
Abstract
Objective:
To identify predictors of maternal dietary diversity in rural Dodoma, Tanzania and assess its association with child growth outcomes.
Methods:
A cross-sectional survey of 361 mothers with children under 24 months of age was conducted in 5 villages in rural Dodoma, Tanzania. Maternal diets were assessed using food frequency questionnaires, and dietary diversity was categorized using Minimum Dietary Diversity for Women (MDD-W) guidelines. Child anthropometric measures were taken to calculate height-for-age z-score (HAZ), weight-for-height z-score (WHZ), and weight-for-age z-score (WAZ). Linear and logistic regressions were used to examine the association between maternal dietary diversity and children’s growth outcomes.
Results:
About 40% of mothers did not consume a diverse diet (MDD-W < 5), and 35% of children were stunted. Household production of greater number of crops was associated with greater MDD-W scores (P < .01). Greater maternal dietary diversity was associated with significantly greater child WHZ (mean difference = 0.44; 95% confidence interval [CI]: 0.10-0.78; P = .01), WAZ (mean difference = 0.37; 95% CI: 0.08-0.65; P = .01), and reduced risk of wasting (odds ratio = 0.22; 95% CI: 0.07-0.66; P = .01).
Conclusions:
Greater maternal dietary diversity was associated with improved child WHZ and WAZ outcomes. Sustainable interventions to increase maternal dietary diversity may improve WHZ and WAZ in young children in similar settings.
Introduction
Over the past 20 years, there have been dramatic declines in global child mortality; however, the rate of decline for child undernutrition has significantly lagged. In sub-Saharan Africa, there has been little to no change in stunting prevalence—from 40% in 1990 to 38% in 2010 1 —and today African malnourished children make up over one-third of all malnourished children under 5 worldwide. 2 Malnutrition and subsequent suboptimal growth puts children at increased risk of mortality 3,4 and was estimated to contribute to about one-third of remaining child deaths in 2011. 5 Childhood malnutrition may also have negative consequences on cognitive and motor development later in life 6 ; malnourished children complete fewer grades of schooling, 7 exhibit poorer intellectual performance, demonstrate lower work capacity, 8 and earn lower salaries 9 compared to their nonmalnourished peers.
A child’s nutritional status is inextricably linked to his/her mother’s nutrition from pregnancy through the postpartum period. A mother’s food intake and nutritional status during pregnancy have implications for birth outcomes and a child’s nutritional status later in life. 10,11 Additionally, nutrients from the mother’s breast milk are passed on to the infant during breastfeeding. Breast milk contains vital nutrients and antibodies that improve infant survival and aid in growth and development. Breastfeeding provides not only short-term benefits to infant health—reduced mortality to infectious disease: diarrhea, ear infections, lower respiratory infections, leukemia 12,13 —but also long-term benefits later in life—better performance on intelligence tests during childhood and adolescence, decreased risk of overweight/obesity and type 2 diabetes, lower mean diastolic blood pressure, and lower mean systolic blood pressure. 14
Dietary diversity is measured using the dietary diversity score (DDS) or a simple count of food groups that an individual consumed during the referent period. Dietary diversity score has been validated as a proxy measure for micronutrient intake in infants, children, and adults.
15
–17
Specifically, the Minimum Dietary Diversity for Women (MDD-W) was developed as a proxy indicator to reflect micronutrient adequacy of women’s diets at the population level. Although targeting a child’s food intake can be an effective method for combating childhood malnutrition, a child’s growth outcomes may be determined long before the child is born or can make his/her own food choices. Children in sub-Saharan Africa have been shown to be particularly vulnerable to micronutrient deficiency due to diets consisting mostly of staple grains and starchy foods, little to no animal products, and few fruits and vegetables.
18
Given a mother’s significant influence on her child’s nutritional status, increasing mother’s dietary diversity may improve child micronutrient and nutritional status. This study will address 2 main research questions: What percentage of mothers consume a diverse diet as defined by Food and Agriculture Organization (FAO), and what are the predictors of maternal dietary diversity in rural Tanzania? Is there an association between mother’s dietary diversity and child growth outcomes in children under 24 months?
