
Abstract
Background:
Ethiopian government was implementing mandatory salt iodization program for the last decade to eliminate iodine deficiency disorders, but several recent studies reported mixed findings.
Objective:
This review aimed to assess the difference in implementation of iodized salt program 10 years before and after mandatory salt iodization being implemented in Ethiopia since 2011.
Methods:
In Ethiopia, legislation that enforces salt producers to iodize all salts used for human consumption started in February 2011. All studies about iodine deficiency and iodized salt conducted in Ethiopia in the last 2 decades were searched. Searches were performed in PubMed database. Google Scholar, Iodine Global Network, and Ethiopian Public Health Institute websites were also searched.
Results:
A total of 235 titles and abstracts were identified. After scanning the abstracts and full papers, 43 articles were remained for final data synthesis. In this review, all studies conducted before 2011 reported a urinary iodine concentration (UIC) value of < 100 μg/L and 66.7% of them reported a goiter prevalence of > 30%. On the other hand, among studies conducted after 2011, 88.9% reported UIC value < 100 μg/L and 73.7% reported goiter prevalence of > 30%. Household availability of adequately iodized salt increased from nearly 20% in pre 2011 to more than 50% in post 2011 period.
Conclusion:
Despite the efforts made by the Ethiopian government on mandatory salt iodization for the last decade, iodine deficiency is sustained in the country. Moreover, the goal of universal salt iodization program is offtrack and needs urgent revision.
Registration:
Registered on PROSPERO register with reg. no CRD42021251124.
Introduction
Despite global improvement in iodine nutrition status, achieving sustainable elimination of its deficiency remained a great challenge in many African countries including Ethiopia. 1 Beside poor consumption of iodized salt, knowledge gap, misperceptions, and improper practices of iodized salt were major problems in Ethiopia, as indicated by previous studies. 2 -4
Young children and pregnant women are the most vulnerable groups of iodine deficiency (ID). 5 Iodine deficiency has serious effect in these groups leading to easily preventable cognitive impairment. 6 Despite its ill-effect, iodine deficiency disorders (IDD) are among the easiest and cheapest of all disorders to prevent. The addition of a small, constant amount of iodine to the salt that people consume every day is all that is needed. 7
After recognizing the consequences of ID and the availability of prevention method, most countries of the world accepted universal salt iodization (USI) as a safe, cost-effective, and sustainable strategy to ensure sufficient intake of iodine and to achieve the virtual elimination of IDD. 8 Ethiopia was one of these countries in Africa to accept the USI goal of achieving more than 90% utilization of iodized salt by households.
As far back as 1988, Ethiopia was achieved almost 80% iodized salt coverage, 9 when most iodized salt came from Eritrea (Red sea). The 1998 to 2000 war between Ethiopia and Eritrean interrupted Ethiopia’s iodized salt supply and the country started importing salt from other countries, such as Djibouti and India, much of which was not iodized. As a result, there was a rapid deterioration in the iodine status of population and the percentage of households consuming adequately iodized salt reduced to below 10%. 9 This was supported by 2 national surveys conducted in 2005 10 and 2011. 11 According to the report of these surveys, only 4.2% and 15.4% of the Ethiopian population use iodized salt respectively. Another national survey conducted in 2016 tested the presence of potassium iodate in household salt using rapid test kit and reported 89.2% coverage of iodized salt. However, in the same survey, a subsample of salt was measured for its iodine content using titration method. According to the finding, only 26% of households get adequate iodized salt for better nutrition. 12
Currently, Ethiopia is producing its own iodized salt using KIO3 compound in Afar and Somali regions of the country. In addition, in February 2011, the Council of Ministers passed mandatory legislation requiring salt producers to iodize their salt for human consumption and in 2012; the government of Ethiopia began to enforce the new rules. 9,13 However, whether the program is going on as intended or not is in question, because several recently conducted national and subnational studies reported a mixed finding. Most of the studies reported presence of severe ID and low availability of adequately iodized salt in Ethiopia. 2 -4,14 -16 On the contrary, some recently conducted national and subnational studies revealed that the country is iodine sufficient and the national household iodized salt coverage reached 89.2%. 12,17
The Research Question
The major research question that initiated this systematic review was the following: “How mandatory salt iodization program implemented for the last 10 years (2011-2020) differ from the previous voluntary implementation period (2001-2010) in reducing IDD and achieving USI goal in Ethiopia?”
