
Abstract
Background:
In 2005, more than 90% of Vietnamese households were using adequately iodized salt, and urinary iodine concentration among women of reproductive age was in the optimal range. However, household coverage declined thereafter to 45% in 2011, and urinary iodine concentration levels indicated inadequate iodine intake.
Objective:
To review the strengths and weaknesses of the Vietnamese universal salt iodization program from its inception to the current day and to discuss why achievements made by 2005 were not sustained.
Methods:
Qualitative review of program documents and semistructured interviews with national stakeholders.
Results:
National legislation for mandatory salt iodization was revoked in 2005, and the political importance of the program was downgraded with consequential effects on budget, staff, and authority.
Conclusions:
The Vietnamese salt iodization program, as it was initially designed and implemented, was unsustainable, as salt iodization was not practiced as an industry norm but as a government-funded activity. An effective and sustainable salt iodization program needs to be reestablished for the long-term elimination of iodine deficiency, building upon lessons learned from the past and programs in neighboring countries. The new program will need to include mandatory legislation, including salt for food processing; industry responsibility for the cost of fortificant; government commitment for enforcement through routine food control systems and monitoring of iodine status through existing health/nutrition assessments; and intersectoral collaboration and management of the program. Many of the lessons would apply equally to universal salt iodization programs in other countries and indeed to food fortification programs in general.
Keywords
Introduction
Iodine is an essential micronutrient required for normal thyroid function, growth, and development. 1 Iodine deficiency is the single most important preventable cause of brain damage and affects child’s learning capacity, women’s health, the quality of life in communities, and economic productivity. 2 However, it can be easily prevented through the addition of iodine to salt, and in 1993, the World Health Organization (WHO) and the United Nations Children’s Fund (UNICEF) recommended universal salt iodization (USI; note 1) as the main strategy to achieve elimination of iodine deficiency disorders (IDDs). 3 Today, 75% of households in the world are estimated to consume adequately iodized salt, 4 and an assessment of global data in 2012 concluded that the number of iodine-deficient countries has decreased from 54 to32 and the number of countries with adequate iodine intake increased from 67 to 105 between 2003 and 2011 as a result of salt iodization. 5
Vietnam was part of this global success story as it was one of the first countries in the world to achieve USI and the elimination of IDD. However, these achievements were not maintained. This article discusses how the salt iodization program in Vietnam was implemented and why achievements were not sustained in order to draw lessons learnt for Vietnam and other countries attempting to achieve sustained elimination of IDD through salt iodization.
Methods
A variety of published and unpublished documents related to the Vietnam salt iodization program were reviewed including progress reports, survey results, evaluations, program reviews, related legislation, and published articles on iodine deficiency and salt iodization in Vietnam. Key program stakeholders from the Ministry of Health (MoH), Hospital of Endocrinology (HoE), Vietnam Food Administration (VFA), Ministry of Agriculture and Rural Development (MARD), UNICEF, and WHO were interviewed in order to identify strengths and weaknesses of the program and to acquire qualitative data on the reasons for and motivations behind government policy and program decisions. These stakeholders also provided many of the materials reviewed. Data collected by the primary author from a previous program assessment (internal agency report; unpublished) 6 and field visits also contributed to the findings.
Findings
National IDD Control as a National Priority Program: 1994 to 2005
In the 1970s and 1980s, Vietnam implemented a salt iodization program in areas with high goiter rates for the control of IDD. 7 In 1994, following a national survey demonstrating high prevalence of goiter and low median urinary iodine concentration (MUIC) in school children, 8 the government extended the IDD control program to the whole country, with salt iodization as the primary strategy. In a separate development, iodized salt was included in a list of subsidized essential commodities for minority communities. In 1994, the National IDD Control (NIDDC) program was designated a national priority program, with special funds and oversight. 9 It was managed by a multisectoral Central IDD Committee, chaired by the Vice Minister of Health. Despite this, the NIDDC program was run very much as a health program, with limited collaboration with other ministries and no involvement of the salt industry.
Government legislation Decision No 481 10 issued in 1994 called upon the whole population to purchase and use iodized salt. It was replaced in 1999 by Decree 19 on the Production and Supply of Iodized Salt for Human Consumption. 11 The Decree aimed to eliminate IDD by regulating the production and supply of iodized salt for human consumption. It specified that all salt for human consumption, otherwise called “edible salt,” must be iodized. Salt for human consumption included “salt for direct human consumption and salt used in food.” It excluded however “common salt” which was defined as “noniodized salt including grain salt, refined salt, crushed salt, pit salt, and other types of salt produced from sea water or exploited from salt mines.” As the definition of common salt included refined salt, it could be interpreted to mean that any salt, processed and unprocessed, not marketed for human consumption did not need to be iodized. As a result of this exclusion, Decree 19 did not require the iodization of all salt for human consumption and did not enable a ban on noniodized salt. There was also ambiguity around the term “salt used in food” such that Decree 19 was not interpreted to require iodized salt to be used in commercially processed foods.
Decree 19 specified the roles and responsibilities of government ministries and production facilities with respect to edible salt. It required that all producers of edible salt apply for and be granted a special “certificate of eligibility and qualification” from the MoH. Furthermore, producers of iodized salt needed an internal quality control system and to meet established hygiene and quality criteria. Decree 19 required all salt producers to procure potassium iodate (KIO3) only from the NIDDC, through the HoE. Decree 19 therefore created a separate system for the production of iodized salt, rather than incorporating iodization into the routine practices of the salt industry. Moreover, producers of iodized salt had to comply with several additional requirements than producers of other salt and were closely monitored by and dependent on the NIDDC.
Salt is produced throughout the country from sea salt and mined rock salt, with the majority produced in southern Vietnam by solar evaporation. It is produced by a mixture of private producers, members of the National Salt Corporation (NSC) of Vietnam (a state-owned corporation), and provincial government authorities. A list of all salt producers do not exist, but the Ministry of Industry and Trade (MoIT) reported in 2005 (Ministry of Industry and Trade, 2005) that Vietnam produces about 1 million metric tons (MT) of salt per year, with about 300 000 MT of that being sold in retail packs for household consumption. The remaining amount is used by (nonfood) industry (200 000 MT) for animal consumption, food processing (400 000 MT) and export (100 000 MT). Imports of food grade salt are not permitted, and high-grade industrial salt is imported under a quota system.
