
Abstract
Background:
Childhood obesity has been growing steadily, at an earlier age, and currently comprises a public health issue. A number of studies have pointed to perinatal factors as possible determinants in the development of childhood obesity.
Objective:
To evaluate the influence of perinatal factors on the development of obesity in children and adolescents in southern Brazil.
Design:
Retrospective cohort study in which a linkage was made between anthropometric data of children and adolescents aged 0 to 15 years who had been registered in the Food and Nutrition Surveillance System (SISVAN) from 2008 to 2016 and their perinatal data registered in the Live Birth Information System (SINASC) from 2000 to 2014. The SINASC was used to extract maternal covariables (age, schooling, marital status), prenatal variables (parity and number of prenatal visits), and perinatal variables (type of delivery, sex, and birth weight). Variables such as age, inclusion in the Bolsa Família income transfer program, and the number of anthropometric evaluations were extracted from SISVAN.
Results:
The sample comprised 537 children and adolescents. The median age was 8 years (interquartile range: 2-11 years). The prevalence of obesity was 15.1%. Poisson regression revealed a higher risk of obesity in children born via cesarean delivery (relative risk [RR] = 1.48; 95% CI: 1.01-2.17), children of primiparous mothers (RR = 1.72; 95% CI: 1.16-2.53), girls (RR = 1.77; 95% CI:1.21-2.60), and those aged between 5 and 9 years (RR = 26.8; 95% CI: 3.75-191.55) and older than 10 years (RR = 20.74; 95% CI: 2.89-148.61).
Conclusions:
The linkage between SINASC and SISVAN allowed identification of prenatal and perinatal risk factors for the development of childhood obesity. These findings should contribute to the development of health promotion and prevention policies.
Background
Health information systems (HISs) supply data that provide insight into and allow monitoring of the health situation of a population, through health indicators that support the planning, management, and evaluation of health policies; health surveillance; and health care. 1 In Brazil, HISs have been increasingly used in research due to their availability and quality, 2 in addition to the low cost of HIS-based research and the possibility of population-based studies with nationwide coverage. 3
Among the HIS available in the country, the Live Birth Information System (SINASC), implemented by the Ministry of Health in 1990, aims to monitor the epidemiological profile of newborns nationwide as well as collect data on pregnancy, prenatal care, and childbirth, all drawn from information contained in the Statement of Live Birth. 4 Thanks to its good coverage, 5 greater completeness, 6,7 and higher reliability 5,8 compared to the Mortality Information System (SIM), the number of publications using SINASC data has been growing, mainly in the Southeast (44.1%) and Northeast (23.5%) regions of the country. 9 Furthermore, several studies are now using linkages between SINASC and other secondary databases, such as the Unified Health System Hospital Information System and, especially, the SIM, 9 to obtain additional insights.
In the context of nutrition, the National Food and Nutrition Policy (PNAN) describes the importance of the Food and Nutrition Surveillance System (SISVAN), aimed at local, continuous monitoring of the dietary pattern and nutritional status of individuals covered by the primary health care component of the Unified Health System, including beneficiaries of the Bolsa Família Program (PBF), a federal income transfer program aimed at very low-income families, 10,11 The SISVAN makes it possible to generate specific reports from each municipal Basic Health Units (BHUs), including individual monitoring of each registered user. Such information allows tracing of the epidemiological and nutritional profile of the assisted population and its determining factors, characterizing social groups at risk and providing inputs for policy-making, program design, and implementation of interventions, as well as providing evidence of the impact of these actions on certain populations. 11,12
Thus, considering the current epidemic status of obesity, 13 a significant increase in its prevalence at increasingly earlier ages, 14,15 the evidence that prenatal and perinatal factors may be determinants of its development (and of other chronic diseases), 16 -20 and the 2013 PNAN guidelines 10 on the need to carry out a comprehensive diagnosis of this problem at the BHU level through integration and interaction between available HIS, this study was designed to use a pioneering linkage of 2 important repositories of secondary data, that is, SINASC and SISVAN, to evaluate the influence of maternal, prenatal, and perinatal factors on child and adolescent obesity.
Methods
This was a retrospective cohort study of children and adolescents born in Porto Alegre, capital of the state of Rio Grande do Sul in the extreme south of Brazil, presented their anthropometric data registered in SISVAN between 2008 and 2016; and whose maternal, prenatal, and perinatal information could be correlated according to data recorded in SINASC between 2000 and 2014. This population received primary health care in the Unidade Básica de Saúde Santa Cecília affiliated with Hospital de Clínicas de Porto Alegre (HCPA), a university hospital of the Federal University of Rio Grande do Sul. Children and adolescents who had been born preterm or with congenital anomalies that might interfere with normal growth and development, as well as twins and children and adolescents whose anthropometric data were missing or incompatible with age, were excluded.