To answer the above question, this review assessed the current iodine nutrition status indicator (median urinary iodine concentration [mUIC]), long-term ID impact indicator (goiter prevalence), and iodine content of salt at household level. The indicators were assessed in all papers published in the last 2 decades (2001-2020) in Ethiopia and compared for the differences.
According to World Health Organization (WHO), mUIC is the main indicator used to assess iodine status of a population. 18 Goiter prevalence may be useful in assessing thyroid function and long-term iodine nutrition status. However, a combination of mUIC, goiter prevalence, and availability of adequately iodized salt at household level can be used to assess the impact of salt iodization on the reduction of IDD and sustainability of ID prevention and control programmes. 7,18
Based on the above research question, this review assessed the difference in implementation of previous voluntary and current mandatory salt iodization programs and compared its impact in prevention and control of IDD and utilization of iodized salt.
Methods
Search Strategies
This review was conducted from May 1 to June 30, 2021. During this period, all studies about ID and iodized salt conducted in last 2 decades (2001-2020) in Ethiopia were searched. The period of the study searched was limited to 20 years because mandatory legislation that enforces salt producers to iodize all salts used for human consumption was passed by Ethiopian government in 2011 (10 years back) and it is fair to compare this period with the similar previous nonmandatory salt iodization period (10 years before 2011).
The search terms included were keywords describing the following concepts: “Iodine” and “Ethiopia”; iodized salt and “Ethiopia”; “Universal Salt Iodization” and “Ethiopia”; “Availability of iodized salt at household” and “Ethiopia”; “Iodine deficiency” and “Ethiopia”; “Causes of iodine deficiency” and “Ethiopia”; “Iodine deficiency disorders (IDD)” and “Ethiopia”; “Effects of iodine deficiency” and ‘Ethiopia”; “IDD indicators” and “Ethiopia”; Urinary iodine concentration” and “Ethiopia”; “Urinary iodine excretion” and “Ethiopia”; “Thyroid gland enlargement” and “Ethiopia”; “Goiter” and “Ethiopia”; “knowledge of iodine deficiency” and “Ethiopia”; “knowledge of iodized salt” and “Ethiopia”.
Using the above terms, searches were performed in PubMed database for relevant articles published in English language. Google Scholar and Iodine Global Network (IGN) websites were also searched and Ethiopian Public Health Institute was contacted for possible grey literatures (workshops, reports, newsletters, and conference proceedings).
Eligibility Criteria
Inclusion criteria
An attempt was made to include all study designs in this review, as such inclusive approach allows for examination of the totality of empirical evidence and may provide invaluable insights regarding the agreement or disagreement of the results from different study designs. Therefore, studies that fulfilled the following criteria were included: All studies about iodine nutrition status and iodized salt in the last 20 years (2001-2020) Only studies conducted in Ethiopia (primary, review, or grey literature) Studies that reported any of the following outcomes: goiter prevalence, median UIC, and household salt iodine content.
Exclusion criteria
Studies with the following characteristics were excluded: Published after February 2011, but the data collected before 2011 Studies conducted in individuals with thyroid disorders Studies published/written in languages other than English.
Study Selection
Two reviewers independently assessed the title, abstract, and keywords of references for potential relevance. The full manuscript was retrieved when the prespecified inclusion criteria were met or when there was uncertainty to reject the study. An adapted reporting item for systematic reviews (PRISMA) flowchart was used to depict the selection of studies for inclusion and the grey literatures were included based on relevance (Figure 1).
