
Abstract
Background:
Surveillance of nutrition indicators is critical for informing nutrition policies and programs. The failure by many sub-Saharan countries to maintain functional surveillance systems for maternal and child health (MCH) hampers their capacity to achieve the 2030 Sustainable Development Goals relevant for MCH. The nutrition surveillance system (NSS) for MCH in the southern African country of Lesotho is no exception to this problem despite the country having some of the highest maternal and child mortality ratios globally.
Objective:
The study reviewed Lesotho’s quantitative nutrition surveillance data and qualitatively analyzed the structure and functionality of Lesotho’s NSS to identify imperatives for an effective nutrition surveillance policy framework for MCH in the country.
Methods:
Descriptive quantitative analyses were based on NSS data and nationally representative Lesotho Demographic and Health Survey (LDHS) data while qualitative analysis on data obtained through interviews with purposefully selected key informants working in the NSS of Lesotho was based on grounded theory.
Results:
Nutrition surveillance system data were inconsistently compiled across Lesotho’s 10 districts, while LDHS data suggested that stunting, maternal anemia, child overweight, and low birth weight remain high. Challenges with the NSS were linked to poor coordination of the NSS due to an indistinct organogram of nutrition offices and poor cooperation among stakeholders in the NSS.
Conclusions:
To improve the NSS in Lesotho, the most critical imperative is to capacitate the Food & Nutrition Coordinating Office which in turn should create distinct nutrition offices yet with adequate cooperation and clear benchmarks for monitoring and evaluation of the NSS.
Keywords
Introduction
Given the significance of nutrition as a core component of health and well-being, the periodic surveillance of nutrition status in all populations is critical for informing nutrition policies and programs. 1 Nutrition surveillance refers to the continuous monitoring of nutrition-related time trends for various ends including predicting change in nutritional status, monitoring factors that underpin national and subnational food production, distribution and consumption, and identifying nutritional imbalance in affected populations and places. 2 -6 Many developing countries, particularly in sub-Saharan Africa, are failing to implement effective nutrition surveillance systems (NSSs), 2,7 including those for maternal and child health (MCH) despite this region having unacceptable maternal and child mortality ratios. 8
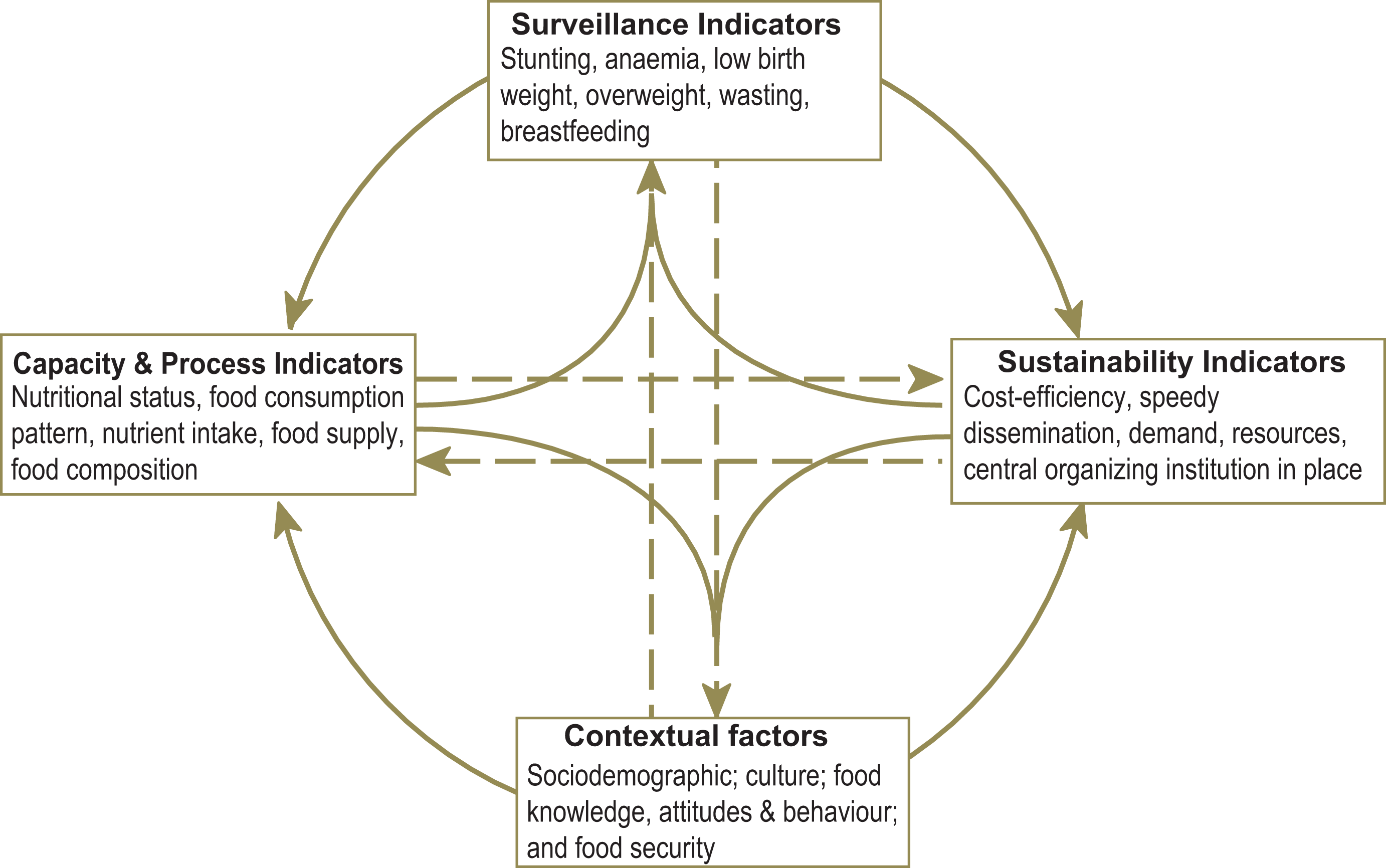
To achieve effective NSSs, World Health Organization (WHO) reiterates that NSSs should be based on broad multisectoral frameworks (see Figure 1). 2 Fundamentally, ministries responsible for NSSs, besides reporting nutrition indicators themselves, should collect capacity, process and sustainability indicators, and adequately consider contextual factors in the local surveillance framework. 2,10,11
