
Abstract
Palestine refugees comprise the largest refugee population in the world, most of whom are encamped in Middle Eastern countries. In the Gaza Strip, where ∼1.4 million Palestinians reside, there are high prevalences of anemia and multiple micronutrient deficiencies (MNDs), including those of iron, zinc, vitamins A, B12, D, and E, ranging from 11.4% to 84.7% among pregnant women and 2.9% to 70.9% among preschool children. Dietary diversification and adequate food fortification are framed in policies but remain aspirational goals. Alternative, effective, targeted preventive approaches include, for women, replacement of antenatal iron-folic acid with multiple micronutrient supplementation, and for young children, point-of-use multiple micronutrient powder fortification to prevent anemia, both of which can reduce other MNDs and may bring additional health benefits. These interventions coupled with monitoring of dietary intakes, periodic assessment of MNDs, and implementation research to improve existing nutrition interventions are warranted to protect the health of the Middle East Palestinian diaspora.
Introduction
There are approximately 5.5 million registered Palestine refugees living in the Middle East, representing the largest refugee population in the world. 1 The United Nations Relief and Works Agency for Palestine Refugees in the Near East (UNRWA), established on December 8, 1949, was mandated by the United Nations General Assembly to provide humanitarian aid and protection to registered Palestine refugees across 5 fields of operation located in Jordan, Lebanon, Syria, the West Bank, and the Gaza Strip. 1,2 The UNRWA provides primary health care through 144 health centers, elementary and secondary education, relief and social services, camp infrastructure and improvements, microfinance, and emergency response to this vulnerable population. 1 Over the last 3 decades, host countries and territories in the region have experienced substantial demographic, economic, political, social, environmental, and dietary changes that likely impact the quality of life, mental health, and general health of the Palestinian refugees. With respect to diet, each of these host countries are undergoing a nutrition transition, characterized by a shift away from a healthy Mediterranean Diet, rich in vegetables, pulses, grains, and olive oil, to a diet higher in other fats, added sugars, and salty, processed foods. 3 While these host populations experience an escalating burden of overweight, obesity, and noncommunicable diseases, 4,5 encamped Palestinians are experiencing similar trends but with also a documented high burden of multiple micronutrient deficiencies (MNDs), 1,6,7 attributed to limited availability of nutritious food within a constrained food system, exacerbated by stresses from crowding, joblessness, political instability, and conflict. In the Gaza Strip particularly, where approximately 1.4 million Palestine refugees reside, populations experience restricted movement due to an imposed blockade and limited access to food and basic goods wrought by periodic armed conflict, restrictions on trade and investment, economic stagnation, and inadequate purchasing power (Figure 1). 1,8 Socioeconomic deterioration in this society is evidenced by one of the world’s highest unemployment (46%) and poverty (53%) rates. 9,10 It is estimated that 68.5% of the population in the Gaza Strip is food insecure and 51.8% of households receive food or monetary assistance through the international agencies, such as the World Food Program (WFP), the United Nations Children’s Fund, and UNRWA. 10

Market in the Gaza strip. Photo by Dr Ghada Al-Jabda.
Given that improved food access and dietary diversification have been challenging to achieve, UNRWA primary health care centers have long sought to mitigate consequences of MNDs by providing high-potency, 6-monthly vitamin A supplements to children aged 6 to 59 months to reduce risks of xerophthalmia and severe morbidity, 11 iron-folic acid (IFA) supplements to prevent anemia among pregnant women in the second to third trimesters and 3 months after delivery, 12 and therapeutic iron to patients with anemia (Figure 2). In 2006, the Ministry of Health in Palestine began implementing an extensive program to fortify wheat flour with vitamins B1, B2, B6 B12, A, and D, folic acid, niacin, iron, and zinc, 6,7,13,14 requiring all of the wheat flour in the Gaza Strip, including that produced by 3 local mills, to meet the stated technical specifications. 14 While the policy has remained in place, a recent World Health Organization (WHO) study found only 11% and 1.7% of flour consumed by the population in the Gaza Strip to meet the prescribed iron and other micronutrient fortification levels, respectively. 14 Among cited challenges to this program are restrictions on imported supplies at the border, suboptimal monitoring and tracking of operational processes, and a lack of subsidization for premix purchase leaving mills to either absorb its cost or raise the price of flour, 14 neither of which are economically feasible.

Antenatal clinic in the Gaza strip. Photo by Dr Ghada Al-Jabda.
