
Abstract
Despite increased political attention, foodborne diseases still cause a substantial public health, economic, and social burden worldwide. Children younger than 5 years, people living in developing regions, and in the poorest areas of the world are disproportionally affected, bearing a large proportion of the global burden of foodborne disease. Yet, food safety is a prerequisite to ensuring food security globally: Foods that are responsible for important food safety problems are also crucial to ensure food security in some regions and are essential sources of nutrition. Moreover, together with calls for action to meeting international sustainable development goals, global efforts to promote food security and healthy diets have now highlighted the need to modify food systems globally. This article therefore explores the food safety dimensions of transitions toward food systems that promote sustainable healthy diets. The current body of evidence points to the combined health and environmental benefits of shifting toward a more plant-based diet, including vegetables and fruits, nuts, pulses, and whole grains. As a shift toward more plant-based diets may also lead to higher exposures to chemicals or pathogens present in these foods, an evaluation of food safety implications of such transitions is now imperative. We conclude that several synergies between public health, environmental, and food safety strategies can be identified to support dietary transitions.
Introduction
Food safety is a prerequisite to ensuring food security globally. Access to safe and healthy foods is essential for achieving several of the Sustainable Development Goals for promoting health and well-being, socioeconomic development, and the declining of inequalities worldwide. 1
Despite increased political attention, foodborne diseases (FBDs) still cause a substantial public health, economic and social burden worldwide, and particularly in low- and middle-income countries (LMICs). While food safety concerns have been high on the political agenda in some high-income countries, inadequate attention and underinvestment have stunted the implementation of food safety systems in LMICs. 2 These countries are also disproportionally affected due to poorer production processes and food handling, sanitation and water safety, access to storage infrastructure, and climate impact on the proliferation of pests and naturally occurring toxins. 3
Reducing the burden of FBD depends upon informed policy-making and effective intervention strategies that are focused on the most important food safety problems. This process is challenging in several ways. First, FBD can be caused by a variety of hazards, from microbial agents to chemical contaminants and toxins. Second, only a fraction of those who fall ill from contaminated food seek care, are treated, and reported to public health authorities; the large majority of acute cases of, for example, gastroenteritis go undiagnosed, and several foodborne hazards lead to chronic diseases (such as cancer) that appear a long time after exposure, which makes it impossible to directly associate illnesses with the consumption of foods. Third, foodborne hazards are most commonly transmitted through contaminated foods, but exposure through other pathways, including drinking water, contact with animals, or other environmental routes may occur; the relative contribution of such pathways varies across the world and is linked to overall socioeconomic condition, access to safe water, adequate food storage infrastructure, and food production practices. Fourth, informing action depends on accurate data on the most important causes and sources of FBDs, which requires collecting, compiling, and analyzing data from public health, food, and animal surveillance. In many parts of the world, such surveillance systems and data are lacking.
Various calls for action to meeting international sustainable development targets have highlighted the need to modify food systems. While the goal is to move toward food systems that promote sustainable healthy diets, such transitions, along with effects of modifications of the global socioeconomic landscape and the increasing demand for food by a growing world population, may have implications in terms of food safety. This article explores the food safety dimensions of the topics discussed in the companion papers. First, it summarizes current knowledge on the global burden of FBD, discussing differences between regions and population groups. Next, it examines the potential impacts of current and predicted dietary transitions from a food safety angle to allow for holistically approaching the issue of sustainable healthy diets. The potential dilemmas associated with choices between safe, healthy, sustainable, affordable, and accessible food products are outlined and discussed. This review was conducted in the context of the International Expert Consultation on Sustainable and Healthy Diets organized by the Food and Agriculture Organization (FAO) and the World Health Organizations (WHO).
The Global Burden of Disease Due to Contaminated Foods
Foods can be contaminated by a wide range of hazards, known to cause more than 200 acute and chronic diseases. Foodborne hazards include microbiological agents such as bacteria, virus, fungi, or parasites, and chemical hazards that can originate from anthropogenic pollution, from processing or packaging of foods, or that occur as naturally occurring toxins in raw materials. The occurrence of FBD and their impact on societies may vary among regions, locally and globally. Measuring this impact is crucial to identify food safety problems and establish priorities at national, regional and global levels.
Global Burden of FBDs, 2010
To obtain a better insight in the global and regional burden of FBD, WHO established the Foodborne Disease Burden Epidemiology Reference Group (WHO-FERG) in 2007. 3 The WHO-FERG estimated that, in 2010, there were 600 million cases of foodborne illnesses and 420 000 deaths (note 1). 3 The 31 hazards resulted in the loss of 33 million years of healthy life globally, demonstrating that the global burden of FBD is of the same order of magnitude as major infectious diseases such as HIV/AIDS, malaria, and tuberculosis. 4 The burden is also comparable to that related to diet, unimproved water sources, or air pollution. 5 Still, these estimates are acknowledged to be an underestimation, mainly because the initiative was unable to estimate the disease burden of a more comprehensive list of foodborne hazards due to data limitations. In particular, the final list of hazards addressed included only 3 chemical contaminants, which unavoidably leads to a lack of knowledge on the true burden of exposure to harmful chemicals through foods.
The WHO-FERG’s estimates demonstrated inequalities in terms of public health impact of FBD. Children younger than 5 years bore 40% of the total global burden, but represent only 9% of the world population (Figure 1). People living in developing regions and in the poorest areas of the world were also disproportionally affected, bearing over 70% of the global burden. Africa and South-East Asia had the highest incidence and mortality of foodborne illnesses across all ages. At the other end of the spectrum, high-income countries within the European, American, and Western Pacific regions had the lowest burden of disease (Figure 1).