Limited financial and human resource bases remain the biggest constraint to functional surveillance systems. 12 Friedman notes that out of 16 developing countries recently surveyed, only 8 African countries, namely, Mozambique and Zambia in Southern Africa, Djibouti, Ethiopia, Somalia, Sudan, Uganda in East Africa, and Democratic Republic of Congo in Central Africa, had institutionalized NSSs. Nonetheless, all the 8 countries with established surveillance systems had their surveys characterized by limited geographic coverage, poor sample sizes, and numerous data gaps. 13 Despite recommendations for WHO member countries to improve their surveillance systems by monitoring at least 6 indicators critical for monitoring the success of MCH programs in addressing nutrition challenges, full compliance remains far off. 2 Of note, the recommended 6 indicators are micronutrient status of children and women of childbearing age, child feeding practices, and anthropometric status of children aged 0 to 59 months, particularly overweight, stunting, low birth weight (LBW), and wasting. 2
World Health Organization recommends that despite funding challenges, developing countries should at least strive to collect secondary data from feeding centers, health facilities, and community-based data collection sites such as mass screening programs for malnutrition in children; and where possible primary data should be collected through repeated cross sectional surveys, community-based sentinel monitoring or from schools. 2 However, due to poor NSSs, nutrition policies in these countries are often based on scanty data from small cross-sectional studies, 12,14 which fall short of the multisectoral framework recommendations of the WHO, 2 with data collection methods in most studies being inconsistent. 6
Lesotho is one sub-Saharan country with a challenged NSS that is likely to affect the country’s progress in reducing maternal and child mortality ratios, which were estimated at 487 per 100 000 and 93.5 per 1000 live births in 2015, respectively. 15 Timely and accurate nutrition surveillance data are therefore needed to guide the country’s nutrition policy. This study evaluated the NSS for MCH in Lesotho, with the overarching aim to identify imperatives for improving the country’s NSS policy framework.
Nutrition Situation and the Surveillance Policy Framework in Lesotho
The sub-Saharan country of Lesotho, located within the border of South Africa, has 57.1% of its estimated 2 million population living below the official poverty line of US$1.25 per day. 16 With only 10% of the land being arable, 17 food insecurity is a challenge for the inhabitants of Lesotho, 77% of whom live in the rural areas and are dependent on subsistence farming. 18 Of note, Lesotho has 10 administrative districts categorized into 4 agroecological regions, namely Lowlands, Foothills, Senqu River Valley, and Mountain Range. 19 Of the 10 districts, Maseru, Berea, Leribe, and Botha-Bothe are predominantly in the Lowlands where there is relatively higher rainfall and more arable land compared to the other regions; Mafeteng, Mohale’s Hoek, and Quthing are in the Foothills characterized by lower rainfall and less arable land, although these districts also extend to the lowlands and the fertile Senqu River Valley; Qacha’s Nek, Mokhotlong, and Thaba-Tseka are in the extremely cold Mountain Range, also with some smaller parts of these districts lying in the Senqu River Valley. 19 With low food production in rural communities, dependence on remittances from migrant workers in South Africa and social grants by rural households remains the norm. 20,21 High unemployment in urban areas, estimated at 29.2%, 22 also means that a significant proportion of the urban population also faces hunger and malnutrition.
