
Abstract
Background:
As the Scaling Up Nutrition (SUN) movement gains momentum globally, more attention and resources are being given to integrated nutrition interventions. In 2013, the Government of Malawi, with support from the World Food Programme and partners, initiated such an intervention in Ntchisi District. Aimed to reduce the prevalence of stunting, the intervention has several components, including the provision of a small-quantity, lipid-based nutrient supplement (SQ-LNS) for children aged 6 to 23 months.
Objective:
This paper describes formative research findings derived from a Rapid Assessment Procedures (RAP) approach to inform the integrated nutrition intervention.
Methods:
With a three-phase, emergent research design, this study utilized ethnographic methods including in-depth interviews, direct meal observations, and full-day child observations. Free lists and pile sorts were conducted to define food and illness domains through cultural domain analysis. Participants included community leaders, caregivers, health surveillance assistants, and children aged 6 to 23 months.
Results:
Community members felt that nutrition-related illnesses were less salient and threatening than other illnesses, and food quality was less important than food quantity. Household food allocation occurred in predictable patterns and varied by type of household member and season. Considered an energy-giving food, the SQ-LNS was accepted, but health education and communications tailored to local understanding of nutrition and health are necessary to ensure its appropriate utilization.
Conclusions:
Tailoring a communications strategy to Ntchisi, Malawi could only be done through formative research to understand the sociocultural factors influencing nutrition-related behaviors. A RAP approach allowed for a comprehensive understanding of this local environment.
Keywords
Background
Chronic malnutrition is estimated to affect 165 million children globally, with lifelong and intergenerational consequences for the health of individuals, communities, and countries. 1 In recent years, attention has focused on preventing stunting, an indicator of chronic undernutrition. 2 This attention has been channeled into the Scaling Up Nutrition (SUN) movement, to which 50 countries were committed as of mid-2014. 3,4 With unprecedented political commitments in place and donor money more available than once existed for maternal and child nutrition, interventions to address this issue are being rolled out in an increasing number of low- and middle-income settings.
There is a strong scientific case that intervention strategies designed to improve child nutrition should be implemented during the first 1,000 days of life—from conception until 2 years. 5 Thus, SUN activities in any particular country are often composed of a combination of nutrition-specific and nutrition-sensitive interventions 6 that include 13 interventions recommended to have the most substantial impact on maternal and child health. 7 Many of those suggested interventions require some level of behavior change by the maternal caregiver and other household members. Whether that means going to the health center for supplementation (e.g., vitamin A, iron, zinc, multiple micronutrients) or adhering to health promotions and education (e.g., exclusively breastfeeding from 0 to 5 months, complementary feeding from 6 to 23 months, hygiene promotion), SUN activities are largely behavior change interventions.
There is ample evidence to support the use of behavior change interventions to improve key health-related behaviors and child nutrition outcomes. 7 -9 Given the range of behavior change interventions available to prevent stunting, nutrition programs commonly focus on promoting optimal complementary feeding practices for children aged 6 to 23 months. In a systematic review of behavior change interventions to promote complementary feeding 10 , researchers concluded that effective interventions are derived from well-planned and thorough formative research to inform intervention design and implementation. This type of research is carried out prior to implementation of intervention, with the goal of collecting detailed information to gain an in-depth understanding of both the target population and the local context where the intervention will take place. 11 Understanding the array of sociocultural and context-specific determinants that impact key behaviors related to nutrition is important for intervention design. 10,12 -15
Currently, there is no universally agreed-upon methodology for conducting the requisite formative research for undernutrition interventions. 16 However, due to the relatively recent attention to specialized nutritious foods, such as micronutrient powders (MNP) and small-quantity, lipid-based nutrient supplements (SQ-LNS), in nutrition interventions that aim to enhance the quality of complementary foods of young children, there have been a growing number of formative research studies described in the literature. 16 -22 The methodologies of these studies vary greatly, making comparisons among them difficult and leaving researchers without a consistent basis on which to model new formative research studies that include specialized nutritious foods.
Objective
Our objective in this formative research was to inform the design and implementation of a Government of Malawi nutrition intervention that aims to prevent stunting during the first 1,000 days of life through a series of interventions, including the provision of a small-quantity (20-g), lipid-based nutrient supplement (SQ-LNS) to be consumed by every child from 6 to 23 months of age once a day either directly out of its sachet or fortified in a complementary food. The SQ-LNS used for this research was Nutributter, made by Nutriset (Maulanay, France). Each reference to “SQ-LNS” hereafter refers to this particular small-quantity (20-g) product unless otherwise specified. Our research questions were as follows: What cultural perceptions and household behaviors exist in relation to childhood illnesses, concepts of healthy growth and development, and food utilization? How can an ethnomedical model, which describes a local body of knowledge about a specific illness or group of illnesses
23
, be developed for salient nutrition-related illnesses in this setting? What are community members’ attitudes toward an SQ-LNS that will be introduced as part of the integrated nutrition intervention in this setting?
In answering these questions, we sought to also pilot a methodological approach developed for the World Food Programme that could serve as a template for formative research in other interventions with specialized nutritious foods in other settings.
Methods
Study Setting
Data were collected from February until May 2013 in all seven traditional authorities (geographic areas) of Ntchisi District, which lies in the Central Region of Malawi and is home to approximately 250,000 residents. Nearly 70% of both men and women engage in agricultural activities as their primary livelihood. Only 6.4% of the population has access to electricity.
Ntchisi children under 5 years of age suffer from a high disease burden. A malaria-endemic area, the Central Region has a mortality rate among children under five of 129 per 1,000 live births, as well as the highest prevalence of anemia (64%) and diarrhea (20%) in this age group in the country. 24 Where two-thirds (66.3%) of the population reported suffering from food shortage during the year, Ntchisi has a 58.1% prevalence of stunting among children under five, the second highest in the country among 31 districts. 25
Although nearly all children under 2 years of age are breastfed (99%), a smaller percentage is exclusively breastfed until 6 months (71%) or continuously breastfed until 2 years (76.8%). Among all children aged 6 to 23 months surveyed in this region, only 30.2% received food from more than four food groups in the previous 24 hours, and just 52.9% met minimum meal frequency standards. Complementary foods are composed primarily of grains, which were consumed more than any other food group by children aged 6 to 23 months. 24
Overall Study Design
The formative research design was based on a Rapid Assessment Procedures (RAP) approach. 26,27 The design drew from a RAP manual that was recently developed for the World Food Programme to use during programs that utilize specialized nutritious foods. This manual, which is being piloted in various World Food Programme program contexts, has four sections: 1) situational analysis, 2) selection of an appropriate specialized nutritious food for a given setting, 3) introducing the specialized nutritious food to the community/social marketing, and 4) monitoring and evaluation. The tool uses mixed methods to aid practitioners in successfully choosing, introducing, and monitoring specialized nutritious foods as part of integrated nutrition programs (see Note 1).