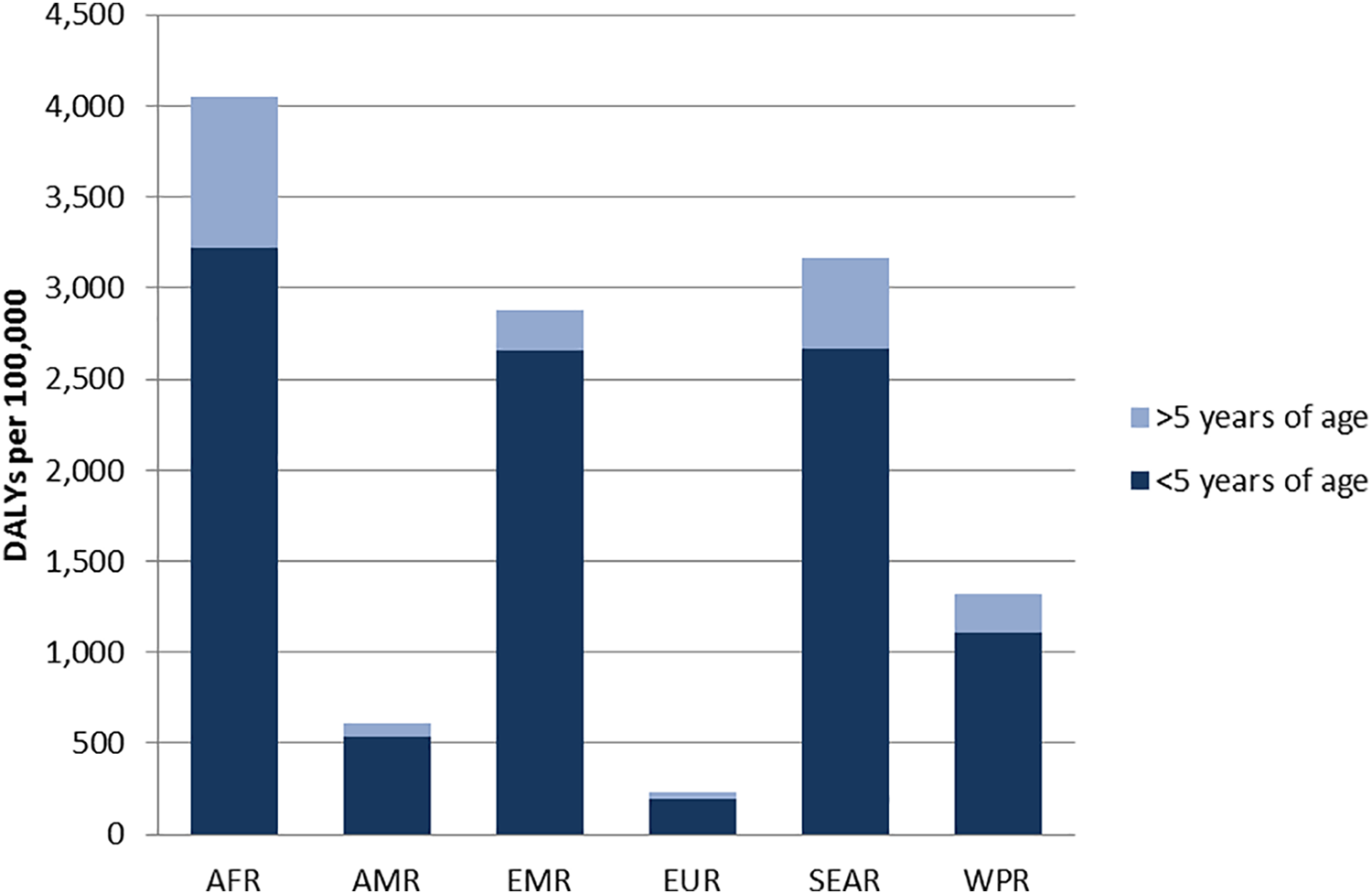
Total foodborne disability adjusted life years (DALYs) per 100 000 inhabitants per age group and WHO region (based on reference 3 ). AFR indicates African region; AMR, Americas region; EMR, Eastern-Mediterranean region; EUR, European region; SEAR, South-East Asian region; WHO, World Health Organization; WPR, Western Pacific regions.
The priority hazards and diseases varied among regions. Pathogens leading to diarrhea caused a large proportion of the total burden of FBD in all regions, 6 but hazards leading to other types of disease such as invasive infectious agents (leading to, eg, meningitis, tuberculosis, or hepatitis) and helminths (causing, eg, liver or lung disease) had a high health impact in some regions, particularly in African region (AFR), South-East Asian region (SEAR), and Eastern-Mediterranean region (EMR). 4 While some hazards were found to be important causes of FBD in all regions of the world, others were only important locally, resulting in a high local disease burden.
As a group, infectious agents that cause diarrheal disease caused the majority of the foodborne illnesses globally (550 of 600 million cases) and over half of the foodborne deaths (230 000 of 420 000) and disability adjusted life years (DALYs; 18 of 33 million). Among all microbiological agents, the hazards causing highest burden of disease due to foodborne transmission globally were nontyphoidal Salmonella enterica (NT Salmonella), S typhi, enteropathogenic Escherichia coli (EPEC), Taenia solium, and norovirus. However, the top agents varied substantially between regions, with Campylobacter, NT Salmonella, and Toxoplasma gondii causing a large proportion of the burden in high-income regions, while EPEC, ETEC, and T solium were more important in lower income subregions (Figure 2). 3,6,7
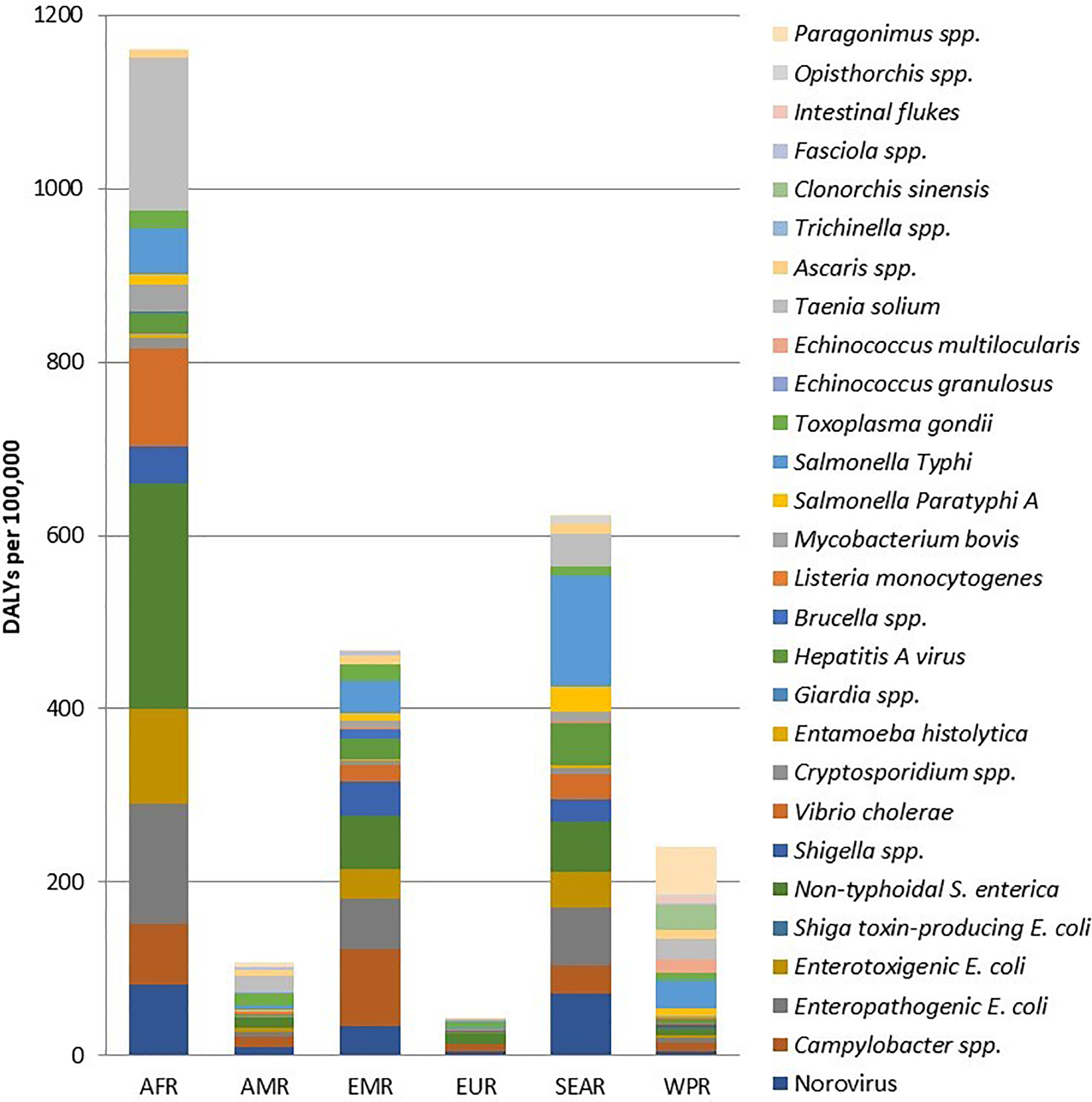
Total foodborne disability adjusted life years (DALYs) per 100 000 population caused by microbiological agents by WHO region (based on references 3,6,7 ). AFR indicates African region; AMR, Americas region; EMR, Eastern-Mediterranean region; EUR, European region; SEAR, South-East Asian region; WHO, World Health Organization; WPR, Western Pacific regions.