Objectives
The purpose of this commentary is to raise awareness of the burden of MNDs among the Palestinian refugee diaspora in the Middle East, particularly among pregnant women and preschool-aged children in the Gaza Strip and offer recommendations for strengthening the prevention of MNDs in this nutritionally, economically, and politically vulnerable population.
Methods
The design and methods of the Palestinian Micronutrient Survey in 2013, conducted by the State of Palestine Ministry of Health, have been previously described. 7 Briefly, the survey was conducted in 2013, by sampling 600 pregnant women and 600 children aged 6 to 59 months at health clinics, which yielded 587 pregnant women and 582 children aged 6 to 59 months in the Gaza Strip. In addition to measuring hemoglobin to estimate the prevalence of anemia, 7 a Chemiluminescent Microparticle Immuno Assay was conducted to assess ferritin, 15 folic acid, and 25-OH-cholecalciferol, 16 and ultra-performance liquid chromatography with UV-detection was used to assess retinol, β-carotene, and α-tocopherol. 17 Serum data were available and reported for 587 pregnant women aged 18 to 43 years and 582 children aged 6 to 59 months in the Gaza Strip. 6,7,18 Findings are summarized in tables as percentages of individuals anemic and below-defined cutoffs to assess prevalence (with imputed 95% confidence intervals) of nutrient deficiencies for pregnant women and children aged 6 to 59 months. Survey findings related to anemia have been further supplemented with 2019 UNRWA health department annual report. 2 The reports from WFP 8 and WHO 14 have been reviewed to summarize program activities.
Results
Among pregnant women, the prevalences of anemia (plasma hemoglobin <110 g/L) were estimated to be 20.7% in the first trimester and 42.8% in the second to third trimesters, whereas iron deficiency (serum ferritin <12 ng/mL) was 23.6% in the first trimester and 38.6% in the second to third trimesters (Table 1). 7 The prevalence of zinc deficiency was strikingly high, with rates of 67.9% in the first trimester (<8.6 µmol/L) and 84.7% in the second to third trimesters (<7.6 µmol/L). 6,7 While <2% and 10% were low-to-deficient in folate in the first and second to third trimesters, respectively, the prevalences of deficiency during these stages of gestation for vitamins A (<0.7 µmol/L), B 12 (<110 pmol/L), and D (<25 nmol/L) were 11.4%, 18.6%, and 27.9% and 51%, 78.6% and 69%, respectively. 6,7 Nearly 18% of mothers were deficient in vitamin E (<11.6 µmol/L) in the first trimester, while the apparent prevalence was far lower (3.3%) later in pregnancy, seen elsewhere and attributed to a rise in low-density lipoproteins that transport α-tocopherol during pregnancy. 19
Prevalence of Micronutrient Deficiencies Among Pregnant Women Assessed in the Palestinian Micronutrient Survey 2013, 7 the Gaza Strip (N = 583).