Drawing from sections 2 and 3 of that manual, this formative research followed a three-phase, emergent design that was iterative in nature. Designed to be exploratory, without preconceived hypotheses but instead with an open-ended, flexible, and inductive approach to data collection and analysis 28 , this study used mixed methods to collect multiple forms of data. Phase 1 explored the food, illness, and health domains of caregivers, as well as household food preparation and feeding practices. Phase 2 collected ethnographic data and built off phase 1 findings to develop an ethnomedical model of nutrition-related illness through cultural domain analysis for illustrating cultural perceptions of the Chewa medical system. This phase also introduced an SQ-LNS to households as part of an 8-week feeding trial. Phase 3 was designed to capture caregiver experiences during the trial and develop community-developed communications strategies for the effective promotion of the SQ-LNS. Further details of the study design are described elsewhere (see Note 1).
Sampling
We recruited participants through a two-tiered, purposive sampling strategy. 29 To ensure the study collected data from all seven traditional authorities in Ntchisi, the district nutrition team first identified an equal number of representative villages in each area. Once these villages were identified and village chiefs provided permission for community participation, information-rich participants who met the specific criteria described below were recruited for participation. 28,30
In-depth interviews, direct observations, and full-day child observations
Community leaders, caregivers of children aged 6 to 23 months, and households with children aged 6 to 23 months were purposively sampled. 29 To identify community leaders, health surveillance assistants, who were paid government employees working at the 11 Ntchisi health centers, helped identify village chiefs who could speak not only about themselves but also about their communities with deep insight. 30
Working together, the health surveillance assistants and community leaders identified caregivers of children aged 6 to 23 months who could offer rich information about both the Chewa culture of central Malawi and young child health, as well as represent a diverse interview sample stratified by sex (21 women and 5 men), location of residence within the district (equal representation from all seven traditional authorities of the district), and number (range, one to nine; median, three) and age (youngest child aged 6 to 23 months) of children 31,32 to ensure inclusion of different perspectives. Final sample sizes were based on the amount of data needed to reach data saturation, i.e., the point at which additional data collection no longer generated new understanding. 33,34
Pile sorts and free lists
Caregivers were purposively sampled, as described above. 31,32 Data were collected using guidelines proposed by Weller and Romney 35 , who suggest that 20 to 30 free list informants are sufficient for coherent domains, such as causes of illnesses, and 30 to 40 pile sort informants will produce reliable data. The caregivers who free listed were different from those who pile sorted.
Data Collection
Tables 1 and 2 provide an overview of the methods and sample sizes described below. Data were collected in all seven traditional authorities of Ntchisi during each phase.
Summary of Ethnographic Methods Used in This Study.
Summary of Data Collection Efforts by Phase of Formative Research.
aThe same 19 households were observed in each phase, except that 2 households were not observed in phase 2 because of impassable roads during the rainy season.
bThe same seven children were observed in each phase.
cThis total represents the number of different participants in all three phases of the research, not merely the sum of each row due to repeated observations of the same participants.
Phase 1 (exploring cultural perceptions and behaviors of food and illness)
Phase 1 used in-depth interviews and free lists (e.g., “List all of the illnesses that young children suffer from in this community”) to explore the cultural domains of community members. Direct observations of midday and evening meals were used to understand household food preparation and feeding practices. Full-day child observations documented the dietary behavior of children aged 6 to 23 months in this setting from 8:00 A.M. until sundown.
Phase 2 (developing an ethnomedical model of nutrition-related illness)
Phase 2 collected further cultural data on food and illness domains using free lists of illness causes (e.g., “Please list all of the different causes of kunyentchera (wasting)” to finalize construction of an ethnomedical model of nutrition-related illness. Unconstrained pile sorts of salient foods for young children were completed to determine local food groupings. 35,36 A second round of direct meal observations and full-day child observations was conducted with the same households observed in phase 1 with special attention to infant and young child feeding practices after the introduction of the SQ-LNS.
Phase 3 (understanding caregiver experiences with an SQ-LNS)
Phase 3 used in-depth interviews to elucidate caregivers’ experiences with the SQ-LNS, specifically identifying barriers and facilitating factors to its appropriate use. For triangulation, in-depth interviews with health surveillance assistants were also conducted to corroborate and help explain findings from phases 1 and 2. A third round of meal observations and full-day child observations were completed with the same households from the previous two phases to minimize reactive behaviors and to observe feeding practices on three separate days over the 3-month study period.
Data Analysis
In-depth interview data
Textual data were translated and transcribed verbatim from Chichewa digital recordings into written English, maintaining local terminology. 37 Atlas.ti version 7.0 computer software (Scientific Software Development, Berlin, Germany) was used for data management and coding. We inductively analyzed the textual data drawing from the procedures of Grounded Theory. 38 The process began with line-by-line coding until strong analytic directions were identified and a codebook was developed (Table 3). Using that framework, focused coding was then applied to the data set to synthesize and explain larger segments of text. Upon development of analytic categories, axial coding reassembled the data to give coherence to the emerging analysis. 39 Constant comparisons were made throughout the coding process 33 , and memos, or analytic notes, were written to draw comparisons among codes, categories, and quotations from text. 38
Guiding Analytic Categories for Textual Data Analysis of Caregiver Interviews.a
SQ-LNS, small-quantity, lipid-based nutrient supplement.
aPhase 1 interviews explored sociocultural characteristics in general, whereas phase 3 interviews focused more specifically on caregiver experiences with the SQ-LNS during a small home-feeding trial.