The burden due to the 3 considered chemical hazards was highly localized. 8 Aflatoxins caused the highest burden in AFR, AMR, EMR, and WPR, whereas dioxins caused the highest burden in SEAR, EMR, and EUR. The burden of cassava cyanide was limited to the AFR regions where cassava is a staple food (Figure 3). Peanut allergy caused a relevant disease burden in the most developed subregions (subregion A in EUR, WPR, and AMR) but was not assessed in remaining parts of the world due to lack of data. Dioxins and dioxin-like polychlorinated biphenyls (dl-PCBs), which are persistent environmental pollutants that accumulate in the food chain, primarily in the fatty tissue of animals, were relevant in many regions, even though they do not lead to mortality.
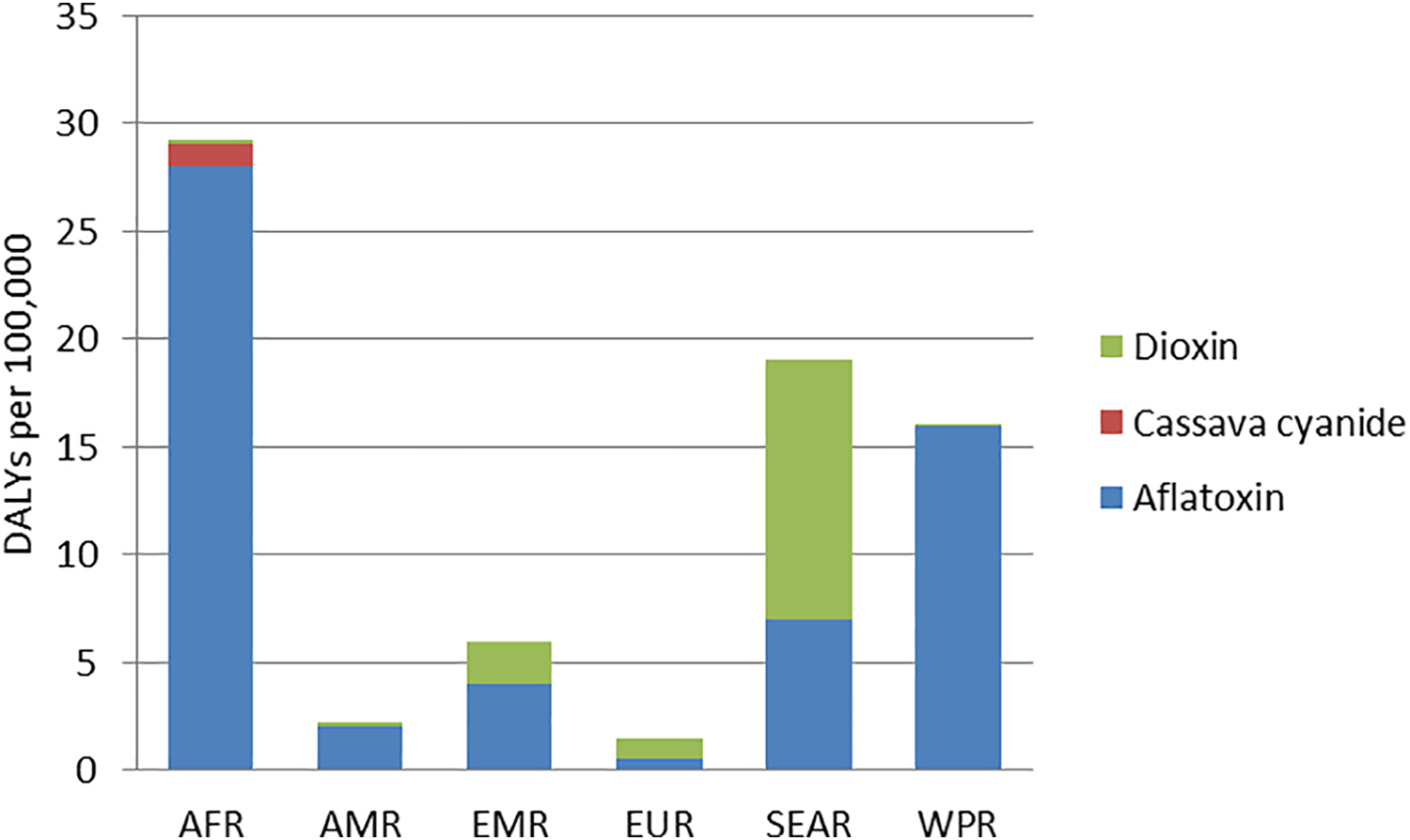
Total foodborne disability adjusted life years (DALYs) per 100 000 population caused by 3 chemical hazards by WHO region. Due to data limitations, the WHO-FERG was not able to study the disease burden of other chemical hazards that are present in foods (based on references 3,8 ). AFR indicates African region; AMR, Americas region; EMR, Eastern-Mediterranean region; EUR, European region; FERG, Foodborne Disease Burden Epidemiology Reference Group; SEAR, South-East Asian Region; WHO, World Health Organization; WPR, Western Pacific regions.
The chemical contaminants assessed were a short list of a range of chemical contaminants and toxins that were considered of potential relevance. While WHO-FERG acknowledged the diversity of harmful chemical contaminants in foods and the potential (and unknown) health impact globally, several data and methodological limitations at the time hampered the inclusion of more hazards in the final study.