First, all children and adolescents under the care of the nutrition team, who were registered in SISVAN at BHU Santa Cecília/HCPA from 2008 to 2016 and who had anthropometric data (weight and height) available on file, were selected. Classification of obesity was performed using the body mass index (BMI)-for-age parameter, in WHO Anthro and Anthro Plus software (version 3.2.2.1). Based on the SISVAN protocol, 21 z scores were considered as the cutoff point for obesity, with z values above +3.00 standard deviations in children younger than 5 years and values above +2.00 standard deviations for children aged 5 years or older. Among the children and adolescents who were receiving anthropometric and/or nutritional follow-up, that is, for whom more than one anthropometric evaluation had been recorded in SISVAN during the period of analysis, only the first record was considered for the purposes of the analysis, prior to any type of intervention. Additionally, the inclusion of children and adolescents in the PBF was observed. No information on breastfeeding (BF) practices or dietary intake could be collected, as the data recorded in SISVAN were minimal.
The second stage consisted of linking the 2 databases—SISVAN and SINASC—to obtain maternal information about the prenatal and perinatal period, present at SINASC between 2000 and 2014, of these children and adolescents, registered with SISVAN between 2008 and 2016. Due to the impossibility of performing automatic linkage between the 2 databases, this process was carried out manually using data present in both databases (mother’s name, child’s birth date, and sex), and the data were double-checked by the main researcher. Initially, the search in SINASC was done through the mother’s name and later confirmed by the child’s date of birth and sex. Thus, another database was set up with information from anthropometric data registered in SISVAN and maternal, prenatal, and perinatal data in registered SINASC. For this reason, data processing and analysis took place between July 2017 and November 2018.
The maternal information of interest comprised age, educational attainment (measured in years of schooling), and marital status. Maternal age, which was reported continuously in the SINASC database, was categorized into 3 ranges (≤ 18 years, 19-34 years, and ≥ 35 years). Educational attainment—originally categorized in the SINASC as no schooling, primary school 1 (first-fourth grade), primary school 2 (fifth-eighth grade), secondary school (high school), some higher education, or a higher degree—was converted into years of schooling. The first 3 categories were pooled and considered as ≤ 8 years of schooling, the fourth category as 9 to 11 years of schooling, and the latter 2 categories were pooled and considered as ≥ 12 years of study. Marital status was recategorized dichotomously as “has partner” (married or cohabitating) and “no partner” (single, widowed, or divorced).
The prenatal parameters of interest were parity, number of prenatal visits, and type of pregnancy (singleton, twin, or triplet/other multiple). The parity variable, originally continuous in the SINASC database (relating to the number of live children), was dichotomized into primiparous or multiparous. Regarding the number of prenatal visits, the first 2 categories (none and 1 to 3 visits) were grouped into 0 to 3 visits, since it is known that in Brazil, 3 or less prenatal consultations are considered insufficient in terms of quantitative and qualitative 22 ; and the other categories were kept as in the original database: from 4 to 6 visits and equal to or more than 7 prenatal visits.
The perinatal parameters of interest were birth weight, gestational age, and mode of delivery (vaginal or cesarean). Birth weight could not be classified by adequacy to gestational age because gestational age was recorded in the SINASC as a categorical variable until 2011 (it has since been recorded continuously). Thus, birth weight was classified as low (< 2500 g) or not.
Initially, a descriptive analysis of the continuous and categorical variables was performed. Continuous variables were described as mean and standard deviation, when parametric, or as median and interquartile range, when nonparametric. Categorical variables were described as absolute and relative frequencies.
To analyze the associations between categorical variables, Fisher exact test was used when 25% or more of the expected values were less than 5, while for values smaller than 25%, Pearson chi-square test or continuity correction for 2 × 2 layouts was used. A significance level of 5% (P < .05) and 95% CIs were considered for all analyses. Those associations that proved significant in the crude analysis were carried forward to a Poisson regression model as an adjustment on multivariate analysis.
Data storage and processing were performed in Microsoft Office Excel software. Analyses were carried out in PASW Statistics for Windows, Version 18.0.
Results
The study included 537 children and adolescents, aged 0 to 15 years of age, who were registered in both SISVAN and SINASC (flow diagram in Figure 1). The median age was 8 years (interquartile range, 2-11 years). The prevalence of excess weight (overweight and obesity) was 34.1% (n = 183), while the prevalence of obesity was 15.1% (n = 81).