Direct observation data
Both qualitative (descriptive data related to types and amounts of foods consumed) and quantitative (frequencies of giving or receiving food) information was recorded with standardized forms. Observations were recorded at a minimum every 5 minutes and more frequently when events related to the research questions occurred. 40 The research team aggregated the descriptive field notes from the observations, applied focused codes, and drew out key themes salient to the research questions. 38
Free list data
Anthropac, version 4.98 (Analytic Technologies, Lexington, KY, USA), was used to analyze lists of foods, illnesses, and causes of illness. Items of salience (S)—a statistic accounting for rank and frequency—were generated, as well as a rank-ordered identification of the most commonly mentioned items. 41 These items of salience were merged with findings from interview data to construct an ethnomedical model of nutrition-related illness.
Pile sort data
After the participants sorted food cards into piles, the numbers identifying the cards being coded for analysis were entered into the software and aggregate proximities were calculated, yielding 18 ×18, item-by-item matrices of food items with cells indicating the proportion of times two items appeared in the same pile across participants. The aggregate proximity matrices were then analyzed using multidimensional scaling (MDS) as recommended by Weller and Romney. 35 Stress, taken as a goodness-of-fit statistic in MDS analyses, was calculated for each aggregate proximity matrix.
Ethical Approval
The study protocol was approved by the Institutional Review Board of the Johns Hopkins Bloomberg School of Public Health and the Malawi National Health Sciences Research Committee. Adult participants provided informed oral consent for themselves and assent on behalf of child participants.
Results
Cultural Perceptions of Health, Foods, and Illnesses
In Ntchisi, caregivers and community leaders shared similar overall perceptions related to illness, food, and nutritional status. The data exhibit a strong fit to the cultural consensus model 42 , supporting the assertion that, despite some individual differences, the majority culture of Ntchisi is relatively homogenous in these domains.
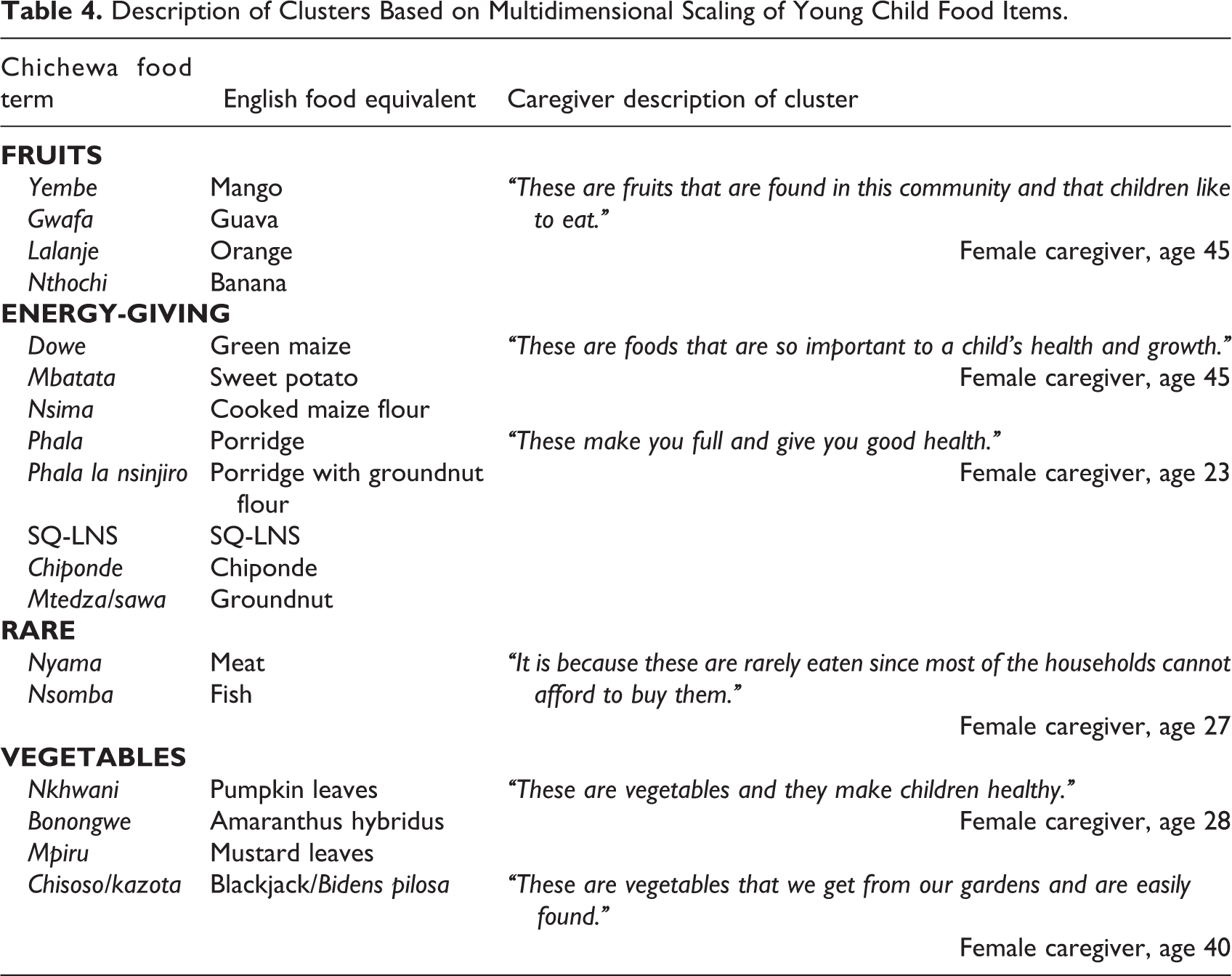
Caregivers defined “healthy growth and development” (kukula mwa thanzi) as a child who is happy, not getting sick frequently, gaining weight, and eating a diet of “different food groups” (zakudya za magulu or zakudya za kasintchasintha). Consuming “different food groups” was a salient theme and is considered important for child health. Caregivers categorized foods into four general categories which they labeled as “fruits,” “vegetables,” “energy-giving” (e.g., porridge, groundnuts, SQ-LNS), and “rare” (e.g., meat, fish) (Figure 1 and Table 4).