In 2003, 75 NSC, private and provincial producers registered with the NIDDC program, undertook salt iodization. All registered producers received free KIO3 from the NIDDC. No other salt producers manufactured iodized salt. In 2003, KIO3 disbursements suggested that 206 501 MT of iodized salt was produced, providing about 71% of the estimated national requirements. About 55% of the total supply of iodized salt was produced by the NSC facilities. Private and provincial producers produced the remainder. The remaining amount of salt required for household consumption was believed to be noniodized salt produced by other producers. Because a total list of salt producers did not exist, it was not possible to control the production of noniodized salt for human consumption, except through market monitoring, which was not routinely practiced.
Although salt production overall was under the direction and assistance of MARD, the production of iodized salt was essentially managed by the MoH. This administrative arrangement created 2 salt production systems in Vietnam, with iodized salt seen as a “special, health commodity.” In addition, MARD was critical of the iodized salt program as it was seen as limiting the salt trade and having negative impacts on salt farmers and the salt industry (unpublished data). Collaboration between the MoH/HoE and MARD and the NSC was very limited, and information was not routinely shared between them, despite the existence of the Central IDD Committee.
Coverage of iodized salt was greatly facilitated by a government subsidy for essential items for people living in remote and disadvantaged areas, such as mountainous areas, offshore islands, and ethnic minority areas. Government Decree 20 12 aimed to ensure that people living in subsidy areas could buy iodized salt, and other essential products, for the same price as in mountain towns through subsidies for transport costs. The subsidies were allocated to Provincial People’s Committees (PPCs), which passed them on to NSC or selected local salt iodization facilities. The subsidy system benefited an estimated 12 million people in 2004 or just under 15% of the Vietnam’s population (note 2). In addition to subsidizing supplies of iodized salt, PPCs were encouraged to introduce local regulations banning the production, sale, and distribution of noniodized salt. Thus, in subsidy areas, selected salt producers were paid to supply iodized salt, and noniodized salt was banned, essentially ensuring household use of only iodized salt. Many provinces in the subsidy areas achieved 100% coverage with adequately iodized salt as a result of the subsidy system.
An extensive and effective internal and external quality assurance system was established for producers of iodized salt. Internal quality assurance requirements were specified in Decree 19 and its implementing guidelines, and all registered iodized salt producers had an on-site titration laboratory and tested each batch of salt. Staff of the provincial IDD department visited registered producers of iodized salt, usually twice per month, to take samples for titration testing in the provincial salt laboratory present in all provinces. In 2003, 11% of the NIDDC budget (excluding the proportion spent on purchase of KIO3) was spent on external quality assurance monitoring. Therefore, there was capacity and incentive to ensure accurate iodization, and the quality of iodization was high.
Significant investments in information, education, and communication (IEC) on IDD and iodized salt were undertaken at all levels. These IEC activities achieved high levels of public awareness about iodine deficiency, and the 2005/2006 National Survey 13 found that 99% of people knew that goiter was a consequence of iodine deficiency and 46% knew it also caused mental retardation. The IEC activities were not able to remove negative impressions of iodized salt; however, in the same survey, when asked about reasons for not consuming iodized salt, 34% of people said they were “in the habit” of using noniodized salt and 24.5% said iodized salt had a bad taste and smell. In 2003, 33% of the NIDDC budget (excluding the proportion spent on KIO3) was spent on IEC.
The monitoring and evaluation component of the Vietnamese NIDDC program was a clear strength. The system consisted of periodic household and school-based surveys and frequent surveillance surveys. The surveillance surveys were undertaken by provincial IDD committees 3 times per year and collected information on household iodized salt coverage, use of other salty condiments, knowledge, attitudes, and practices, and urinary iodine levels. National household surveys were undertaken in 1997, 1998, 2000, 2003, and 2005/2006, and school-based surveys were undertaken in 1994, 1998, 2000, 2003, and 2005/2006. The surveys assessed iodine content in household salt (note 3) and urinary iodine concentrations (UICs) in women reproductive age (16-49 years) and children of 8 to 10 years. Goiter data were also collected from school surveys. These 2 data collection systems, in particular the household surveys, generated significant amounts of data for evaluation and fine-tuning of the program. In 2003, 33% of the NIDDC budget (excluding the proportion spent on KIO3) was spent on monitoring. The monitoring system was funded and supported wholly by the NIDDC. None of the monitoring activities were integrated into other existing systems.
Achievements of the NIDDC Program: 1994 to 2005
The NIDDC program enabled Vietnam to achieve the goal of USI and eliminate IDD within a decade. National surveys from 1994, 1998, 2000, 2003, and 2005/2006 indicated that household coverage of adequately iodized salt increased from 24.9% in 1994 to 93% in 2005/2006, 14 reaching the international goal of >90%. 2 As a result, the proportion of school-age children with MUIC <100 μg/L fell from 84% in 1994 to 43.5% in 1998, and the MUIC of school-age children increased from 14 μg/L in 1998 to 130 μg/L in 2005/2006. Similarly, the MUIC among women of reproductive age was maintained above 100 μg/L between 2000 and 2005/2006. In addition, goiter rate in school-aged children fell from 12.9% in 1998 to 3.5% in 2005/2006 (Figure 1). The global and national targets were to achieve a total goiter rate of less than 5%. Subnationally, 5 of 7 regions achieved >90% household use of adequately iodized salt (and in the other 2, it was over 85%), and UIC of reproductive age women was >100 μg/L in 6 of 7 regions in 2005/2006. Only in the Mekong River Delta region, was women’s UIC inadequate.