Methods
Study Design and Population
The cross-sectional study was conducted among mothers with children under 2 years of age in Chamwino District located in the Dodoma Region of central Tanzania. Dodoma is semiarid with 1 rainy season from November to April. Most inhabitants raise livestock or grow crops, primarily millet, sorghum, maize, and groundnuts. 19,20 This study was nested within the Dodoma Household Demographic Surveillance System (HDSS) launched in 2016 which is a longitudinal data collection system for health and demographic information. Nutrition data were collected in the middle of the rainy season from December 2016 to January 2017 in 2 wards (Mlowa Barabarani and Makang’wa) with 5 villages (Mloda, Chiwona, Mlowa Barabarani, Mlowa B, and Makang’wa). Women were eligible for the study if they were of reproductive age (15-49 years of age) and were responsible for infant feeding. Of the 12 263 women of reproductive age included in the HDSS, 1214 women had children under the age of 2. A minimum sample size of 321 was calculated from the Cochran formula, and with an expected response rate of 70%, 459 of these women were randomly selected to participate in the nutrition survey. About 76% of mothers responded, and the final sample size was 361 mother–child pairs. In a post hoc power analysis, assuming a 2-sided test with an α of .05, we had 80% power to detect an effect size of 0.30 z-scores for the continuous height-for-age z-score (HAZ), weight-for-age z-score (WAZ), and weight-for-height z-score (WHZ) outcomes. As a result, we had adequate power to detect relatively large effect sizes.
Data Collected
Food frequency questionnaire
A food frequency questionnaire (FFQ) with 88 food items was adapted from a previous dietary study in Rufiji, Tanzania. 21 Mothers were asked about the consumption of foods over the last month on a frequency scale from 1 (never) to 9 (6+ times per day). Maternal DDS was constructed from the FFQ. Mothers were asked for their frequency of consumption of 88 context-specific food items. Food groups were not given to reduce reporting bias of mothers responding positively to food groups learned at antenatal care or well-baby visits. Per the MDD-W guidelines, foods were classified into 10 food groups 22 : (1) grains, white roots and tubers, and plantains; (2) pulses (beans, peas, and lentils); (3) nuts and seeds; (4) dairy; (5) meat, poultry, and fish; (6) eggs; (7) dark green leafy vegetables; (8) other vitamin A-rich fruits and vegetables; (9) other vegetables; and (10) other fruits. For each food group, if mothers had consumed any food item in the group at least 2 times per week, they were marked as having consumed from that food group. The DDS was calculated by summing up the number of food groups consumed. Mothers’ diets were considered diverse if they consumed from at least 5 food groups of 10. 22
Nutritional anthropometry
Anthropometric measures were taken for all children in the study. Date of birth was recorded from birth registration cards where possible, and age of the child was calculated by subtracting birth date from the survey date. It is possible that misclassification by days or weeks may occur on birth registration cards, but this would have minimal impact on HAZ and WAZ calculations. The low rate of homebirth and high rates of 6-week vaccination attendance lead to relative accuracy. A Seca digital weighing scale was used to weigh children to the nearest 0.1 kg. Children’s heights were recorded using a stadiometer, having them stand straight up against a wall with heels touching the wall and eyes looking forward. A research assistant held a flat board against the top of the child’s head and used a tape measure to measure the height from the ground to the board. For young children who could not stand, infant length was measured by laying the infant on a flat board and measuring from the top of the head to the end of outstretched legs to the nearest 0.1 cm.
Likely predictors of maternal dietary diversity were drawn from the underlying and immediate causes of maternal and child malnutrition framework developed by UNICEF and modified based on the availability of data from the HDSS. 23 These included mother’s age, maternal education, wealth quartile, and household size.
Home food production
To assess agricultural diversity, participants were asked whether they grew, stored, and/or sold various crop groups during the previous growing season.
Food security
Questions about food security were adapted from the FAO Household Food Insecurity Access Scale questionnaire. 24 Participants were also asked to indicate their primary source for obtaining different food groups: own production, purchased, borrowed, or another source.
Water, sanitation, and hygiene
The water, sanitation, and hygiene (WASH) questionnaire was adapted from the World Health Organization (WHO) Core Questions on Drinking Water and Sanitation for Household Survey 25 and the UNHCR WASH Standardized Expanded Nutrition Survey. 26 Questions asked about the aspects of drinking water (source, method for obtaining, quality, satisfaction with source), toilet facilities (type, private/public), and water storage (container form, size of container).
