
Abstract
Background:
Adequate quality complementary diets and appropriate feeding practices are important for proper growth and development of young children.
Objective:
To assess factors associated with diet diversity, meal frequency, and acceptable diet of children aged 6 to 23 months in two agroecological zones of Rongai subcounty, Kenya.
Methods:
A cross-sectional study was conducted among 384 mothers/caregivers with children aged 6 to 23 months. A structured questionnaire was used to assess sociodemographic characteristics and child feeding practices. Diet diversity, meal frequency, and acceptable diet were derived from a 24-hour recall of child’s food intake. Factors associated with diet quality were determined using binary logistic regression.
Results:
Mean child diet diversity score was 3.54 ± 1.0 of 7 food groups, with 56.8% of the children achieving minimum dietary diversity. A majority of the children (81.8%) received minimum meal frequency (MMF), with significant (P < .05) difference between low (91.1%) and high (75.2%) agricultural potential areas. Children who received minimum acceptable diet (MAD) were only 34.1%. Mother/caregiver education level positively (P < .05) associated with minimum diet diversity in low potential area (adjusted odds ratio [AOR] = 3.79, 95% CI: 1.47-9.75) and with MAD in high potential area (AOR = 1.87, 95% CI: 1.01-3.46). Other factors associated with MDD, MMF, and MAD included household income and slow feeding in low potential area, and child gender and active feeding in high potential area.
Conclusion:
There is a variation in factors associated with diet quality and child feeding practices in different agroecological zones. Therefore, nutrition education and behavior change communication interventions aimed at improving child nutrition should be context-specific.
Keywords
Introduction
Many developing countries are still facing the problem of malnutrition, especially among children younger than 5 years. Globally, 22.9% of children younger than 5 years are stunted and 7.7% are wasted. 1 In Kenya, the national level of stunted, underweight, and wasted children is currently at 26%, 11%, and 4%, respectively. 2 Children below 2 years are particularly a vulnerable group since inadequate nutrition during this period is associated with growth faltering, increased risk of morbidity and mortality, impaired motor and cognitive development, reduced educational attainments, and social capacities. 3,4 The first 1000 days of a child’s life is an important period for growth and development 5 where much growth faltering takes place during the complementary feeding period (gradual introduction of soft and semisolid foods alongside breast milk) at age 6 to 23 months. Inappropriate complementary feeding practice is a major factor contributing to inadequate nutrient intake among infants and young children. 6 Complementary feeding practices have been associated with factors such as maternal knowledge on complementary feeding, child’s age, access to postnatal health-care services, and maternal busy schedules. 7 However, specific patterns and contexts within particular communities need to be better understood.
Consuming a diverse diet increases the possibility of adequate intake of essential nutrients. 8,9 However, in Kenya, traditional diets fed to infants and young children during the complementary feeding period are characteristically based on starchy staples with little or no nutrient-rich food sources such as animal source protein, fruits, and vegetables. Mothers/caregivers’ lack of nutrition knowledge and their feeding attitudes have been identified as predictors of a child’s meal frequency and diet diversity. 10 In our previous work in Rongai subcounty, 11 we found that mothers/caregivers consumed poor quality diets despite diversity of food in their farms, suggesting lack of knowledge on locally available nutrient-rich foods and the best ways to utilize them in diet. This may have implications on quality of diets given to the children.
Minimum dietary diversity (MDD) for children is defined as consumption of at least 4 of the 7 food groups recommended by World Health Organization (WHO). 12 Although consuming a variety of foods increases the chances for provision of diverse nutrients, 7 meal frequency is equally important in order to attain an acceptable diet for children. Children aged 6 to 23 months should receive complementary foods 2 to 4 times a day with 1 or 2 snacks as the desired minimum meal frequency (MMF). 12 Meeting the MDD requirement together with the stipulated MMF contributes to achieving a minimum acceptable diet (MAD). In Kenya, 41% of children attained MDD, with 51% meeting the MMF requirement and consequently only 22% achieved MAD. 2 Clearly, meeting both the MDD and MMF requirements concurrently seems to be a limiting factor of diet quality that needs to be addressed.
Improving mother/caregivers’ child feeding practices such that they observe attainment of both MDD and MMF requirements can contribute to improving the quality of complementary diets. 13 Therefore, it is vital to understand how mother/caregivers’ child feeding practices influence the diet diversity, meal frequency, and subsequently acceptable diet of children aged 6 to 23 as these may vary from region to region. This would be an important input to developing contextualized interventions that are based on prevailing child feeding practices instead of generalized interventions that may not relate well to the context.
Different agroecological zones have been identified to contribute to variation in diets of children. 10 The variation in diet diversity was observed across agroecological zones in Nepal, 14 while in rural Ethiopia, 15 differences in MDD, MMF, and MAD were reported in lowland and midland agroecological zones. However, adequate research has not been done to further explore such occurrence in Kenya. Therefore, the objective of this study was to determine how mother/caregiver characteristics and child feeding practices influence diet quality of children aged 6 to 23 months in 2 agroecological zones (low and high agricultural potential areas) of Rongai subcounty in Nakuru County, Kenya.
Methods
Research Design and Sampling
A cross-sectional study was conducted in Rongai subcounty of Nakuru County in Kenya during the lean season of January/February when food supply was scarce. Rongai subcounty has 2 major agroecological zones: the low and high agricultural potential areas. The low agricultural potential area lies at an altitude of 1520 to 1890 m with higher temperatures ranging from 26°C to 30°C and receives an average of 760 mm of rainfall annually. The high agricultural potential area lies at an altitude of 1800 to 2400 m with lower temperatures ranging from15°C to 20°C and receives an annual rainfall averaging between 760 and 1270 mm. 16 This study was part of a bigger project aimed at determining the relationship between agrobiodiversity and dietary diversity of women and young children in Rongai subcounty, Kenya. Two divisions were purposively selected from Rongai subcounty, Kampi Ya Moto from low potential area and Menengai from high potential area. Eight sublocations were then purposively selected from the 2 divisions, with Kampi Ya Moto, Makutano, Kapsetek, and Morop sublocations from low potential area and Ogilgei, Kamungei, Mang’u, and Sumek sublocations from the high potential area. This study targeted mothers/caregivers with children aged 6 to 23 months from households that practiced smallholder farming. A list of these households in the 2 divisions was obtained from the Ministry of Agriculture, Nakuru County population records. The sample proportion of respondents desired from each sublocation was determined using proportionate sampling based on this list of households. A sample of 388 mother/caregiver–child pairs were randomly selected using Statistical Package for Social Sciences (SPSS) version 20.0 software 17 (low potential, n = 161; high potential, n = 227) for participation in the study.