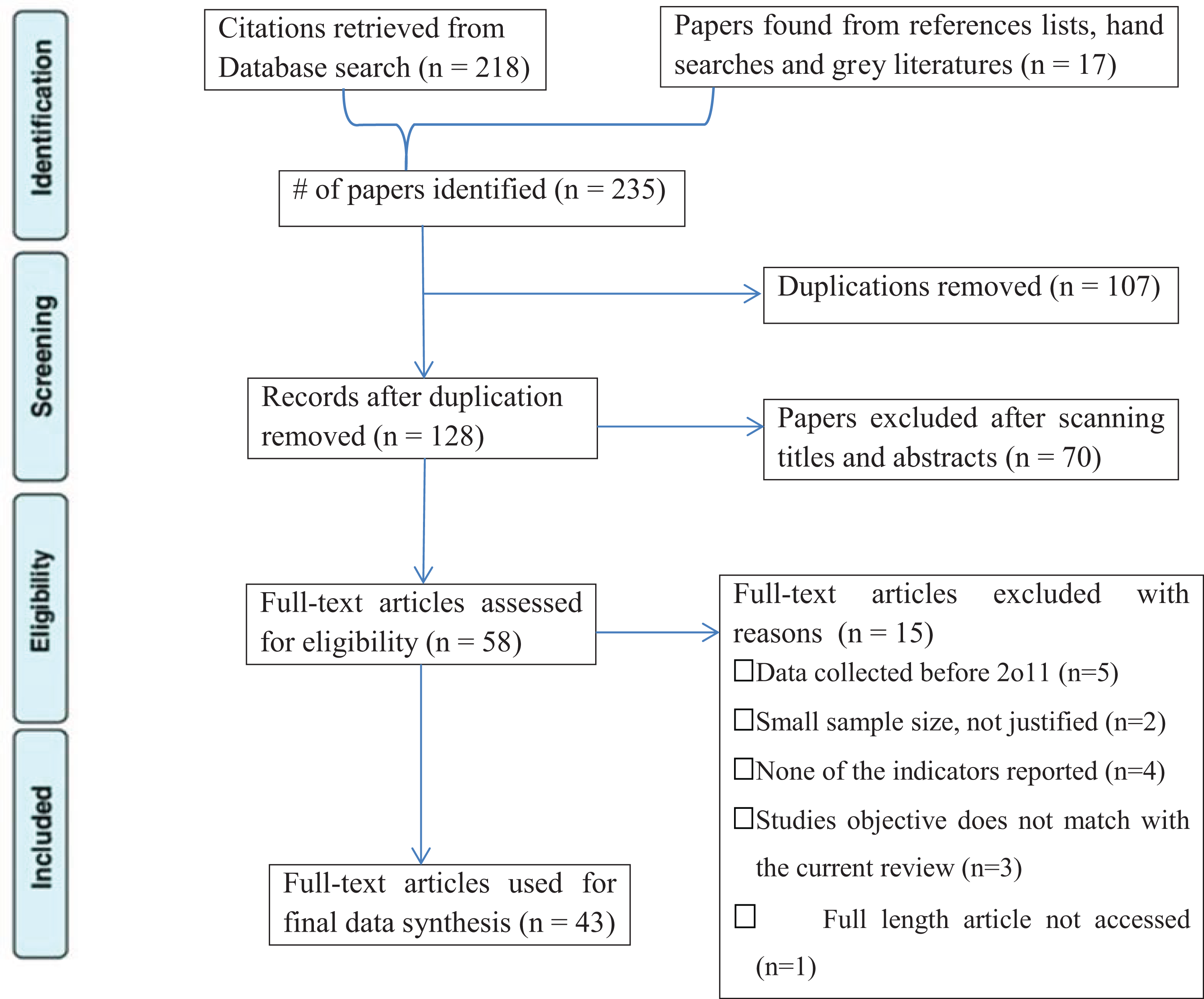
PRISMA Flow Diagram.
Data Extraction
Data extraction parameters were ID indicators or markers (mUIC, goiter prevalence, and household salt iodine content). Data were extracted and tabulated independently by the 2 reviewers. All of the retrieved publications were checked for agreement between the reviewers. When there was discordance between the 2 reviewers against the set criteria, a third reviewer (senior professor in nutrition) was invited to review the discordant results and his report was taken as a final resolution for the disagreement.
Outcome Measurement
There were 3 main outcomes in this review. Median UIC at population level, adequately iodized salt at household level, and goiter prevalence at population level that indicates long-term impact of iodine insufficiency. In addition to these main indicators, other programmatic indicators assessed by the primary authors were also considered. Such programmatic indicators include government concerns (political will), availability and access of laboratories to measure UIC and salt iodine content, presence of active educational and social mobilization programs on the importance of iodine, and the use of iodized salt and presence of robust monitoring systems.
Quality Assessment of the Included Studies
All papers selected for inclusions in the review were subjected to a rigorous appraisal by 2 independent reviewers using the Joanna Briggs Institute quality appraisal tool adapted for studies reporting prevalence data. 19 Then the 2 reviewers work was cross-referenced and any disagreements were discussed with a third independent reviewer for final resolution.