Statistical Analysis
Descriptive statistics were used to summarize demographic characteristics for all mothers and their children. There were 12 instances of mothers having more than 1 child under 24 months in which case both children were included. Mother’s dietary diversity was classified both as continuous and binary DDS ≥ 5 to indicate adequate diet diversity using the 10 food groups from the MDD-W. 22 Child growth status was calculated using height, weight, and age data from anthropometry. Z scores were calculated using the WHO AnthroPlus 2006 macro for Stata. Outcomes were classified as continuous HAZ, WHZ, and WAZ. Scores were also classified as binary per WHO standards: stunting was HAZ less than 2 standard deviations (SDs) below the median, wasting was WHZ less than 2 SDs below the median, and underweight was WAZ less than 2 SDs below the median. 27
Univariate and multivariate logistic and linear regression analyses were performed to identify significant predictors of mother’s dietary diversity. We also evaluated the relationships of continuous DDS and adequate diet diversity (DDS ≥ 5) with child anthropometric outcomes (HAZ, WAZ, WHZ) using linear and logistic regression, respectively. Covariates in multivariate models included mother’s age, maternal education, wealth quartile, food insecurity, household size, main source of drinking water, type of toilet facility, breastfeeding status of the child, child’s age, and child’s sex. Crop production type and number of crop groups produced were not included in the same models due to collinearity. All analyses were performed using Stata 13 (2013; StataCorp LP, College Station, Texas).
Ethical Considerations
The research protocol was approved by the institutional review boards of Harvard T.H. Chan School of Public Health (IRB15-1899), University of Dodoma (UDOM) (UDOM/DRP/VOL II/32), and National Institute of Medical Research (NIMR) (NIMR/HQ/R.8a/Vol.1x/2319). Village consent was obtained prior to entry into the study area. The study was communicated to Dodoma Regional Health Management Team, the Chamwino District Council, the village elders, and the community members for approval. Written informed consent was obtained from mothers for their and their child’s participation before administration of the nutrition survey.
Results
Study Population
Characteristics of 361 mothers and their children are presented in Table 1. About 97% of mothers had a singleton child under 24 months, 9 had twins under 24 months, and 3 had 2 siblings under 24 months. The median household size was 5, indicating that these were mainly single-family households. About 78% of households had a male head of household. About one-third of households (36%) owned 1 to 2 acres of land used for agricultural purposes, most households did not own livestock (52%), and about 16% owned chickens/other poultry and no other animals. Cereals (95%) and legumes (70%) were the most commonly produced crops. About 70% of households were severely food insecure, 85% had an improved source of drinking water, and 15% had an improved toilet facility (Table 1). Mothers consumed from an average of 5 of 10 food groups (median = 5, SD = 1.12, interquartile range [IQR] = 1; Figure 1). About 40% of women did not meet minimum diet diversity requirements.
Demographic Characteristics.
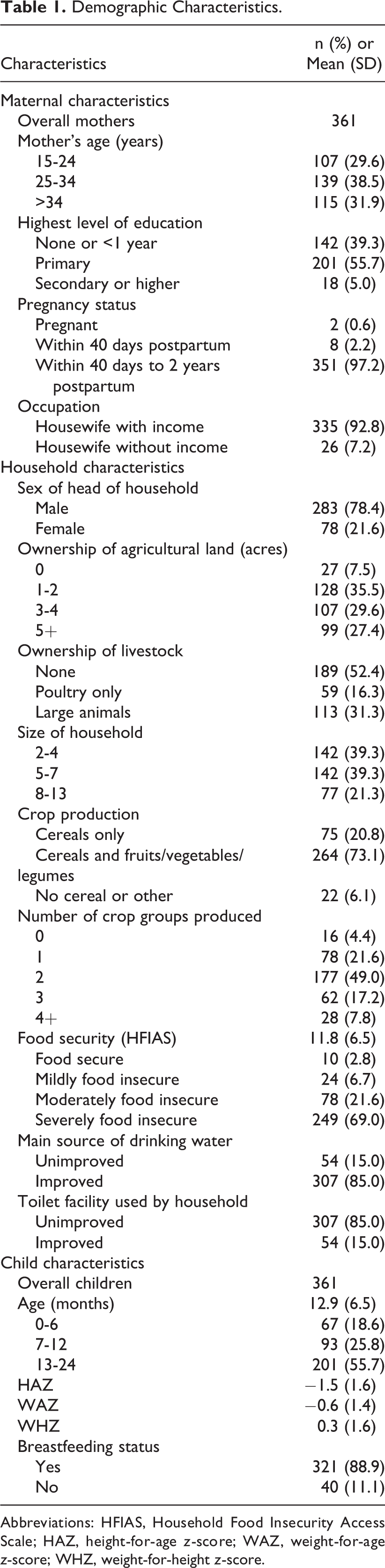
Abbreviations: HFIAS, Household Food Insecurity Access Scale; HAZ, height-for-age z-score; WAZ, weight-for-age z-score; WHZ, weight-for-height z-score.