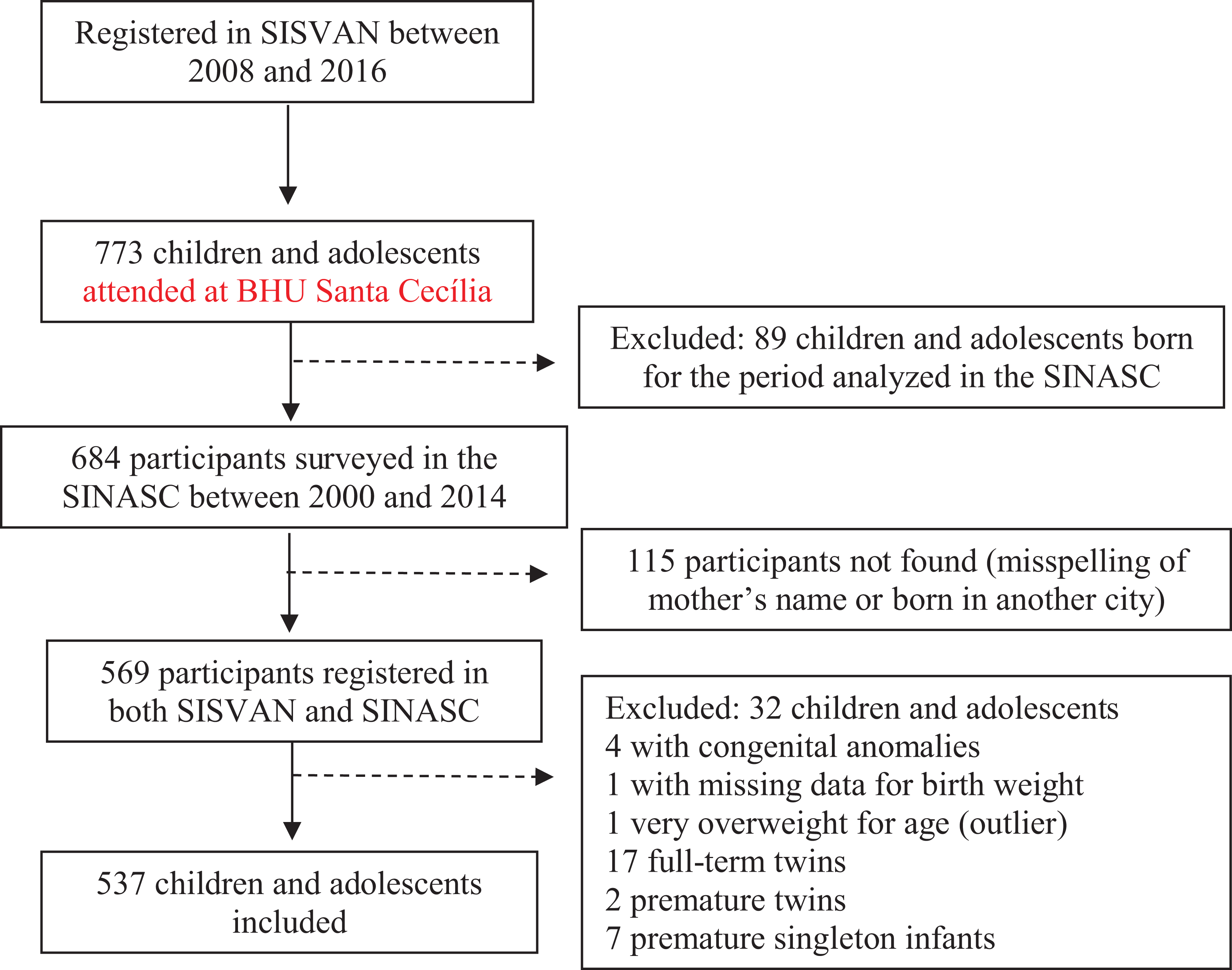
Flow diagram of participant screening. SISVAN indicates Food and Nutrition Surveillance System; SINASC, Live Birth Information System.
Table 1 describes the general profile of the sample. Overall, 52.3% (n = 281) of participants were male. The mean maternal age at birth was 26.28 (6.64) years. More than half of the children and adolescents (61.5%) had only one anthropometric evaluation recorded in SISVAN, and the median number of evaluations was 1 (interquartile range, 1-3).