Items used to appraise the included studies were (1) inclusion criteria, (2) study subject and setting, (3) valid and reliable exposure measurement, (4) use of objective and standard criteria, (5) confounder factors identification, (6) strategies for confounder identification, (7) valid and reliable outcome measurement, and (8) use of appropriate statistical analysis.
Studies were considered low quality and excluded from the review whenever the cumulative fitted result is below 50% in the quality assessment checklist criteria. 19 Accordingly, no study was excluded in our review Table 1.
Critical Appraisal Result of the Included Studies, 2021.
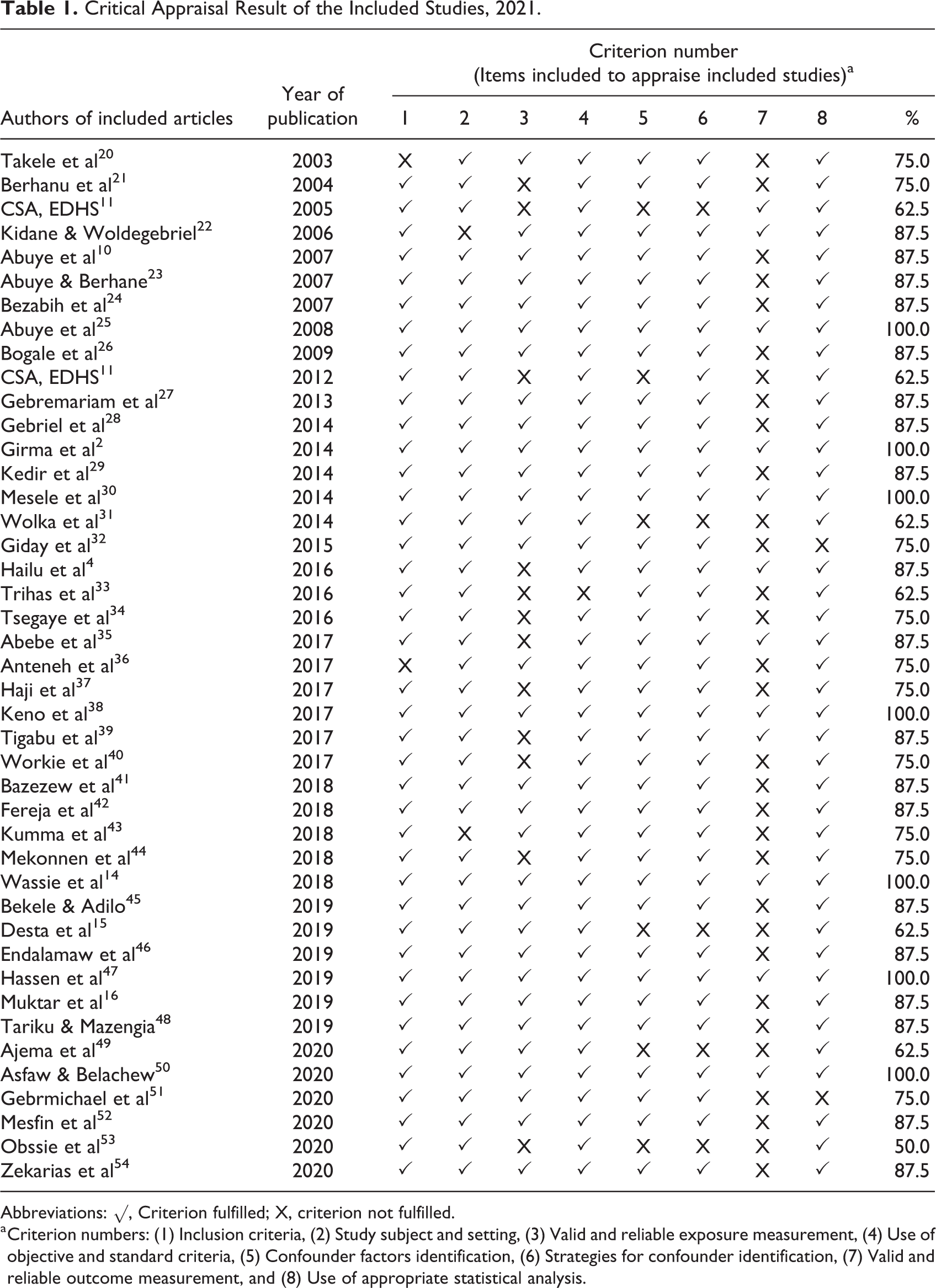
Abbreviations: √, Criterion fulfilled; X, criterion not fulfilled.
a Criterion numbers: (1) Inclusion criteria, (2) Study subject and setting, (3) Valid and reliable exposure measurement, (4) Use of objective and standard criteria, (5) Confounder factors identification, (6) Strategies for confounder identification, (7) Valid and reliable outcome measurement, and (8) Use of appropriate statistical analysis.