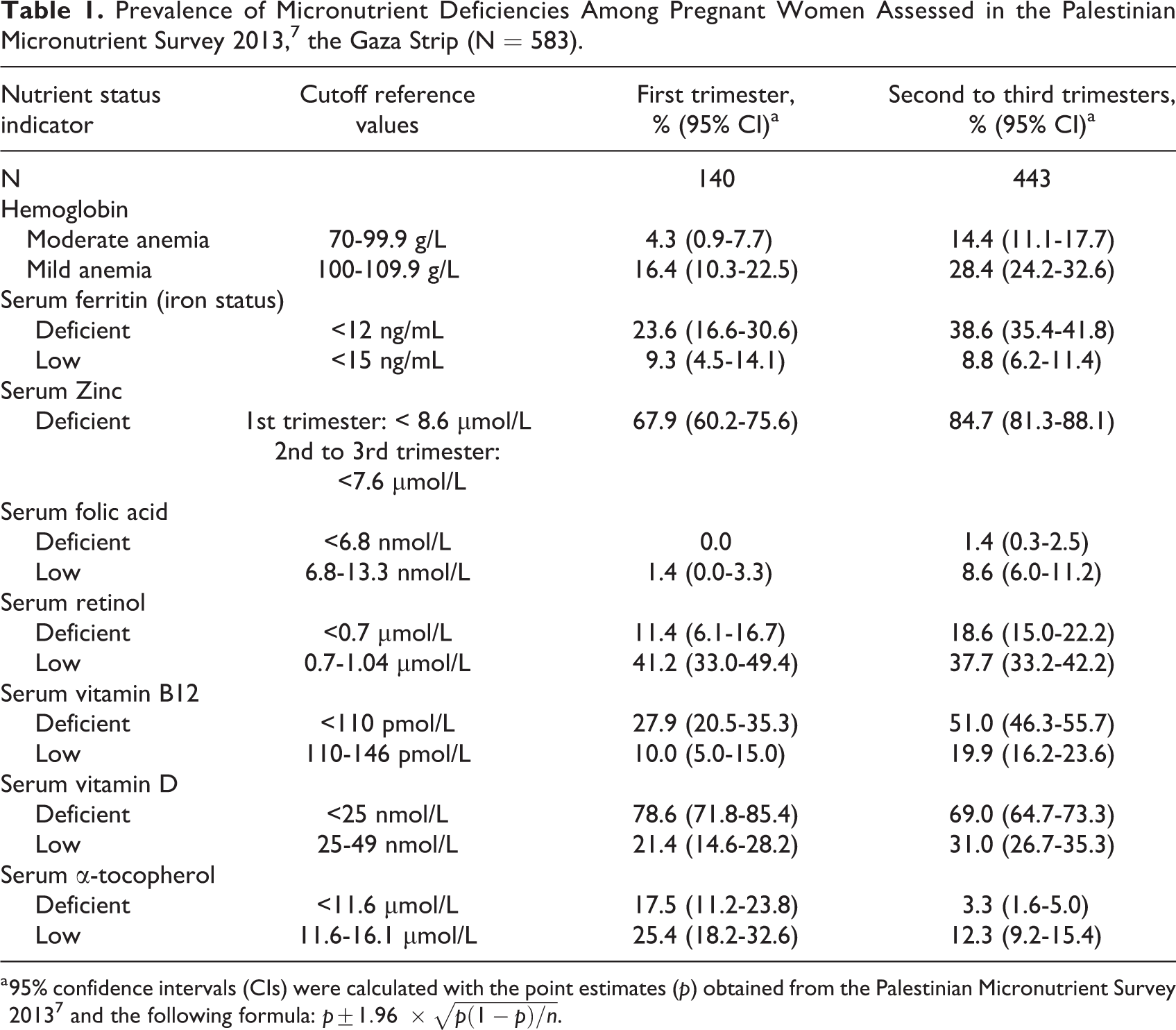
a 95% confidence intervals (CIs) were calculated with the point estimates (p) obtained from the Palestinian Micronutrient Survey 2013
7
and the following formula:
The prevalence of iron deficiency (serum ferritin <12 ng/mL) among children aged 6 to 59 months in 2013 was 19% (Table 2), 7 with anemia (hemoglobin <110 g/L) affecting 30.7%. Seventy-one percent of young children were found deficient in zinc (<9.9 µmol/L). As with mothers, few children were also low-to-deficient in folate (∼2%). While surprisingly, few (∼3%) were deficient in vitamin D (<25 nmol/L) and 62.5% were low in vitamin D status. Other nutrient deficiencies were common: 35.3% and 37.1% and 32.5% and 33.1% of children were deficient and low, respectively, in vitamins A (<0.7 µmol/L) and E (<11.6 µmol/L) status. 6,7,18
Prevalence of Micronutrient Deficiencies Among Children 6 to 59 Months of Age Assessed During the Palestinian Micronutrient Survey 2013 7 , the Gaza Strip (N = 582).
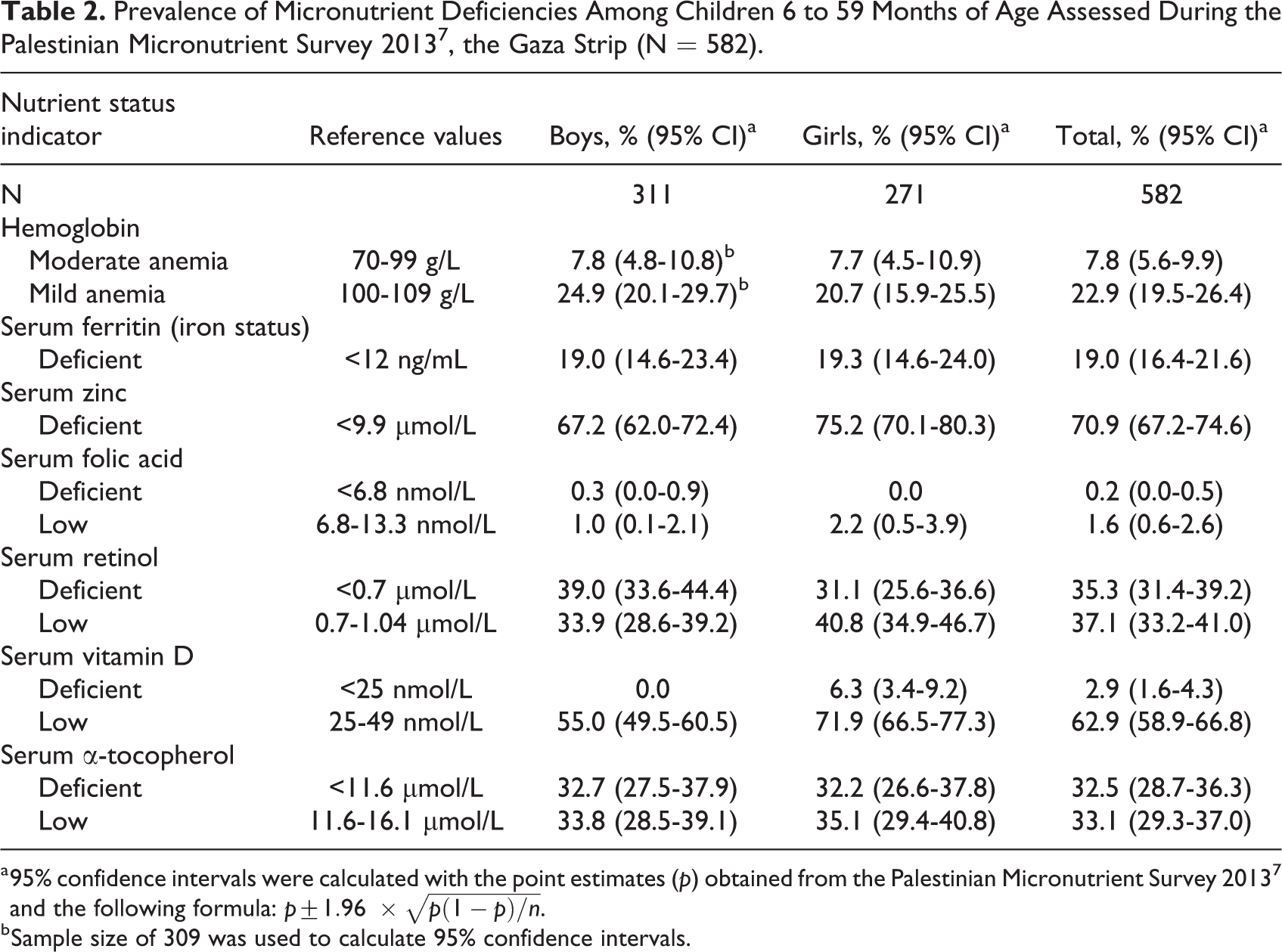
a 95% confidence intervals were calculated with the point estimates (p) obtained from the Palestinian Micronutrient Survey 2013
7
and the following formula:
b Sample size of 309 was used to calculate 95% confidence intervals.
While this commentary focuses on nutritional burdens in the Gaza Strip, where deficiencies were highest, the 2013 Palestinian Micronutrient Survey nonetheless reported comparable magnitudes of deficiency for vitamins B12, A, D, and E in the West Bank.
7
Serum β-carotene, a biomarker for carotenoid-containing vegetables and fruits, was reported to be markedly low (<0.373 µmol/L) in
Discussions
Data from the most recent Palestinian Micronutrient Survey of women and preschool-aged children in 2013 revealed a widespread burden of MNDs in the Gaza Strip. 6,7,18 Among the Palestinian diaspora, anemia and deficiencies in iron, zinc, vitamins A, B 12 , and E coexist and are prevalent among both pregnant women and preschool-aged children, in addition to the high burden of vitamin D deficiency among pregnant women. Anemia and iron deficiencies affected more than one-fifth of pregnant women in the first trimester with the conditions raising to ∼40% in the second to third trimesters. More than half of the pregnant women were low or deficient in vitamins A and B 12 , and nearly all the pregnant women included in the survey were either low or deficient in vitamin D. Approximately one-fifth of the pregnant women were vitamin E deficient in the first trimester. More than one-third of preschool-aged children were anemic, which coexists with ∼20% of iron deficiency, vitamins A and E deficient, and more than 70% of them presented with zinc deficient. It is unlikely that the