Data Collection Tools and Procedures
Sociodemographic characteristics
A structured questionnaire was used to collect data on sociodemographic characteristics of the household and mother/caregiver–child pairs. These data included mother/caregiver’s age, relationship to household head, education level, household income, household food access (using Household Food Insecurity Access Scale [HFIAS]), child’s age, and gender. Education level was based on formal education and was categorized into low and high education level. Mothers/caregivers who had no formal education and those who attained up to primary level were considered to have low education level. Those who attained secondary and tertiary education levels were considered to have high education level. Household income was determined by asking the respondents to indicate their household income range in the following categories: from below 3500 Ksh/month (US$35) up to 7000 Ksh/month (US$70) (low income) and from 7001 Ksh/month (US$70.01) up to more than 14 000 Ksh/month (US$140) (high income). Household Food Insecurity Access Scale was based on the Food and Nutrition Technical Assistance guidelines of assessing food insecurity. 18 The HFIAS indicators were grouped into 2 categories of food secure and food insecure households (mildly, moderately, and severely food insecure households).
Infant and young child feeding practices
Mothers/caregivers provided information regarding child feeding practices and dietary intake within the previous 24 hours. The child feeding practices assessed were based on the principles of psychosocial care in responsive feeding. 19 Mothers/caregivers were asked questions regarding the method of child feeding, person feeding the child, types of food fed to the child, time and place of feeding the child, and active participation in child feeding. A series of 10 questions regarding child feeding practices were asked and scores of 1 and 0 given to correct and incorrect responses, respectively. The responses were then scored and compounded into 2 categories of poor and better child feeding practices. A score of below 5 was considered poor practice and score of 5 and above was considered better practice.
Child dietary patterns
The children’s dietary patterns (MDD and MMF) were assessed using a 24-hour food recall. Data from the 24-hour food recall were used to compute child dietary diversity score (CDDS) based on the 7 food groups recommended by WHO. 12 These 7 food groups included (1) grains, roots, and tubers; (2) legumes, nuts, and seeds; (3) eggs; (4) flesh foods; (5) dairy products; (6) vitamin A-rich fruits and vegetables; and (7) other fruits and vegetables. 12 Nonbreastfed children who consumed foods from at least 4 food groups were considered to have achieved MDD. Breastfed children who consumed at least 3 food groups from 6 food groups (with dairy products excluded) were considered to have achieved MDD. Meal frequency was determined based on the number of main meals and snacks consumed by the child as indicated by 24-hour food recall. Breastfed children who ate 2 to 4 times a day plus at least one snack were considered to have attained MMF. Nonbreastfed children who ate 4 to 5 times a day plus at least 1 snack and 2 milk feeds were considered to have achieved MMF. If both MMF and MDD were attained, then the child’s diet was considered to have met MAD requirement.
Data Analysis
Data were analyzed using SPSS, version 20.0. 17 Data on mother/caregiver and child sociodemographic characteristics and IYCF practices were analyzed using χ2 test and independent sample t test for comparison of means between high potential and low potential areas. Binary logistic regression was used to determine the association of independent variables with dietary adequacy of children (MDD, MMF, and MAD). P < .05 was considered statistically significant.
Ethical Considerations
Ethical clearance was obtained from Egerton University Ethical Clearance Board and research permit from National Council of Science and Technology, Kenya. Permission from the relevant authorities at subcounty, location, and sublocation levels was also sought prior to data collection. Informed consent was obtained from the participants before any data were collected. The participants were also assured of confidentiality of information provided during the study.
Results
Sociodemographic Characteristics
The sociodemographic characteristics of mothers/caregivers and their children are shown in Table 1. Overall, mothers/caregivers had a mean age of 29.09 ± 9.17 years, while each family had an average of 3 children in total (2.80 ± 1.97). The mean age of the surveyed children 6 to 23 months was 15.58 ± 5.63 months, with 51.6% being male and 48.4% female. Literacy levels were low, with more than half (53.6%) of the mothers/caregivers having no education or primary education level. There were no significant differences (P < .05) in all the sociodemographic characteristics of mothers/caregivers and children between low and high potential areas.
Sociodemographic Characteristics of Mothers/Caregivers and Children Aged 6 to 23 Months in Low and High Agricultural Potential Areas of Rongai Subcounty.