WHO-FERG’s estimates showed that global and regional studies face substantial methodological challenges and data gaps, particularly because they need to secure data harmonization, which often leads to a simplification of approaches. As a consequence, the results of WHO-FERG have their limitations and uncertainties and left many important knowledge gaps that need to be addressed. These gaps were particularly evident in low-income regions, where the burden is highest. Expert judgments and modeling approaches for data imputation were used to address them, which allowed for an assessment of the impact of FBDs where data were lacking but also increased associated uncertainties and limitations. 9
Another important limitation of WHO-FERG was the unequal ability to estimate the burden of disease of chemicals when compared to microbiological hazards. This discrepancy is explained by several factors. Burden of disease estimates for any foodborne hazard carry uncertainties, but estimating the burden of foodborne chemicals is particularly challenging. The degree to which it is possible to trace a foodborne illness back to its causative chemical contaminant depends on the nature of the adverse health effect, its disease epidemiology, and exposure pattern. 10 First, a usually long lag-time between exposure to a harmful chemical and the manifestation of symptoms, as well as a multicausal nature of several chronic diseases (ie, cancer, chronic liver disease, etc) hamper the allocation of a disease to its exposure. Second, and related to this long lag-time and multicausality, robust dose–response data are lacking for many chemicals. Third, it is virtually impossible to identify and monitor all potential sources of exposure to harmful chemicals through foods, even in developed countries with extensive monitoring of chemical contaminants in foods and dietary surveys of the population’s food consumption patterns. Lastly, knowledge of the mechanisms behind combined and concomitant exposures to multiple chemicals from all sources (the cocktail effect, ie, when chemicals interact and inflate the effect of the individual chemicals, even though exposure to these is below the levels of observed adverse effects 11 ) is to a large extent lacking, and scientific evidence to document and quantify such effects is not yet available. To add to these limitations, the fact that the burden of disease caused by microbiological hazards and by chemicals is estimated using different methodologies complicates comparison of results.
WHO-FERG did not estimate the burden of antimicrobial resistant foodborne pathogens. Antimicrobial resistance is a global public health crisis that threatens our ability to successfully treat bacterial infections, and the transmission of resistant bacteria through foods has long been established. 12 Resistance in microorganisms present in foods can develop through use or overuse of antimicrobials in food-producing animals. Other important drivers of antimicrobial resistance in foodborne pathogens are use of antimicrobials in humans, environmental contamination of waters and the environment (including other foods), and any other factors that promote the spread of resistant bacteria and their genes locally and globally. 13 Estimating the burden of foodborne antimicrobial resistance is particularly challenging. On one hand, the health consequences of infection with resistant bacteria add to the ones of the original infection (eg, severe diarrhea or septicemia), either by increasing the severity of the symptoms or by leading to treatment failure; quantifying the incidence of these is compromised by lack of health registry data globally. 14 On the other hand, the epidemiology of antimicrobial resistant bacteria and determinants is more complicated than most foodborne pathogens. This is because people may be asymptomatic carriers of these resistant bacteria over long periods and therefore an organism that originated from an animal-derived food may manifest as, for example, a hospital-acquired infection (ie, acquired by person-to-person transmission). Moreover, resistant bacteria can infect individuals directly, but can also transfer resistance genes to other bacteria, including in the human gut.
Recent Evidence on the Burden of FBDs
Several countries have published recent estimates of the burden of foodborne pathogens. While these include mostly high-income countries (the Netherlands, 15 Japan, 16 Denmark, 17,18 Belgium, 19 the United States 20 ), initiatives in low-income countries have taken the first steps to address knowledge gaps. 21 Comparing national estimates with the regional burden of diseases estimated within the WHO-FERG shows differences in numbers, but in general not in ranking. Continuing these efforts and increasing the number of national studies will improve current regional estimates, reducing uncertainties by using local data, adapting methodologies, and updating with new data.
Similarly, evidence on the burden of individual foodborne chemicals in some countries has been published. 17,22 -24 Again, these studies were conducted in developed countries, where the disease burden may be lower when compared to LMICs. Global disease burden of 4 metals contaminating foods—arsenic, 25 cadmium, 26 lead, 27 and methylmercury 28 —have recently been estimated. Exposure to these heavy metals may lead to health effects with potentially high societal impact (such as intellectual disability caused by maternal exposure of the fetus or exposure of small children to methylmercury and lead) or severe disease (eg, cancer caused by arsenic). Results show that these 4 heavy metals alone account for 9 million DALYs globally each year, and that of the 4 metals, lead accounts for the most illnesses and DALYs. 8 These estimates also corroborate the disproportionally higher burden in some population groups: The burden of disease of lead and methylmercury is carried as life-long intellectual disability and was particularly high in Africa, the Eastern Mediterranean, and low-income countries in the America. 8 The burden of disease of inorganic arsenic was 2.5 times higher in SEAR B when compared to the global burden (adjusted for population size). 25 Heavy metals are either naturally present in the earth’s crust or anthropogenic pollutants that contaminate important food sources such as fish, rice, and vegetables. Therefore, the disparate disease burden across regions reflects both the difference in the level of the contaminants in the environment of regions and in the main staple foods of the same regions (ie, rice is an important staple food in some countries in SEAR and inorganic arsenic is present in high levels in the soil and water in the same region).
Food Safety Versus Nutritional Needs and Benefits
Burden of disease estimates are important to raise awareness of the impact of FBDs on public health and may be used as a basis for prioritization of risk management strategies. Developing these strategies requires more information on which foods are the sources of exposure to the causative agents. Moreover, while it is imperative to identify risk management options focused on the most important food sources causing FBDs, food safety strategies should also consider the food security and nutritional needs of populations. Food safety policies and intervention strategies must be developed in the context of overall impacts on food security, public health, economy, sustainability, and other societal needs. In this section, we present evidence of the main sources of foodborne agents, followed by a discussion of the importance of the context in which food safety policies act, and of ways to provide the evidence of the health and social risk–benefit balance of foods and diets to inform policy-making in these different contexts.
Sources of FBDs
The most important reservoirs, foods and transmission routes of each hazard vary across regions or countries, depending on levels of contamination of foods, animals and the environment, food consumption and preparation habits, food availability, and levels of hygiene. The responsible sources for some agents are easy to identify (eg, the only source of T solium is pork; several parasites are transmitted only through the consumption of fish 29 ; cassava is the source of cyanide exposure 30 ). However, other causative agents can be transmitted through a variety of sources and routes, including several foods and also environment, direct contact with animals and/or with people.