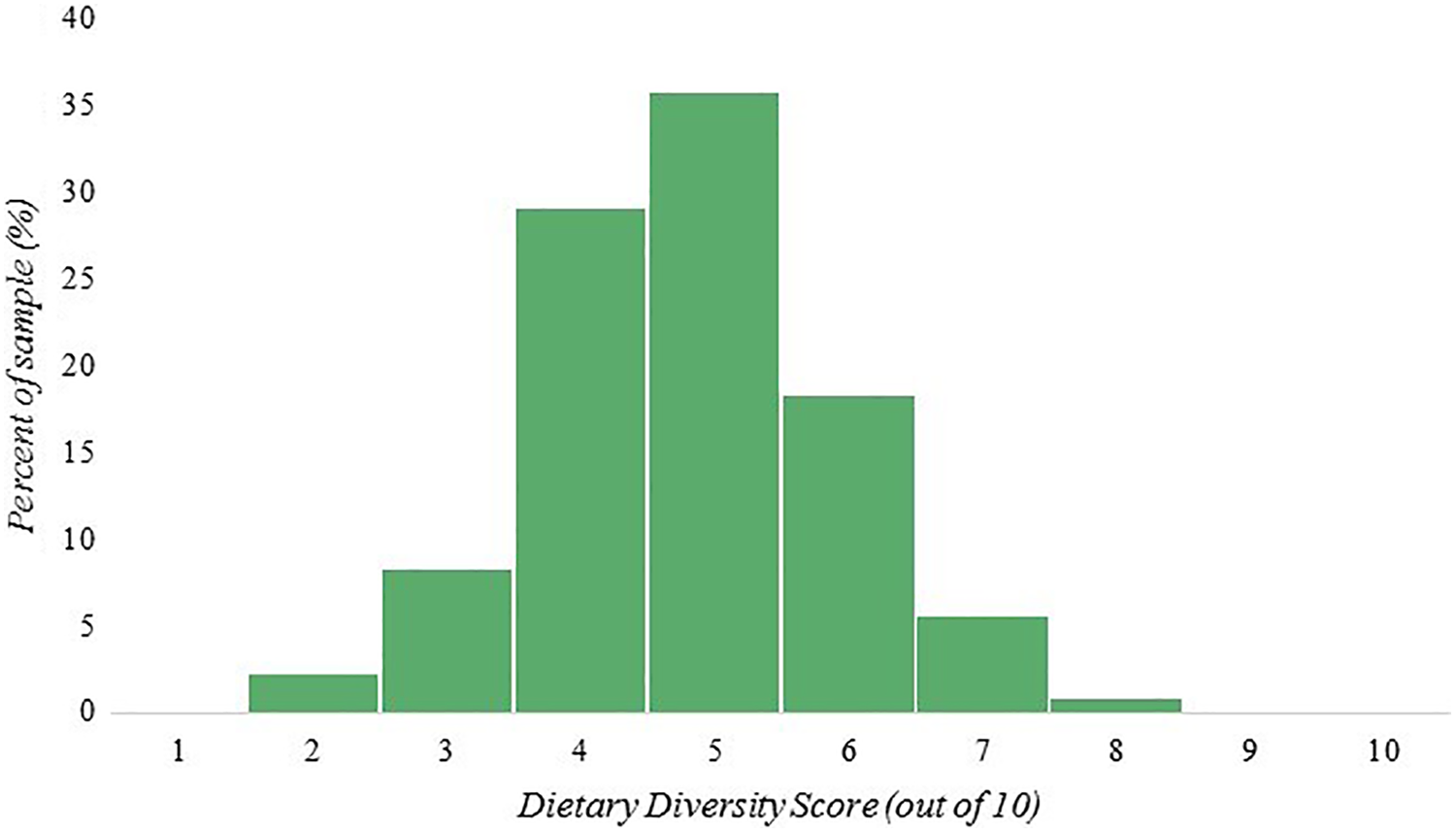
Distribution of maternal dietary diversity scores of 10 food groups in 361 mothers in rural Dodoma, Tanzania.
There were 361 children under the age of 24 months included in the study. A little over half were between 13 and 24 months old (56%), and most were breastfeeding at the time of the survey (89%). The prevalence of stunting was 35%, while wasting was 6%.