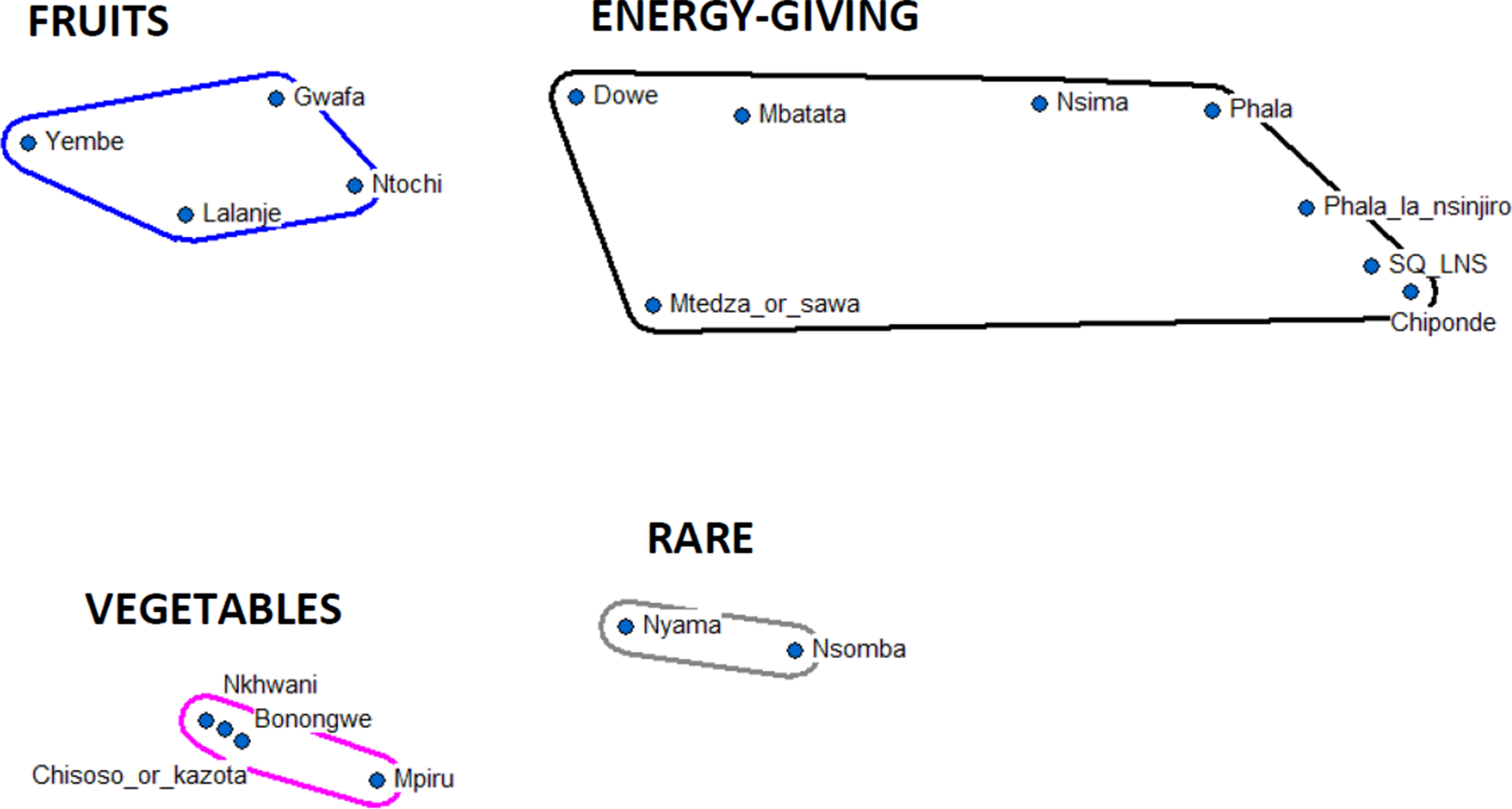
Multidimensional scaling map of Chewa young child food items (n = 18).
Description of Clusters Based on Multidimensional Scaling of Young Child Food Items.
When asked to describe challenges that they face in the village, community members explained that childhood illness is not considered a major challenge in comparison with more formidable barriers such as “lack of money,” “hunger,” and “long distance to the hospital.” Cultural domain analysis results illustrate that the three illnesses most salient to community members were malaria (S = 0.91), cough (S = 0.72), and diarrhea (S = 0.71). Caregivers explained that there is stigma attached to many illnesses afflicting young children, especially those that are nutrition-related, because they are feared to be an indication of poor caring practices. This stigma results in caregivers sometimes avoiding health clinics and instead visiting traditional healers. Community members invoked both naturalistic and personalistic causes in explaining episodes of illness; they just as often pointed to a creator who is responsible for illness as they discussed poor health-related behaviors, such as poor handwashing.
Understanding Prevention and Treatment of Salient Nutrition-related Illnesses
Nutrition-related Illnesses in Order of Salience to Caregivers.
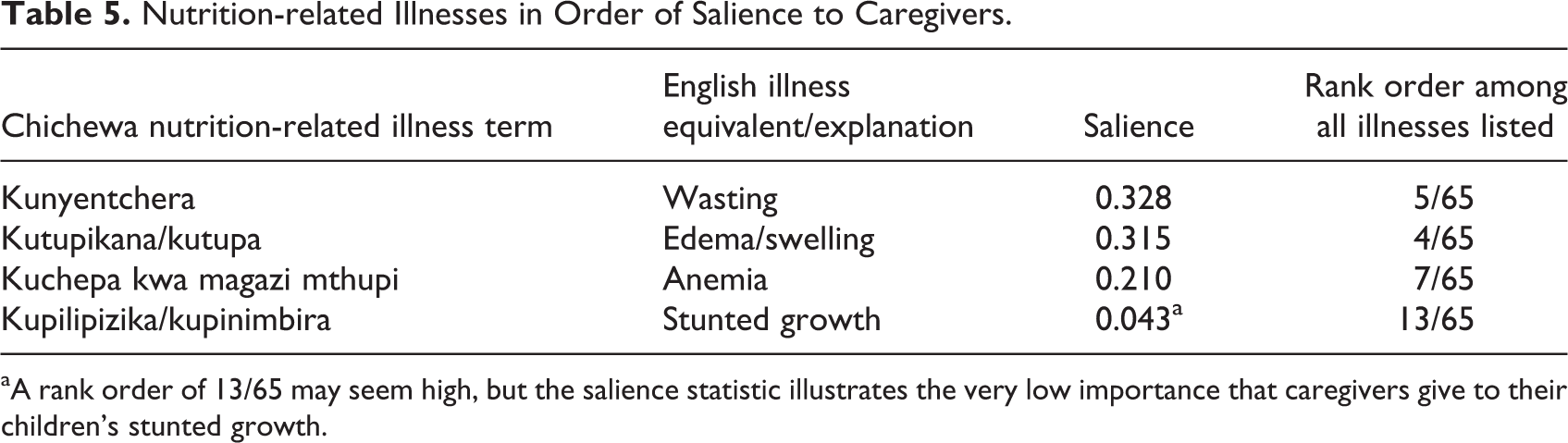
aA rank order of 13/65 may seem high, but the salience statistic illustrates the very low importance that caregivers give to their children’s stunted growth.