The process of measuring the relative contribution of different sources for a specific foodborne agent is called source attribution. 31 Most approaches for source attribution rely on the availability of empirical data on the contamination and consumption of foods and/or epidemiological data on different diseases, and these are often lacking. To overcome these missing data, WHO-FERG embarked on the first global and regional source attribution effort by conducting a structured expert elicitation. 9
The findings of WHO highlighted the diversity in the foods causing highest burden in the different regions. 32 Most importantly, they also showed that foods that are responsible for important food safety problems and health consequences in a region are also crucial to ensure food security and are essential sources of nutrition in those same regions. Animal source foods such as dairy, eggs, and meat explained approximately 35% of the burden of FBD due to all foods globally. 33 However, animal source foods are also important sources of high-quality nutrients, particularly in regions where the availability of other sources of the essential nutrients is low, thus increasing the risk of nutritional deficiency in children leading to stunting, anemia, or poor cognitive and motor development. Likewise, staple foods in low-income regions such as grains and nuts, fish, seafood, and cassava and other vegetables contribute to the disease burden of pathogens and chemicals. 4,26,33 For example, an increasing number of illnesses and wide-impact outbreaks associated with fruit and vegetables have been registered in recent years. 34 -36 At the same time, these food groups are all important components of healthy diets, promoted and communicated to prevent malnutrition and noncommunicable diseases. 37
Food Safety Policy in Context
The importance of considering factors such as social and cultural context when defining food safety policy is illustrated by its interplay with food security and nutrition. In areas with marginal food supply, the conflict between food safety and food security requires specific focus. In areas where food supplies are abundant and have elasticity, food safety requirements will be easily absorbed, whereas in areas with limited food supply, acute risks such as hunger are often ranked higher in public policy priorities than risk of chronic disease (eg, liver cancer due to exposure to aflatoxins; intellectual disability due to exposure to methyl mercury).
In addition, changes in consumption patterns resulting from, for example, new food trends, introduction of foods uncommon in specific regions due to increased global food distribution and commerce, or recommendation by official dietary guidelines will imply the need for changes in food monitoring and capacity to ensure food safety of all foods. For example, an increased consumption of nuts as advised by health authorities will require identification of associated hazards and monitoring to ensure that there is no contamination above defined safety levels; increased consumption of fish will require improved surveillance and processing requirements; inclusion of novel foods aimed at minimizing environmental impact of diets while promoting health will require evaluation of food safety implications of those foods.
Furthermore, food preferences or trends may vary between countries or regions due to differences in cultural acceptability of specific risks. This is the case for consumption of raw milk or raw-milk products, which is common practice in several countries and banned in others. 38 Consumer-driven trends are in some communities motivated by health or gastronomic claims but may lead to an increased risk of FBD. Where specific health risks are culturally accepted, other risk management and risk communication strategies may be required, targeted at the relevant population. In this context, it can be particularly relevant to characterize and balance the potential trade-offs between health risks and benefits of foods, to provide food safety authorities with objective evidence for decision-making, and to provide consumers with science-based information on potential the health impact of their dietary choices.
Assessing Food Risks and Benefits
In general, foods can present both beneficial and adverse effects on health, linked to, for example, foods’ inherent properties, processing practices, growth conditions, and so on. Despite being developed for the protection of public health, food safety measures may also lead to changes in consumption patterns that impact availability and accessibility of foods or have other health consequences for consumers. Therefore, food policy decisions require consideration of the potential trade-offs. Without assessing the various health consequences associated with changes in consumption of foods, it may be difficult to decide how to intervene in the food chain for optimal health of populations. Risk–benefit assessments compare the positive and negative health effects of foods by integrating scientific knowledge on nutrition, toxicology, and microbiology with human epidemiology. 39 -41 Building on the risk analysis and risk assessment paradigms, risk–benefit assessment was developed recently for decision support. Although the evidence to support policy-making that integrates food safety, nutritional needs and food security of populations is still sparse, an increasing number of risk–benefits is being performed. For example, previous work by FAO-WHO and several international consortia and national research groups has assessed the risk–benefit balance of different foods. 42 -46
Fish is an example of a food commodity for which public health policy needs to consider both adverse and beneficial health effects. Recognized as a healthy food choice because it is a rich protein source and contains omega-3 fatty acids that are important for early brain development and cardiovascular health, fish species may also be contaminated by heavy metals and persistent environmental pollutants responsible for various adverse health effects. 47,48
So far, fish is also the food commodity for which most risk–benefit evidence is available. Risk managers are interested in addressing the health impact of fish for specific risk groups (such as pregnant women) to define interventions or dietary guidelines for these groups. A FAO-WHO Joint Expert Consultation on the risks and benefits of fish consumption reviewed data on levels of nutrients and specific chemical contaminants (methylmercury and dioxins) in a range of fish species globally and concluded that health benefits outweigh the risks in the general adult population. However, the expert group found that at levels of maternal exposure to dioxins (from fish and other dietary sources) that exceed the established provisional tolerable monthly intake, risk of compromised neurodevelopment of the fetus may no longer be negligible. 42 This calls for specific (and restrictive) guidelines for amounts and types of fish consumed for pregnant women as a sensitive subpopulation. Other assessments focusing on the neurodevelopmental effects of fish consumption during pregnancy have supported these findings of the risk–benefit balance of fish consumption (eg, references 44,49 ). These assessments evaluated the impact on neurodevelopment in terms of change in intelligence quotient (IQ) due to the intake of both omega-3 fatty acids and methylmercury in fish. They found that the beneficial effects outweigh the adverse effects at fish consumption in the recommended amounts (between 200 and 500 g/wk). However, the risk–benefit balance varied greatly between fish species, which are known to have different contents of fatty acids and methylmercury. 44,49,50 The highest benefits were estimated for consumption of a variety of fish (both lean and fatty fish), whereas consumption of large predatory and highly contaminated fish species was associated with an overall negative impact on IQ. 44,50 New evidence on the adverse effects of dioxin and dl-PCBs on male fertility of newborn boys suggests that fish consumption advice for women in the childbearing age should be updated, 51 Risk–benefit assessments of fish taking into account this most recent evidence are still lacking.
Another example of risk–benefit evaluation includes an assessment of risks and benefits of nut consumption in Sweden, which found that, on average, the benefits of omega-3 fatty acids in preventing heart diseases are larger than the risks associated to mycotoxins when intake of nuts is limited to a handful of nuts per day. 43 Risk–benefit assessments focusing on hygiene practices or conservation processes such as salting, curing, or smoking of food have also been performed. 52 For example, a study assessed the impact of the use of chlorine-containing disinfectants in food production and food processing to control the contamination by pathogenic and nonpathogenic microorganisms. 53 It identified several disinfectant use scenarios where there were no health concerns, while there was a benefit for microbial food safety and in terms of food spoilage prevention. 53 Another study evaluated the health impact associated with Listeria monocytogenes in cooked ham, the amount of food wasted due to the growth of spoilage bacteria, and the electrical consumption to maintain product temperature through the cold chain. 54 The risk–benefit assessment evaluated the trade-offs between the 3 criteria by applying multicriteria decision analysis and concluded that setting the thermostat of the domestic refrigerator to 4 °C presents the best compromise between them. Assessing the risks and benefits of food processing techniques that are frequent practice of some regions of the world is still lacking but can also be useful to provide advice for consumers or industries.