Predictors of Women’s Dietary Diversity
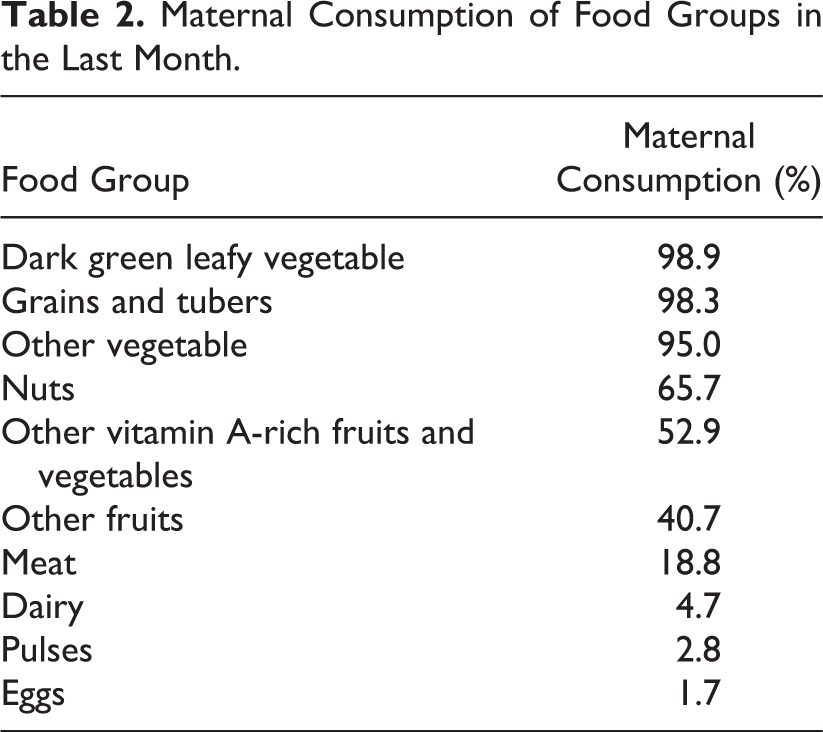
The percentage of mothers consuming from each of 10 food groups in the last month is presented in Table 2. The greatest percentage of mothers consumed from the dark green leafy vegetables (99%) and grains and tubers food groups (93%), and the lowest percentage consumed from eggs (2%) and pulses (3%). Predictors of continuous (1-10) and meeting minimum diet diversity (DDS < 5, DDS ≥ 5) are presented in Table 3. When assessed continuously, maternal dietary diversity was positively associated with households growing cereals along with fruits, vegetables, or legumes (mean difference in MDD-W score = 0.37; 95% confidence interval [CI] = 0.07-0.67; P = .02) and growing a greater number of crop groups (P trend < .01). It was also negatively associated with ownership of poultry only compared to ownership of no livestock (mean difference = −0.36; 95% CI = −0.70 to −0.02; P = .04) in multivariate models. When maternal dietary diversity was classified as binary DDS ≥ 5 to indicate meeting adequate diet diversity, it was positively associated with growing a greater number of crop groups (P trend < .01) and having a female head of household (odds ratio [OR] = 2.06; 95% CI = 1.07-3.96; P = .03). It was negatively associated with ownership of poultry only compared to ownership of no livestock (OR = 0.36; 95% CI = 0.18-0.72; P < .01). Additionally, mothers older than 34 years of age had reduced odds of consuming from at least 5 food groups compared to mothers 15 to 24 years of age (OR = 0.42; 95% CI = 0.20-0.90; P = .03).
Maternal Consumption of Food Groups in the Last Month.
Predictors of Women’s Dietary Diversity Among 361 Households in Rural Dodoma, Tanzania.