Well people are different from each other…one can be tall and the other can be short…it’s just by nature that the person is like that…it’s just how God created the child.
–Female caregiver of six children, in-depth interview
We generated an ethnomedical model of causes, illnesses, and treatments for these illnesses from the data (Figure 2). The model illustrates that a “lack of food in the body” is the perceived primary cause of nutrition-related illness, highlighting a focus on dietary quantity, not quality. The least salient nutrition-related illness, stunted growth, is considered locally to stem from “a lack of food in the body,” “genetic inheritance,” and, less commonly, “frequent illness.” Compared with edema, wasting, and anemia, there is less consensus among caregivers around the causes of stunted growth.
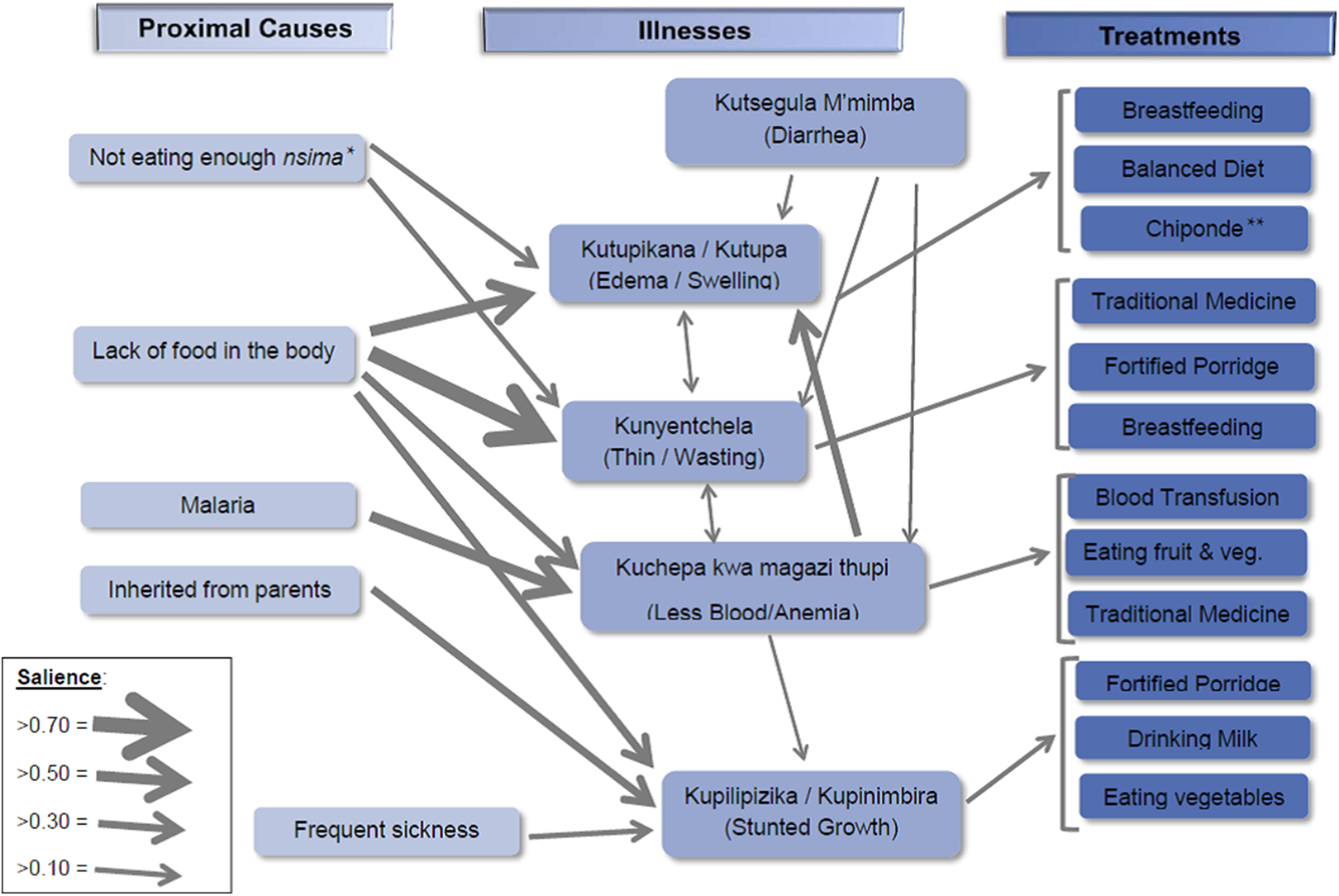
Ethnomedical model of nutrition-related illness in Ntchisi. *Nsima is cooked maize flour. **Chiponde is a locally produced ready-to-use therapeutic food (RUTF) used for the treatment of acute malnutrition in Ntchisi.
Caregivers do not hold distinct concepts of prevention and treatment in relation to nutrition-related illnesses as clearly as they do with other illnesses, such as malaria and diarrhea, on which previous extensive health promotion efforts in Ntchisi have focused their attention. For those illnesses, prevention is commonly understood in concrete terms, such as using an insecticide-treated bednet for malaria, or practicing hygienic hand-washing behavior for diarrhea. For nutrition-related illnesses, concepts of prevention focus on dietary quantity (e.g., “lack of food in the body”), whereas those of treatment highlight the perceived importance of dietary quality (e.g., “breastfeeding,” “balanced diet,” “drinking milk,” “fruits and vegetables,” and “eating vegetables”).