Characteristics of Cohort Participants.a
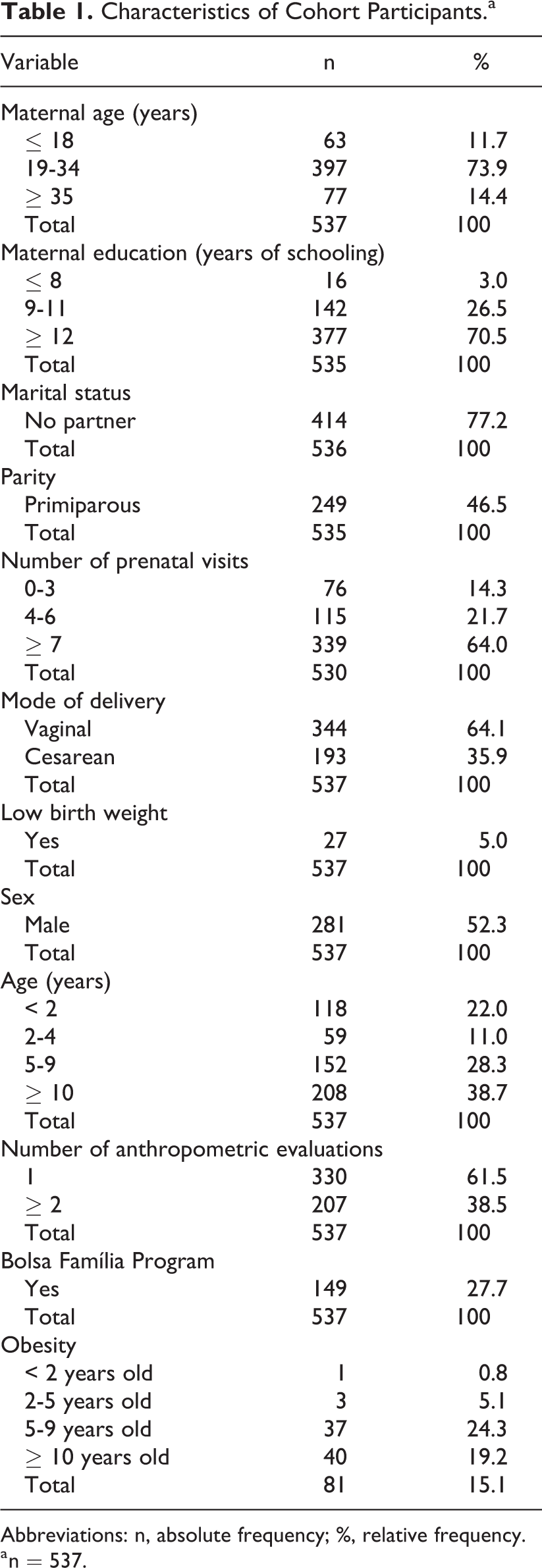
Abbreviations: n, absolute frequency; %, relative frequency.
a n = 537.
Bivariate analysis (Table 2) of maternal, prenatal, and perinatal factors with childhood obesity showed that children born via cesarean section, children of primiparous mothers, girls, and children older than 5 years were at higher risk of obesity. These associations remained significant in the model adjusted by Poisson regression (Table 3). In the 5 to 9 age-group, a 26-fold relative risk (RR) of obesity (P = .001; 95% CI: 3.75-191.55) was observed, while adolescents (≥ 10 years of age) showed a 20-fold higher RR (P = .003; 95% CI: 2.89-148.61) compared to children younger than 2 years of age. A greater number of anthropometric evaluations recorded in SISVAN and receipt of the Bolsa Família benefit were shown to be protective factors against childhood obesity on crude analysis. Nevertheless, this effect was not observed after adjustment on multivariate analysis.