Lesotho’s nutrition surveillance policy framework, which is guided by the National Food Policy (2005) and the Lesotho National Action Plan for Food Security (2007-2017) spearheaded by the Ministry of Health (MoH) and the Ministry of Agriculture and Food Security (MAFS), respectively, 23 has been criticized for failing to eradicate hunger and malnutrition particularly in children and pregnant women. Of note, the Hunger and Nutrition Commitment (HANC) index which ranges from 1 to 5 where lower ranks signify more compliance, measures the level of commitment to reduce hunger versus that of reducing malnutrition. 24 For example, South Africa’s HANC index (0.3/3.5) indicates a higher commitment to reducing hunger than malnutrition. 24 Lesotho’s HANC index 24 which is estimated at 1.5/4.5 therefore implies that the country has even less equitable commitment to reducing hunger than malnutrition compared to the neighboring South Africa, with disproportionately more effort being put in reducing hunger. Lesotho therefore faces severe challenges in achieving MCH.
Methodology
Study Design and Setting
The study used a triangulation of quantitative and qualitative data to evaluate the NSS for MCH in Lesotho. Quantitative assessment was based on benchmarking surveillance data against mandatory nutrition indicators 2 while qualitative analysis was based on interview data obtained from policy makers and key informants (KIs) purposefully selected for their role in the NSS from the MoH, MAFS, supporting partners, and nongovernmental organisations (NGOs), who were all located in the capital city, Maseru except District Health Management Team (DHMT) whose staff were based in Mafeteng and Leribe districts.
Interview Guide and Validation
The interview guide was designed by the researcher following guidelines for evaluating surveillance systems 25 and with peer inputs from a nutrition expert (PhD graduate on nutrition). The interview guide sought to understand: (1) the structure of the surveillance system; (2) surveillance methodologies for maternal and child nutrition; (3) challenges faced in carrying out the surveillance activities, and (4) stakeholder cooperation in the surveillance system. The interview guide was translated to vernacular Sesotho and back-translated to English with the help of a language specialist for verification. The interview tool was piloted with 2 other nutrition experts for validation.
Data Collection
Interviews were conducted between January and May 2018. Key informants were identified using a “snowball” approach, starting with those working in the relevant line ministries being asked about which agencies/personnel to interview next. A total of 15 KIs were interviewed, with interviewees’ responses tape-recorded. These were namely, 2 nutrition officers in the MoH; 4 principal nutrition officers in the MAFS; 2 nutrition officers at Food & Nutrition Coordinating Office (FNCO); 2 World Food Program (WFP) officers; 2 DHMT officers; 1 officer at the Demographic and health Survey office; 1 officer at Disaster Management Authority (DMA), and 1 officer at United Nations International Children's Emergency Fund (UNICEF). All interviews, which lasted 30 to 45 minutes, were conducted in person by 2 interviewers, and these excluded the author. Relevant policy documents were also obtained from MoH and MAFS.
Nutrition surveillance system data were obtained from the quarterly National Nutrition Surveillance Bulletin collected from each district across the country for the years 2002, 2003, 2005, 2007, and 2015, while nationally representative data for nutrition indicators were extracted from the Lesotho Demographic and Health Survey (LDHS) reports for 2004, 2009, and 2014. Six variables with data available were collected, namely LBW, stunting, underweight, exclusive breastfeeding, wasting, and vitamin A supplementation coverage. Notably, data for the quarterly nutrition bulletin are compiled from routine monthly data collected by the DHMT officers from the 10 districts of Lesotho. Under-weight data are compiled by community health workers from maternal, newborn, and child health facilities’ registers for growth monitoring, whereas LBW and other malnutrition data are abstracted from hospital records.
Data Analysis
Tape recorded interview data were manually transcribed and coded, based on the constant comparative method 26 to identify themes related to the structure, functionality, and constraints to the surveillance system, and thereafter to identify imperatives for improving the NSS. To ensure reliability and consistency of data, a second coder with expertise in qualitative coding was consulted and the final codes were agreed to by all the coders. Transcribed qualitative data were validated with KIs through member checking 27 (second visits to all the interviewees) within a 4-week period to confirm interview themes and for purposes of triangulation, 28 that is, to check whether qualitative data from interviews complemented the NSS data. During the second visits, KIs were also asked to express their opinions concerning the trends of the indicators and possible reasons for missing data.
Emerging themes were summarized through open coding by breaking down data into distinct parts to allow a comparison of similarities. Axial coding was then applied to find connections in the themes associated with NSS, making recourse to the principles of grounded theory analysis. 26
For quantitative data, mean quarterly statistics were calculated using Stata version 13 (StataCorp, College Station, Texas) from the raw quarterly NSS data (Raw NSS data are available from the author). Descriptive analysis of the regional and time trends in the mean quarterly NSS data was then carried out, with further comparisons being made against the nationally representative data from LDHS, based on WHO benchmarks for nutrition indicators. 2
Ethical Clearance
This study was approved by the institutional ethical review board of the author’s institution and the ethics committee of Lesotho’s MoH. Key informants agreed to be interviewed through written informed consent and agreed to the use of anonymized quotations in this report. Identity information for KIs were not included in this report to protect their anonymity.
