
Abstract
Background:
A mandatory universal salt iodization (USI) has been implemented in Sarawak, Malaysia since 2008.
Objectives:
The aim of this study is to assess the current iodine status among school-aged children (SAC) and pregnant women (PW) after 10 years of USI implementation in Sarawak.
Methods:
This cross-sectional survey among school-aged children and pregnant women was conducted between July and October 2018 in Sarawak. The multistage proportionate to population size sampling technique was used to select 30 schools and 30 maternal and child health care clinics. A total of 1200 children aged 8 to 10 years and 750 first-trimester pregnant women were randomly selected to participate in the study. Iodine excretion level in urine was determined according to the World Health Organization classification.
Results:
A total of 988 children and 677 PW participated in the study with a response rate of 82.3% and 90.2%, respectively. The overall median urinary iodine concentration (UIC) level among the children was 126.0 μg/L (interquartile range [IQR], 71.0-200.9 μg/L) and classified as adequate iodine status. The median UIC among PW was 123.9 μg/L (IQR, 56.5-192.1μg/L) indicating inadequate iodine status.
Conclusion:
The present findings indicate that despite adequate iodine status in children, the majority of PW still showed inadequate iodine status. Thus, comprehensive monitoring of the iodine deficiency disorder problem among PW is warranted.
Introduction
Iodine is an integral part of the thyroid hormone, and a low level of iodine in human will reduce the production of thyroid hormones (thyroxine and 3,5,3′-triiodothyronine). 1 This deficiency may lead to a broad spectrum of adverse health effects collectively termed iodine deficiency disorders (IDD). 2 A severe iodine deficiency (ID) is associated with severe retardation of growth and maturation in almost all organ systems in early fetal life throughout to adulthood. It is noted that the school-aged children (SAC) and pregnant women (PW) are 2 of the vulnerable groups for IDD. The spectrum of IDD in fetus is associated with ID in mother during pregnancy which may cause abortions, stillbirths, congenital abnormalities, increased perinatal, and infant mortality. In neonates, the continuing of ID may result in the formation of goiter and hypothyroidism, while IDD in children may impair mental function and retard physical development. 3
Sarawak, the largest state in Malaysia, it has long been well known that endemic IDD is common over wide areas of the state. During the 1970s, most of the interior and coastal regions of the state had been endemic for IDD. A goiter prevalence of 40% to over 90% in respondents older than 15 years, and occasionally congenital iodine deficiency syndrome had been observed in some villages. 4 -6 Hence, in 1982, the Sarawak government enacted legislation designating 16 districts and 3 subdistricts in interior Sarawak as “Goiter Endemic Areas” (GEA), where only iodized salt can be sold. However, the lack of enforcement of the legislation and difficulty to access the GEA have resulted in IDD continuing to be a major public health problem in these areas. 7 Recognizing the partial iodization of salt in Sarawak may not be enough to bring about the elimination of IDD in Sarawak. The Sarawak State Health Department in 1995 implemented iodization of water supply in villages and schools in most of the interior Sarawak to ensure a continuous supply of small doses of iodine to this population. 8 In 2008, a national IDD study was conducted in Malaysia including Sarawak, and the result revealed the median urinary iodine concentration (UIC) of primary schoolchildren aged 8 to 10 years in Sarawak was at a borderline adequate level of 101.9 µg/L, but the median UIC of school-aged children in rural areas was only at 96.6 µg/L (inadequate). 9 Hence, a decision was made by the Malaysian government to introduce a mandatory universal salt iodization (USI) in Sarawak in July 2008, which requires all salt sold for human consumption in the state to contain not less than 20 mg of iodine/kg and not more than 40 mg/kg. 10
In 2011, after 3 years of USI, a state IDD study was conducted by the Sarawak State Health Department among school children aged 8 to 10 years. The results of the study reported a goiter prevalence of 0.3%, and the median UIC level was 154.2 µg/L indicating an adequate iodine status. 11 In PW, a study conducted in 2015 in all 11 divisions in Sarawak among first-trimester PW revealed the median UIC was 105.6 µg/L, indicating iodine deficiency. 12
The results of both studies were in agreement with several studies conducted among SAC and PW in many countries, which had also found that the adequate iodine status in SAC may not reflect adequate iodine status in PW although USI has been implemented. 13 -15 Thus, in this study, we conducted a study among the SAC and PW simultaneously with the aim to determine the current status of IDD in both groups after 10 years of USI implementation in Sarawak.