The examples given show that it is necessary to assess the trade-offs between the risks and benefits of consumption of foods and eventually other indicators and to build on this evidence when defining dietary guidelines and food preparation advice for consumers as well as public health and food safety policy. Even though formal quantitative risk–benefit assessments are still to be conducted for various foods and regions, recognized health benefits and risks can be listed for important food groups. Risk–benefit assessment of foods is particularly important for highly exposed population groups or segments of the population that are more susceptible to particular health end points/hazards. This is essential for providing dietary advice to, for instance, pregnant women, or more generally to women in the childbearing age, who are particularly sensitive to pathogens like L monocytogens and T gondii, as well as chemicals like methylmercury, and at the same time may benefit from specific nutrients present in potentially contaminated foods. With regard to the consumption of fish, specific species and specific preparation methods may be advised for this population group, whereas this advice may be less relevant for the general population. In this context, it is important to focus on risks and benefits, as a single focus on risk or benefit alone may result in unbalanced and inappropriate dietary advices.
Risk–benefit assessment of foods has now been adopted by several national and international authorities. The dominant challenges to develop and implement risk–benefit assessment and the need for international collaboration have been discussed. 55,39 While risk–benefit assessment of foods has so far mostly focused on health impact of foods and been conducted in western countries, it has the potential to consider of other factors, such as food security, foreseen changes in contamination of foods due to climate change or pollution, or local food safety policy.
Impact of Diets on the Environment and Food Safety Implications
The environmental pressure of global food systems has intensified over time, following growth of the human population, changes in food consumption patterns, and intensification of production systems. These developments increase the need for efficient and sustainable food production and a reduction of food losses and waste. Yet, as is evident from the past, more intensive agriculture may give an increased risk of food contamination and an increase in the incidence of FBDs, especially in LMICs. 56,57 Likewise, studies investigating associations between agricultural intensification and human health have found links between irrigation and fish-borne parasites, livestock manure and contaminated produce, antimicrobial use and transfer of resistant bacteria through food, and pesticide use and contaminated foods. 58 Therefore, food safety issues that are a consequence of the responses to the growing demands for nutritious foods and the environmental pressure must be properly managed. This requires increased awareness by all those involved in the food production process and a developed capacity to apply good practices. Highlighted below are areas of particular importance for food safety concerns.
Contaminated Environment and Food Safety
The potential role of wildlife, livestock, human activity, climate, flooding, seed and crop selection, and prior land use in microbial contamination of foods such as leafy vegetables and herbs has been extensively studied. 53 As demonstrated in several high-profile multinational outbreaks, nonanimal food products are increasingly identified as sources of foodborne pathogens, for example, of Shiga toxin-producing E coli (STEC; environmental 36,59,60 exposure plays a role in transmission of a number of pathogens in addition to STEC, eg, Cryptosporidium spp, norovirus, Giardia spp, and T gondii. 9
The role of irrigation water in contamination of leafy vegetables and herbs is particularly important. The water sources at greatest risk of contamination include waters derived from surface or subsurface sources, in which microbiological safety is highly variable. In contrast, potable supplies or rainwater stored in closed containment systems have been considered safest for the production of leafy vegetables and herbs. The use of contaminated water in the preparation of insecticide, herbicide, and fungicide solutions for application to the surfaces of leafy vegetables was also considered to present a risk. 61
Antimicrobial use and overuse in humans and animals (particularly food-producing animals) are important drivers of antimicrobial resistance, 62 but not the only ones. Among other factors that promote the spread of resistant bacteria and their genes locally and globally, environmental contamination plays an important role. Wherever antimicrobials are used, reservoirs of resistance are created, such as within humans and local communities, but also in animals and the farm and aquaculture environments, in water, soil, wildlife, and many other ecological niches due to pollution by sewage, pharmaceutical industry waste, and manure runoff from farms. 13 The role of the environment in the emergence and spread of resistance and its public health impact globally is increasingly recognized and is now identified as an emerging issue of environmental concern. 63 Human exposure to resistant bacteria or resistance genes can then occur through the food chain or direct contact with the environment. In any case, the impact of increasing the resistome in the environment may be substantial due to the possibility of further contamination of the food system.
Current Impact of Climate Change and Food Safety
Intensive food systems are one of the leading causes of climate change, which is unequivocal and progressing fast (note 2). The food safety and public health impact of climate change are closely linked to effects on food security and on nutrition and must be considered together. 64 Projected climate change effects include global air and sea temperature increase, variation in precipitation, drought, and the atmospheric greenhouse gas accumulation. Several of these can be drivers of food safety issues worldwide, mainly due to the impact on the occurrence of food safety hazards at various stages of food chain. By favoring conditions of survival and transmission such as increased temperature and humidity, climate change can lead to increased levels of bacteria, virus, and toxin-producing fungi or parasites in water and food. Food safety implications due to higher rates of microbial growth at increased temperatures may be particularly relevant in fresh fruit and vegetables and fisheries supply chains. 65 Changes in climate may enable growth of mycotoxin producing fungi, including Aspergillus spp producing aflatoxin which may cause hepatic cancer and already now causes a high burden of disease in some regions of the world, particularly Africa. 3 Improved growth conditions for fungi following climate changes might increase exposure to mycotoxins in already affected geographical areas but may also be introduced in areas where current exposure is limited. 24 As foodstuffs providing essential sources of energy and nutrition often can be contaminated in geographical regions with a high FBD burden, climate change may amplify this and thus incur substantial public health, social, and economic impact. 24 In addition, the negative effects of climate change in food systems and safety may be felt particularly in countries that have limited capacity and experience with the management of some of these food safety threats and hence pose new challenges for a potentially underprepared public and institutional setting.
Climate change is also likely to increase the exposure to food contaminants through the tendency to increase the use of agrochemicals to balance the effects of more frequent extreme weather events and water scarcity in some regions, 65 or of veterinary medicines, especially in fisheries. 66 Antimicrobial resistance and zoonotic diseases, both directly linked to food safety, are also expected to be affected by climate change. Other climate change consequences, such as increased sea temperature and acidification, may lead to, for example, harmful algal blooms and consequent public health risk due to fish poisoning. 67 Again, such incidents are more likely to occur in countries where food monitoring and surveillance systems are less robust, therefore unable to detect environmental and chemical contamination, further increasing the risk to public health through the acute and chronic exposure to contaminants.
Dietary Changes to Minimize Environmental Impact and Improve Health
Dietary changes toward healthier diets can reduce the environmental impacts of the food system when the consumption of some intensive-produced foods, particularly animal-based foods, is reduced. 68 Driven both by the United Nations Decade of Action on Nutrition and the general recognition of agriculture’s effect on the environment, some countries have developed dietary guidance that promotes global health by specifically addressing the importance of sustainability as an integral aspect of healthy foods, 69 for example, the Netherlands, Sweden, and Brazil. 70 -72 Still, even if the need to incorporate sustainability considerations into food policies and consumer education programs is increasingly recognized, formally integrating sustainability in official food-based dietary guidelines and actual measurement of impacts of change are only taking initial steps. 73 Additionally, integrating food safety considerations in such assessments will allow for more comprehensive food policy development.