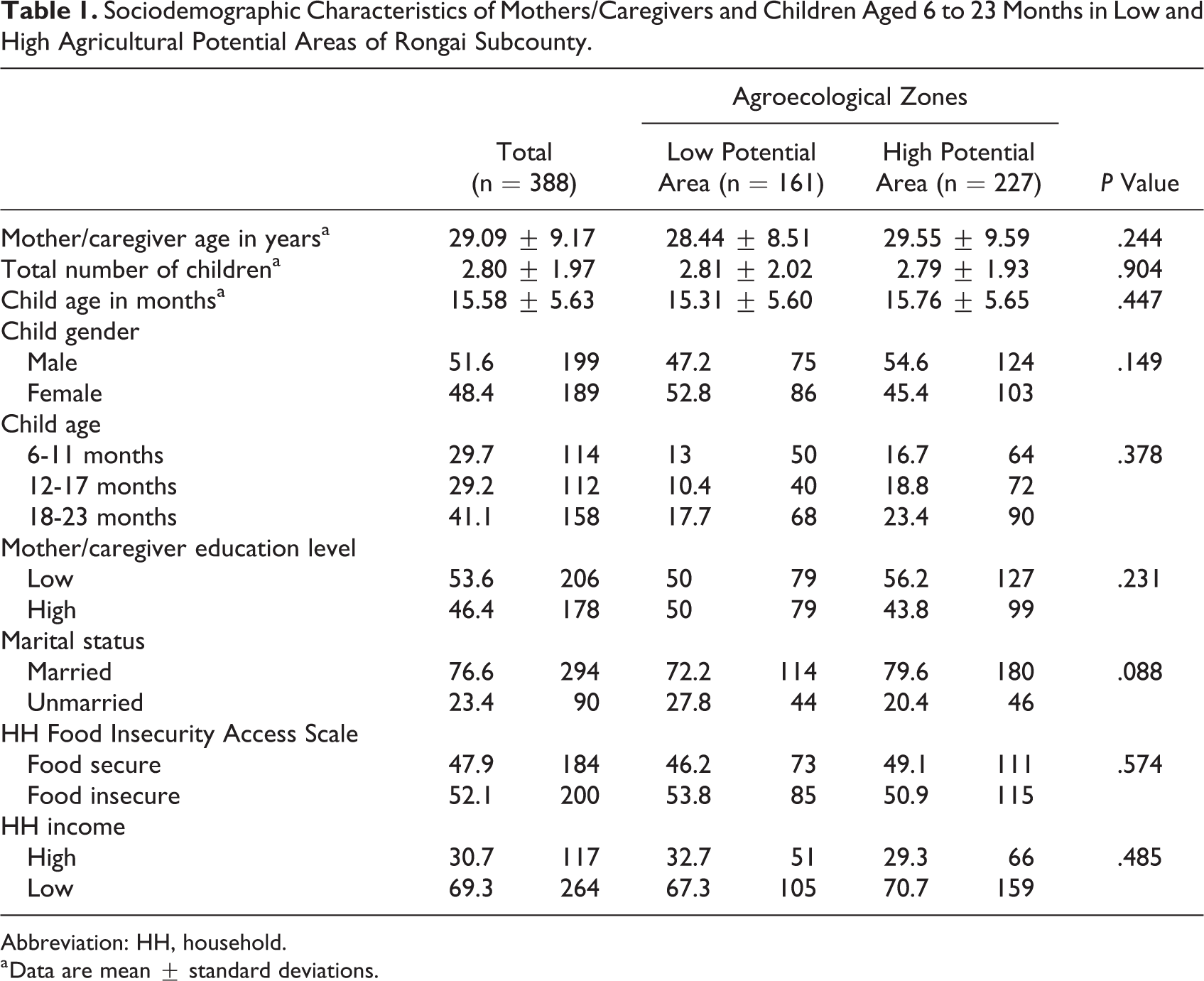
Abbreviation: HH, household.
a Data are mean ± standard deviations.
Infant and Young Child Feeding Practices
Table 2 shows child feeding practices of mothers/caregivers of Rongai subcounty. Generally, the mean age at which complementary feeding was started was 17.93 ± 9.16 weeks. Among the children, 75.6% were still breastfeeding alongside being given other foods. There was no difference (P > .05) between the 2 agroecological zones in the proportion of mothers/caregivers feeding the child with family foods. Furthermore, 74% of the mothers/caregivers prepared special meals for their children (no difference between the 2 agroecological zones). The main reasons given for not preparing special meals for the child were that the child was old enough to eat family food followed by lack of food. More mothers/caregivers (P > .01) in high potential area (35.1%) mentioned that the child is old enough as compared to only 17.3% in low potential zone. More mothers/caregivers (P = .034) from low potential area (13.6%) pointed out the lack of food as a reason for not preparing special meals for their children compared to mothers/caregivers from high potential area (6.0%). In addition, a majority of the children were fed by mothers/caregivers using separate feeding equipment (87.6%). Most mothers/caregivers (49.5%) practiced feeding the child slowly and patiently in order to ensure that the child eats required portion of food. When the child refused to eat a particular type of food, mothers/caregivers mainly tried feeding that particular food again after a few days (26.2%). There was a significant difference (P < .05) between the 2 zones where the practice was to combine the particular food with another food and force feeding the child upon refusal to eat a particular type of food.
Infant Feeding Practices in Low and High Agricultural Potential Area of Rongai Subcounty.
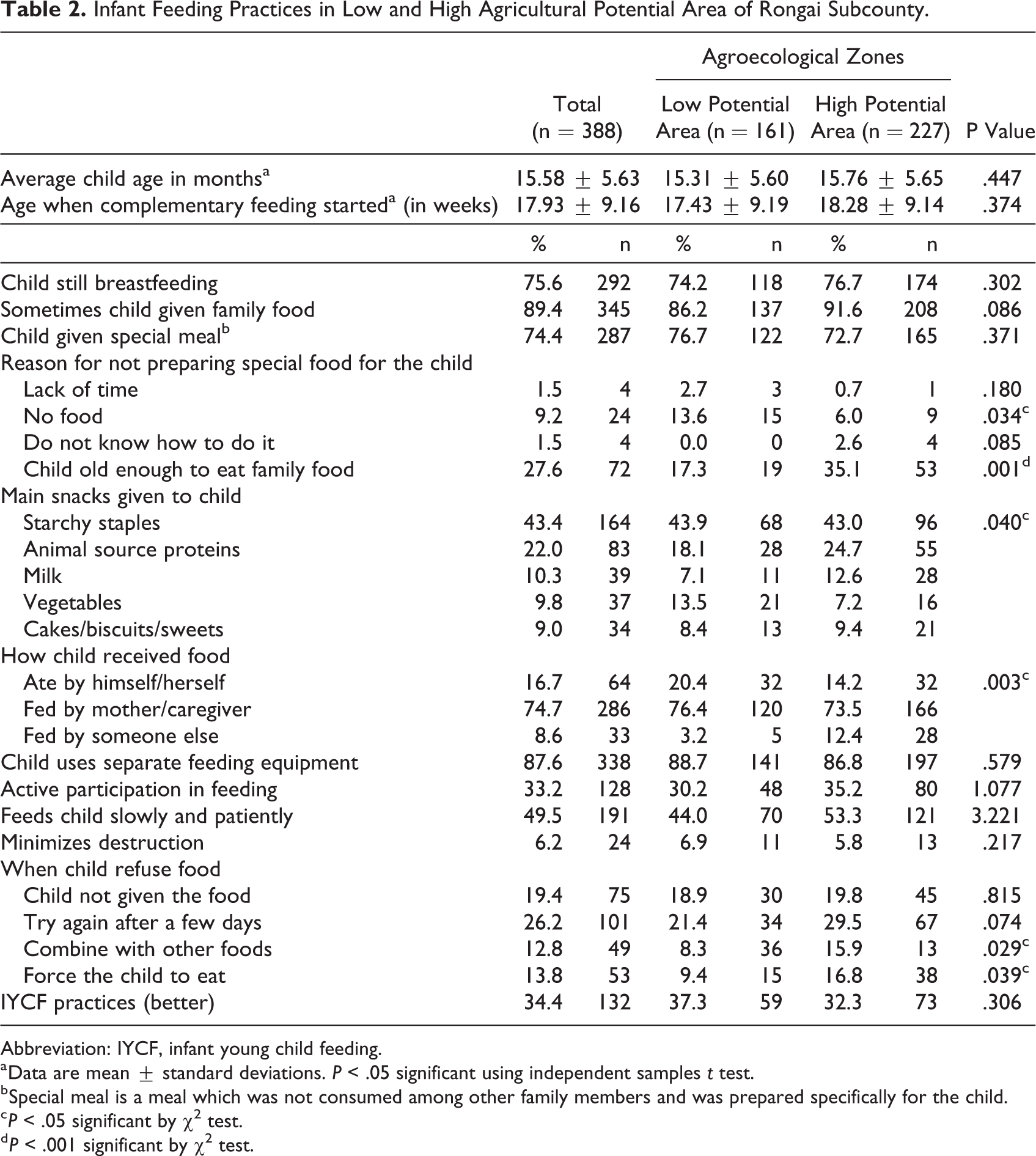
Abbreviation: IYCF, infant young child feeding.