Data Synthesis
As there were no randomized controlled trial (RCT) or quasi-experimental design in included studies, a meta-analysis was not conducted. In addition, due to the heterogeneity relating to the goiter examination and grading, variation in participants and outcomes assessed, the main data analysis method used was a narrative approach. The synthesis aimed to describe the existing body of literature and identified strengths and gaps in the prevention of ID and utilization of iodized salt in last 2 decades in Ethiopia. The findings were summarized in a narrative interpretation focusing on years of publication, characteristics of study participants, outcome measures, the way outcome variables assessed/measured and the aims of the review.
Results and Discussion
Studies Characteristics
A total of 235 abstracts were identified in our search, of which 107 duplicates were excluded and the remaining articles were scanned for titles and abstracts. A total of 58 articles remained for full-text assessment. During full-text assessment, 15 articles which did not fulfill the set criteria were excluded with reasons and 43 full-text articles were used for final data synthesis. Almost all studies included for full-text assessment were cross-sectional design except one study which was systematic review.
No reports were found on RCTs or quasi-experimental studies concerning iodine nutrition and the consequences of its deficiency in Ethiopia. Because the numbers of research reports in the country were relatively small and of similar design, they were all included in the review. The extracted studies, outcome variables with their measurement, and major findings of published studies were summarized in Table 2.
Design, Outcome Variables With Their Measurement, and Major Findings of Published Studies on IDD and Iodized Salt in Ethiopia in Last 2 Decades (2001-2020).a
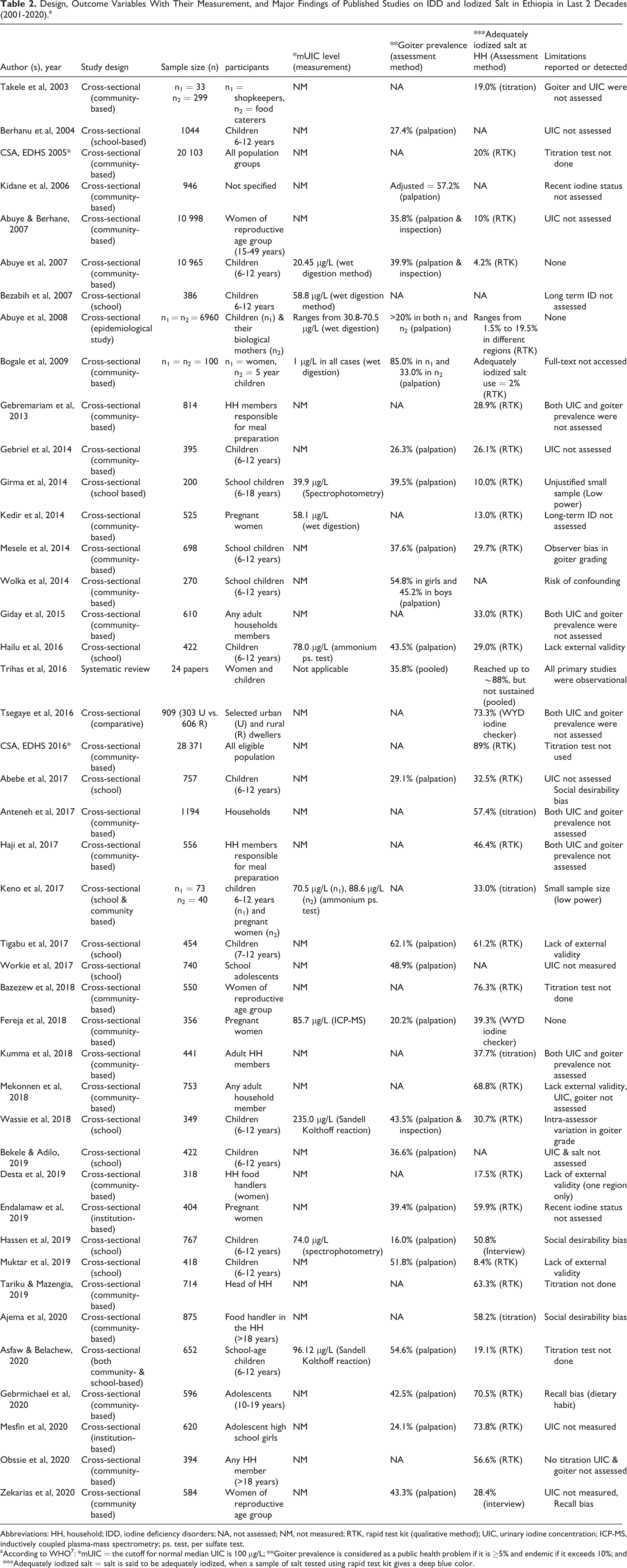
Abbreviations: HH, household; IDD, iodine deficiency disorders; NA, not assessed; NM, not measured; RTK, rapid test kit (qualitative method); UIC, urinary iodine concentration; ICP-MS, inductively coupled plasma-mass spectrometry; ps. test, per sulfate test.