micronutrient status of the population in the Gaza Strip has improved since this survey and may have worsened, given the area’s sustained socioeconomic, civil, and food system disruptions. While more recent population data are not available, this concern finds support in UNRWA antenatal and child clinic data from 2019, 2 revealing anemia (hemoglobin < 110 g/L) affecting 32% of pregnant women at the time of registration and 71% by the 24th week of gestation and 77% of infants at ∼12 months of age. 2
Complex political and social conditions are likely to underlie nutritional deficiencies in the Gaza Strip. These include a sea, land, and air blockade that has been imposed since 2007, in addition to conflict and civil unrest, which have limited local access to resources. These constraints have curtailed growth in local agricultural, manufacturing, and livestock sectors, which historically have been the backbone of the local economy. 8 Global concerns expressed by the World Bank of increased malnutrition as a consequence of the coronavirus pandemic 20 are also relevant to institutionally and socially fragile contexts of the Gaza and West Bank territories. 21
Two demographic groups in Palestinian refugee settings at highest risk of MNDs are pregnant women and young children, groups for which improved, evidence-based, preventive options exist. For pregnant women, antenatal IFA can now be replaced with multiple micronutrient supplements (MMS). 22 -24 Many MMS trials, conducted in settings with nutritional risk profiles similar to Palestinian camp realities, have revealed comparable effects on anemia as obtainable with IFA supplementation, with additional effects of reducing risks of low birthweight (risk ratio [RR]: 0.88, 95% confidence interval [CI]: 0.85-0.91), currently affecting 8.3% of newborns in the Gaza Strip, 25 small-for-gestational age birth (RR: 0.92, 95% CI: 0.88-0.97) 22 and possibly benefiting early childhood cognition. 26 Thus, while promoting access to a diverse, nutritious diet and advancing food fortification 27 remain fundamental public health goals in Gaza and other UNRWA fields of operation, substitution of daily IFA with MMS via antenatal care offers a low-risk approach to meeting nutrient requirements of pregnancy 28 and can prevent gestational MNDs, which may benefit health of mothers and their offspring. According to the most recent WHO guideline, published in August 2020, MMS is now “recommended in the context of rigorous research,” where in countries considering a programmatic switch from IFA to MMS, this refers to evaluating the impact of MMS on acceptability, feasibility, sustainability, equity, and cost-effectivenss, 29 sine qua non aims of implementation research. While initiating MMS early in pregnancy has been shown to be equivalent to IFA in preventing iron deficiency anemia, 30 routine MMS should not preclude the use of therapeutic iron for treating anemia, as required.