Results
Nutrition Indicator Trends
Table 1 presents the mean quarterly NSS data. Note the general improvement in the trend for LBW and underweight, with the exception of 2 districts, Mokhotlong and Thaba-Tseka in the mountain range (Table 1). Also note the unavailability of 2015 LBW data in 1 Foothills district, Mafeteng.
Quarterly Surveillance Data for Maternal and Child Nutrition Indicators by District.a
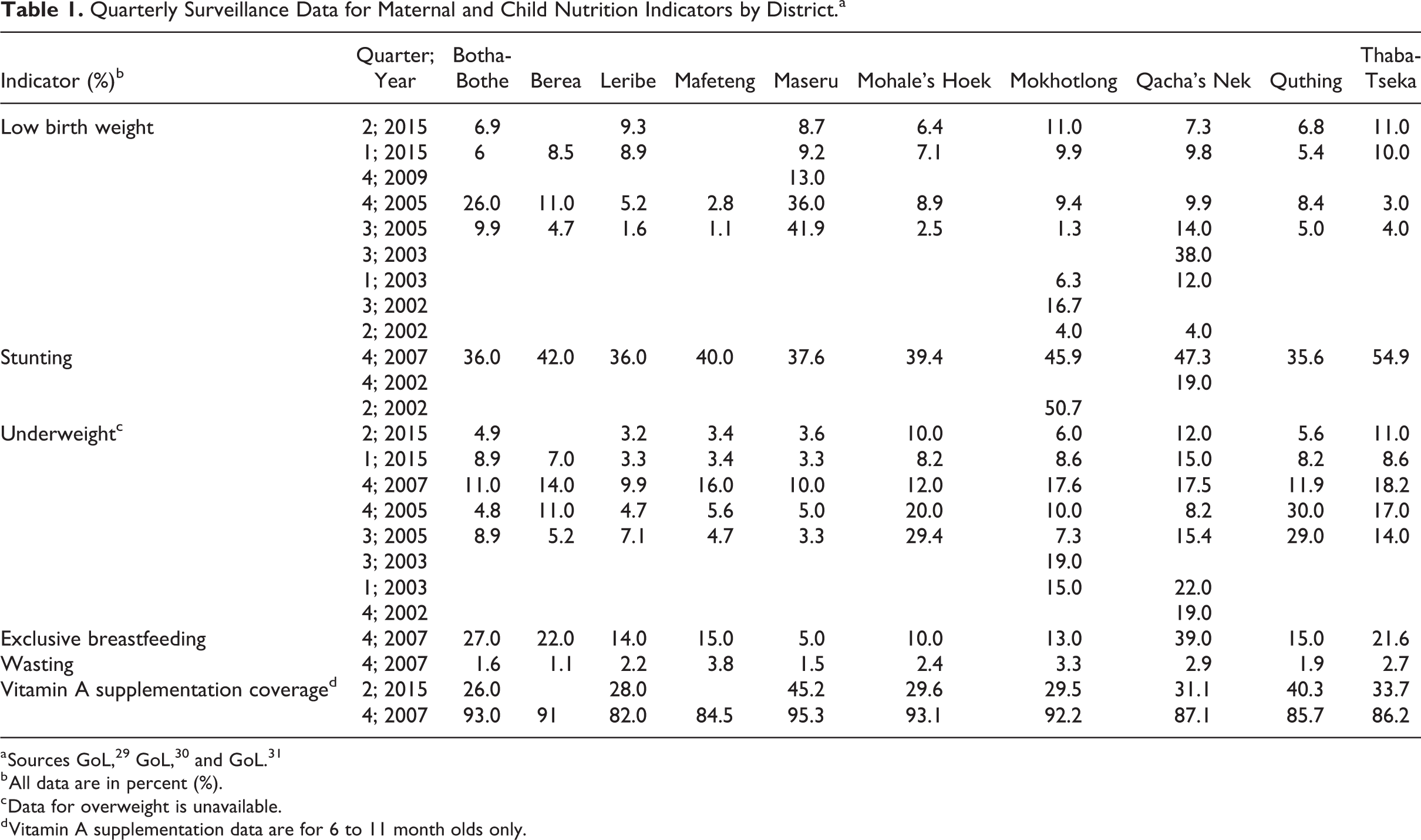
b All data are in percent (%).
c Data for overweight is unavailable.
d Vitamin A supplementation data are for 6 to 11 month olds only.
Except for Qacha’s Nek, no follow-up data for stunting and wasting were available since the fourth quarter of 2007 (Table 1). The 2007 fourth quarter data for these 2 indicators revealed that there was high levels of stunting across all the districts in that year, with exceptionally high levels this indicator (>50%) being recorded in Thaba-Tseka, whereas wasting was relatively low across all the districts in the same fourth quarter of 2007.