Bivariate Analysis Between Obesity and Maternal, Prenatal, and Perinatal Factors.a
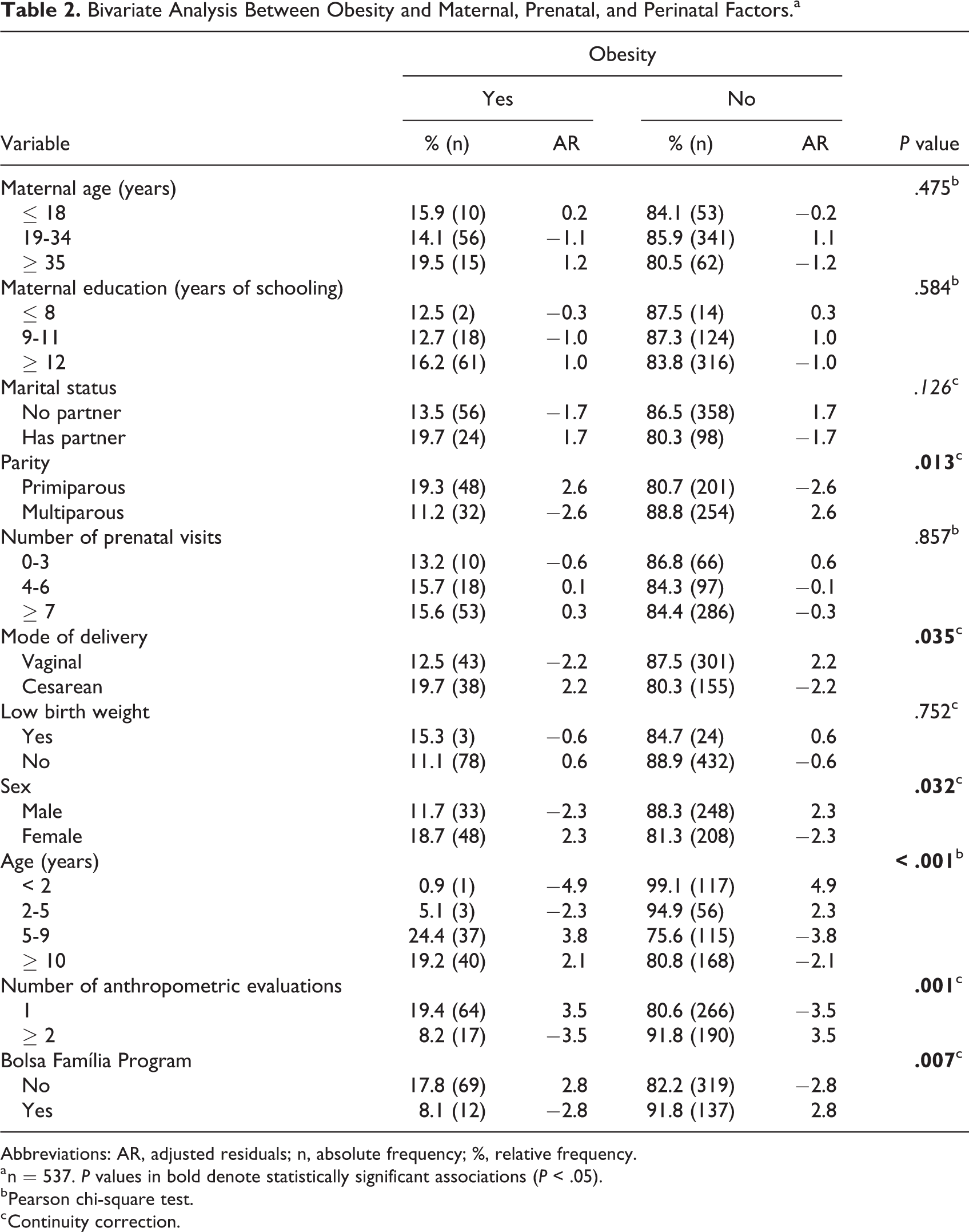
Abbreviations: AR, adjusted residuals; n, absolute frequency; %, relative frequency.
a n = 537. P values in bold denote statistically significant associations (P < .05).
b Pearson chi-square test.
c Continuity correction.