Intra- and Interhousehold Food Allocation Patterns and Behavior
In Ntchisi, food is allocated in predictable patterns that vary according to the time of year and type of household member. Direct observations revealed that caregivers favor children aged 6 to 23 months in terms of the food they receive, the time they receive it, and the individual attention they are given during meal times. During non-meal times, these children are given extra maize-based porridge, usually at mid-morning and mid-afternoon. During midday and early evening meal times, they eat with their caregivers. In many instances, these children eat before the rest of the family in the evening due to early bedtimes. Data indicate that this caregiver favoritism provides additional and more frequent food rations to children aged 6 to 23 months throughout the day. When possible, caregivers add special complementary foods, such as soybeans or groundnuts, to children’s diets, a strategy promoted by the health surveillance assistants and government. Forced hand-feeding of children aged 6 to 23 months was commonly seen during meal observations.
Intrahousehold food sharing—eating from shared plates, caregiver-to-young-child feeding, and child-to-child food sharing—is influenced by many factors. Caregivers explained that sharing patterns vary by season as well as by the age and sex of household members. We observed extensive eating from shared plates during the lean season from January to April when food stocks are carefully being conserved until the harvest. After the harvest (May to July), husbands reportedly steal food from the household to sell for money to buy alcohol. During this same time, caregivers explained that less intrahousehold food sharing occurs because an abundance of food allows for individual portions during meal times (Table 6).
Projected Food and SQ-LNS Sharing Practices by Season.a
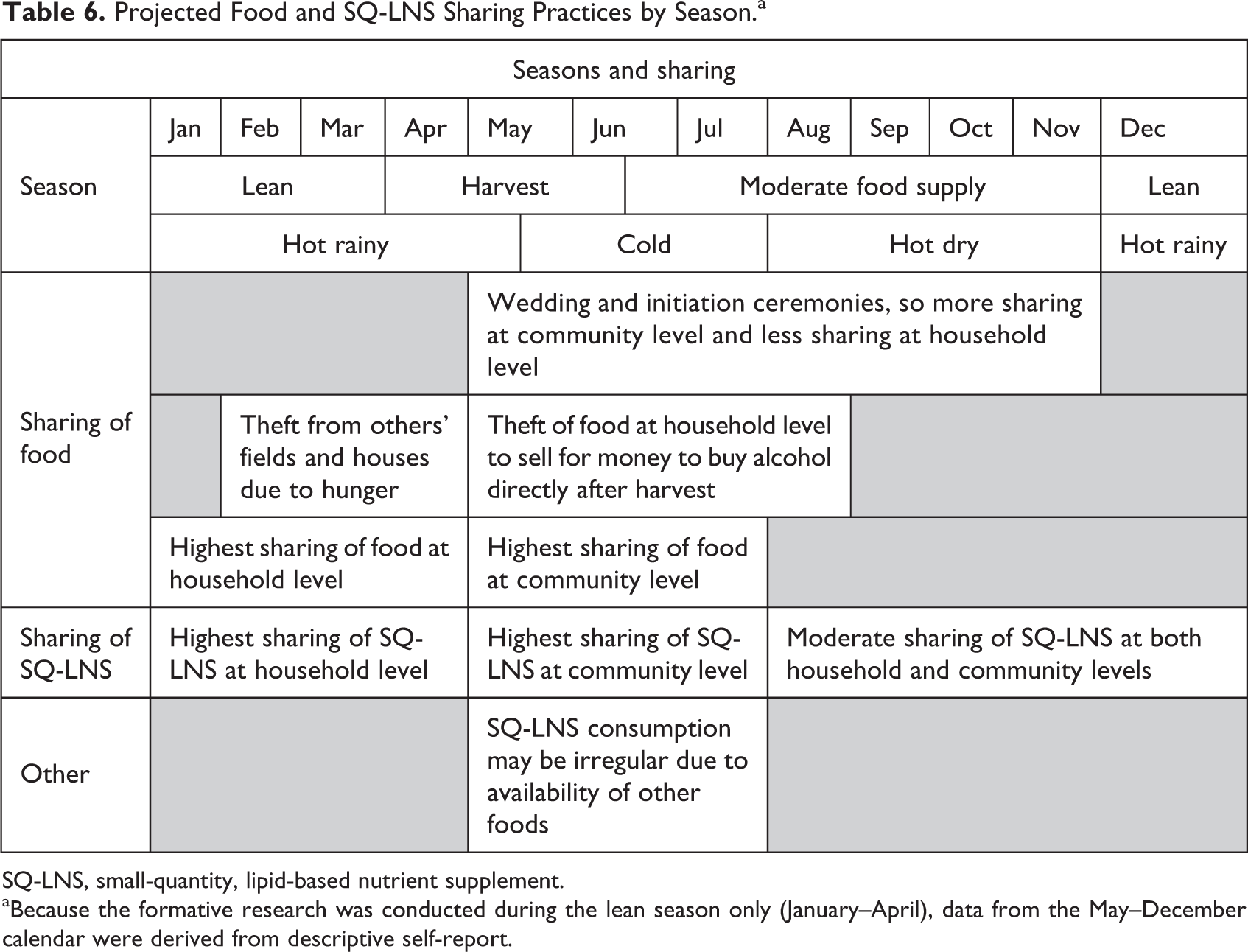
SQ-LNS, small-quantity, lipid-based nutrient supplement. aBecause the formative research was conducted during the lean season only (January–April), data from the May–December calendar were derived from descriptive self-report.
Similarly, interhousehold food sharing—food sharing among households, barter of food for other foods or goods, food sharing at community gatherings, and theft—also varies by season. Caregivers explained that these practices peak during and soon after the harvest when there is an abundance of food for barter. Also, they described interhousehold food sharing to be common practice during times of celebration, such as initiations and weddings. However, during the lean season, interhousehold theft of food occurs from both fields and households. We observed children of similar ages who tend to live, play, and eat together—a situation that facilitates food sharing among children of similar age and sex in village settings.
Impressions of the SQ-LNS
Caregivers had positive impressions of the SQ-LNS, and children aged 6 to 23 months were highly accepting of its flavor, a driver of product sharing and overuse that occurred within and between households. Community members suggested that sustained compliance will be more feasible with development of culturally appropriate packaging that includes the sachet language in Chichewa as well as locally developed images and clearer instructions for use. Most people asked for larger quantities of the SQ-LNS, comparing it to the locally produced ready-to-use therapeutic food (RUTF) Chiponde, which is already being used in Ntchisi for the treatment of acute malnutrition and has a weight of 92 g (Figure 3). Even after the research team explained the reasons for the SQ-LNS, confusion about its purpose vis-à-vis that of Chiponde existed among caregivers.