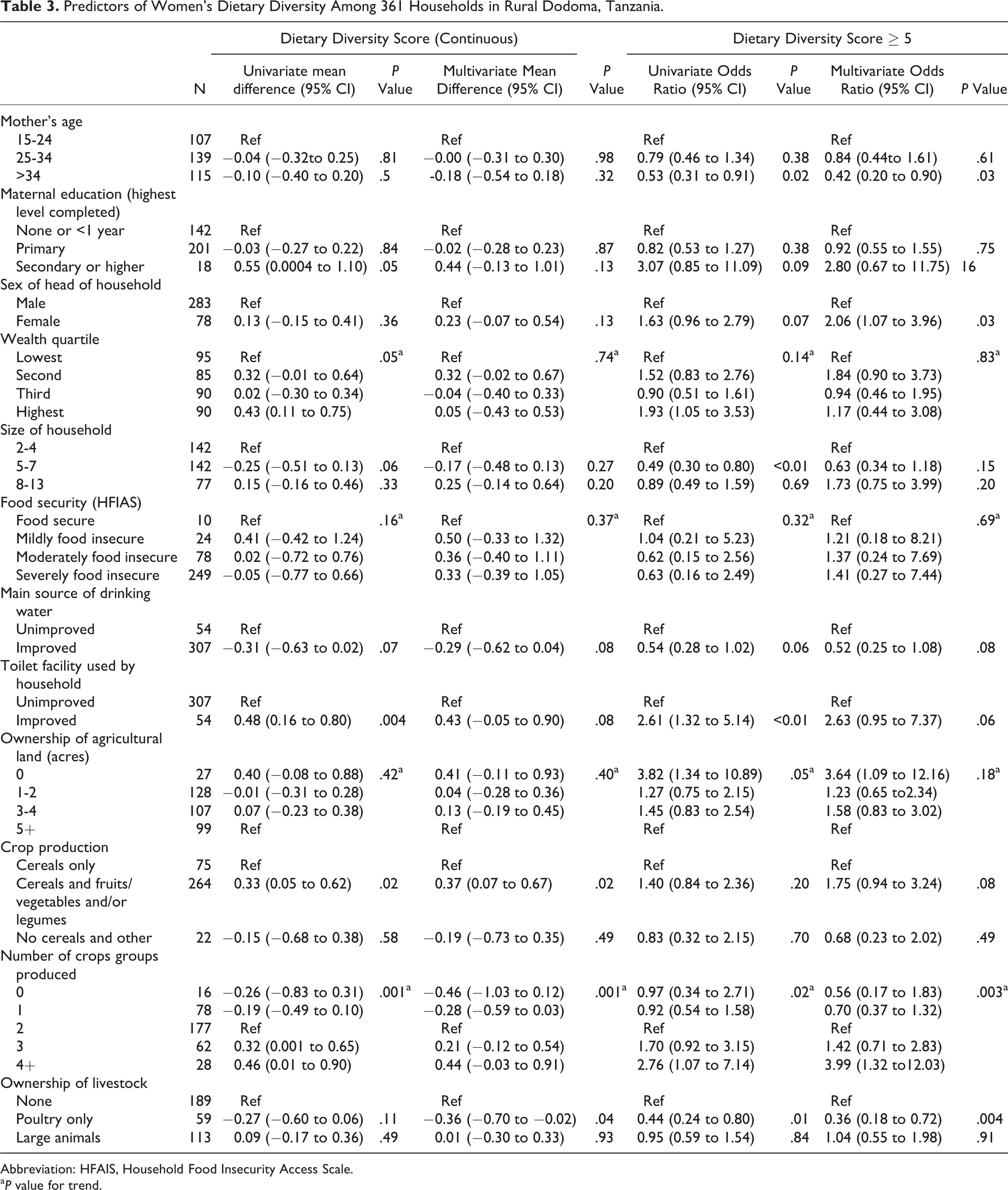
Abbreviation: HFAIS, Household Food Insecurity Access Scale.
a P value for trend.
Association Between Women’s Dietary Diversity and Children’s Anthropometric Measures
Results from univariate and multivariate analyses of maternal dietary diversity and growth outcomes in children less than 2 years are presented in Table 4. Diverse maternal diets (DDS ≥ 5) were significantly associated with greater WHZ (mean difference = 0.44; 95% CI = 0.10-0.78; P = .01), greater WAZ (mean difference = 0.37; 95% CI = 0.08, 0.65; P = .01), and reduced odds of wasting (OR = 0.22; 95% CI = 0.07-0.66; P = .01) after multivariate adjustment.
Association Between Maternal Dietary Diversity Score (DDS) With Continuous Child Growth Outcomes.