Vitamin A supplementation coverage declined between 2007 and 2015 by more than half across all districts while exclusive breastfeeding in the fourth quarter of 2007 was largely below 30% except for Qacha’s Nek in the Mountain Range, with Maseru District in the Lowlands having the lowest proportion of 5% (Table 1). Note the lack of data for maternal anemia and overweight data in the NSS across all districts. Table 2 presents the trends of the 6 mandatory indicators and the key mitigation strategies for the nutrition outcomes.
Trends in 6 Mandatory Nutrition Indicators From Lesotho Demographic and Health Survey (LDHS) and Key Interventions.
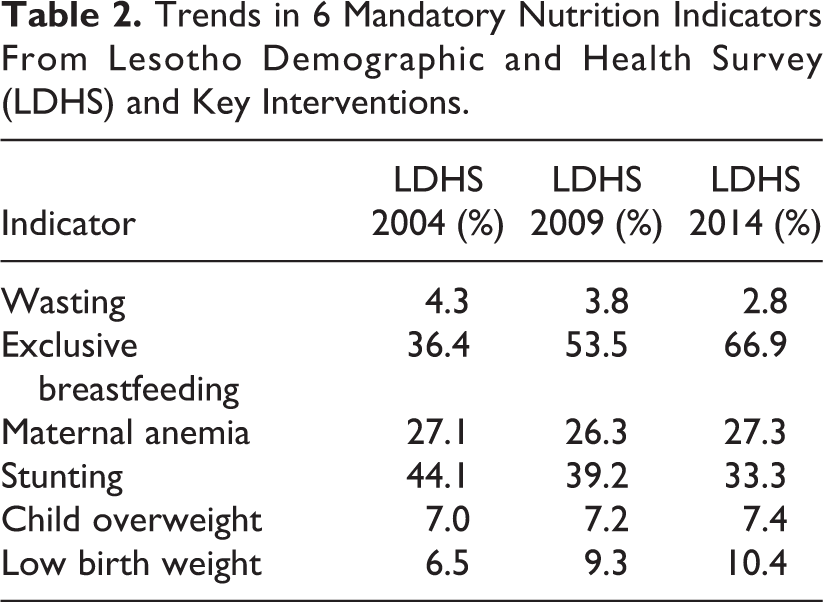
Note the general improvement for wasting, exclusive breastfeeding, and stunting between 2004 and 2014, although stunting remained high in 2014 (Table 2). Of the remaining 3 indicators in Table 2, child overweight and LBW deteriorated between 2004 and 2014 while maternal anemia slightly improved in 2009 and deteriorated to 2004 levels in 2014. Notable in 2014 is that stunting, maternal anemia, child overweight, and LBW remain of critical concern to MCH in Lesotho.
However, comparing Tables 1 and 2, LBW deteriorates in the LDHS survey data (Table 2) while it generally improves in the NSS (Table 1). The other indicators are incomparable due to lack of data in the NSS in Table 1. For example, whereas the NSS has been tracking underweight data, the LDHS reports child overweight data. Similarly, the LDHS reports on maternal anemia, data which has not being surveyed for in the NSS.
Structure, Functionality, and Constraints to the National Surveillance System
Food & Nutrition Coordinating Office, established in 2002, was the principal stakeholder for the NSS, with 2 ministries, MoH and MAFS being responsible for NSS data collection. The FNCO compiled nutrition surveillance data provided by MoH and MAFS through the Health Management Information System (HMIS), and was responsible for producing a quarterly national nutrition surveillance bulletin which identified geographic areas and groups at risk of malnutrition in the 0 to 59 months category, and also issued early warnings. The FNCO was also responsible for monitoring measles immunization and vitamin A supplementation.
At the time of data collection, the FNCO was manned by 2 nutrition officers and 1 statistician, all under the supervision of the FNCO coordinator. The MoH, on the other hand, had 3 principal officers who were responsible for nutrition surveillance and elimination of micronutrient deficiencies; maternal and infant and young child nutrition; nutrition education and nutrition in HIV/AIDS. Concerning data collection for the NSS, the procedure was outlined as follows: The MoH compiles NSS data from health centres through monthly registers collected by the DHMT, and is the main source of data for the surveillance system [Nutrition Officer, FNCO]. …additional officers for monitoring & evaluation and attendant officers for nutritive diseases; infant nutrition; preventive nutrition; growth monitoring; maternal & family nutrition and micronutrient issues. [Nutrition Officer, MoH]
Supporting partners, particularly DMA, WFP, UNICEF, and World Vision, played significant roles in the NSS, with UNICEF being the main funder and technical advisor for the FNCO. Disaster Management Authority was responsible for conducting Community Health Surveys and Lesotho Vulnerability Assessment Committee (LVAC) surveys. World Food Program provided technical assistance to UNICEF, World Vision, and WHO in their joint programs for monitoring severely malnourished children, pregnant women, and breastfeeding mothers.