Comparison of sizes of the locally produced ready-to-use therapeutic food (RUTF), Chiponde (92 g), and the small-quantity, lipid-based nutrient supplement (SQ-LNS) (20 g). I think it [SQ-LNS] is a medicine…because let’s say if a child is suffering from malnutrition and they start taking this, then they can get better, and the child can become healthy. –Female caregiver of child aged 12 months, in-depth interview
When asked directly for their perceptions of the SQ-LNS, 10 caregivers said that the product was a medicine, 3 that it was a food, and 5 that it had qualities of both a food and a medicine. They either called the product by its name, referred to it as Chiponde, or called it “chakudya,” Chichewa for “food.” Nine of 12 caregivers indicated that they would pay a nominal price (mean, 56 MWK/0.14 USD; median, 35MWK/0.09 USD) for a sachet of the product if it was introduced through a market-based system, citing their children’s health as the reason for this willingness.
Discussion
This paper describes a RAP approach that produced a holistic account of perceptions of illness, food, and health; household food utilization patterns; and SQ-LNS acceptability during formative research within the SUN movement. These findings, which shed light on the sociocultural context of Ntchisi, Malawi, should be used as key considerations in the design, implementation, and monitoring of interventions.
Triangulating in-depth interview, free list, and pile sort data from the RAP methodology allowed us to construct an ethnomedical model of causes, illnesses, and treatments for nutrition-related illnesses in Ntchisi (Figure 2). Program staff can use this model to develop health education materials that directly address community perceptions of the types and causes of nutrition-related illnesses. Distinct concepts of prevention and treatment are not as clearly defined for nutrition-related illnesses as they are for other illnesses. Health promotion teams could thus consider drawing on cultural metaphors from local bodies of knowledge related to other illnesses and applying them to prevention of nutritional illness with an SQ-LNS; such an approach may resonate with community members. 43 For example, health messaging could compare the consumption of an SQ-LNS for prevention of chronic malnutrition to sleeping under an insecticide-treated bednet for protection against malaria. Such messaging would be most effective if it built off the existing bodies of knowledge around nutrition-related illness, while not trying to deconstruct them into entirely new cognitive frameworks unfamiliar to community members. It is far easier to introduce, reinforce, or build on existing frameworks than it is to try to change well-established perceptions. 44
Findings from cultural domain analysis highlighted community members’ low perceived threat of nutrition-related illnesses in general, and child stunting in particular. This finding may prove to be a major barrier to messaging that resonates with caregivers and thus compliance with the SQ-LNS. Developing messaging with consideration of this finding and aligned with behavior change theory will be important for effective development of Behavior Change Communication (BCC) in this setting. The Persuasive Health Message (PHM) framework (Figure 4), which includes elements from several well-known behavioral models, would be especially useful for message development. 45 To develop messages within this framework, Witte 46 recommends the following three steps: 1) identify salient community beliefs and specific behavioral goals, 2) develop an audience profile, and 3) construct a persuasive message that is framed to fit within local bodies of understanding. This formative work has already yielded rich information for steps 1 and 2 in this process and provides further information (e.g., nutrition-related illness risk perception, self-efficacy toward using SQ-LNS, and various cues for action) that can be used to develop persuasive messages in the Ntchisi context.
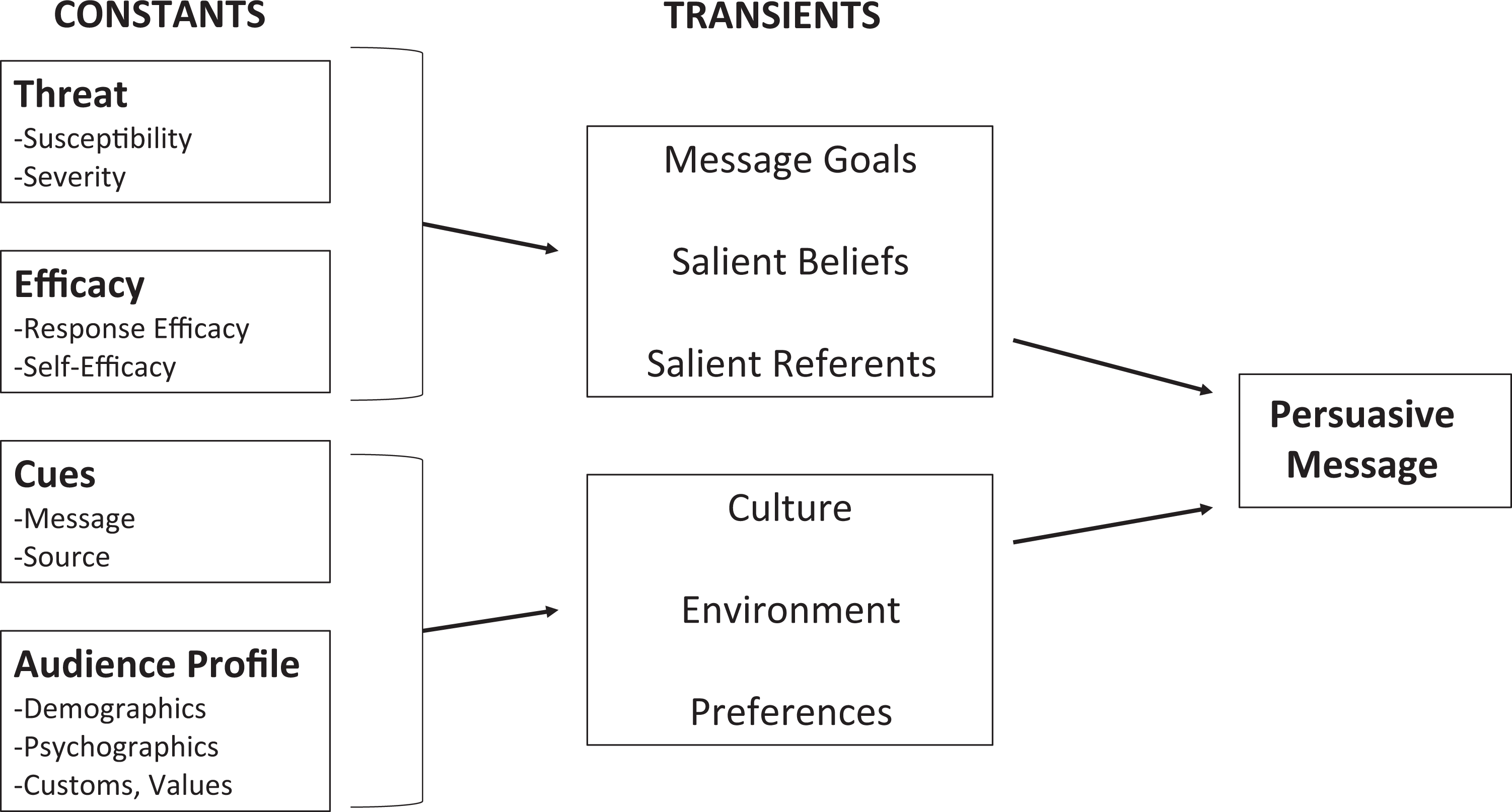
The Persuasive Message Framework. Source: Witte 46
Tailoring health education curricula and BCC that address the determinants of home fortification at multiple behavioral levels through varied communication channels, as has been effective in other similar programs, is also necessary in this setting. 47 Promotion of the SQ-LNS should link the desired behaviors to more salient community challenges; for example, the SQ-LNS could fight off other childhood illnesses and thus reduce trips to the hospital and cut healthcare costs for a household. BCC efforts also need to sensitize the community to the benefits of a 20-g SQ-LNS when the perceived foremost cause of nutrition-related illnesses in this setting is related to dietary quantity (“a lack of food in the body”).