a According to WHO 7 : *mUIC = the cutoff for normal median UIC is 100 μg/L; **Goiter prevalence is considered as a public health problem if it is ≥5% and endemic if it exceeds 10%; and ***Adequately iodized salt = salt is said to be adequately iodized, when a sample of salt tested using rapid test kit gives a deep blue color.
Prevalence of Iodine Deficiency Disorders in Ethiopia (2001-2020)
According to WHO/UNICEF/IGN, the mUIC taken from a representative sample is a good indicator of the current iodine status in the general population and any mUIC value < 100 μg/L is considered as an indicator of ID at population level. 18 Previously, the prevalence of goiter was considered as a public health problem if it is equal to or greater than 5% and endemic if it exceeds 10% 7 but currently, the prevalence of goiter is no more used as a sensitive indicator of ID. It may be used to assess a long-term impact of iodine insufficiency in a given population.
Median urinary iodine concentration
In this review, among the 9 studies conducted before 2011, 4 of them (44.4%) assessed mUIC and all of them reported a mUIC value of < 100 μg/L (100.0%). Among the 4 studies, 2 of them (50.0%) conducted in school children aged 6 to 12 years and the remaining 2 (50.0%) conducted in both the children and their biological mothers. Similarly, among 34 studies conducted after 2011, 9 of them (26.5%) assessed mUIC and 8 of the studies (88.9%) reported a mUIC value of < 100 μg/L. Six out of the 9 (66.7%) studies were conducted in school-age children and the remaining 3 (33.3%) were conducted in pregnant women. Due to such variation in participants and number of studies that assessed mUIC, it is hard to conclude that the observed difference is the mere result of mandatory program implementation. However, the mUIC at population level was < 100 μg/L in all primary studies included in this review. This fact indicates that, despite the efforts made by the Ethiopian government on mandatory salt iodization for the last decade, ID is sustained in the country.
Goiter prevalence
World Health Organization categorizes the prevalence of goiter as mild, moderate, and severe if its prevalence is 5% to 19.9%, 20% to 29.9%, and greater or equal to 30% respectively. Among the 9 studies conducted before 2011, 6 of them (66.7%) assessed goiter prevalence and 4 of them (66.7%) reported a goiter prevalence of more than 30% and the remaining 2 studies reported the prevalence of 20% and 27.4%. On the other hand, among 34 studies conducted after 2011, 19 (55.9%) of them assessed goiter prevalence and 14 (73.7%) of them reported a goiter prevalence of more than 30%. In the other 5, the prevalence ranged from 16% to 29.1%.
In this review, all studies reported more than 10% prevalence of goiter confirming that it is an endemic in the country. 7 However, we cannot determine iodine status of population using goiter prevalence, as changes in goiter prevalence lag behind changes in iodine status. Therefore, it is no more used as a sensitive indicator of iodine nutrition status and cannot be relied upon to accurately reflect current iodine intake. However, it can be used to assess program sustainability and progress when used in combination with mUIC levels in the population, availability of adequately iodized salt at the household level, and other programmatic indicators.