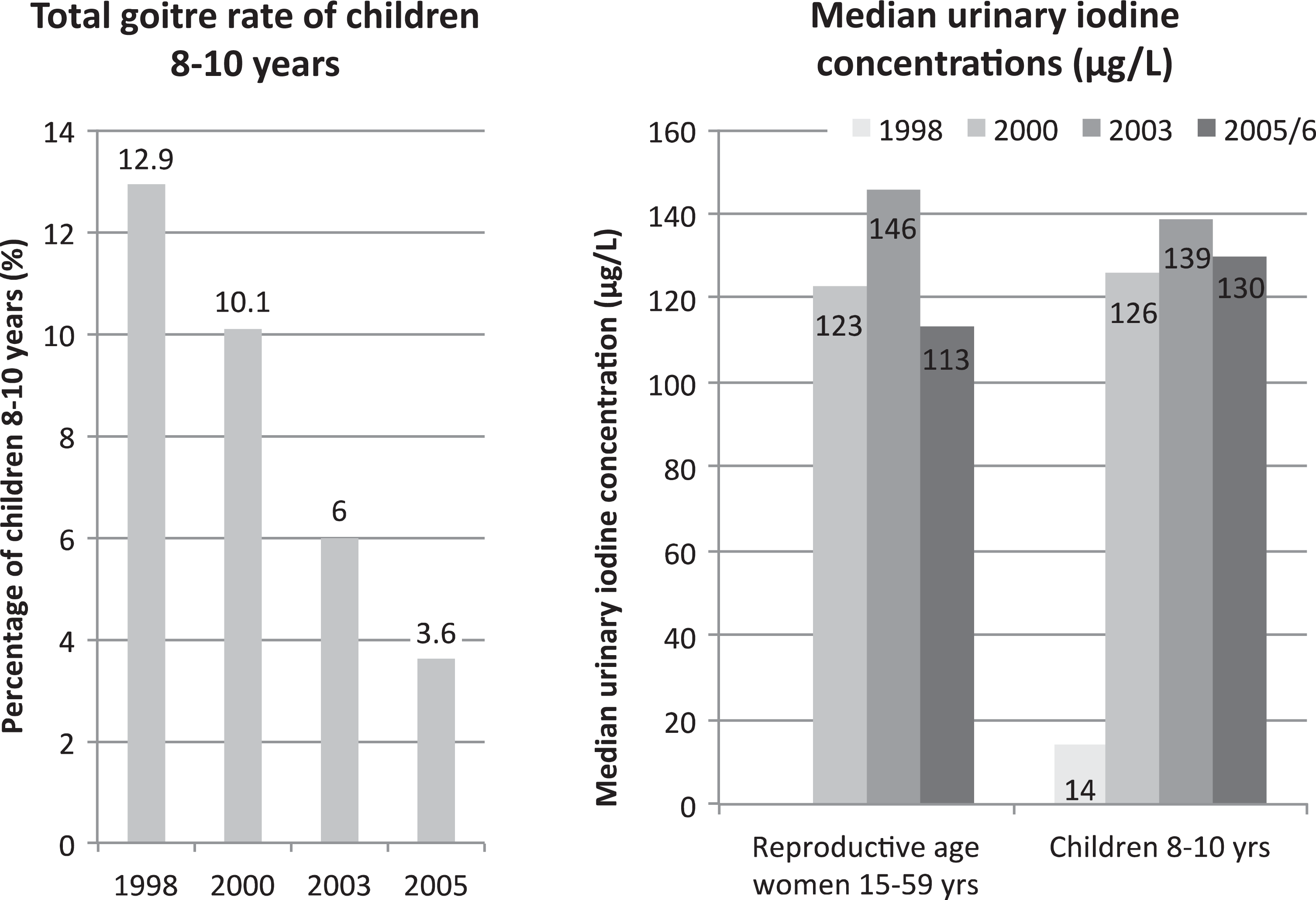
The National IDD Control (NIDDC) Program Achievements: 1994 to 2005: Health impact. National goiter target is <5%, and optimal median urinary iodine concentration for reproductive age women and children is 100 to 200 μg/L. 15
National surveys from this period recorded that processed foods were not made with iodized salt, in particular frequently consumed salty condiments. Almost 100% of households in all regions of Vietnam, except the North Mountain region, consumed fish sauce, and very little of this was made with iodized salt. On the other hand, about half of all households in the North Mountain and Red River Delta regions consumed bot canh, a seasoning powder that included iodized salt. This was potentially a problem because in Vietnam, salty condiments are frequently consumed in place of household salt. A study in 2004 16 found that total salt consumption (including household salt, salt from fish sauce, seasoning salt [bot canh], and soya sauce) in the Mekong River Delta was 10.99 ± 5.18 g/d, of which 5.06 g came from household salt, 3.6 g came from fish sauce, and the remainder (2.33 g) came from bot canh and soya sauce. The study calculated that at the current salt iodization levels, people with this pattern of consumption would only achieve 50% of their iodine requirement if only household salt was iodized. Another study showed that overall intakes of salt were relatively similar across 6 provinces; consumption varied between 10 and 14 g per person per day. 17 A further study of sodium intakes in a rural district of Hanoi found the mean salt intake to be 10.8 ± 3.3 g/d. It also showed that seasoning, such as bot canh and fish sauce, made up 67% of sodium intake compared to just 6% from household salt. Other processed foods contributed 11.6% of sodium intake, with the majority coming from instant noodles (unpublished data; Figure 2). These data suggest the optimal way to ensure appropriate iodine intakes and to ensure all foods, in particular salty condiments, are made with iodized salt. This strategy recognizes that patterns of household salt and salty condiments vary throughout the country and is easier to monitor and enforce the iodization of all salt than direct iodization of selected salty condiments. A study has shown that iodine losses from fish sauce made with iodized salt are minimal, and there are no significant negative effects on the appearance or taste of fish sauce. 18
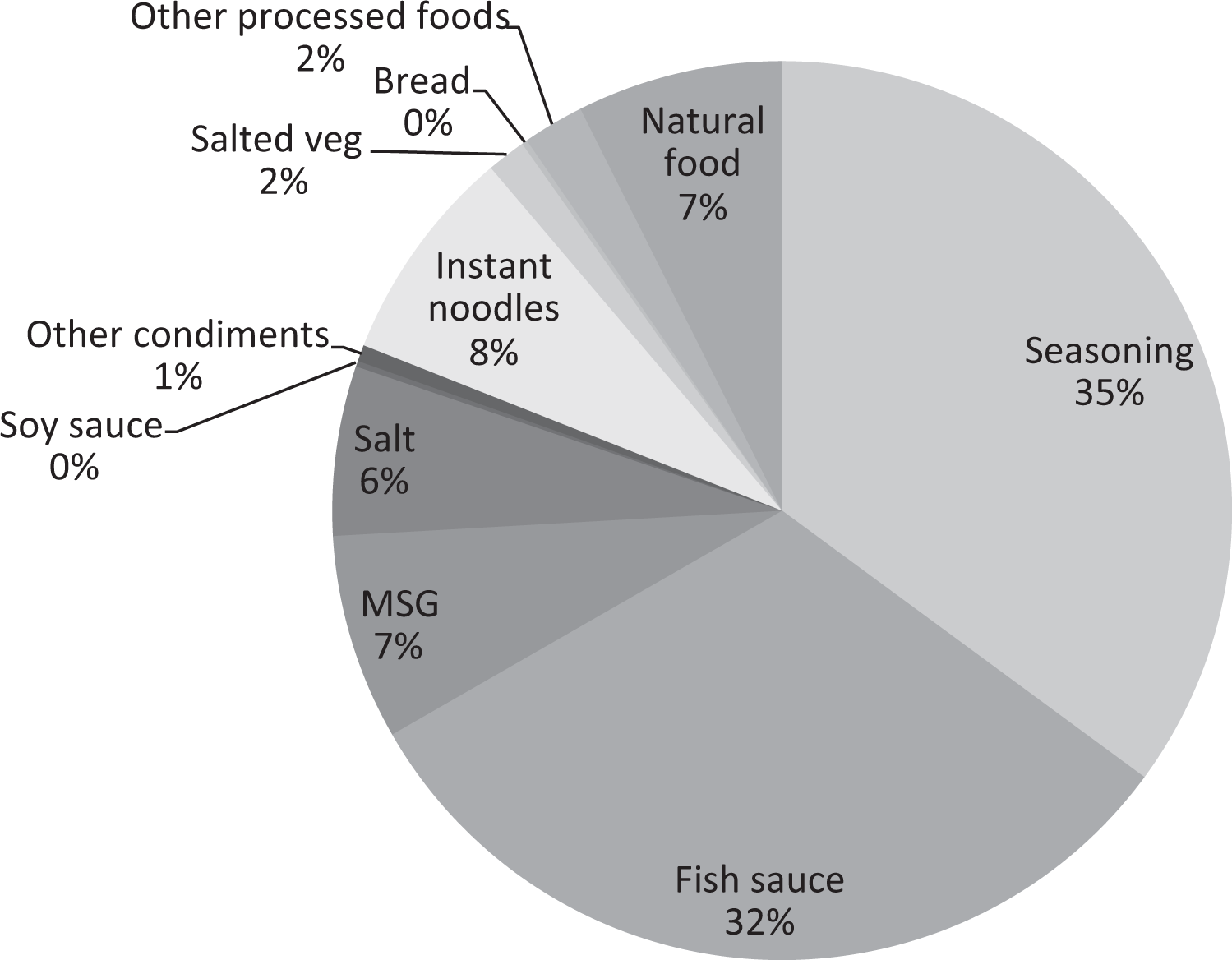
Sources of sodium intake in a rural district of Hanoi (unpublished data).