a Data are mean ± standard deviations. P < .05 significant using independent samples t test.
b Special meal is a meal which was not consumed among other family members and was prepared specifically for the child.
c P < .05 significant by χ2 test.
d P < .001 significant by χ2 test.
Child Dietary Patterns
The proportion of children who consumed food from the 7 recommended food groups is presented in Table 3. Overall, the frequently consumed foods were grains, roots, and tubers (99.5%) and dairy foods (87.5%). Eggs (3.1%) and flesh foods (4.7%) were the least consumed foods. More (P < .05) children from high potential area (85.7%) consumed other fruits and vegetables as compared to those from low potential area (77.6%). The snacking pattern, number of meals, and dietary diversity scores of children in low and high potential area are illustrated in Figure 1. There was no difference (P > .05) in the number of snacks consumed per day among children in low (2.47 ± 1.559) and high agricultural potential area (2.32 ± 1.183; Figure 1). The number of main meals given to children was different (P < .001) between low (3.23 ± 0.811) and high (2.92 ± 0.718) agricultural potential areas. In addition, the total number of meals consumed was different (P < .001) between the 2 areas. Children from low potential area had more number of meals (5.71 ± 1.739) compared to those from high potential area (5.19 ± 1.231). Overall, mean CDDS was 3.54 ± 1.01, with no difference between low (3.52 ± 1.00) and high (3.57 ± 1.04) agricultural potential areas (P > .05; Figure 1).
Proportion of Children Aged 6 to 23 Months Who Consumed Foods From Different Food Groups in Low and High Agricultural Potential Area in Rongai Subcounty.
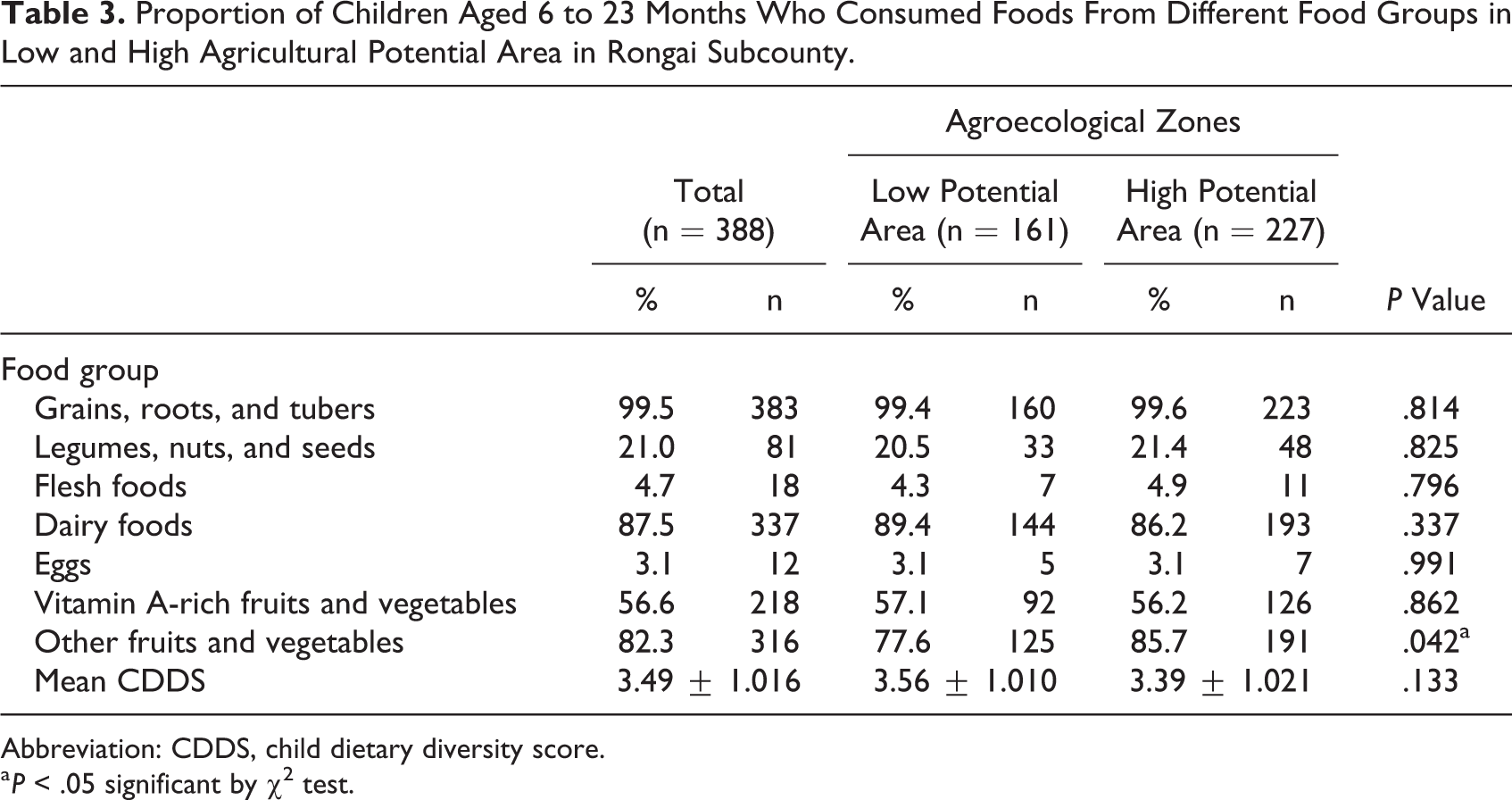
Abbreviation: CDDS, child dietary diversity score.
a P < .05 significant by χ2 test.