Iodine Content of Household Salt in the Last 2 Decades in Ethiopia
World Health Organization recommends a daily intake of 90 µg of iodine for preschool children (0-59 months); 120 µg for schoolchildren (6-12 years); 150 µg for adolescents (above 12 years) and adults; 250 µg for pregnant and lactating women. 4 To achieve these requirements, many countries of the world are implementing the goal of USI (more than 90% of households using iodized salt).
Ethiopia as a country accepted the strategy and passed a mandatory legislation requiring salt producers to iodize their salt for human consumption. In addition, following the border conflict between Ethiopia and Eritrea (1998-2000), the country began to explore indigenous salt production sources in different sites and started producing about 95% of the salt for its own use in the country. Despite these and other efforts made by the Ethiopian government, several recent researches had shown conflicting results about the Ethiopia’s progress toward achieving the goal of USI. 3,11,51,53
In a study conducted in eastern Ethiopia, the median UIC was 146 μg/L reflecting iodine sufficiency at population level, but 31% of the study participants had UIC < 100 μg/L (though an individual’s UIC value cannot be used to judge iodine status of any population) and utilization of inadequately iodized salt were high (90.0%). 3 Another study conducted in northeast Ethiopia had shown high prevalence of goiter (42.5%). 51 Similarly, the southeast Ethiopian study revealed only 56.6% of households were using adequately iodized salt 53 which is far below WHO recommendation (> 90%).
According to this review, in all studies conducted before 2011, the availability of adequately iodized salt at household level was found to be less than or equal to 20%. However, in studies conducted after 2011, only 14.3% reported less than 20% availability. Nearly half of the studies (46.4%) reported more than 50% possession of adequately iodized salt at household level. This finding indicates that the availability of adequately iodized salt at household level increased from nearly 20% to more than 50%. However, we cannot conclude that the iodized salt utilization is improved after 2011, because of methodological differences. For example, among all studies conducted before 2011, only one study used titration test to assess iodine content of salt at household level, whereas 7 studies used the same method in post 2011 studies. In addition, neither pre nor post 2011 studies had shown the achievement of USI goal of utilizing adequately iodized salt by more than 90% of the households.
Other Programmatic Indicators
In addition to the main iodine status indicators, it is important to assess other programmatic indicators which are regarded as evidence of sustainability. Among 43 primary studies included in this review, 4 of them (9.3%) reported less political commitment from government side, 5 (11.6%) complained poor access to UIC and salt testing laboratories, and 7 (16.3%) reported absence of effective monitoring system to assess the iodine status of population. Above all, majority of the studies, 28 (65.0%) raised the need for social mobilization and awareness creation programs on the importance of iodine and the use of iodized salt.
Limitations of the Review
Except one, all the primary studies included in this review used cross-sectional deign. Even though WHO recommends such design with a representative sample for population level iodine status studies, they often had methodological weakness.
For determination of iodine content of household salt sample, most primary studies used iodine rapid test kit which shows only the presence or absence of iodine in the salt.
Most of the primary studies included in this review were area specific and subnational which may not represent the national figure. However, we tried to include different studies from all regions in addition to the 5 national surveys conducted in the country.
Conclusion
This review used all relevant studies published in last 2 decades and provided them in a single document for policy makers to reach evidence-based decision-making. The review is the most recent compilation of studies regarding the difference in implementing voluntary and mandatory salt iodization programs. It compared the 2 period implementation statuses. The findings suggested that ID is sustained in the country, despite the efforts made by the Ethiopian government on mandatory salt iodization for the last decade. In addition, the USI program aimed to achieve the goal of utilizing adequately iodized salt by more than 90% of the households is offtrack and calls for a revision of its implementation strategies.
Recommendations
There is urgent need for revision of USI program strategies, action plans, and the legislation as it is offtrack.
National representative survey that encompasses all possible factors that affected the progress of iodized salt program such as loss of iodine at different supply chain management system, poor practice of iodized salt at population level, political will and support from government side, and the monitoring system should be conducted.
Footnotes
Authors’ Note
All methodologies and search strategies were indicated in the manuscript and if additional information is required, corresponding author is ready to share.
Acknowledgment
The authors would like to thank EPHI for the provision of valuable data.
Author Contributions
AA = Conceived and designed the study, performed the search, data extraction, data synthesis, interpretation, and drafted the manuscript. DT = Participated in the study design, search, and data synthesis, and manuscript revision. TB = Participated in the data synthesis, interpretation, and manuscript revision. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.