The Decline of USI in Vietnam: 2005 to 2015
The 2005/2006 national survey indicated that Vietnam had achieved national USI that reproductive age women’s median urinary iodine levels were within the WHO recommended range and that the total goiter rate of children had declined below the national and global target of 5%. As global and national targets had been met, the Government of Vietnam downgraded the NIDDC program to be a routine program. This decision led to a change in management and supervision structure, a cut in the budget, and the issuance of a new Decree. As a result of these programmatic changes, there was a dramatic decline in iodized salt coverage and urinary iodine levels to the extent that IDD has reemerged as a public health problem. In 2008/2009, just 3 years later, median urinary iodine levels of women fell to 83 μg/L and only 70% of all Vietnamese citizens were consuming adequately iodized salt. Household consumption of adequately iodized salt further declined to 45% by 2011 (Figure 3).
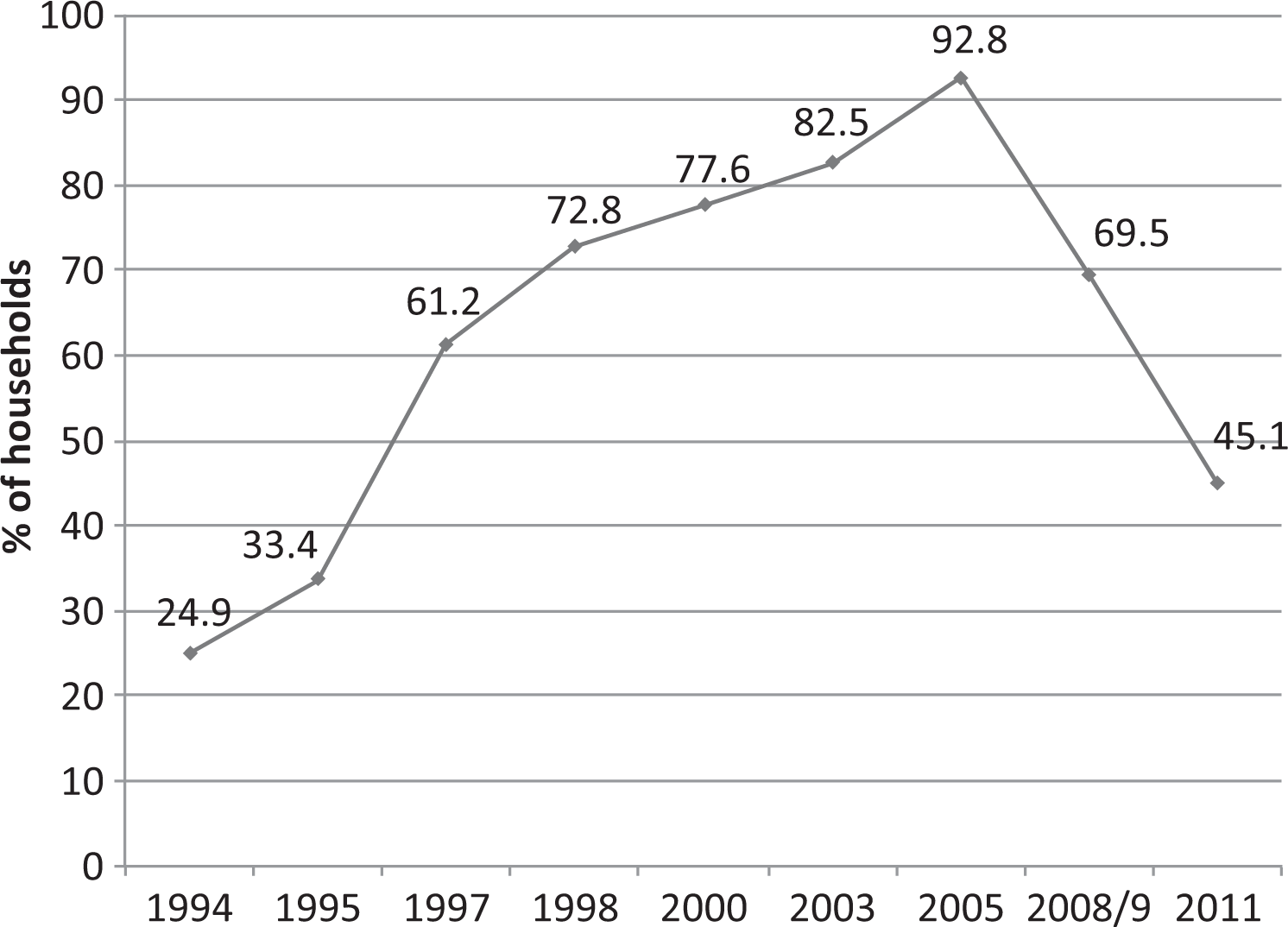
Household consumption of adequately iodized salt: 1994 to 2011. 19
At the time of the 2008/2009 national survey, coverage of adequately iodized salt had declined in 5 of the 7 regions, while in Hanoi (not previously measured as a separate region in the national surveys), coverage had fallen from 100% to 26%, the lowest of any region. In Ho Chi Minh City, the coverage was also very low at 54% (Figure 4). Urinary iodine levels had also fallen such that MUICs for women were lower than the optimal range in 5 of 8 regions and borderline in 2, in 2008, compared to only 2 regions in 2005 (Figure 5).