Various studies have assessed the environmental impact of current diets or dietary shifts, most using greenhouse gas emissions (GHGE) as an environmental indicator. 74 -76 The large body of evidence compiled so far points to the combined health and environmental benefits of shifting toward a more plant-based diet, find that meat and dairy are among the largest contributors to GHGE, whereas high consumption of vegetables, fruits, and legumes/pulses/nuts is associated with the lowest GHGE. The production of animal products is particularly problematic due to the low feed-conversion efficiency, enteric fermentation in ruminants, and manure-related emissions. In addition, feed production for animals contributes to fresh water uses and pressures on cropland. Thus far, health benefits have been measured in terms of nutritional adequacy and reduction of risk of noncommunicable diseases.
It has been seen that diet types with no or little meat intake like vegetarian, flexitarian, pescetarian, vegan, as well as Mediterranean and New Nordic diets (NND) would all provide both environmental and health benefits compared to the current consumption patterns in numerous countries globally. 77 -80 This is primarily due to the low amount of meat-based products and processed food in these diets, and the higher proportion of wholegrain, fruits, vegetables, and locally produced foods. If these diets were adopted on a global scale, considerable benefits for environment and human health would be expected. The improvement in health would most likely be highest in countries where the consumption of animal-derived products is high, such as the US and European countries. Studies demonstrating a health benefit of, for example, replacing meat consumption by fish 44 or of following specific territorial diets such as the Mediterranean diet (MD) 81,82 suggest that the beneficial effects are both due to the reduction of meat consumption and due to the increase of replacement foods in the diet, such as vegetables, pulses, and fish. In their assessment, Thomsen et al also consider exposure to chemical contaminants through the foods included red meat, processed meat, and fish, demonstrating that food safety can be included via a risk–benefit assessment. 44
Affordability and Accessibility of Food and Food Safety
While food safety is a major concern globally, the public health impact of FBDs varies substantially across regions. Low- and middle-income countries, which bear the largest proportion of the burden of FBDs, also have lowest capacity and incentives for enhancing food safety systems. 2 Ensuring safety may increase the costs for food business operators and therefore also for the consumers. Furthermore, in extreme/severe poverty scenarios, communities are unlikely to discard foods, even if contaminated and unfit for human consumption. Still, consumers in LMICs value food safety and many are willing to pay more for safer food. 2 Several studies have found that consumers in, for example, Southeast Asian countries (China, Vietnam, Thailand, and India) would be willing to pay from 10% to over 100% more for foods with a “safe food” label. 2 However, the actual behavior of consumers may differ from what is measured in surveys and theoretical exercises and not all may be able to pay more for foods. The poorest households in LMICs spend approximately 70% on total expenditure on food; in South Sudan, for example, people would have to spend 155% of daily income on a basic plate of the main staple. Thus, in many instances availability and affordability of foods will be the first priority.
In the case of weak food safety systems and absence of control measures in the food production chain or in the informal food sector, training and education of those working in all steps of the production chain, as well as consumer awareness, have the potential to reduce the burden of FBDs. 83 Current estimates show that foodborne microbiological hazards are the major causes of the disease burden globally. In LMICs, traditional informal food markets, for example, street food and wet markets provide up to 85% to 95% of the market demand for food, 84 and it is estimated that 2.5 billion people eat street food daily, as this offers easily accessible and affordable meals. 85 Several risk factors are identified in the street food settings, including but not limited to unhygienic location in high traffic areas, methods of transporting raw foods including fresh meat, poor hygienic design of food carts, use of contaminated water and ice, lack of knowledge on temperature control, poor personal hygienic practices, and low awareness of chemical and microbial contamination. 2
Efforts to control these risks range from improving the safety of the raw materials used, to practices in the food production chain, where ensuring good hygiene practices, proper storage, sufficient heating, and avoiding cross-contamination of foods are crucial. Most foodborne bacteria, viruses, and parasites are thermolabile and can be reduced or eliminated when foods are stored and cooked properly. 86 However, these practices cannot ensure food safety of fresh produce and ready-to-eat products due to inevitable human errors in strict hygiene performance all over the food chain or of products that are contaminated by hazardous chemicals. The latter may be particularly important in LMICs. Food groups that are essential to ensure food security in populations, such as grains and beans in Africa and fish and seafood in Southeast Asia, may be contaminated with, for example, mycotoxins due to fungal proliferation or with heavy metals as a consequence of environmental pollution, respectively. Pesticides and biocides used to increase the yield of staple foods and fresh produce or to inhibit the postharvest growth of molds may also pose a food safety concern if good manufacturing practices are not followed.
Exposure to chemical contaminants through food may be mitigated by the setting and enforcement of food safety standards in the raw materials. 87 Implementation and enforcement of safety standards in informal/street food market settings is complex, but economic development in LMICs may in the future promote transformation into formal food markets, which will bring about improvements in food safety management. However, monitoring and enforcing food safety standards (ie, limit values for contamination) may impact the affordability and accessibility of foods on several levels. In a domestic market, enforcing safety limits at the production level will likely increase the costs of production and reduce supply of the food (as foods exceeding limits will not be fit for human consumption), which will result in a higher price for the consumer. This is particular the case in LMICs, where removal of heavily contaminated staple food may even result in a food shortage crisis, thus giving rise to the undesired dilemma of choosing between insufficient available food and access to food that is considered unsafe. Too strict food safety guidelines may need to be relaxed temporarily if such a dilemma occurs, and health impact assessments as in risk–benefit assessments of foods may offer a tool to support decision-making.
In an international market, food safety standards may also have detrimental impact on LMICs. In the case of aflatoxin, the toxin produced by the fungi Aspergillus flavus growing on crops before and after harvest, strict maximal tolerable levels in human foods have been established by more than 100 countries. 88 As a consequence, producers in LMICs export the crops of highest quality, leaving the most contaminated for domestic consumption. 89 This is, for example, a particular health problem for aflatoxin, which may cause liver cancer, aflatoxicosis, and immunological disorders. The last 2 are more likely to occur in malnourished individuals, and the liver cancer risk is higher when accompanied by exposure to the hepatitis B virus. 90 These risk factors are more prevalent in several LMICs and may explain the higher disease burden due to liver cancer in regions with high aflatoxin exposure through the diet.