Model Adjusted by Poisson Regression for Significant Associations Between Obesity and Maternal, Prenatal, and Perinatal Factors.a
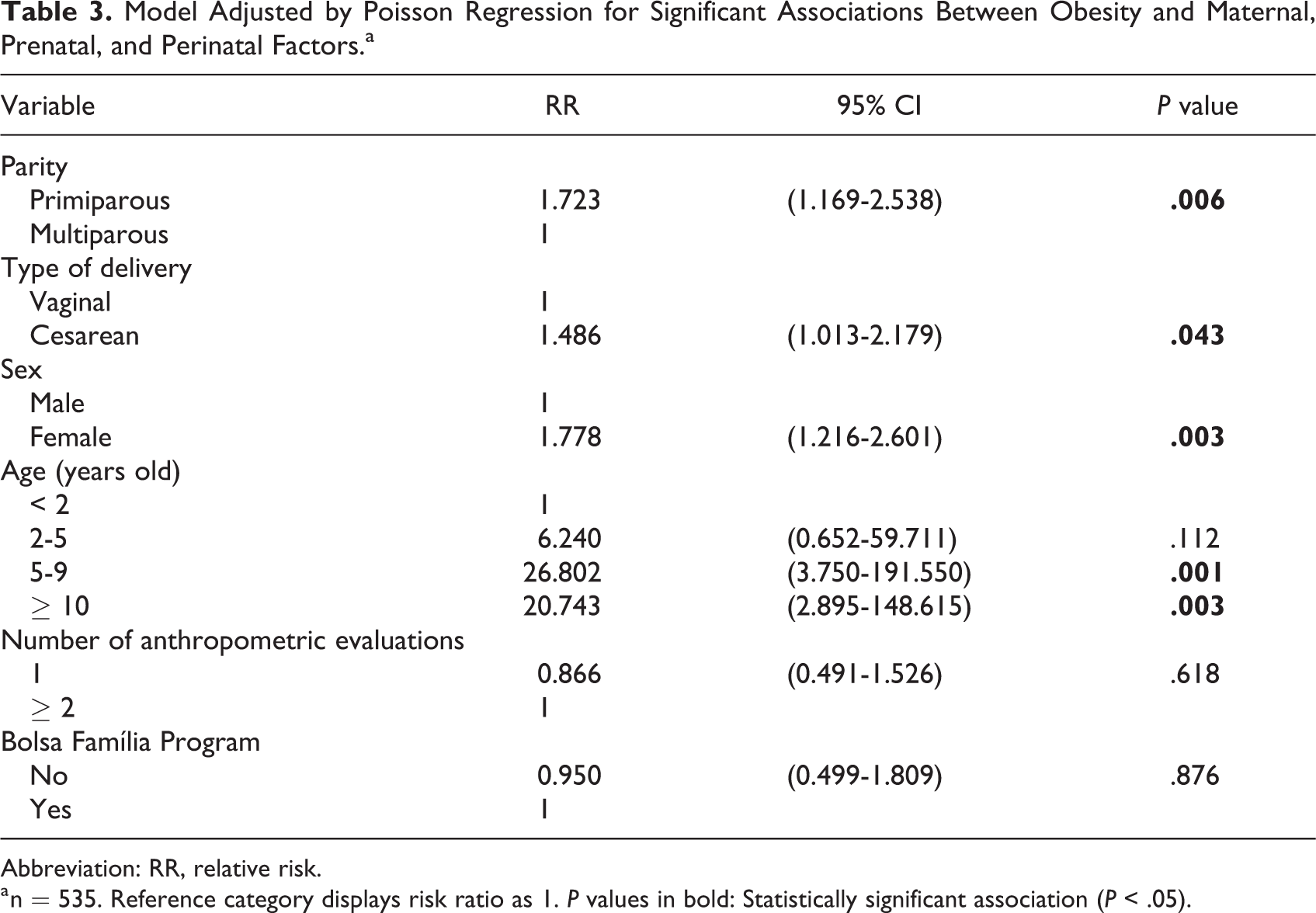
Abbreviation: RR, relative risk.
a n = 535. Reference category displays risk ratio as 1. P values in bold: Statistically significant association (P < .05).
Discussion
From the point of view of applying the linkage between the 2 secondary databases studied, it was possible to identify the possible factors associated with childhood obesity in children and adolescents born in the city of Porto Alegre, south of Brazil, and attended by the UBS Santa Cecília. Thus, among children and adolescents born in Porto Alegre, girls, children older than 5 years of age, children of primiparous mothers, and those born via cesarean delivery had a higher risk of obesity.
The prevalence of childhood obesity has increased sharply in recent decades, being considered a worldwide public health problem to be overcome. 13,14,23 -25 According to World Atlas of Obesity and World Health Organization, 25 Brazil will be in the fifth position in the ranking of countries with the highest number of children and adolescents with obesity in 2030, with only a 2% chance of reversing this situation if nothing is done. In Brazil, 7.9% of children younger than 2 years of age and 6.5% of children between 2 and 4 years of age are obese. 25 And for this age-group under 5 years, 5.1% of girls and 7.0% of boys being obese. 26
Among children and adolescents aged 5 to 19 years, the global obesity prevalence increased from 11 million to 124 million between 1975 and 2016 and is estimated to exceed the prevalence of malnutrition by 2022. 13 National data from the 2008 to 2009 Family Budget Survey 24 also suggest an increase in the prevalence of obesity in this age range in Brazil, with 14.3% of children aged 5 to 9 years and 4.9% of adolescents aged 10 to 19 years affected. More specifically in the southern region, more recent data show that 18.4% of children between 5 and 9 years old are obese. 25 Regarding sex differences in the same age-group, boys presented higher worldwide rates (7.8%) when compared to girls (5.6%), and Brazil had even higher obesity rates, with 12.7% of boys and 9.4% of girls, aged 5 to 19 years, being obese. 13
In contrast, the results of the present study showed a 78% greater risk of obesity in girls, although current evidence shows higher rates of obesity in boys. Nevertheless, in both Europe and Latin America, girls gained more weight than boys over the last 4 decades, narrowing this difference. 13
Another important finding observed was a higher risk of obesity in children from the age of 5 years, with the 5 to 9 age-group being most at risk (RR = 26.8; 95% CI: 3.75-191.55) and those aged 10 to 15 years experiencing a 20-fold risk of obesity compared to children younger than 2 years of age.