Methods
This cross-sectional IDD study was conducted from July to October 2018 among SAC aged 8 to 10 years and first-trimester PW in Sarawak. A multistage proportionate to population size sampling technique was used to randomly select 30 schools and 30 government maternal and child health care clinics (MCHCs) in Sarawak. The schools and government MCHCs were selected because of easy recruitment and were representative of different socioeconomic classes, since in Sarawak, almost all children of this age-group attended school. 9 The majority (> 80%) of PW received their antenatal care at the government health facility. 16 In each school, 40 SAC were randomly selected by systematic sampling and if the selected school had < 40 children aged 8 to10 years, all of them will be included in the study. The total sample size for SAC in this study was 1200. 1 In terms of PW, the sample size of the study was calculated based on anticipated prevalence of 65.0%, 95% confidential interval (CI), relative precision of 5%, design effect of 2, and nonresponse rate of 5%. The calculation of sample size for PW was based on the following formula: 17
Based on the formula, the sample size given was 350. Since design effect was 2, the sample size required was 700 (350 × 2) to cater for nonresponse rate of 5% (35). The final total sample size was 735 (rounded up to 750). The World Health Organization (WHO) Expanded Program on Immunization (EPI) studies approach was used to randomly select the first respondent, and then, subsequent respondents were chosen until the required number of pregnant women was met. 18 In addition, the sample size of both SAC and PW exceeds the WHO-recommended sample size of 300 for reliable assessment of iodine status of the population. 19
All required data were obtained through interviews on sociodemographic and analysis of urine from the study respondents. Spot urine samples were collected using urine containers with screw cap from all the respondents by trained medical laboratory assistants. The samples were stored in a cool, dry place before being sent to the regional IDD Laboratory in Kota Kinabalu, Sabah, Malaysia. The samples were frozen at −18 °C until analysis using in-house modified microplate method based on the Sandel-Kolthoff reaction method to detect urinary iodine excretion levels. 20 Based on median UIC in school-aged children, iodine status is classified using the following cutoff points: median UIC < 100 µg/L (iodine deficiency) [50-99 µg/L (mild deficiency); 20-49 µg/L (moderate deficiency); < 20 µg/L (severe deficiency)]; 100 to 199 µg/L (adequate); 200 to 299 µg/L (higher than adequate); and > 300 µg/L (excessive). In addition, no more than 20% of urinary iodine samples in SAC should be below 50 µg/L. 1 However, for the current analysis, the median UIC in SAC in the range of 100 to 199 µg/L and 200 to 299 µg/L will be presented as a single category (100-299 µg/L, adequate iodine status). 21 Based on median UIC in PW, the median UIC levels of < 150 µg/L were considered inadequate; 150 to 249 µg/L, 250 to 499 µg/L, and ≥ 500 μg/L were considered to have adequate, more than adequate, and excessive iodine status, respectively. 1
Ethical approval was provided by the Medical Research and Ethic Committee, Ministry of Health Malaysia (NMRR-17-2931-39285 and NMRR-17-2932-39316). In SAC, parent’s written informed consent forms were given to the school teachers for them to help distribute to the parents a week prior to the study. On the day of the study, children’s consent was distributed to the respondents before the study was conducted. In PW, they are provided with information sheets and written informed consent forms before participating in the study. All individual information was kept confidential, and a specific identification code was given to each respondent to make sure the study was anonymous.