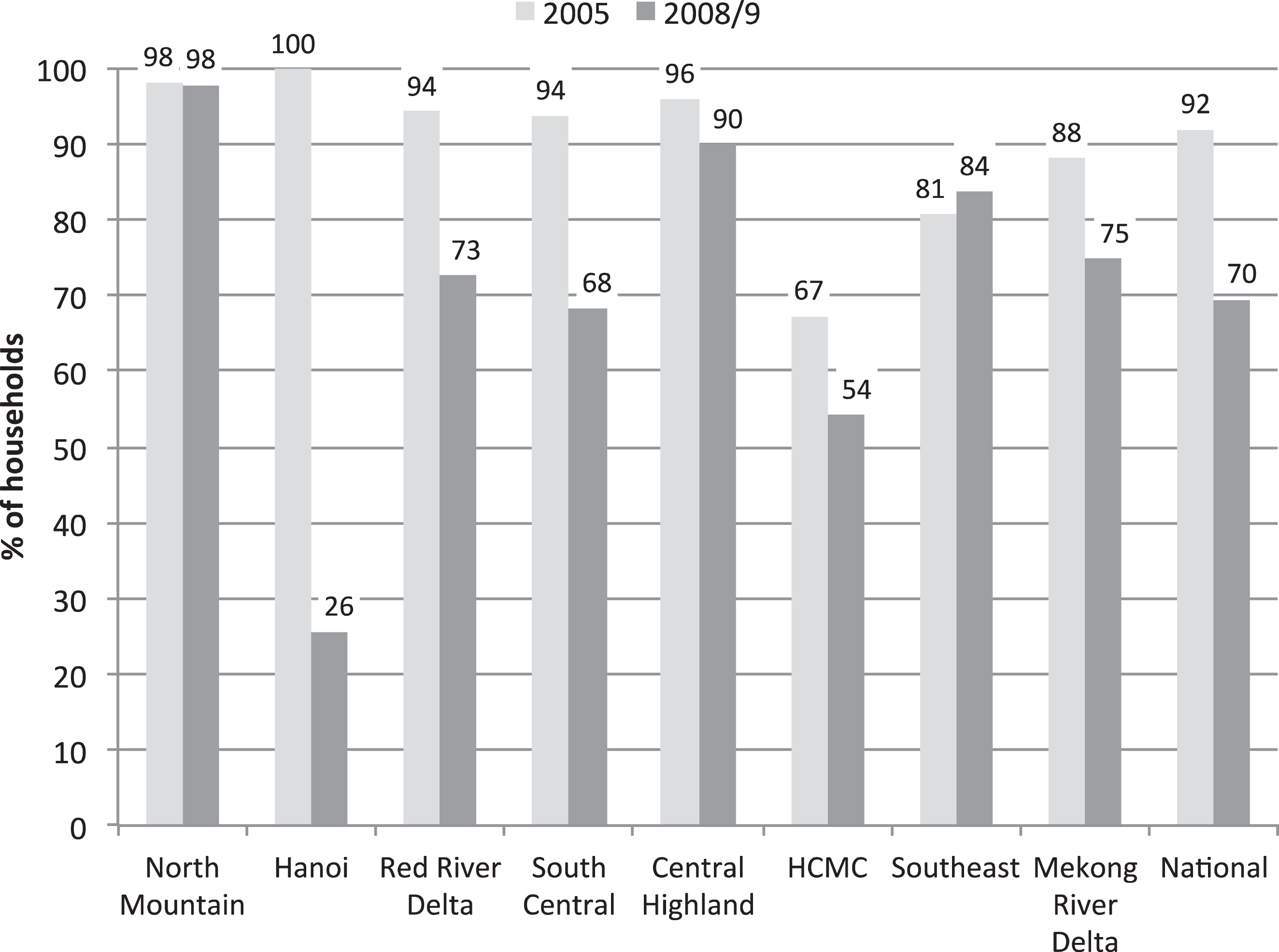
Coverage of adequately iodized salt, 2005 and 2008/2009. 15
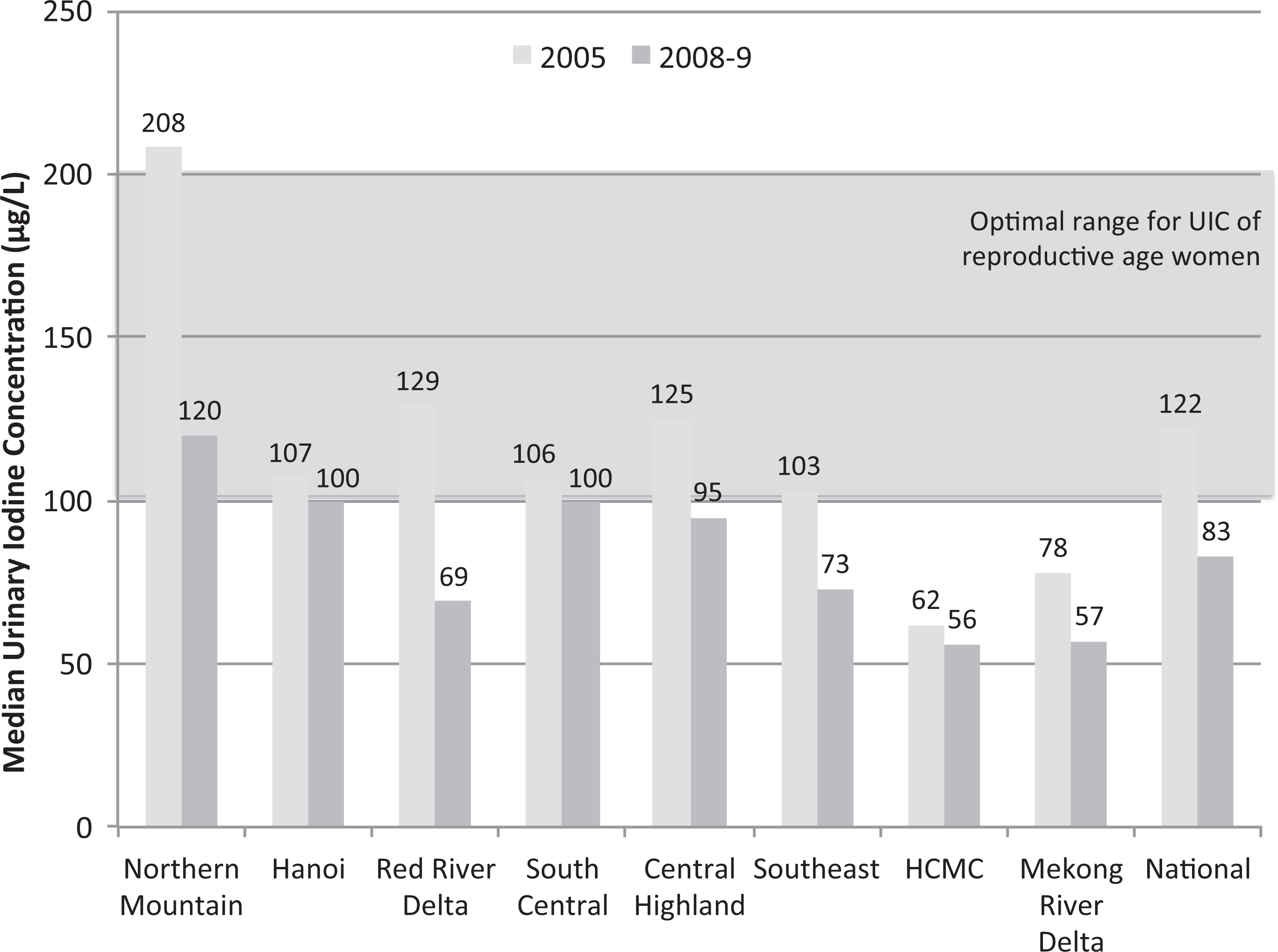
Median urinary iodine concentration of reproductive age women, 2005 and 2008/2009. 15
The iodine status of pregnant women, the population group most severely affected by iodine disorders, 20 was particularly alarming. Three small-scale studies measured UIC in this population group between 2008 and 2010 in a number of different provinces and regions of Vietnam. The studies reflect the situation in 2 regions in the south and in Ho Chi Minh City, 21 a province in the Mekong River Delta (south), 22 and another in the Red River Delta (north). 23 The MUIC of the pregnant women studied ranged from 52 to 71 μg/L, far below the optimal level of 150 to 249 μg/L, recommended by WHO. 2
There are several reasons for the dramatic decline in achievements of the NIDDC program. In 2005, the NIDDC program was changed from a “national priority program” to a “routine program.” As a result, the Central IDD Committee was disbanded, the number of staff for the NIDDC program was scaled down, and the budget was cut. Although the HoE was still designated as the central-level institution to advise and implement IDD control activities, many central-level activities such as monitoring, training, maintenance of the regional and provincial urinary iodine laboratories, and supervision were drastically reduced due to budget and staff constraints. Primary responsibility for implementing the IDD control program was transferred to the PPCs. The budget cut meant that funds were no longer transferred to the provinces for program implementation and insufficient budget was available for the purchase of KIO3. The HoE figures indicate that procurement of KIO3 declined from about 75% of national requirements between 2006 and 2008 to about 20% in 2011. In the context of voluntary salt iodization, the decline in government budget for KIO3 was a major disincentive for continued salt iodization.
Potassium iodate shortages may have contributed to the apparently high proportion of noniodized and inadequately iodized salt use recorded by the Multiple Indicator Cluster Survey (MICS) in 2011. 19 The MICS reported, for the first time, on household usage of noniodized and inadequately iodized salt (as measured by rapid test kits) rather than coverage of adequately iodized salt only, and the data indicated that in 2011 more than one-third of households were using noniodized salt and 16% were using inadequately iodized salt. In several regions, more than 50% of household salt was either inadequately iodized or not iodized at all. In 2010, the categorization of ecological regions was changed, and this survey used the new ecological regions. Therefore, analysis and presentation of subnational trends in household iodized salt coverage from 2005 are not possible (Figure 6).