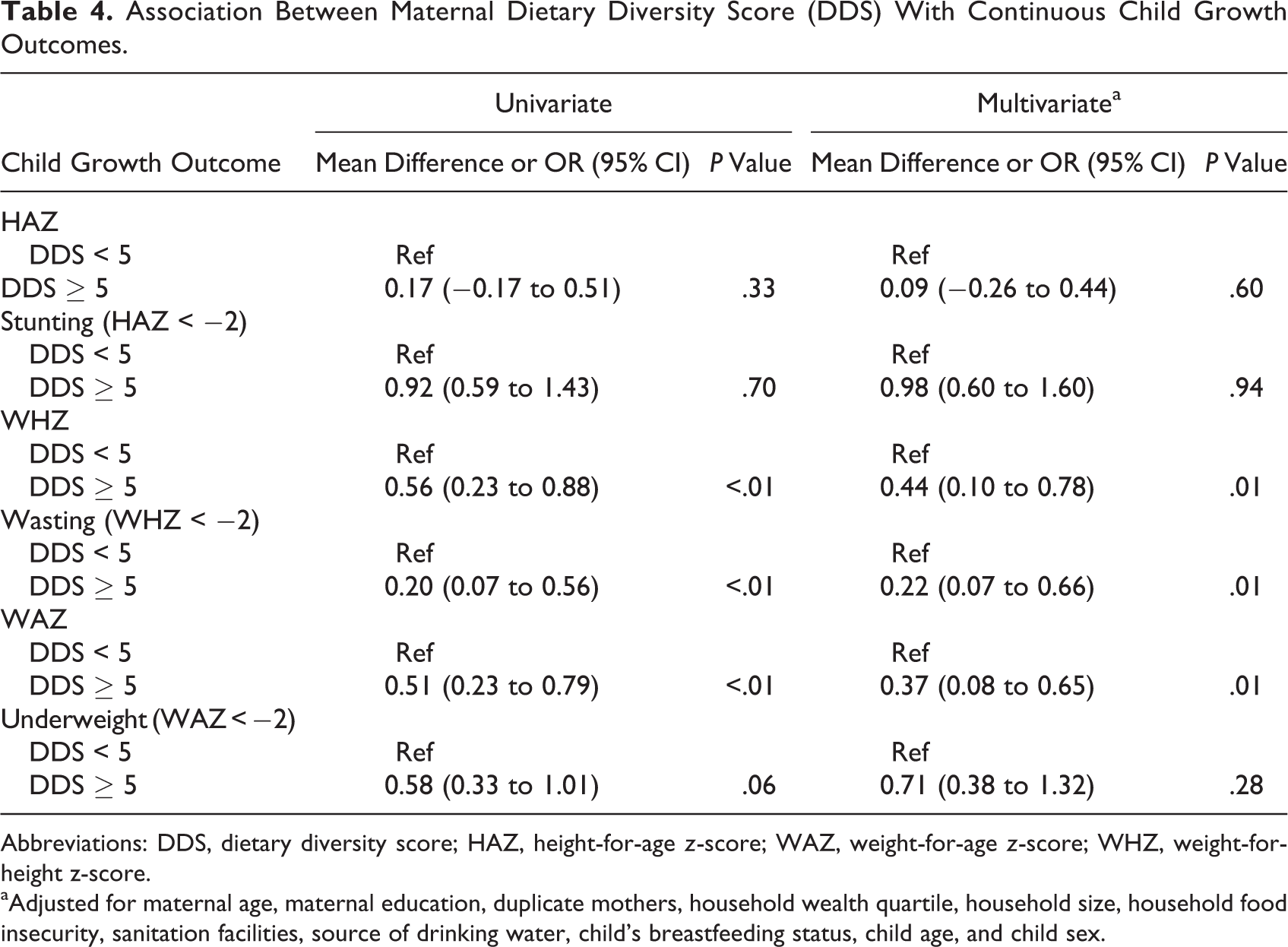
Abbreviations: DDS, dietary diversity score; HAZ, height-for-age z-score; WAZ, weight-for-age z-score; WHZ, weight-for-height z-score.
aAdjusted for maternal age, maternal education, duplicate mothers, household wealth quartile, household size, household food insecurity, sanitation facilities, source of drinking water, child’s breastfeeding status, child age, and child sex.
Discussion
This study aimed to identify the predictors of maternal dietary diversity among mothers in rural Dodoma, Tanzania and assess the association between maternal dietary diversity and child growth outcomes in children under 24 months of age. The analysis found that mothers who were over 34 years of age compared to 15 to 24 years of age or owned only poultry compared to no livestock were less likely to consume a diverse diet (DDS ≥ 5). Mothers were more likely to consume a diverse diet when they came from a household with a female head and grew a greater number of crop groups. We also determined that children whose mothers consumed from at least 5 food groups had greater WAZ and WHZ and reduced prevalence of wasting as compared to children whose mothers ate a less diverse diet.