The FNCO confirmed that they were not consistently producing the quarterly bulletins which carried the nutrition indicators, with some quarterly bulletins not being released at all. The FNCO has not been tracking most of the six mandatory indicators since 2002 due to untimely submission of data, incomplete and entirely missing data cohorts. The bulletin stalled in 2015 because MoH has not been submitting any data since then. [Nutrition Coordinating Officer, FNCO] The spatial distribution of the LDHS surveys and the quality of raw data analysis are unsatisfactory. The surveys are too general, lacking specific data for calculation of certain nutrition indicators. [Nutrition Officer, MoH] Most of our assessments are small surveys based on limited survey criteria and analysis. [Community Nutrition Officer, MAFS] …mountainous terrain that restricts access to some areas, low education levels of mothers, and inadequate access to health services limit participation by certain population groups [Community Nutrition Officer, MAFS] …inadequate capacity to monitor district nutrition officers and area technical officers. [Community Nutrition Officer, MAFS] The status of nutrition indicators for Lesotho may be due to poor knowledge of nutrition among pregnant women and breastfeeding mothers, including feeding habits and rural agricultural practices which often lack diversity. [Community Nutrition Officer, MAFS]
Cooperation Between Line Ministries and Supporting Partners
Key informants at MoH and MAFS revealed that despite considerable information sharing between the ministries and NGOs such as WFP, UNICEF, and WHO, cooperation was still weak. It was clear that organisations such as the WFP had capacity to inform the NSS program although this opportunity was underutilized. For example, one KI at WFP expressed that: Yes, cooperation in surveillance activities is possible. Nutrition surveillance data such as exclusive breastfeeding is obtainable from WFP’s programme. [WFP 2] WFP provides nutritional foodstuffs including supplementary meals fortified with macro- and micro-nutrients particularly proteins and vitamins to people living with HIV; and is also working with the MoH on one program, Safety Net, to identify malnourished patients in health facilities. [WFP 1] Incoherent organisation affects nutrition surveillance programmes in the country. For example, LVAC and LDHS data on stunting are analyzed in parallel. [WFP 2] Cooperation is possible across technical working groups, committees and task forces, such as the Health and Nutrition Team, Water and Sanitation and Micronutrient Task Forces. [Nutrition Officer, MoH]
Imperatives for an Effective NSS in Lesotho
Figure 2 presents the emerging themes finally regarded as imperatives needed to address challenges in the NSS for Lesotho. Identified imperatives were namely, to strengthen the office of the FNCO as the overarching coordinator of the NSS; putting in place distinct organograms of nutrition offices within the respective ministries; cooperation to leverage on existing networks for better coverage and quality of nutrition surveillance indicators; deliberation on contextual factors hampering collection of surveillance data; improving monitoring and evaluation; and considering sustainability, capacity, and process factors in the NSS.
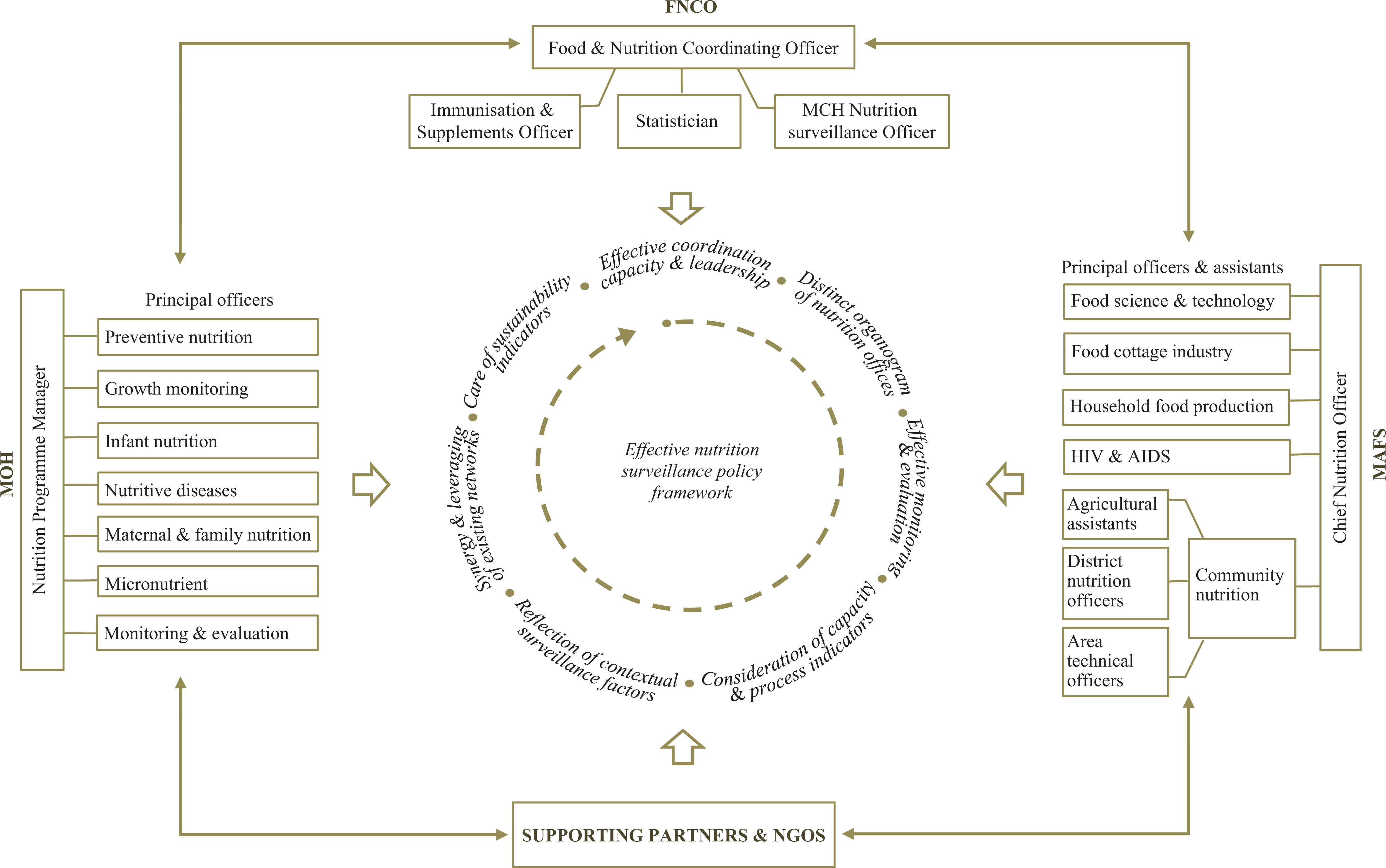
A framework of imperatives for an effective nutrition surveillance system for maternal and child health in Lesotho. FNCO, Food & Nutrition Coordinating Office; MoH, Ministry of Health; MAFS, Ministry of Agriculture and Food Security; NGO, Nongovernmental organisations; MCH, Maternal and child health.