Territorial Diets and Food Safety
Territorial diets have been molded by the availability of foods in different locations and by the traditions of particular cultural groups in these same geographical areas. Some of these diets have been linked to countries, such as the Japanese Diet (JD) or to regions like the MD, the Traditional Nordic Diet, and the NND. Even without an attributed label, several other dietary patterns are territorial throughout the world. Because by definition they are characterized by consumption of locally available and seasonal foods in a specific geographic area, territorial diets naturally contribute to sustaining and preserving the environment and the limited global natural resources. In addition, the health benefits of adhering to the regional European diets MD and the NND, particularly for the prevention of noncommunicable diseases, are well established. 91 However, food safety issues related to these types of diets have thus far not been well studied.
Potential food safety implications of the NND and the MD are linked to consumption of food groups that can lead to exposure to certain chemicals and pathogens and thus pose a risk to human health. Specifically, increased consumption of vegetables could lead to increased exposure to pesticides and heavy metals 92,93 ; increased consumption of raw vegetables could increase risk of infection by several pathogens 34,35 ; increased consumption of nuts can lead to increased exposure to mycotoxins 94 ; increased consumption of fish could lead to increased exposure to methylmercury and other pollutants 95 ; among others. Safety evaluations of the MD and NND as whole diets appear to be lacking, but specific foods typical for these types of diets have been evaluated in food risk assessments. As an example, one of the guidelines for the NND is to eat more food from wild landscapes, which is suggested for its environmental and nutritional benefits but has called for an evaluation of food safety implications. The safety of wild plants used in the NND has been assessed in 2 risk assessments of 4 wild plants potentially used as vegetables and 23 flowers served at restaurants. 96,97 One of the 4 assessed plants (common lambsquarters [Chenopodium album L]) was found to potentially pose a risk due to high levels of oxalic acid. The authors emphasized the need for more and better compositional analyses of potential edible plants before recommending these as a substantial part of a healthy diet. 96 Other authors emphasized the lack of both chemical and toxicological data for the risk assessment of wild or cultivated flowers for food use. 97
Various specific dietary aspects of the NND and the MD have been subject to risk–benefit assessment. Both diets are characterized by a high intake of plant-based foods, a moderate intake of fish, and a low intake of red and processed meat and sweets. 91 The risk–benefit balance of changing from current consumption habits toward these characteristics has been assessed individually for various populations. As mentioned above, in particular the risk–benefit balance of increased fish consumption has been evaluated extensively, comparing the chemical and/or microbiological risks with the nutritional benefits. 98 Across assessments and countries, increased fish consumption has been found to be overall beneficial and safe when choosing fish with low levels of contaminants such as methylmercury and dioxins and with high contents of the fatty acids docosahexaenoic acid and eicosapentaenoic acid, 44,49,50 when stored properly. 99
One component of the MD is a high intake of nuts, which have been found to significantly reduce the risk of mortality due to cardiovascular disease, myocardial infarction, and stroke. 91 However, in addition to a range of other beneficial nutrients, nuts may also contain carcinogenic mycotoxins. As mentioned earlier, in a risk–benefit assessment, increased nut consumption was found to be beneficial in the Swedish adult population. 43
The consumption of fruit and vegetables is dominant in both the MD and NND, and the latter advises specifically to give preference to organic production foods. Valcke et al assessed the risk of cancer from pesticide residues in fruit and vegetables and held it against the cancer-protective effects of fruit and vegetable consumption. 100 They found that the cancer protective effects of fruit and vegetable consumption dominated over the risk from pesticide residues. 100 While some studies have suggested that organic farming practices such as the use of animal manure can increase the probability of contamination by pathogenic microorganisms and may consequently pose health risks. 101 The number of studies comparing organic and conventional produce regarding microbiological safety is scarce. Comparing organic and conventional production in terms of food safety is a difficult task due to the limited and conflicting evidence. 102
Overall, current scientific evidence suggests that the health benefits of the European territorial diets MD and NND outweigh food safety risks on a population level. However, evidence for the overall health impact for other territorial diets is still missing. Still, even if not classified as territorial diets, the beneficial and/or adverse health effects of dietary habits that are characteristic of specific geographic areas can be evaluated. 103 Rice is a staple food in many parts of the world and provides basic nutrition to many populations; however, rice may also be contaminated with inorganic arsenic, which is a human carcinogen. 104 Likewise, consumption of cassava, which is an important staple food for over 800 million people in approximately 80 countries, mostly in sub-Saharan Africa but also in Asia, the Pacific, and South America, may lead to intoxications with neurological complications due to high cyanide exposures. 30 Smoking fish, when carried out with traditional methods involving direct contact with wood combustion fumes, is responsible for high contamination levels with carcinogenic polycyclic aromatic hydrocarbons. 105 Finally, insects are a traditional part of the diet in specific areas of the world, receiving increasing interest as a novel food and an environmentally sustainable alternative to animal-based protein sources in other world regions. However, to this date not much is known about the safety and allergenicity of insect processing and consumption. 106
Concluding Remarks
Dietary changes toward healthier diets can at the same time reduce the environmental impacts of food systems. The current body of evidence points to the combined health and environmental benefits of shifting toward a more plant-based diet, including vegetables and fruits, nuts, pulses, and whole grains. As a shift toward more plant-based diets may also lead to higher exposures to chemicals or pathogens present in these foods, an evaluation of food safety implications of such transitions is now imperative.
Available studies taking into account nutritional and food safety considerations, mostly in high-income countries, have provided scientific evidence on the balance between adverse and beneficial health effects of consumption of a number of food groups. Evidence to evaluate the balance between food safety and nutritional impact of other foods and in wider geographical representation is lacking. Based on the identified need for a more plant-based diet that contains sufficient protein and recognizing the existing regional variations, we have identified the following priority areas for further study: Assessment of the health impact of increased consumption of pulses, taking into account substitution of animal-based foods and regional variability in terms of age and gender distribution, consumption patterns, and food contamination. Assessment of the health impact of increased consumption of vegetables, distinguishing between raw and heat-treated vegetables, taking into account substitution of other foods and regional variability in terms of age and gender distribution, consumption patterns, and food contamination. Assessment of the health impact of increased consumption of insects, taking into account substitution of other animal-based foods and regional variability in terms of age and gender distribution, consumption patterns, and food contamination.
Currently available evidence also shows that several synergies between public health, environmental, and food safety strategies can be identified to support dietary transitions. As an illustration, reducing meat consumption will lead to an overall health gain due to decreased incidence of noncommunicable diseases; reduction of the exposure to foodborne pathogens in general; and reduction in usage of antimicrobials, leading to a reduction in antimicrobial resistance. At the same time, it will have a positive sustainability impact due to decreased meat production and consequent decreased environmental pressure. The identification of other synergies, supported by scientific evidence of the recommended policies, will facilitate implementation and adherence to the proposed dietary transitions.
Footnotes
Authors’ Note
SMP, STT, and LJ conducted the literature review and wrote the manuscript. MP and MN reviewed the text provided input to various versions of the manuscript.
Acknowledgments
The authors thank FAO and WHO secretariat and staff for valuable review comments to the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This paper was made possible with funding from WHO.