SPSS software version 21 for windows (SPSS Inc) was used for data analysis. Normality assumptions were assessed using the Kolmogorov-Smirnov test, and homogeneity of variances was tested using Levene’s test. Continuous variables were expressed as means (± standard deviations) or medians (interquartile range). Categorical data were described as frequency and percentages.
Results
A total of 988 SAC from 30 randomly selected primary schools in all 12 divisions in Sarawak responded to the study, with a response rate of 82.3%. Of these, 495 (50.1%) were males and 493 were (49.9%) females. The mean age, weight, and height of the children were 9.1 years, 30.7 kg, and 129.3 cm, respectively. The majority of them were Iban (28.0%), followed by Malays (26.8%) and Chinese (16.7%). In terms of PW respondents, 677 women from the first trimester of pregnancy from 30 randomly selected government maternal and child health care clinics (MCHC) agreed to take part in the study (response rate, 90.2%). Their mean age, weight, and height were 27.6 years, 60.7 kg, and 153.9 cm, respectively. The majority of them were Malays (35.2%), followed by Iban (29.5%) and Chinese (13.0%). With regard to the pregnant women gravidas, the majority of them were from gravida 2 (30.7%) followed by gravida 1 (29.5%) (Table 1).
Sociodemographic Characteristics of School-Aged Children and Pregnant Women in Sarawak.
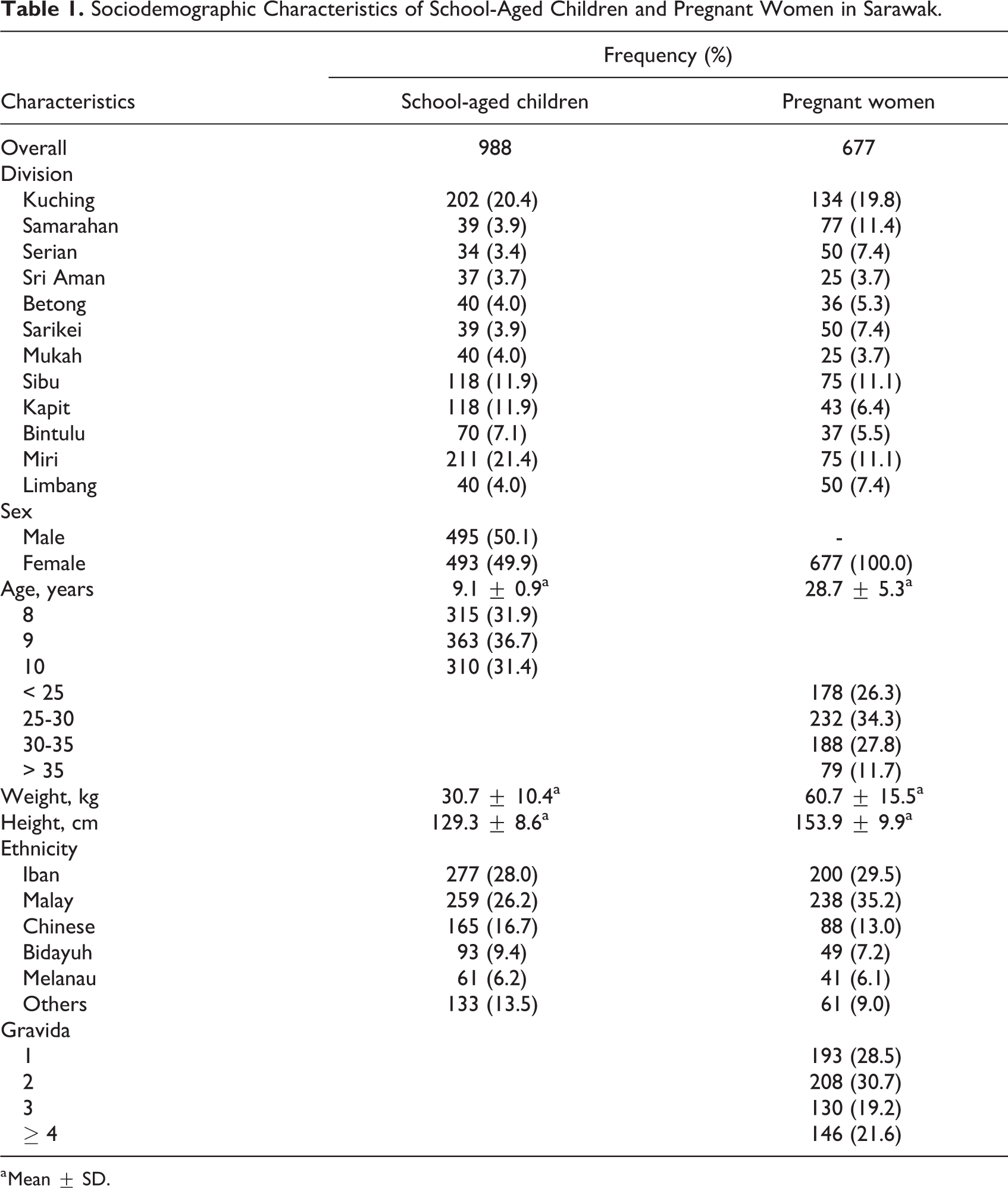
a Mean ± SD.
The median UIC value among the SAC was 126.0 µg/L (interquartile range [IQR], 71.0-200.9), which was within the recommended WHO/UNICEF/ICCIDD reference range of 100 to 199 µg/L. The distribution of UIC among SAC showed more than half (n = 531) of the SAC having adequate iodine status. However, approximately 22% of the SAC are categorized as having a mild iodine deficiency (UIC, 50-99 µg/L), about 14% having a moderate iodine deficiency (UIC, 20-49 µg/L), and only a fraction of SAC (3.3%) having severe iodine deficiency (UIC, < 20 µg/L). In terms of UIC among PW, the median UIC value was 123.9 µg/L (IQR, 56.5-192.1), which was lower than the WHO/UNICEF/ICCIDD-recommended reference range of 150 to 249 µg/L. The distribution of UIC among PW showed 61.5% (n = 397) of them having inadequate iodine status compared to only 26.2% (n = 169) having adequate iodine status and about 12% having more than adequate iodine status (UIC, 250-499 µg/L; Table 2).
