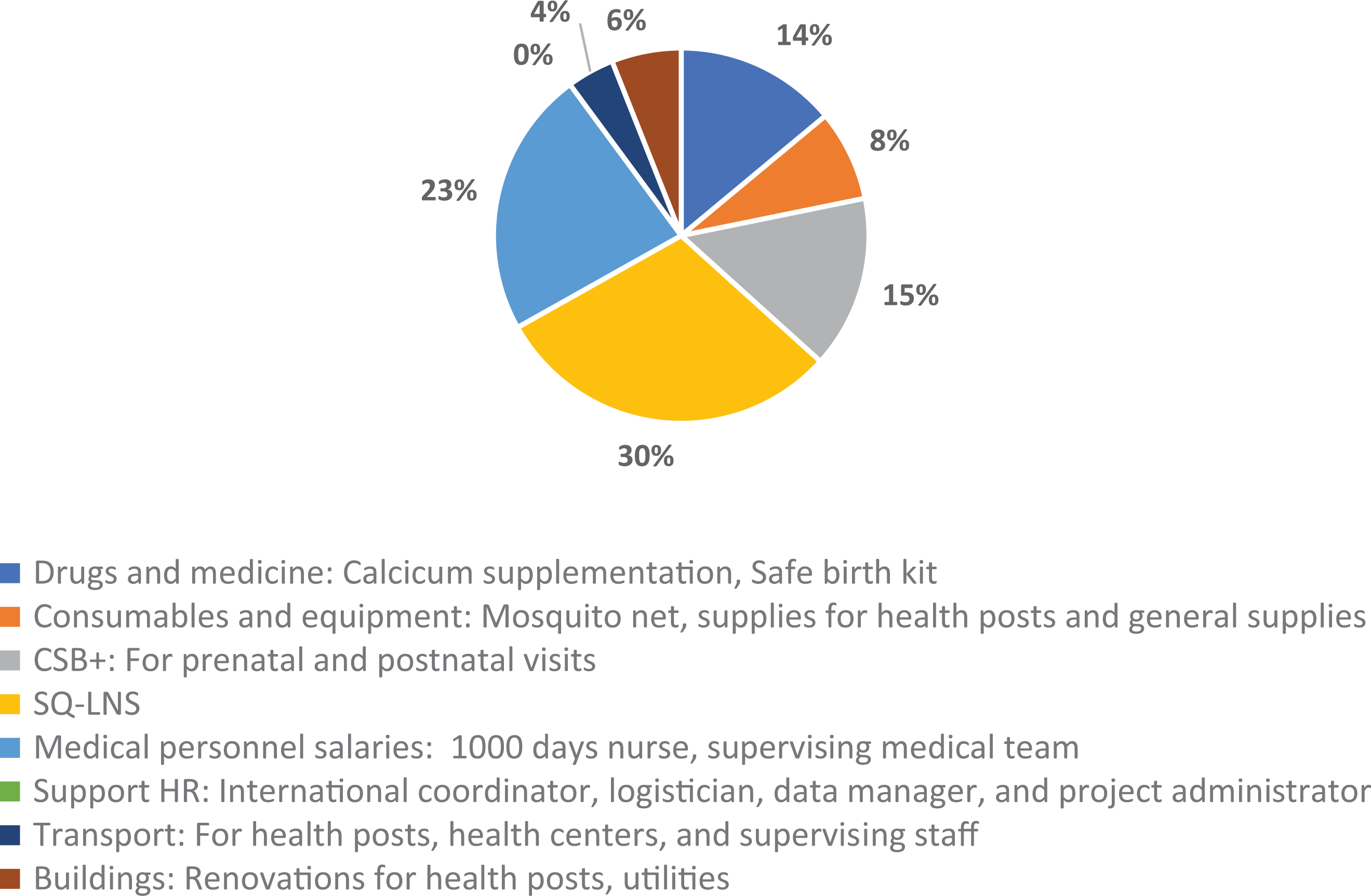
Breakdown of incremental 1000 Days Program costs by input categories (%).
Supplementary Table S3 includes a breakdown of the 1000 Days Program incremental costs.