The RAP approach also highlighted factors that may facilitate successful programming with an SQ-LNS used for prevention. This study found high acceptability of the SQ-LNS, similar to previous research. 48 -53 Modification of packaging for specific cultural contexts based on formative work has been successfully achieved in other settings 54 and should be considered in interventions that utilize specialized nutritious foods, both in Malawi and elsewhere. The sweet flavor of this product, in settings such as Ntchisi where monotonous dietary intake prevails, provides an incentive for caregivers to fortify their children’s complementary foods with it regardless of the health benefits, potentially reducing the practice of traditional forced hand-feeding due to poor child appetite stemming from dietary monotony.
The high acceptability of the SQ-LNS was reportedly one primary reason for its overuse (see Note 2). To overcome this barrier to smooth program implementation, a RAP approach can elucidate season-specific food-sharing practices that may help to predict when and how SQ-LNS overuse may also occur (Table 6), enabling more targeted communications to community members of different age groups and sexes. Positioning the SQ-LNS within the already-existing cultural food domain of caregivers during BCC and using emic terminology to appeal to a local, rather than a biomedical, concept of “healthy growth and development” may be more familiar and thus likely to resonate with caretakers. Also, using existing or preferred communication methods by local authorities (e.g., village chiefs and health surveillance assistants) to deliver salient, local messages to entire household units will be important during a BCC campaign. 13
By identifying local dietary practices, the findings from the RAP built upon health behaviors within the community for BCC development and tailoring. For example, during the postharvest period in Ntchisi, caregivers indicate that they enrich flour-based maize porridge with soybeans or groundnuts, a similar practice to home fortification of complementary foods with an SQ-LNS. Because this local practice already exists and is readily understood to be a healthful way to feed a child, BCC messaging should piggyback on this existing behavior and related perceptions. By contrast, the program may benefit by distancing itself from other existing behaviors. For example, targeted messages to concerned caregivers should clarify the distinction between consumption of Chiponde, the ready-to-use therapeutic food (RUTF) used for treatment of people living with HIV and malnourished children, and an SQ-LNS used for prevention, with care not to create undue stigma for those accessing such community-based management of acute malnutrition programs.
This study has some limitations. There was probably reactivity as a result of data collectors observing household food preparation and eating behaviors of community members. We employed repeated observations of the same households in order to minimize the negative manifestations of reactivity and documented frequency of reactive behaviors, as has been done in previous work. 55 Also, although some meaning may have been lost during the process of translation from Chichewa into English, we used verbatim translations with emic language to maintain local words and meanings, as well as using a triangulation of both methods and participants to help ensure data credibility. 56,57 We also employed member checking, a process in which we took key findings back to the communities themselves in order to verify and confirm the accuracy of the interpretations made by the research team. 56,58
Formative research has increasingly informed international nutrition programming in recent years, and researchers and practitioners are beginning to embrace this pre-implementation phase as critical to successful design and implementation of BCC programs. 12,17,21 Just as a new monitoring manual for home fortification has been developed for the intervention nutrition community 59 , so too should one be developed to guide formative research and translation of findings into program design. For the next steps of this program, a BCC team should utilize the ethnomedical model of nutrition-related illness to develop health messages that are aligned with local understanding and that utilize the emic terminology of Ntchisi. Table 6, which outlines projected SQ-LNS sharing based on current food-sharing patterns, should serve as a starting point for developing a BCC strategy that aims to reduce the likelihood of product sharing. Finally, momentum stemming from the positive community feedback and high acceptability of the SQ-LNS can be harnessed during early social mobilization efforts. Considering the complexities around home fortification, ethnographic formative research is an important step in thoughtful nutrition intervention design.
Footnotes
Acknowledgments
The authors gratefully acknowledge the Ntchisi community for participating in this study. Thanks also go for the invaluable data collection efforts by our local team, including Yamikani Kunashe, Evelyne Kamwendo, Ndapile Bwanausi, Chifundo Nsanjama, and Eric Maonga. We would also like to sincerely thank the World Food Programme head of suboffice in Ntchisi, Trust Mlambo, and the Government of Malawi, Ntchisi nutritionist James Mtonga for their on-the-ground help and unwavering support through the project. Finally, a special thanks to former Boston Consulting Group team leader Patrick Cleary, who provided much in-country support during the planning of the formative research.
Authors’ Contributions
Stephen Kodish and Joel Gittelsohn led the design, data collection, and data analysis of the formative research. Nancy Aburto, Mutinta Nseluke Hambayi, and Caitlin Kennedy supported the overall project with continual guidance, feedback, and support. Stephen Kodish drafted the first version of the manuscript. Nancy Aburto, Mutinta Nseluke Hambayi, Caitlin Kennedy, and Joel Gittelsohn critically reviewed and revised the subsequent drafts prior to finalization. All authors read and approved the final submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Stephen Kodish and Joel Gittelsohn were consultants to the World Food Programme, funded by the Children’s Investment Fund Foundation, and received support for the conduct of the research.