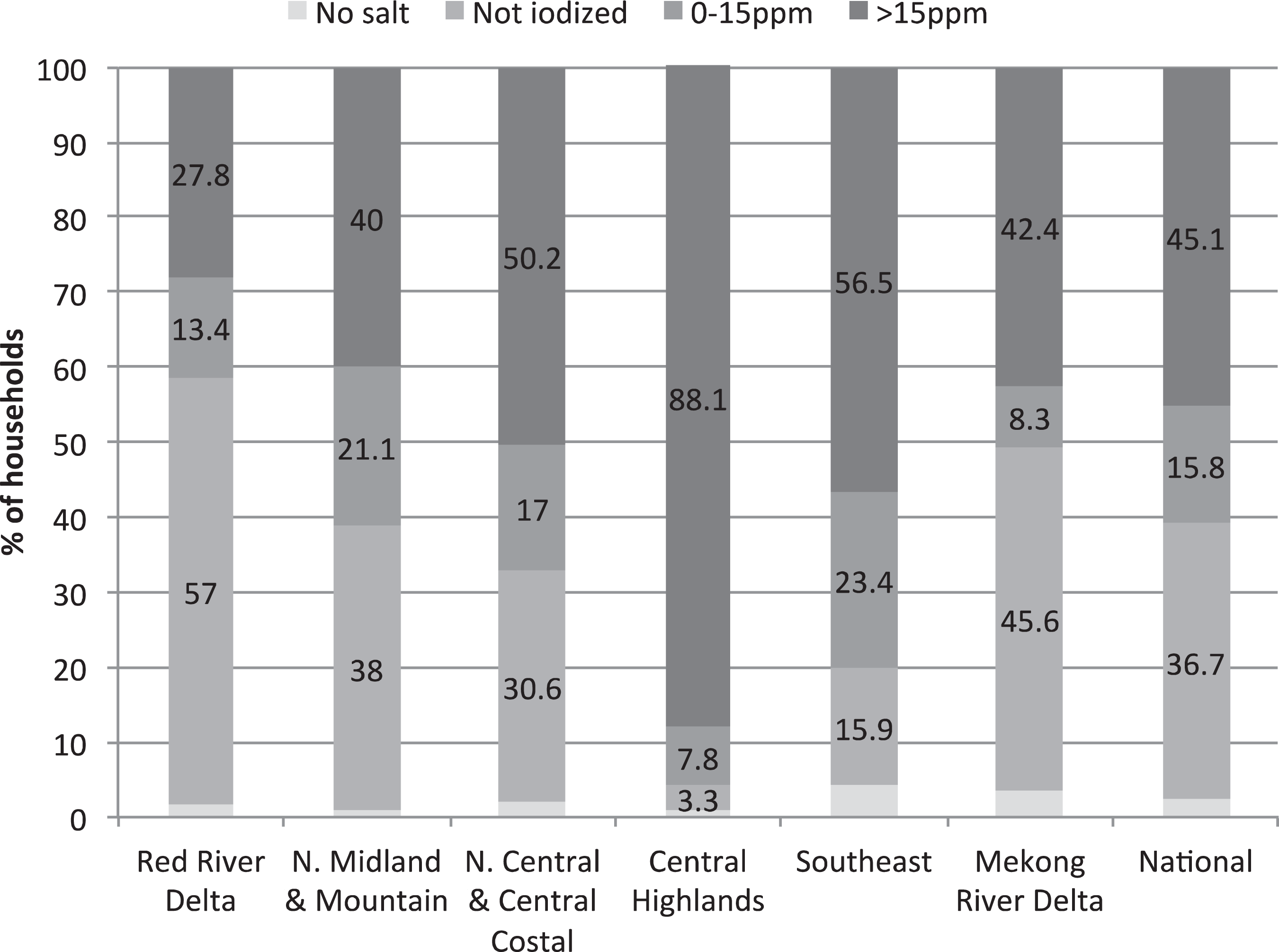
Household consumption of iodized salt, 2011. 19
Low iodized salt coverage in the North Midland and Mountain and Red River Delta regions shown in Figure 6 is potentially due to changes in the salt subsidy program. Although the subsidies were given directly to salt producers previously, in 2010, the administration of the program was changed and the subsidies were instead given directly to the provinces to procure subsidized items for their population or to give the funds directly to families to purchase normally priced goods. 24 Several provinces elected the latter option, but families did not necessarily use the funds to purchase iodized salt. The new system also meant that some salt producers were no longer receiving orders for iodized salt for the subsidy program and either switched to producing noniodized salt or closed down altogether because they lost the competitive advantage they benefited from under the subsidy system. The total budget for the subsidy system from the central level was also reduced, with provinces expected to make up the difference.
A further reason for the decline in iodized salt coverage is that Decree 19 was replaced with Decree 163 in December 2005. 25 Despite the weaknesses of Decree 19, Decree 163 is significantly weaker. Unlike Decree 19 that called for the iodization of salt for human consumption, Decree 163 establishes “conditions for the production and supply of adequately iodized salt for human consumption” and indicates the roles and responsibilities of various ministries and the PPCs in ensuring that iodized salt is available. It calls on the MoH and Ministry of Culture and Information to encourage people to use iodized salt, but it does not require the iodization of all salt for human consumption (or food processing) and also does not require the MoH to provide free KIO3. As a result, there is little incentive for salt processors to iodize.
Despite high political commitment, the Vietnamese NIDDC program, as designed and implemented between 1994 and 2005, was not sustainable. It relied on iodized salt subsidies and was not based on a commercially viable business model, with a subgroup of salt producers only producing fortified salt because they were provided with free KIO3. The salt subsidy and free KIO3 and the nature of governance in Vietnam made up for deficiencies in the legislation, which did not require the iodization of “common salt.” The data generated by the strong monitoring and evaluation system also motivated provinces to ensure the availability of iodized salt and encourage its purchase.