Sensitivity Analyses
When the price of SQ-LNS was reduced by 25% from US$0.07 per sachet including freight to US$0.055, the total costs of the program are estimated to fall to US$2.2 million, a modest savings of 4%. Shortening the length of SQ-LNS from 18 months to 12 months per child would reduce program costs by 6%. Integration of the program management into the Ministry of Health is estimated to decrease costs by 7%. A combination of all these independent actions would lower program costs by 15% to US$2.0 million, a significant potential savings in a country with severe fiscal constraints like Niger.
If the 1000 Days Program were scaled to all of Mirriah district, the total costs at baseline for 2 years of enrollment would be between US$13.7 and US$15.8 million, with an average cost of mother–child pair of US$219 to US$252, depending on the number of efficiency measures implemented. The total costs to cover all children in Zinder region for 2 years of enrollment would range between US$69.2 and US$79.3 million, with an average cost of US$178 to US$204 mother–child pair. To deliver the package to all of Niger for the same period would require US$324.0 to US$371.3 million. At this national scale, the average cost per mother–child pair could be as low as US$182 with all efficiencies implemented, or about 30% less than baseline average cost of US$257 per mother–child pair in the small ALIMA-BEFEN 1000 Days pilot. The impact of efficiency measures at different geographic levels is shown in Figure 2. Full results are in Supplementary Table S5.
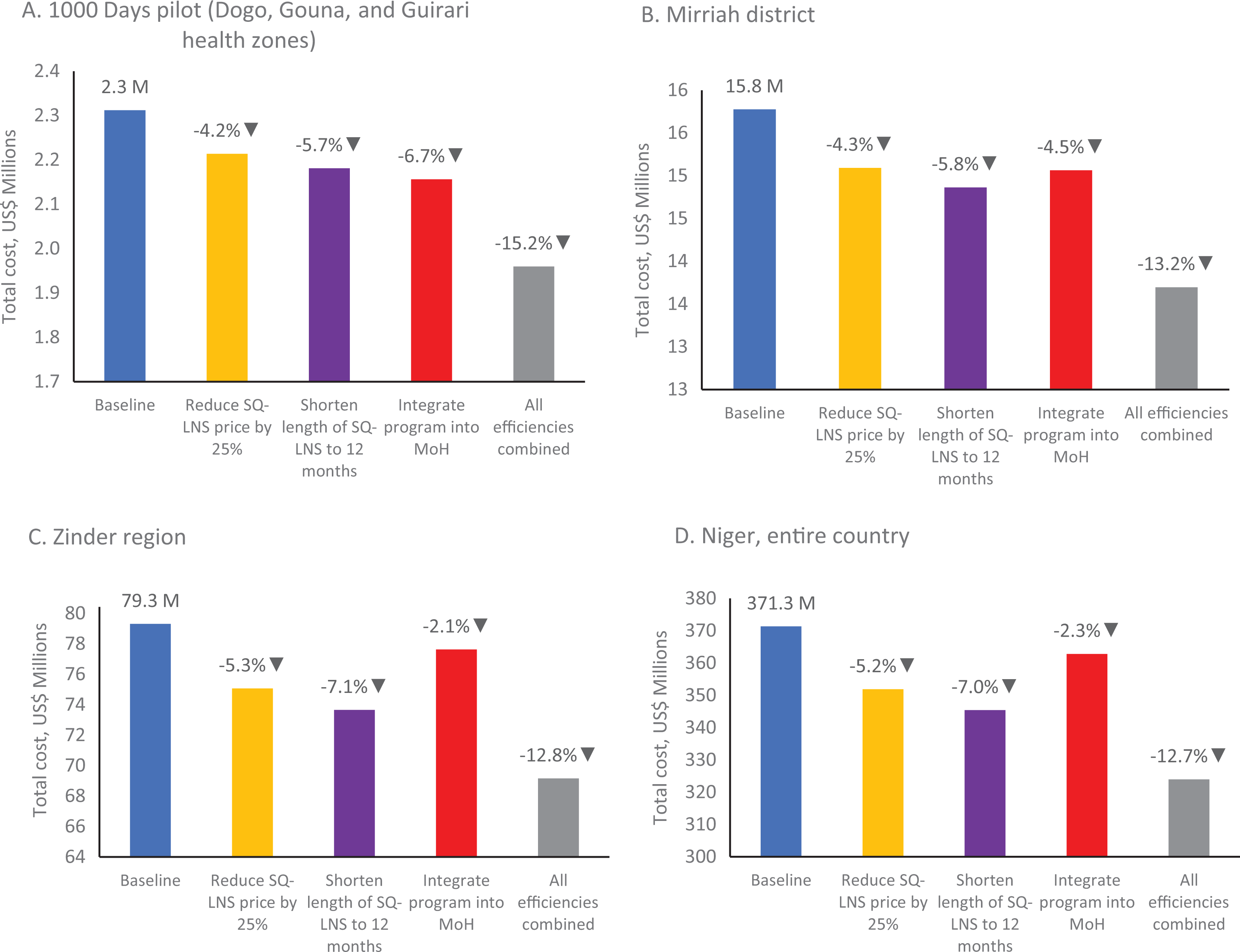
Sensitivity analysis results for 1000 days program for (A) the pilot in 3 health zones and (B) at scale for Mirriah district, (C) Zinder region, and (D) the entire country of Niger.
Discussion
Significance of the Study
This study is the first to estimate the costs of an integrated preventative–curative package of maternal–child health interventions with SQ-LNS for mother–child pairs over 45 months in a country that faces high rates of malnutrition and under-5 mortality. The total cost of the 1000 Days Program carried out in 3 zones of Mirriah district in the Zinder region was US$2.31 million with an average cost per mother–child pair of US$257. Personnel (31%), child health and nutrition consultations (17%), and childbirth/delivery (12%) were the most expensive activities in the package. Across all interventions, the dominant cost inputs were medical supplies and materials (37%), followed by medical staff salaries (31%) and therapeutic and supplementary food (25%).