Corroborating these findings, there is mounting evidence of early childhood as a critical window for the development of later sustained obesity. 27 -29 A population-based longitudinal study evaluated weight and adiposity gains in 51 505 healthy Germans through BMI trajectory during childhood (0-14 years of age) and adolescence (15-18 years) and found that the majority of adolescents had normal BMI between 1 and 2 years of age, remaining within normal range throughout childhood. The authors also observed that approximately half of the obese adolescents (53%) were overweight or obese from the age of 5 years, and almost 90% of children who were obese at 3 years of age were overweight or obese in adolescence, exhibiting greater acceleration in weight gain between 2 and 6 years of age, regardless of gender. 29 This highlights the importance of observing the BMI pattern in early childhood, that is, when exaggerated weight gain arises or persists after 2 years of age, given that the risk of obesity in adolescence appears to manifest itself between the ages of 3 and 5 years. 29
Regarding cesarean delivery, the risk of obesity was 48% higher in children and adolescents delivered via this route than in those born by vaginal delivery (P = .043; RR = 1.48; 95% CI: 1.01-2.17), irrespective of gender, age, and parity. Several findings in the literature corroborate these results. Mueller et al 20 demonstrated that children born by cesarean delivery had 46% higher odds of developing obesity at 7 years of age, irrespective of antibiotic exposure during the prenatal period. In a multicenter Chinese study of 18 780 children, Liang et al 30 found a 51% greater probability of obesity among children born by cesarean delivery, irrespective of birth weight, gestational age, maternal age, and educational attainment, despite higher daily intake of meat, fruits, and vegetables and shorter durations of sedentary behavior when compared to children born via vaginal delivery. A prospective cohort study found a 2-fold likelihood of obesity at 3 years of age in children born via cesarean delivery, irrespective of maternal BMI and birth weight. 31
Nevertheless, this association seems to be more pronounced in the first years of life, but not later. 32 -34 The authors suggest that the magnitude of this effect may decrease the extent to which children grow, attributing it to increased exposure to an obesogenic environment, wherein factors such as eating habits and physical activity may become more important than the type of birth, which may mask this association between cesarean delivery and later obesity development. 30,34,35
It is also known that children born by cesarean delivery are less likely to start BF 36 and are more prone to early weaning, regardless of income, schooling, parity, prematurity, maternal physical and mental health, ethnicity, or BF difficulties. 37 One possible explanation for this association is interruption by cesarean delivery of the hormonal pathway that stimulates lactogenesis, either due to maternal stress or to reduced secretion of oxytocin, thus reducing the production of breast milk. 37 This could be a possible confounding factor on the influence of mode of delivery on the development of childhood obesity, as the protective effect of BF against the development of obesity is well-established in the literature. 38
The risk ratio of obesity in children of primiparous mothers should also be highlighted (P = .006; RR = 1.72; 95% CI: 1.16-2.53). Studies have shown that both maternal weight 39,40 and the birth weight of the child tend to increase with parity. 41 Thus, firstborn infants tend to have a lower birth weight than their siblings, 42,43 which could explain the well-established potential association between low birth weight and later development of obesity. 16 -20 Corroborating these findings, recent study also found an association between being an only child and a greater chance of obesity at 4 to 8 years of age, irrespective of birth weight, food insecurity, and maternal marital status, depression, or weight. 44
A recent meta-analysis showed that both lower birth order and having fewer siblings are associated with risk of obesity (odds ratio = 1.46, 95% CI: 1.17-1.84), suggesting that only children are at increased risk. The authors attribute this association to the fact that only children have a higher energy intake, perhaps because their mothers are more concerned with persuading them to eat than mothers with multiple children, or because additional siblings may decrease the availability of food for each child, particularly in more vulnerable families (resulting in lower odds of obesity). Only children may also engage in less physical activity and have a higher screen time than children with siblings. 45 In addition, Brazilian and international studies in infants have shown that primiparity is a risk factor for early weaning. 46,47 These factors, such as birth order, lower food insecurity, lower level of physical activity, and early weaning, may contribute to the fact that children of primiparous women have a higher prevalence of obesity.