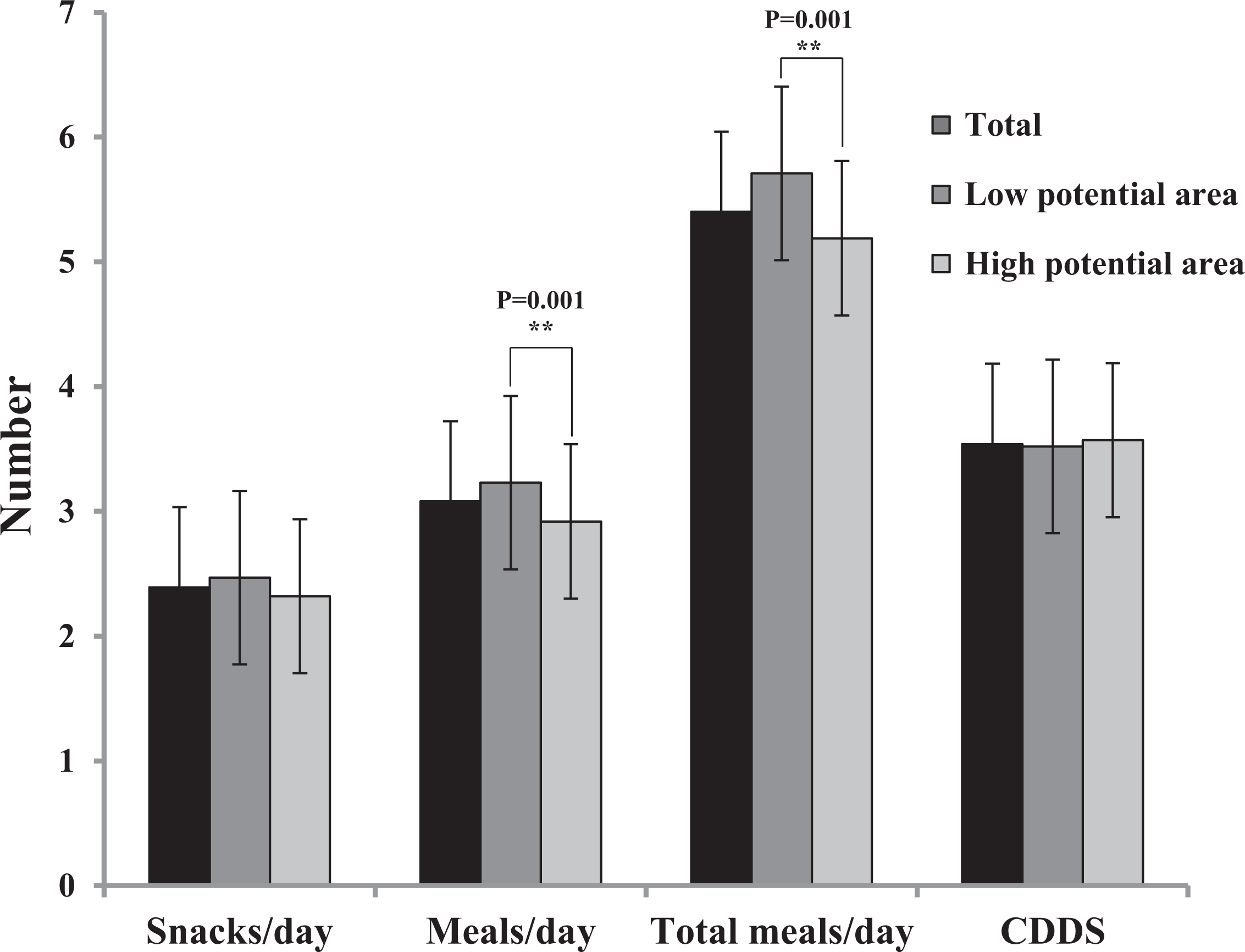
The minimum number of snacks taken per day, main meals, total number of meals, and dietary diversity score for children aged 6 to 23 months old in low and high agricultural potential areas of Rongai subcounty. **P < .01 significant by independent samples t test. CDDS indicates child dietary diversity score.
Figure 2 illustrates the proportions of children who met MDD, MMF, and MAD in low and high potential areas. Overall, more than half (56.9%) of the children consumed a diverse diet (>4 food groups) with no difference (P > .05) between low (57.1%) and high potential areas (56.7%). Generally, most (81.8%) of the children attained the MMF requirement, with the majority from low potential area (91.1%) compared to high potential area (75.2%). Only 34.1% of children attained MAD with no difference (P > .05) between high (35.8%) and low (31.6%) potential areas.