Although the 1000 Days Program includes individual interventions and combinations of interventions that have been previously costed, 40 -42 at the time of this analysis, no other study had estimated the costs of an integrated maternal and child health package with routine SQ-LNS supplementation to children from 6 to 23 months. Given the growing evidence-base for the impact of SQ-LNS, such a costing study is urgently needed. A robust integrated maternal child health package delivered through a community health worker network in Bolivia was estimated to cost US$296 per mother–child pair, similar to the average cost reported here. This Bolivia project did not incur the cost of SQ-LNS, but higher salaries in Bolivia made up the difference. 43 A more limited package of maternal and child health interventions in Nigeria composed of antenatal services and secondary care for pregnant women and primary care services for children was estimated to cost between US$35 and US$76 per mother and child pair, similar to the average cost for the same activities in the 1000 Days Program. 44
Additional evidence is needed on the costs of these types of integrated maternal–child health packages from other countries and settings, especially packages that include new interventions like SQ-LNS. The methodology and approach used in this article can help inform additional studies.
Potential for Return on Investment
Although costs of the 1000 Days Program, particularly for the new activities, are relatively high, such investments could generate substantial returns in terms of preventing malnutrition and improving child health outcomes. There is mounting evidence from individual studies and from meta-analyses that nutritional supplementation of children, especially with LNS products, has a significant impact on improved developmental growth, as well as triggering reductions in acute malnutrition and mortality. 21 -24,36 Early initiation of treatment for moderate acute malnutrition has been shown to be cost-effective, 45 and cost-effectiveness analysis of SQ-LNS supplementation in the PROMIS trials is underway. The costing methods and data in this article can provide key input into additional cost-effectiveness exercises for integrated packages with SQ-LNS.