Discussion
Nutrition Indicator Trends
The import of this study is that the NSS data in Lesotho are inconsistently compiled across most districts in Lesotho and that the NSS data are inconsistent with LDHS data. Clearly, the data inconsistency is a cause of concern for the nutrition policy in Lesotho given that the LDHS and NSS data are supposed to complement each other in diagnosing anomalies in the nutrition programs. The NSS which apparently stalled in 2015 certainly needs to be scaled up across all districts.
While the general improvement in the trend for LBW and underweight is commendable, districts in the Mountain Range such as Mokhotlong and Thaba-Tseka need more resources for nutrition programs while the NSS has to reach out to Mafeteng District for data on LBW and to all the districts in Lesotho for stunting, wasting, exclusive breastfeeding, maternal anemia, and child overweight.
Data gaps on stunting, wasting, and maternal anemia in the NSS indicate the need to improve the national strategy for monitoring of child growth in the communities. For example, new strategies are needed for collecting data items such as height and weight for calculation of stunting and wasting indices, respectively, while data for hemoglobin and iron indices also need to be tracked for calculating maternal anemia. It is also possible for the Government of Lesotho to increase targeted funding to ensure that data for exclusive breastfeeding and overweight that are routinely recorded by rural health centers and clinics are included in the NSS.
The high levels of stunting recorded in 2007 across all the districts in the NSS and the LDHS data for 2004, 2009, and 2014 indicate deeper challenges with malnutrition in Lesotho. This calls for a review of the National Nutrition Policy and the Nutrition Strategy 2014-2019. 32 More government support for nutrition intervention programs supported by WFP in collaboration with UNICEF, WHO, and World Vision is also needed. Importantly, more resources are needed to cover districts with more data gaps in the NSS. Critically, the LDHS data suggest that Lesotho is unlikely to meet global nutrition targets for stunting, maternal anemia, child overweight, and LBW. Apparently, the 2015 report on Lesotho’s progress on the Sustainable Development Goals (SDGs) also warns that Lesotho may fail to achieve SDG target on Zero Hunger. 15
The apparent decline in vitamin A supplementation coverage between 2007 and 2015 may be due to poor government funding for this program. Therefore, there is need for the Government of Lesotho to increase funding for promotion of exclusive breastfeeding, particularly in Maseru District which had the lowest proportion according to the data available for this indicator in 2007. Possibly, the low levels of exclusive breastfeeding in Maseru District could be due to a higher proportion of working mothers in this district compared to the predominantly rural ones, meaning there is a need to look at possible interventions to improve the situation such as increasing the duration of maternity leave.
The inconsistency in data trends between NSS and LDHS data particularly for LBW and the lack of comparable data between the NSS and LDHS child overweight and maternal anemia data is a cause of concern, with the LBW data inconsistency between NSS and LDHS likely to be a result of divergent sampling techniques between the NSS and LDHS.