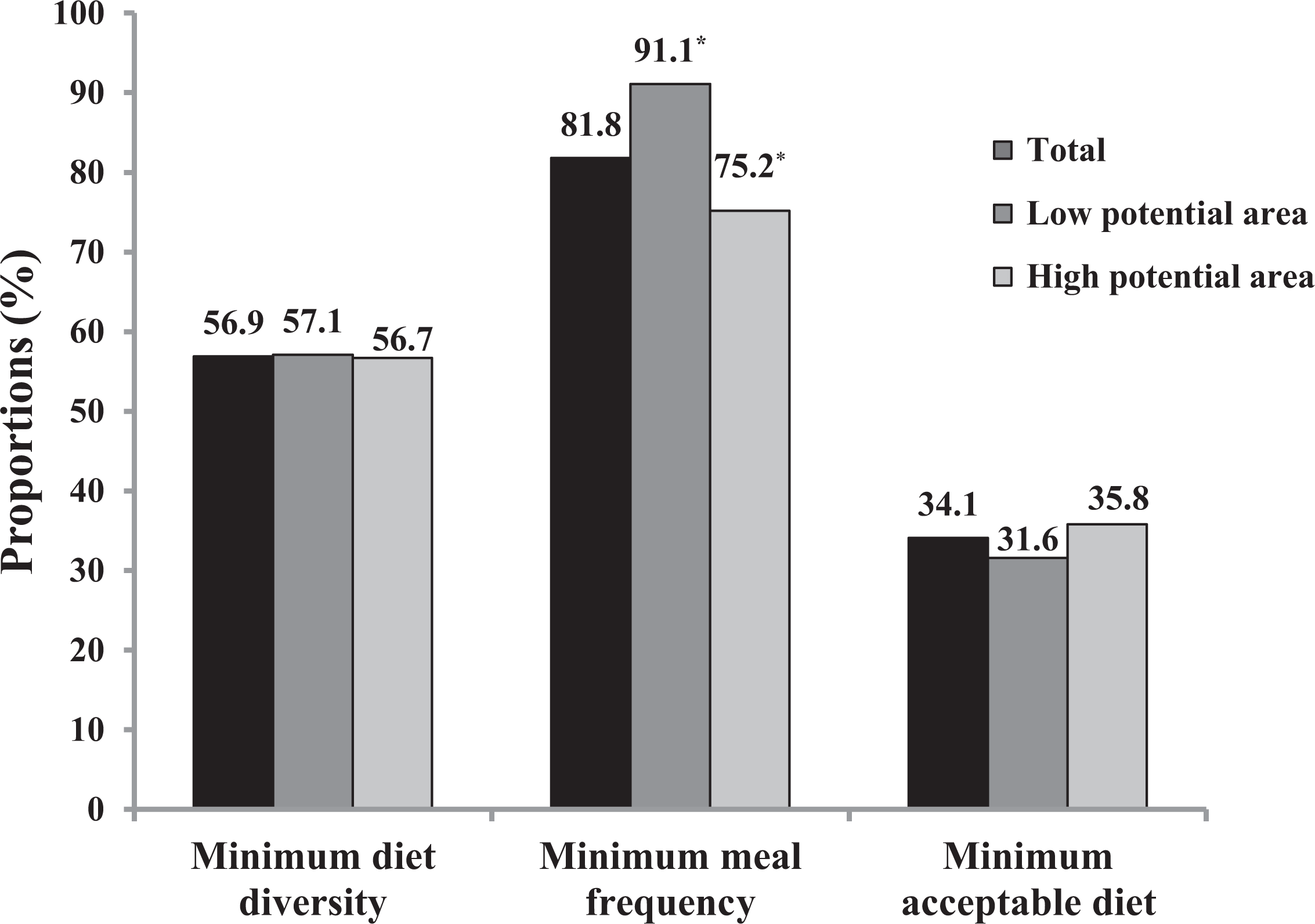
Proportion of children meeting minimum dietary diversity, minimum meal frequency, and minimum acceptable diet in low and high agricultural potential area of Rongai subcounty. *P < .05 significant by χ2 test.
Factors Associated With Children’s Dietary Patterns
Table 4 presents the factors that were associated with MDD, MMF, and MAD of children compared across the 2 agroecological zones of Rongai subcounty. In low potential area, children who were fed slowly were more likely to attain adequate MDD (adjusted odds ratio [AOR] = 3.46, 95% confidence interval [CI]: 1.31-9.10; P < .05). Children whose mothers/caregivers had high education level (AOR = 3.79, 95% CI: 1.47-9.75; P < .05) and those who were from households with high-income level (AOR = 3.07, 95% CI: 1.16-8.14; P < .05) were more likely to be fed a diverse diet. Furthermore, those who achieved MMF were more likely to consume an MDD (AOR = 6.81, 95% CI: 1.13-41.11; P < .05).
Factors Associated With Child Diet Diversity, Meal Frequency, and Acceptable Diet in Low Agricultural Potential Area of Rongai Subcounty.
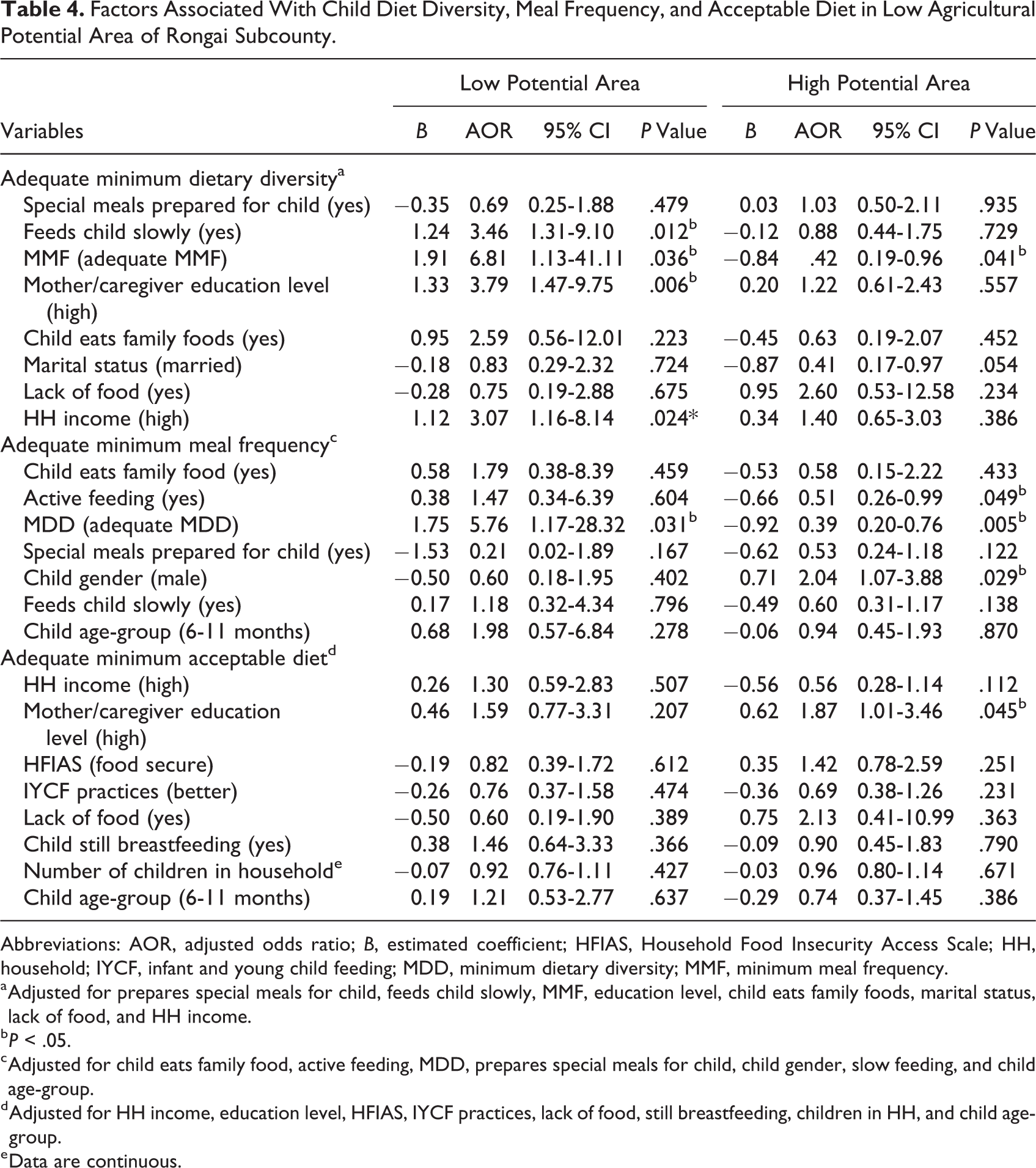
Abbreviations: AOR, adjusted odds ratio; B, estimated coefficient; HFIAS, Household Food Insecurity Access Scale; HH, household; IYCF, infant and young child feeding; MDD, minimum dietary diversity; MMF, minimum meal frequency.