Impact and cost-effectiveness analyses should also consider long-term benefits in the form of improvements in human capital and economic productivity resulting from nutritional supplementation with a high-quality child-adapted food product, as was seen in Guatemala. 46
Affordability and Financing
Even if the expanded package of services under the 1000 Days Program generates large health benefits and is proven to be cost-effective, whether Niger and other low-income countries with large burdens of child malnutrition can afford to pay for and sustain such a comprehensive program is a major issue. About 35% of the total estimated spending on the 1000 days package in Mirriah is already routinely covered by the Ministry of Health and other traditional donor partners as part of the SOC, but the remaining parts of the 1000 Days Program were funded by ALIMA/BEFEN’s donors, including 8% of costs that should be covered by the government as part of the SOC. Financing of the program costs for new activities will likely have to come from external sources as a part of long-term development assistance until Niger’s economic and fiscal situation improves.
Although the analysis presented above suggests that the average cost of the 1000 days package per mother–child pair could be reduced by 15% through greater efficiencies, the total funding required to deliver the entire package to all malnourished children in Niger would amount to about US$162 million per annual birth cohort equivalent to, over 20% of national health expenditures.
In planning and advocating for an expansion of the 1000 days package in Niger, therefore, the issue of financing may prove to be even more vexing than convincing decision-makers of the health impact and cost-effectiveness of the program. If resources remain scarce, one option would be initially to target the program to the districts and regions with the highest rates of malnutrition and associated child and maternal mortality. Another possibility would be to focus available money on a more selective set of interventions that are the most effective. This more selective package would be built around supplementation of children aged 6 to 18 months with SQ-LNS, given the extensive evidence base for the benefits of SQ-LNS in the prevention of wasting, underweight, stunting, anemia, and mortality. 21,23,24,47 Recent analyses show a strong impact of SQ-LNS on growth over 12 months, as long as the children are close to 6 months of age at inclusion. 34 Additional interventions in the package could include investments to enable service delivery, especially rehabilitating and making health posts functional and covering salaries for a registered nurse in each health post (current policy in Niger calls for staffing posts with health agents only). The extra financing needed per mother–child pair for these 3 high-impact activities would amount to US$58 over 30 months, about 40% of the incremental cost of the full package delivered in the Mirriah pilot.
To expand and sustain the 1000 days package in Niger, the government will have to allocate more of its budget to health, particularly to maternal–child health activities. At the same time, Niger’s health sector partners including Gavi, the World Bank, UNICEF, the World Food Program, and the Governments of France and the United States could also be asked to pledge predictable long-term financial support for the 1000 days approach.
Sustained external financing is already in place for other interventions in Niger, including HIV antiretroviral therapy, childhood vaccination, and malaria prevention, diagnosis, and treatment, with the latter 2 embedded in the 1000 days package. Other parts of the 1000 days package could be underwritten in the same way. SQ-LNS has characteristics similar to those of vaccines and essential medicine that already receive stable long-term financing from donors. Recognizing this, the World Bank recently agreed to a credit for Madagascar to locally purchase several hundred metric tons of SQ-LNS over a 2-year period, as part of the country’s Nutrition Action Plan.
The cost analysis of the 1000 Days Program described in this article can be translated into other country contexts with similarly high rates of acute malnutrition and child mortality. Several of the unit costs for key inputs including SQ-LNS, vaccines, malaria chemoprophylaxis, and other drugs and diagnostic tests are likely to be similar across countries. At the same time, costing and budgeting for other countries will need to consider specific local differences such as staffing norms, salaries, and costs of transport.
Limitations
This analysis was based on budget data from ALIMA/BEFEN and not on program expenditures, which reflect actual resource outlays. Such spending might be different than budgets if program implementation varied from the original design or if suppliers offered commodities at different prices. To address this limitation, we verified that the activity levels and outputs over 2015 to 2018 in the 1000 days health zones in program reports and closely matched these to budgets and planning documents. We also compared the unit costs used against sources for other similar programs. For example, the cost for 4 cycles of seasonal chemoprophylaxis in this analysis was US$1.19, sourced from the MSF Supply List. This price was almost identical to the UNICEF Supply Division price of US$1.20 48 and close to a Niger-specific price of US$1.30 from a multicountry study of chemoprophylaxis costs conducted by Management Sciences for Health. 49 Likewise, the unit cost for the full range of childhood vaccines of US$27.61 used in this analysis from the MSF Supply List aligned with other credible sources, such as the prices in the WHO–UNICEF Global Immunization Vision and Strategy. 50
This costing analysis did not include performing full activity–based costing. Cross-cutting support activities such as personnel and program administration could not be disaggregated by health intervention because time use data was not collected at the time of program implementation. However, these cross-cutting costs are still captured separately and are reflected in overall program cost calculations.