Our findings are similar to prior studies that primarily focused on household dietary diversity as opposed to mother’s dietary diversity as assessed in this study. A study also conducted in rural Dodoma, Tanzania found that large cultivated land size, increased literacy status of the mother, and reduced distance to a water source were significant predictors of high household dietary diversity. 27 Two other studies conducted in Ethiopia and South Africa determined that higher socioeconomic status, urban residence, higher literacy of the head of household, greater household size, owning livestock, having an irrigation scheme, and having access to a home garden were predictors of high household dietary diversity. 17,28
In our study, mothers whose households produced a greater number of crop groups and grew cereals and at least 1 other nutritious food group (fruits, vegetables, legumes) appeared to incorporate these foods into their own diverse diets. Additionally, mothers who came from households with a female head of household tended to consume a more diverse diet. This finding aligns with studies showing a positive association between women’s participation in household decision-making and higher DDS. 29,30 Although some female-headed households may have greater food insecurity than male-headed households, they may put greater emphasis on diet variety. Mothers who resided in households that owned only poultry were less likely to consume diverse diets compared to mothers who owned no animals, suggesting that households mostly sell eggs in this context and therefore do not reap the nutritional benefits from poultry ownership. We see this in Table 2 that ∼1% of women reported eating eggs, despite a large proportion of poultry ownership. Finally, mothers who were older than 34 years of age were less likely to consume a diverse diet compared to those 15 to 24 years of age. This may be due to residual confounding by parity and household size.
We determined that increased maternal dietary diversity was associated with reduced risk of wasting and increased WAZ and WHZ in children under 24 months of age. Similarly, prior studies have indicated increased household and children’s dietary diversity are associated with improved child growth outcomes in Nepal, 31 Indonesia, 32 Bangladesh 33 , and others. 34 Maternal dietary diversity has been shown to be positively associated with child dietary diversity. 35 Greater dietary diversity may indicate that households rely on a diverse set of agricultural products or have greater access to a variety of foods from the market, both of which allow their children to reap the nutritional benefits as well. As WHZ and wasting are both indicators of acute malnutrition, children whose mothers consume a diverse diet may be less vulnerable to short periods of food inadequacy from effects of seasonality or spikes in food prices. Evidence suggests that the cumulative effects of inadequate calorie and nutrient intake on stunting peak in children aged 18 to 23 months. 36 In the present study, there was no significant relationship between maternal dietary diversity and stunted growth.
The study has a few limitations. The cross-sectional design of this study does not allow for causal effects to be established. The study also captures dietary diversity during the rainy season and may not reflect dietary patterns during other periods. In addition, although we have adjusted for socioeconomic status and numerous other factors, residual and unmeasured confounding by parity, distance to health center, and other factors are possible. The sample size of 361 mothers only allowed us to detect moderate to large effects of dietary diversity on child growth outcomes, and larger studies are needed to detect smaller effects. Furthermore, the target population (women aged 15-49 with children under 24 months) may not be generalizable to their children, and our sample size was limited to examine the associations with nutritional status in the second year of life. However, there are several notable strengths. The nutrition survey administered provided a broad picture of dietary diversity and malnutrition asking questions about breastfeeding, complementary feeding, home food production, food security, and WASH. Additionally, the DDS was calculated from an FFQ that asked about intake in the past month which produced a more long-term summary of food consumption. Investigating mother’s dietary diversity as opposed to household dietary diversity was also advantageous in producing more accurate data on mothers’ consumption, as household dietary diversity examined in prior studies may not reflect maternal consumption given intra-household distribution of food may be directed to other family members. Additionally, targeting mother’s dietary diversity allows for earlier interventions on child growth that precede the birth of the child.
Conclusion
These observational data suggest that a maternal diverse diet may increase child WAZ and WHZ. The MDD-W score could be further developed to allow for comparisons across seasons and acro-ecological settings. Although associations were found between mother’s dietary diversity and child WAZ and WHZ in this study, interventions and clinical trials are needed to determine causal effects of promoting a diverse diet in mothers. Results from this study may be applicable to other African countries where diets are similarly starchy and nondiverse, 37 although there are context-specific factors that should be considered.
Footnotes
Acknowledgments
The authors would like to thank James Charles, Dodoma Regional Medical Officer, and Abdallah Noor and Chelsey Canavan from Harvard T.H. Chan School of Public Health for their guidance throughout the study. The authors would also like to thank the research team at the University of Dodoma: Augustine Malero for providing technical support and the research assistants for survey implementation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.