In 2005, if the NIDDC program had been downgraded but the salt iodization legislation had been strengthened, it is likely that, after a transition period, USI could have been maintained. If the legislation had been amended to make salt iodization mandatory, as in other countries, the salt industry would have taken on the responsibility of salt iodization. Instead, Vietnam is now in a position similar to that at the start of the IDD program in 1994, when coverage with iodized salt was 24.9% and iodine status was deficient for most of the population. The only aspects that remain of the success of the NIDDC program is the knowledge among some salt producers about how to produce quality iodized salt and public knowledge of its benefits and the experience of using it. However, valuable lessons have been learned about sustainability and how to build back better.
Universal Salt Iodization and the Elimination of IDD in Vietnam—Building Back Better: 2015 Onward
The dramatic decline in iodized salt coverage and UICs has caused concern among health authorities in Vietnam. There is now agreement within the government that the NIDDC program has to be reformulated and revived, and new legislation to make salt iodization mandatory is currently being developed. Reestablishment of the program was also recommended by the International Council for the Control of Iodine Deficiency Disorders (ICCIDD) Global Network (note 4), UNICEF, and WHO in 2012. 26 Throughout the world, salt iodization has proven to be an effective strategy for eliminating IDD. 5 The objective in Vietnam must therefore be to create an environment in which salt iodization is effective and sustainable. Recommendations of the authors, who include individuals directly involved in the NIDDC, for how the new program might be designed are discussed subsequently, drawing upon lessons learnt in Vietnam and experiences of other countries in the region.
The downgrading of the NIDDC in 2005 was not based on a retrospective analysis or programmatic review and evaluation but rather on a rapid decision taken on the basis of achievement of program targets and an apparent misunderstanding that IDD had been “eliminated.” In order not to repeat the mistake, the design of the new program must be based upon a full understanding of (1) why the program was successful during the national priority program phase, (2) why the second phase failed, and (3) what the current situation is. Multisectoral consensus is needed on these issues as it will form the basis for necessary multisectoral collaboration and cooperation when implementing the new program. 27 Information on who produces salt (including noniodized salt) and how salt for food processing is sourced and used should be collated from MARD, the NSC, and the MoH, as information on the salt industry has long been lacking. It would also be useful to understand how the salt subsidy system is operating and what future plans are.