a Adjusted for prepares special meals for child, feeds child slowly, MMF, education level, child eats family foods, marital status, lack of food, and HH income.
b P < .05.
c Adjusted for child eats family food, active feeding, MDD, prepares special meals for child, child gender, slow feeding, and child age-group.
d Adjusted for HH income, education level, HFIAS, IYCF practices, lack of food, still breastfeeding, children in HH, and child age-group.
e Data are continuous.
In contrast, children from high potential area who achieved MMF were less likely to consume an MDD (AOR = 0.42, 95% CI: 0.19-0.96; P < .05). Children from low potential area whose diets were diverse were more likely to attain MMF (AOR = 5.76, 95% CI: 1.17-28.32; P < .05). On the contrary, children from high potential area who consumed a diverse diet were less likely to achieve MMF (AOR = 0.39, 95% CI: 0.20-0.76; P < .05). Children from high potential area who were actively fed were less likely to achieve MMF (AOR = 0.51, 95% CI: 0.26-0.99; P < .05). Male children from high potential area were more likely to be fed frequently than their female counterparts (AOR = 2.04, 95% CI: 1.07-3.88; P < .05). Mothers/caregivers from high potential area with high education level were more likely to feed their children with an acceptable diet (AOR = 1.87, 95% CI: 1.01-3.46; P < .05).
Discussion
The aim of this study was to assess the factors associated with diet quality of children aged 6 to 23 months in Rongai subcounty compared across the low and high agricultural potential areas during the lean season. Diet quality was determined by MAD, a composite indicator of MDD and MMF. There was no difference in MAD and MDD between the 2 agricultural potential areas. However, MMF was different across the 2 zones where children from low agricultural potential area were fed more frequently. Some of the factors that were associated with diet quality of children included mother/caregiver education level, household income, child gender, and slow and active feeding.
Inadequate child feeding practices and poor quality complementary foods are some factors that influence infant and young child growth negatively. 4 Complementary feeding should start at the age of 6 months as recommended by WHO. 12 Nevertheless, many mothers/caregivers did not comply with this recommendation by initiating complementary feeding before the child reached 6 months. In this study, the average age at which complementary feeding was initiated was 4.5 months (Table 1), which was almost similar to Kenya national average age of 4.4 months at which most children start complementary feeding. 2 This early introduction of complementary foods could be attributed to the short maternity leave period provided in Kenya of only 3 months. Early return to work compels mothers/caregivers to start complementary feeding earlier than the stipulated age of 6 months. This is also observed in Northern Ethiopia where unemployed mothers had a higher chance of timely initiation of complementary feeding since they had no need to return to work compared to their employed counterparts. 20 Poor knowledge on complementary feeding practices could also explain the untimely initiation of complementary foods in this study. This was similar in Ethiopia where lack of information on complementary feeding was associated with untimely initiation of complementary foods. 21 Therefore, educating mothers/caregivers on timely initiation of complementary foods and ways to ensure these foods are nutritious and properly prepared could improve their complementary feeding practices.
Most of the mothers/caregivers in low agricultural potential area cited lack of food as a reason for not preparing special meals for their children (Table 2). This describes the food insecurity and poor economic status of households in low agricultural potential area, which limits their financial access to food. The lack of food could also be explained by the timing of the study which was done during lean season when food availability was a challenge to most households in low potential area. Similar findings were observed in rural Ethiopia where seasonality influenced dietary quality of children. 15
Feeding infants directly is one of the responsive feeding practices that ensure optimal complementary feeding. 19 However, mothers/caregivers from high agricultural potential area considered their children old enough to feed themselves (Table 2), which is contrary to the recommended practice. Mothers/caregivers from high agricultural potential area also forced their children to feed when they refused to eat a particular food, which contradicts the outlined responsive feeding recommendations. 22 Nevertheless, these mothers/caregivers combined that particular food with other foods in order to encourage consumption. This is in line with responsive feeding practice recommendation of experimenting with different food combinations, texture, and taste when child refuses many foods. 23
In this study, the proportion of children who attained MDD (Figure 2) was slightly higher (56.9%) than the Kenya national figure of 41%. 2 Notably, the MDD was not different across the 2 agroecological zones. This was similar to findings from a study in Eastern Kenya where differences in agroecological zones did not affect child diet diversity. 24 However, it was noted that food consumption patterns (Table 3) were not different from national trends where diets were mainly based on starchy staples (80%) and dairy products (90.5%) with less consumption of eggs (17%) and flesh foods (21%). 2 The food consumption patterns of children in the present study are also similar to that of Southern Benin where starchy staples were widely consumed (99.2%) while only 2.1% of children consumed eggs. 25 The same consumption pattern was observed in Western Kenya. 26 The sample size of children who consumed fleshy foods was however very small; hence, a difference in consumption between the agroecological zones could not be clearly reflected. Low consumption of fleshy foods such as meats is a poor complementary feeding practice since infants and young children require fleshy foods for optimal growth and development. This was observed in a study by Krebs et al 27 where consumption of meats was associated with reduced chances of stunting and wasting.