Despite the lack of complementary data in the NSS for trend analysis, LDHS data suggest that stunting, child overweight, maternal anemia, and LBW remain of critical concern to MCH in Lesotho. Apparently, the 2015 Global Nutrition Report 24 notes that although stunting and wasting are showing slow and uneven declines, maternal anemia is one of the indicators not improving in most regions of the world.
Corrective measures for maternal anemia include intensifying government and donor supported food fortification programs such as fortification of staple maize flour with an iron fortificant easily bioavailable (sodium iron-EDTA) and folic acid, coupled with heightened surveillance for the iron fortificant using, for example, the iron spot-test, 33 while ensuring that an elaborate monitoring and evaluation framework for the fortification program is timeously designed and suits the local context. 32 However, for better outcomes, fortification of maize flour needs to be combined with the already existing iron and folate supplementation program for pregnant women in Lesotho. Of note, Mugomeri et al 34 observe that iron and folate supplementation during pregnancy has limited effectiveness in settings such as Lesotho due to late attendance of antenatal care sessions by pregnant women and the effects of HIV infection which is highly prevalent in this setting.
As for stunting, child overweight and LBW, Lesotho needs to avail more resources for expedited implementation of National Nutrition Policy and the Nutrition Strategy 2014-2019, 32 paying attention to strategies for improving its disproportionate HANC index 24 and promoting breastfeeding practices.
Structure, Functionality, and Constraints to the National Surveillance System
The weak coordination capacity of the FNCO due to gaps in the surveillance policy framework is the most significant gap in the surveillance system which needs to be prioritized. Strengthening of the FNCO is therefore necessary, with additional staff endowed with leadership competencies 35 to coordinate the entre surveillance system. With this challenge addressed, the next big hurdle is to address the problem of poor organogram of nutrition offices at MoH to effectively supervise the collection of surveillance data across the country. In addition, the need to collect capacity and process indicators such as food consumption patterns and nutrition intake cannot be overemphasized. Of note, the World Health Assembly reiterates the need for collection of these data, noting that a few countries in sub Saharan countries have data on the diets of infant and young children, such as minimum dietary diversity. 24 In addition, MoH and MAFS need to consider using cost-efficient data gathering methods such as decentralized electronic HMIS to reduce costs. 7,36
Cooperation Between Line Ministries and Supporting Partners
Poor cooperation between the responsible line ministries and support partners due to poor information sharing is a major challenge affecting the NSS. One solution is to formalize cooperation partnerships in the surveillance policy framework. Government of Lesotho 37 acknowledges that the NSS is affected by a number of challenges, with the most notable lying in intractable gaps in information systems, legal and policy framework, financing, as well as nutrition monitoring and evaluations. Constraints peculiar to Lesotho’s NSS such as culture, attitudes, and behavior toward nutrition also need to be addressed. Of note, the WHO 7 study of NSSs in Africa, had only 1 out of 11 countries that conducted context analysis on nutrition surveillance, implying that context analysis is an important research gap in the African setting.
Imperatives for an Effective NSS in Lesotho
The most critical imperative is to strengthen the office of the FNCO as the overarching coordinator of whole NSS. With this in place, the FNCO should be able to take care of other imperatives under its purview, such as overseeing the installation of distinct organograms of nutrition offices at MoH and MAFS, as well as strengthening of monitoring and evaluation capacity for nutrition programs. The Government of Lesotho should also leverage on existing networks to improve the NSS. Encouraging formal cooperation partnerships and other mechanisms of engagement is therefore needed. 24
The NSS needs to have an action plan for improving the collection of supporting data for the NSS such as capacity, process, and sustainability indicators. 2,10,11 Furthermore, critical analysis of contextual factors in the NSS is required to motivate for extra resources where necessary. 10
This study has notable limitations. Limited sampling of the NSS data set due to missing data is one major limitation. Also, the purposive sample of KIs excluded NSS users and data collectors at district level, making it difficult to clarify local constraints to the NSS at district level and to explain reasons for missing data, as well as potential actions to improve MCH in Lesotho.
Conclusion
While Lesotho has made commendable progress on guidelines and policies on nutrition surveillance in effort to address MCH, inconsistent collection of NSS data and challenges with sampling of nationally representative data in the country’s LDHS indicate an urgent need to revamp the NSS to address the problem of stunting, wasting, maternal anemia, and child overweight in Lesotho. Increased government funding is needed to capacitate the FNCO. Suggested imperatives presented in this study may contribute to a strategy for improving the NSS and ultimately MCH in Lesotho.
Footnotes
Author’s Note
Eltony Mugomeri is now affiliated with Department of Health Sciences, Africa University, Mutare, Zimbabwe.
Acknowledgments
The author is grateful to the data collectors and all the individuals who assisted in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.