Urinary Iodine Classification in School-Aged Children and Pregnant Women in Sarawak.
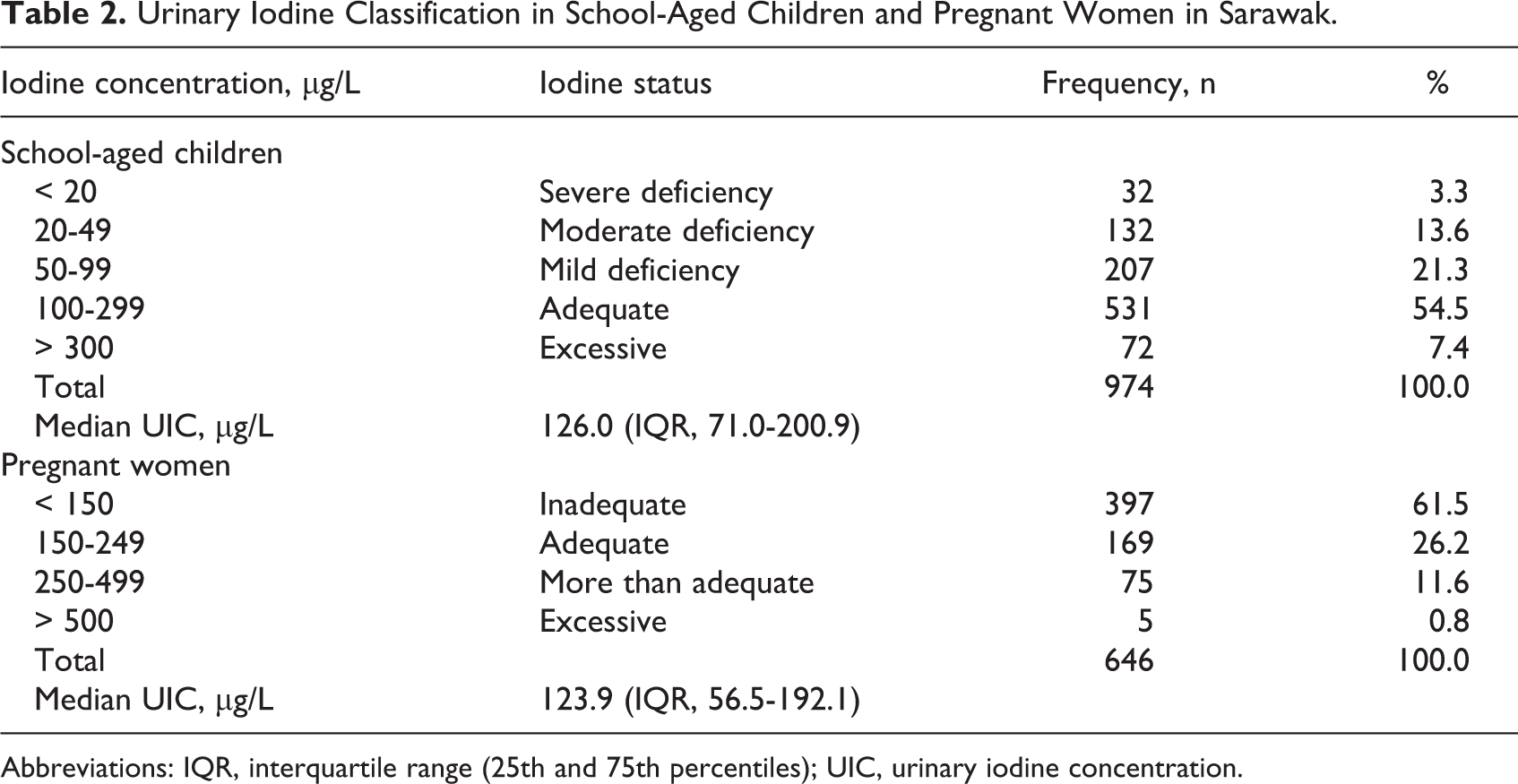
Abbreviations: IQR, interquartile range (25th and 75th percentiles); UIC, urinary iodine concentration.
Discussion
Worldwide, the iodine status of SAC is recognized as a proxy of the iodine status of the population. 1 They were selected because of easy recruitment and were representative of different socioeconomic classes in Sarawak. In addition, the school enrollments in Sarawak are high. 9 Daily UIC of SAC closely reflects iodine status and has been used as an indicator of iodine nutrition in many large-scale nutrition studies. 2 Furthermore, the determination of urinary iodine is the best method to determine the iodine status of the population and is a useful indicator for monitoring the effectiveness of the intervention programs. 1 In this study, the overall median UIC among the SAC was 126.0 µg/L, and the distribution of the UIC shows that only 16.9% of them have UIC < 50 µg/L. Based on these 2 criteria for assessing the severity of IDD in the population, 1 the state of Sarawak would be classified as area of iodine adequacy.