Although our findings are already described in the literature, we highlight the differential of our study in using secondary data that is easily accessible in research health, with the main advantage of saving time and resources spent.
Brazil has several HIS, among which SISVAN is the one with the greatest scarcity of studies exploring its coverage, being still incipient and underused in Brazilian municipalities, especially for monitoring of food intake, as observed in the present study. However, better coverage is observed at ages 0 to 5 years and 5 to 10 years, presenting a significant relationship with the Family Health Strategy and focusing strictly on nutritional status. 48,49
Particularly in Porto Alegre, BHU Santa Cecília has the most effective coverage of SISVAN when compared to other regions in the city. The BHU Santa Cecília was inaugurated in October 2004, the result of a partnership between the City Hall, HCPA and the Federal University of Rio Grande do Sul, with the exclusive objective of providing primary care, being a teaching scenario for health courses. Its coverage area reaches approximately 35 000 residents.
Conversely, SINASC, as previously mentioned, is already a well-established database with high coverage and excellent completeness and is increasingly being used in population-based studies. 7,8 Nevertheless, they are still little used as a basis for population studies, especially in southern Brazil. 3
However, there is a need to ensure quality of its information, being essential that primary health care professionals be encouraged to enter complete and reliable information in these secondary databases in order to assist in the design of more effective local strategies to promote the healthy growth of children and adolescents.
The main limitations of the present study are the impossibility of classifying birth weight by adequacy for gestational age, due to the categorical presentation of the variable gestational age in the SINASC (which may explain the absence of association of this variable with childhood obesity in the present sample); the lack of data regarding BF in the SISVAN, which could be a possible confounding factor between parity, mode of delivery, and childhood obesity; the possibility of information bias linked to the use of secondary data; and the incompleteness of the SINASC and SISVAN systems.
Furthermore, although prenatal care may have a positive effect in preventing obesity in offspring, according to previous publications, 50,51 the design and sample size of the present study were not the most appropriate for assessing this effect. It is possible that for these reasons, no association between prenatal care and obesity was observed as a result of this study.
As a strength of the study, we highlight our pioneering approach in linking these 2 important secondary databases in order to elucidate possible causal relationships of maternal, prenatal, and perinatal factors with obesity in children and adolescents, since there is not until the studies in the literature that link SISVAN with other HIS.
Thus, a new possibility of using these data is suggested, making it possible to obtain evidence about the health conditions of the population and allowing the planning, organization, and evaluation of health services, as well as the monitoring of the epidemiological characteristics of a population. In addition, they provide subsidies to outline health policies and support decision-making by public health managers.
Conclusion
Health information systems are excellent tools for gaining insight into and monitoring the health situation of a population, with low cost being their main advantage. This study established an unprecedented linkage between 2 secondary databases, SINASC and SISVAN, allowing the identification of possible risk factors for the development of obesity in childhood and adolescence: children born of cesarean delivery, children of primiparous mothers, girls, and those aged older than 5 years exhibited an increased risk of childhood obesity.
Therefore, it is crucial to invest in maternal and child health care with a particular focus on these risk factors. Such investment should include actions designed to reduce early adverse events occurring in intrauterine life and to prevent the development of obesity and other chronic diseases in adulthood. The importance of early identification and nutritional monitoring of these at-risk children cannot be overstated, particularly in the first years of life, with an emphasis on maintenance of BF up to 2 years of age or later and adequate introduction of complementary feeding for the establishment of healthy habits since childhood.
Footnotes
Authors’ Note
JMG contributed to conception and design, analysis and interpretation of data, drafting the article, and final approval of the version to be published. MDS, MB, and IS contributed to data acquisition and final approval of the version to be published. VLB and CHS contributed to conception and design, interpretation of data, critical revision for important intellectual content, and final approval of the version to be published. This study was approved by the HCPA Research Ethics Committee of the HCPA under opinion number 2106241. All researchers involved signed a Secondary Data Use Agreement ensuring the confidentiality of information obtained and its use for research purposes only.
Acknowledgments
The authors are thankful for the statistical support provided by the Hospital de Clínicas de Porto Alegre (HCPA) Graduate and Research Group (GPPG).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: HCPA Research and Event Incentive Fund (FIPE).