If the 1000 Days Program is brought to scale, the analysis on the costs of implementation at the district, regional, or national levels should be repeated to examine how unit costs may change. Costs of transport, storage, and personnel may vary across Niger and would need to be adjusted for these different geographic settings.
Another limitation is that this study did not account for costs of the program to the household, such as travel time or opportunity costs. Costs to the household are important for equity considerations and to gauge their potential impact on client demand but were outside of the scope of this study which focused on the cost to public sector payers.
Conclusion
In countries like Niger where rates of childhood wasting often exceed the WHO emergency threshold of 15%, stunting affects more than half of the children, and maternal mortality is among the highest in the world, an integrated package of services including medically assisted births at community level, routine vaccination, provision of bed nets and SMC, treatment of common childhood illnesses, and routine nutritional supplementation is vitally important to save lives. This article comprehensively estimates the cost of such an integrated maternal child health package. The cost per mother–child pair of US$103 per year pays for a wide array of 7 different health and nutrition interventions, including supplementation with SQ-LNS for children 6 to 23 months. Although this cost may be far below what governments spend on maternal–child programs in middle- and high-income countries, sustaining the 1000 days package in Niger nevertheless poses major challenges to a West African country where average annual health spending is highly constrained. Efficiency measures to reduce costs and international financing arrangements, especially for health personnel and the largest new cost driver—SQ-LNS—will likely be needed to implement this program at scale. The approach, methods, and data in this article can help others to conduct the cost-effectiveness and budgeting studies needed to inform decision-makers and plan for large-scale implementation of integrated maternal–child health packages. These packages are urgently needed to reach children in the first 1000 days and ensure all countries make progress toward reaching the SDGs for maternal and child health and nutrition.
Supplemental Material
Supplemental Material, sj-pdf-1-fnb-10.1177_03795721211039869 - Costs of Implementing an Integrated Package of Maternal and Pediatric Interventions Including SQ-LNS in Rural Niger
Supplemental Material, sj-pdf-1-fnb-10.1177_03795721211039869 for Costs of Implementing an Integrated Package of Maternal and Pediatric Interventions Including SQ-LNS in Rural Niger by Lindsey Hiebert, Kevin Phelan, Moumouni Kinda, Nafissa Dan-Bouzoua, Maurice Kyungu, Thomas Bounameaux, Sani Sayadi, Oumarou Maidadji and Robert Hecht in Food and Nutrition Bulletin
Footnotes
Authors’ Note
K.P., L.H., M.Ki., M.Ky., N.D-.B., R.H., and T.B. contributed to the conception and design of the study. K.P., O.M., M.Ki., M.Ky., N.D-.B., S.S., and T.B. contributed to data acquisition. K.P., L.H., M.Ki., M.Ky., and R.H. contributed to the analysis. K.P. and L.H. drafted the manuscript. All authors contributed to the interpretation, critically revised the manuscript, and agree to be accountable for all aspects of the work.
Acknowledgments
The authors are grateful to the dedicated ALIMA/BEFEN staff in Niger who implemented the 1000 Days Program and collected these data. The authors would also like to Dr Sheila Isanaka for her feedback on the analysis plan and also Dr Steven Resch and Dr Steven Forsythe for their review and comments on this paper. The 1000 Days Program was financed mainly by USAID’s Office of Foreign Disaster Assistance (OFDA), the European Civil Protection and Humanitarian Aid Operations (ECHO), with support from UNICEF and WFP. The SQ-LNS was purchased from Edesia with financing from USAID’s Food for Peace program. AMADE Mondiale—Monaco provided some financing for this cost analysis.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: K. P. serves on the Social Purposes Advisory Commission of Nutriset, a main producer of lipid-based nutrient supplement products.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.