For preventing MNDs in children beyond 6 months of age, multiple micronutrient powders (MNPs) offer a low-cost product, suitable for primary care use, which can raise micronutrient intakes by mixing into any semi-solid food. 31,32 Studies in children aged 6 to 23 months have shown MNPs to reduce risk of anemia by 18% (0.82, 95% CI: 0.76-0.90) and iron deficiency by 53% (RR: 0.47, 95% CI: 0.39-0.56) without adverse effects. 31 Among older preschoolers (24-59 months of age), overviews of trials have shown point-of-use MNP fortification of meals to increase hemoglobin levels (by 3.37 g/L; 95% CI: 0.94-5.80), sufficient to lower the prevalence ratio (PR) of anemia (PR = 0.66; 95% CI: 0.49-0.88) and iron deficiency (PR = 0.35, 95% CI: 0.27-0.47) compared to a placebo or no intervention. 32 In the Gaza Strip, with further investments, preschoolers could be provided with MNP as part of UNRWA’s primary care services. In addition to the present coronavirus disease pandemic potentially increasing nutritional and health risks, many countries are also experiencing disruptions in their food systems, health care services and social and food assistance programs, thus further raising barriers to accessing a nutritious diet during pregnancy or by households of low socioeconomic status. In the Gaza Strip, where food insecurity, poverty, and MNDs coexist and are prevalent, widespread receipt of MMS could be expected to help women meet increased gestational micronutrient requirements.
Conclusions
Given the evidence of MNDs and the potential health consequences they pose among women and children, it would appear justifiable to more closely monitor dietary quality, food security, and extent of deficiencies, as well as the adequacy of coverage and adherence to existing supplementation and fortification programs, while considering MMS and MNP for pregnant women and young children, respectively, in the Gaza Strip and other Palestinian communities encompassing UNRWA fields of operation in the Middle East.
Footnotes
Authors’ Note
The views expressed herein are those of the authors and do not necessarily reflect the views of the UNRWA, Ministry of Health in the State of Palestine, or the supporting organizations.
Acknowledgments
The authors would like to thank Dr Majed Hababeh for sharing his expertise on maternal child health and historical knowledge of UNRWA and Palestine refugees in the Middle East. The first author gratefully acknowledges the Ministry of Foreign Affairs of Japan, the Harry D. Kruse Publication Award in Human Nutrition, and support from the Sight and Life Global Nutrition Research Institute, Baltimore, MD.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.