The consumption of plant protein was also relatively low (21%), which was comparable to the national figure of 20.5%. 2 The high intake of starchy staples by the households is attributed to farm production of mainly starchy staples as reported in our previous study. 11 Poor mother/caregiver knowledge on the importance of a diversified diet for children is also a plausible explanation. Similarly, the high consumption of dairy products is attributed to the fact that more than half of the households practiced dairy farming 11 that facilitated access to milk. However, this study did not quantify the milk consumed. Low consumption of fleshy meats could be ascribed to their relatively high cost, making these food groups less accessible in most households due to poor economic status as reported earlier in Malawi. 28 Mothers/caregivers from this study cited that due to the high market value of eggs, they would rather sell the eggs so as to purchase vegetables that will feed the whole family for 2 meals. This necessitates behavior change communication intervention to educate mothers/caregivers on the importance of animal source foods and encourage incorporation of high biological value protein sources such as eggs and fleshy meats in the child’s diet.
Furthermore, most children in this study met the requirements of up to 2 to 4 main meals with at least 1 snack per day (Figure 1), as recommended by WHO guidelines. 12 Interestingly, more children from low potential area (91.1%) met higher meal frequency per day compared to those from high potential area (75.2%; Figure 2). A possible reason for this could be that more mothers/caregivers in high potential area are formally employed, thus requiring them to be away from home for long periods and consequently having less time to feed their children more frequently. This is similar to findings from a study in Ethiopia where employed mothers/caregivers fed their children less frequently. This is because employment requires them to stay in the work place that separates them from their children for long periods of time. 29 However, the type of mother/caregiver employment was not investigated in this study. Generally, the proportion (81.8%) of children meeting MMF in the study was almost similar to a study carried out in Nairobi, Kenya, with 76% of the children attaining MMF. 30
The rates of children who received MDD, MMF, and MAD in this study were slightly higher than the Kenya national rates of 41%, 51%, and 22%, respectively. 2 Although a higher proportion of children achieved MDD and MMF, only a small proportion of them achieved MAD (Figure 2). This shows that although many children were frequently fed, their diets were not diverse to enable them achieve MAD. This could contribute to their diets not meeting the nutrient requirements during complementary feeding period and eventually lead to poor nutritional status. The mothers/caregivers need to be educated on the importance of diversified diets to children and how to ensure that the complementary diets meet the MDD requirements.
Factors that were associated with MDD of children across the 2 agroecological zones included education level, household income, slow feeding, and MMF. Children from low potential area who were fed slowly were 3 times more likely to eat a diverse diet. Thus, paying attention during feeding and doing it slowly and patiently while encouraging the child to eat without forcing them could be an important factor contributing toward consuming a diverse diet. This is in line with the principles of responsive feeding which include feeding infants directly and assisting older children when feeding themselves together with feeding patiently and slowly without force feeding. 19 However, this study did not further assess the extent to which slow feeding contributed to child’s diet diversity. Hence, this finding requires further investigation to understand the mechanism and extent to which slow feeding of children contributes to dietary diversity.
Mother/caregiver educational level is recognized as an important factor that contributes to diet diversity of a child. This was also demonstrated in the present study where mothers/caregivers from low potential area with high education level were 3 times more likely to feed their children with a diverse diet (Table 4). This could be explained by the known observation that educated mothers/caregivers are more likely to know more about child feeding practices and understand messages on the same. This concurs with findings from studies in Ethiopia, Western Kenya, Nairobi, and Tanzania. 20,31 -33 Similarly, high household income in low potential area increased the chances of meeting MDD requirement for the child since high income increases economic access to a variety of foods in the household. Solomon et al 34 also reported that households with high income were more likely to feed their children with a diverse diet. In the current study, achieving MMF was associated with MDD, which implies that children who met MMF requirement from low potential area had an increased chance of achieving MDD, while those from high potential area had a decreased chance of achieving MDD. Most mothers/caregivers from low potential area reported feeding their children themselves (Table 2), which would allow them to ensure that the frequent meals that a child consumes are diverse. This also explains why children from low potential area who ate a diverse diet were more likely to attain MMF.
On the contrary, mothers/caregivers from high potential area reported that their child was fed by someone else other than themselves (Table 2); therefore, no attention was given to diet diversity. Furthermore, a common child feeding practice observed in this study area was the preparation of porridge for the child in the morning in large amounts, which is then used to feed the child on demand throughout the day. The child will then be fed by whoever is left in charge of feeding him/her, which is usually the older sibling. This would therefore contribute to meal frequency but not diversity and explains why children who did not consume a diverse diet in high potential area were likely to achieve MMF compared to those who consumed a diverse diet. This finding however differs with a study in Western Kenya, which showed that households in high agricultural potential area often meet MMF requirement due to readily available food compared to low potential area. 26
Other factors that were associated with MMF included active feeding of children and gender. Male children from high potential area were more likely to be fed frequently than their female counterparts. This could be explained by the common traditional practice that discriminates on female feeding with the sense that the male child needs more food than the female as observed in a study in Eastern Ethiopia. 35
Conclusion
This study demonstrated that the factors associated with diet quality of children aged 6 to 23 months were specific to agroecological zones of Rongai subcounty. These factors included mother/caregiver educational level, household income, child gender, and slow and active feeding of children. There are positive indications in diet diversity and meal frequency of children since most of the children were able to meet MDD and MMF requirement. The study households are predominantly smallholder farmers; hence, agriculture extension workers should strengthen the training of mothers/caregivers on farm diversity and kitchen gardening in order to improve availability and access to more diverse and nutritious foods. There is also a need for behavior change communication and nutrition education of mothers/caregivers on proper infant and young child feeding practices and participatory cooking trainings/demonstration on proper preparation of nutritious complementary foods. These interventions should be designed specifically for low and high agricultural potential areas due to the different dynamics observed in the study. One limitation of the study is the cross-sectional design that may not account for possible seasonal variation, which may influence diet quality and thus the need for a study during different seasons.
Footnotes
Authors’ Note
S.K., D.M-.M., R.R., C.T., N.C., and M.C. conceived and designed the study. S.K., D.M-.M., R.R., and M.C. participated in data collection and analysis. S.K. drafted the manuscript and D.M-.M., R.R., C.T., N.C., and M.C. provided the expertise and critically reviewed the manuscript. All the authors interpreted the data and revised and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by UKAID, the Department for International Development (DFID) through the Transform Nutrition Research Consortium (PO5243, Aries Code 201448) led by the International Food Policy Research Institute (IFPRI).