The most possible factor for optimal median UIC observed in SAC is the successful implementation of mandatory USI in the state since 2008, and it is believed that currently iodized salt is easily available in Sarawak. 9 The other possible factor is the level of socioeconomic development that has taken place particularly during the last 20 years. The infrastructure development, in particular the building of roads into the interior, has given rise to new townships and new businesses that have made outside food including seafood more widely available to communities living in once remote and inaccessible areas. 22 The IDD status among the SAC in this study was found similar to the previous Sarawak statewide IDD study conducted after a 3-year implementation of USI, which showed that the overall median UIC level was 154.2 µg/L. 11 The current median UIC in this study also resembled another statewide IDD study done in neighboring state of Sabah, Malaysia, which has introduced mandatory USI since 2000. It is reported that the introduction of mandatory USI is able to increase the UIC among its population, the median UIC had risen significantly from 187.8 µg/L in 2010 to 227.8 µg/L in 2011, and increased further to 232.1 µg/L in 2012. 9 The use of iodized salt was considered as the effective choice for IDD eradication program and in agreement with many studies conducted among the communities living in ID areas. 23 -25 Perlas et al 23 reported that after mandatory USI was introduced in 1995, the median UIC status among Filipino SAC has increased from mildly deficient (median UIC, 71 µg/L) in 1998 to 168 µg/L in 2013. Chao et al 24 in their study revealed that iodine nutrition in SAC in China was increased to optimal level (198 µg/L) after 10 years of implementation of USI program. Alsanosy et al 25 showed that the IDD control program using USI in Saudi Arabia in 1997 managed to improve the iodine nutrition from 180 µg/L in 1997 to 517 µg/L in 2010.
During pregnancy, iodine requirements increase approximately 50% due to a variety of physiological changes in response to thyroxine-binding globulin and stimulation of thyroid-stimulating hormone. 26 Pregnant women are normally sensitive to marginal iodine deficiency. Thus, they are a prime target group for IDD control. 1 In our study, the median UIC in PW was 123.9 µg/L, indicating that the iodine levels in PW are still below the recommended optimum level of 150 µg/L. In addition, the distribution of UIC revealed that about 60% of the PW UIC is still below 150 µg/L. 1 Based on the median UIC results, the status of IDD among the PW in this study was also essentially unchanged compared to the previous Sarawak state IDD study conducted among first-trimester PW in 2015. 12 There are several reasons for this inadequacy. First, the comparable median UIC observed among PW (123.9 µg/L) and the SAC (126.0 µg/L) revealed that they are most probably sharing a common household food basket. However, the information on food intakes by them was not collected, and if these intakes were measured, the results may be more informative. It is noted that the PW should consume substantially more iodine food compared to other household members in order to achieve the recommended median UIC of > 150 µg/L. Our findings are in agreement with several findings and demonstrated a similar relationship of eating from the same household food basket. 14,27 Second, another possible factor leading to low iodine in the urine among the PW could be due to less iodized salt being consumed by the PW as a result of increased awareness of health issues. It is noted that the study areas have a good coverage of government MCHC clinics. Thus, many PW managed to obtain medical advice from the clinics. 12
The limitations of this study were the in-house modified microplate method based on the Sandel-Kolthoff reaction method 19 has several disadvantages, such as requires dedicated laboratory space, glassware, and experienced technician to provide an accurate urinary iodine result. 28 Currently, the inductively coupled plasma mass spectrometry method is often used as the “gold standard,” and many countries have started to adopt this method due to its high degree of accuracy, versatility, little demand for technician time, and the capacity to analyze large numbers of samples. 28,29 If the urine samples in this study can be analyzed using both methods, the results may be more informative. Another limitation was that we did not include PW who underwent follow-up in private health care facilities, as this study only covered government health care facilities. The strength of our study was that the response rate in this study for both groups was very high (> 80%).
Conclusions
In conclusion, variations in iodine nutrition status among SAC and PW were observed in this study. The present findings indicate that the mandatory USI in Sarawak managed to improve the iodine status in SAC. However, the majority of PW still have inadequate iodine status.
Footnotes
Acknowledgments
We would like to thank the Director General of Health Malaysia for his permission to publish this article. We would also like to thank the Sarawak State Health Department, study participants, and data collectors for their dedicated cooperation. This research was funded by the Ministry of Health, Malaysia.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Ministry of Health, Malaysia.