Global experience is that in order for food fortification programs in developing countries to have a public health benefit, it is necessary that they are mandatory and universal. In 1 decade, countries with mandatory legislation had a greater increase in household coverage (49%-72%) than countries with voluntary iodization (40%-49%). 28 Revised Vietnamese legislation for salt iodization should therefore make salt iodization mandatory, and it should apply to all salt for human and animal consumption, including salt for food processing. 29 As discussed, this is to address the fact that salty condiments are frequently consumed in place of household salt in Vietnam and that iodizing all salt for food processing will be much easier to monitor and enforce than a requirement for all or selected processed foods to be iodized directly. Revised legislation will also need to address the fact that no category of “salt for human consumption” or “food grade salt” appears to exist in Vietnam, which made it difficult for Decree 19 to require the iodization of all food grade salt. Development of the legislation will also have to overcome arguments that consumers should have the right to choose and that salt should be voluntarily iodized with public health campaigns promoting its use. The right to choose by some denies the right to good nutrition by others, as global experience shows that public health campaigns that try to educate the public to choose healthier products over less healthy ones are seldom successful. 28
The new legislation should establish mandatory iodization of all food grade salt within the routine food control system of Vietnam, such that it is monitored and enforced through routine food control systems and not a separate, stand-alone program. One way of doing this may be to simply establish a national technical regulation for food grade salt, including iodization, which replaces the current national technical regulation for iodized salt (note 5). Another option under discussion is to have a Decree on Food Fortification, under the recently passed Food Safety Law. The Decree could mandate the fortification of all food grade salt and other foods deemed important, such as wheat flour and cooking oil. This would follow the example of the Philippines which has an Act mandating the fortification of rice, wheat flour, cooking oil, sugar, and other foods as designated by the MoH. 30
The government will need to decide whether it wishes to continue to provide free KIO3 for salt iodization. Vietnam is currently the only country in the East Asia and the Pacific and South Asia regions (note 6) in which the cost of KIO3 is borne by the government, with the exceptions of Afghanistan and the Democratic People’s Republic of Korea. 31 If all food grade salt is required and enforced to be iodized, there is no need for the government to cover the cost for KIO3, as a “level playing field” will have been created in which all producers have the same costs for iodization, which they can either chose to absorb or pass onto the consumer. In order for optimal legislation to be passed, the support of a variety of ministries will be needed including the Ministry of Justice, Finance, and MARD. It will therefore be necessary to dialogue and advocate with them in advance of submission of new legislation for mandatory salt iodization in order to ensure their support.
It seems unlikely, and potentially counterproductive, that the IDD program would be reestablished as a national priority program. Neither should it be a stand-alone, vertical program. Ideally, it would be part of a general food fortification program or a micronutrient program or it might be part of a program to control and prevent noncommunicable diseases (NCDs), linked to obesity reduction, hypertension prevention, and reduced salt intake, as recommended by the joint ICCIDD Global Network, UNICEF, WHO mission in 2012. 26 There are pros and cons of all the options and these should all be considered before a decision is made. Regardless of how it is positioned, salt iodization should be coordinated with a campaign to reduce salt and sodium intake. 32
Depending on how the salt iodization program is managed, a multisectoral committee that has an oversight function over USI and the elimination of IDD (and possibility other responsibilities) is likely to be needed. This committee should give a much more prominent role to MARD, the NSC, and MoIT than in the previous National Committee for the NIDDC to reflect the fact that salt iodization will be implemented as a routine aspect of salt production in Vietnam. Although the MoH and the HoE should be key members of the committee, ideally a Ministry other than Health or MARD should chair the committee in order to facilitate interministerial collaboration, and the Ministry of Planning and Investment or the Deputy Prime Minister’s Office might be appropriate, especially if salt iodization is implemented as part of a multisectoral strategy to reduce NCDs.
The responsibility of quality assurance of iodized salt should fall to salt producers themselves (internal monitoring) and the VFA, as the primary government institution is responsible for food control (external monitoring). 33 All producers of food grade salt should be monitored by the VFA on all aspects of quality food production, including the national technical requirement for food grade salt, which includes iodine content, in order to ensure food safety and quality. The MARD, NSC, or VFA should support salt producers to implement necessary quality assurance systems in their factory laboratories. Any requirement for salt producer registration/certification should be applied to all producers of food grade salt, rather than only those that produce iodized salt. The VFA should also be responsible for ensuring that food processors use iodized salt, once again, as part of routine food quality assurance measures.
The role of the MoH should be to establish the technical standard for food grade salt and KIO3 and to monitor the outcomes of the program, that is, the household coverage of adequately iodized salt and salty condiments, and UICs of target populations, in particular reproductive age and pregnant women. Measurement of these 2 indicators should be incorporated into appropriate existing national surveys such as national nutrition or health surveys. Only information that can guide program implementation should be collected, and all data collected should be reported to all stakeholders and used for identification of problems and program management. 34
The laboratory of the HoE should be established as the national monitoring laboratory for urinary iodine and sodium excretion. It should provide quality assurance for all regional and provincial laboratories carrying out urinary iodine and sodium excretion analysis. Although if urinary iodine is only to be measured in periodic national surveys, it may not be necessary to maintain the original number of regional and provincial laboratories. Any laboratories that do routinely carry out urinary iodine analyses, and certainly the national reference laboratory in the HoE, should enroll in the US Centers of Disease Control Ensuring the Quality of Urinary Iodine Procedures (EQUIP) quality assurance program for urinary iodine analysis (note 7).
If all food grade salt is iodized, such that only iodized salt is available for purchase, there will be no need to maintain the subsidy system for iodized salt. Along the same lines, if all food grade salt is iodized, it will no longer be necessary to have a large budget for IEC on IDD and iodized salt. Nevertheless, the central level and all provinces should increase public understanding of the value of iodized salt for preventing IDD. The IEC on iodized salt should be coordinated with education on reducing sodium/salt intake, and the role of iodized salt in protecting optimal brain development, rather than causing goiter, should be highlighted.
Conclusions
Although the scourge of iodine deficiency has returned to Vietnam and less than half of the population is currently using adequately iodized salt, important lessons can be learnt from the rise and fall of USI. This article has attempted to summarize some of these lessons and make recommendations for how to apply them to reestablish USI in Vietnam on a more sustainable and effective basis. Many of the lessons would apply equally to USI programs in other countries. It is the hope of the authors that the experience of Vietnam helps to demonstrate some fundamental components of a sustainable food fortification program with public health impact. These program components include national mandatory legislation with an accompanying enforcement system, establishment of fortification as a norm within the food industry through the creation of a supportive and safe environment, multisectoral collaboration within the government and partnership with industry, and an effective monitoring and evaluation system.
Footnotes
Authors’ Note
All authors have seen and approved the contents of the submitted manuscript. Primary data collection for the review was undertaken by Karen Codling, public nutrition consultant, based on semistructured interviews with stakeholders of the salt iodization program in 2013 and a review of a variety of documents, reports, evaluations, and surveys from the Vietnam salt iodization program. She also drew upon several years of personal experience with the Vietnam salt iodization program, including a program assessment and field visits. Nguyen Vinh Quang and Le Phong provided assistance in the writing of the review article based on their personal involvement in the program. Roger Mathisen, Nguyen Dinh Quang, France Bégin, and Do Hong Phuong contributed significant inputs and insights based on their own knowledge of the program and other salt iodization programs in the region. Roger Mathisen was and France Bégin is a UNICEF staff member. The opinions and statements in this article are those of the authors and may not reflect official UNICEF policies.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: UNICEF Vietnam coordinated and supported the preparation of this review article. Financial support for preparation of this article was provided by the US Agency for International Development (USAID).