
Abstract
Background:
Suboptimal infant and young child feeding (IYCF) practices are determinants of poor child nutritional status. In the Democratic Republic of Congo, few children are fed according to international guidelines; this combined with endemic poverty and food insecurity have contributed to the high prevalence of child undernutrition.
Objective:
To characterize IYCF practices and barriers and enablers to optimal child feeding in South Kivu.
Methods:
Focus group discussions, structured and in-depth interviews with women of reproductive age, mothers of children <2 years, and health workers were conducted in 2012 as part of formative research for the US Agency for International Development (USAID)-funded Jenga Jamaa II multiyear assistance program.
Results:
Although breastfeeding was prevalent, few mothers engaged in optimal feeding practices. Barriers included poverty, high work burden, lack of decision-making power in the household, and perceived milk insufficiency. Health provider guidance and mothers’ motivation to breastfeed and feed nutrient-dense foods emerged as facilitators to optimal practices.
Conclusions:
Structural factors, especially long hours working in agricultural fields, impeded mothers’ ability to feed their children optimally. Interventions to address child nutrition and improve IYCF practices should take into account these factors, in addition to food access, nutrition education, and behavior change.
Introduction
The Democratic Republic of Congo (DRC) is one of the few countries where the prevalence of child undernutrition has actually increased in recent years. In 2001, it was estimated that 38% of children under 5 years were stunted, and in 2010, this estimate had increased to 43%. 1,2 In addition to the increasing prevalence of chronic undernutrition, 10% of children under 5 and 13% of children under 2 are wasted. 3 In the DRC’s eastern provinces, the health and nutritional status of the population have been impacted by years of armed conflict and instability. An estimated 5.4 million people died during a 10-year armed conflict, mainly from disease and malnutrition. 4 Although the war ended in 2004, fighting has continued in North and South Kivu, and prevalence of wasting has remained high. 5 South Kivu used to be a major producer of food for the DRC, but food production has been impacted by looting of crops, general insecurity, and poor infrastructure. 6 The impact of ongoing insecurity on agricultural and pastoral practices has resulted in widespread food insecurity, and the higher child morbidity and mortality may be due to the conflict’s economic effects as well. 6,7 Yet growing evidence suggests that suboptimal infant and young child feeding (IYCF) practices may be a major contributor to the high prevalence of chronic undernutrition in eastern DRC. 6 –8
Optimal practices include exclusive breastfeeding for the first 6 months of life and continued breastfeeding at least until 24 months with age-appropriate complementary foods that are adequate in quantity and quality. 9,10 Failure to exclusively breastfeed for the first 6 months increases the risk of morbidity and mortality from diarrhea and pneumonia. 10 Infants between 6 and 18 months of age are in a critical period for growth, as this is the period when complementary foods become an increasingly important part of the diet. 11 If infants do not receive adequate energy and micronutrients from complementary foods in addition to breast milk, they are at high risk of growth faltering during this time. 11 This age-group is also vulnerable to infectious diseases, which combined with poor complementary feeding have a negative impact on growth. 10 Because most stunting incidence occurs in these first 2 years, it is often considered the most important period in which the quality of children’s diets should be ensured. 10
Nationally, breastfeeding is highly prevalent (95%) in the DRC, however, only 48% of children are breastfed within the first hour after birth and therefore miss the nutritional and immunological benefits of colostrum. 3 Only 36% of children are exclusively breastfed for the first 6 months following World Health Organization (WHO) and United Nations Children’s Fund (UNICEF) recommendations, and older children often being fed only 1 meal per day. 3 Suboptimal breastfeeding practices may be associated with the large number of deaths from common childhood illnesses such as diarrhea and pneumonia in the DRC. 12 In South Kivu province, considerably more infants (40%) are fed something other than breast milk in the first 3 days compared to the national average (17.5%), and only 18% of infants 6 to 23 months in South Kivu had received a minimum acceptable diet of complementary foods, which is measured by minimum dietary diversity and meal frequency. 3 Exclusive breastfeeding for the first 6 months is promoted by the DRC Ministry of Public Health, with education and support provided to mothers during antenatal and postnatal consultations. 8 However, more than one-third of women do not have access to a health clinic and are thus not receiving information on optimal IYCF practices. 8
Aside from lack of access to services, there is little understanding of other factors that may be contributing to suboptimal IYCF practices in eastern DRC. Using multiple methods, this study sought to characterize IYCF practices, as well as identify barriers and facilitators to optimal practices, among mothers of children under 2 years of age in Uvira and Fizi territories in South Kivu, DRC.
Methods
Setting
The study was conducted in March and April 2012 in Uvira and Fizi territories and served as formative research to inform the design and implementation of Jenga Jamaa II nutrition interventions. Jenga Jamaa II is a US Agency for International Development (USAID)-funded multiyear assistance program implemented in South Kivu by the Adventist Development and Relief Agency (ADRA) and World Vision, and its objective is to improve household food security and child nutritional status. The original study was intended to assist ADRA with the design of appropriate behavior change communication messages related to nutrition and inform the implementation of Care Groups, following the Prevention of Malnutrition in Children under Two Approach (PM2A), which included promotion of health service utilization and provision of food aid rations for pregnant and lactating women and infants 6 to 23 months of age.
The study area included 10 rural villages in the Jenga Jamaa II catchment area from 3 major agroecological zones: highlands (Lemera, Katala, and Ndolera), lowlands (Ndunda, Katogota, and Kigurwe), and lakeside (Ake, Kenya-Plage, Sebele, and Swima). The lakeside villages were in Fizi territory, and the highland and lowland villages were in Uvira territory. Sites were selected with input from ADRA, based on the security situation at the time, travel and accessibility considerations, and the general comparability of the communities to others within ADRA’s program area. Study participants were a convenience sample of Jenga Jamaa II program beneficiaries (women of reproductive age), PM2A care group lead mothers, and government health workers who lived relatively close to the health centers where the data collection occurred. Oral informed consent was obtained for all participants. Ethical approval was provided by the institutional review board of the Johns Hopkins Bloomberg School of Public Health and the Ministry of Health of South Kivu, DRC.
Data Collection
In each study site, the following research methods were used: (1) focus group discussions (FGDs) with mothers of children <24 months of age and women of reproductive age, (2) structured interviews among mothers with children <24 months of age, and (3) in-depth individual interviews with health workers and lead mothers.
Focus group discussions were conducted among 2 separate, but related, respondent groups: mothers of infants <24 months of age and women of reproductive age (18-45 years). There was 1 FGD per respondent group for each of the 10 study sites for a total of 20 FGDs and 188 participants. Participants were informed of the purpose and general domains of the FGD and then they were invited to discuss the topic of IYCF practices. The facilitator allowed the group to lead the discussion so that flow of the conversation was natural and topics of particular salience to the group were explored in depth. Focus group discussions were conducted in Swahili and lasted approximately 2 hours. Focus group discussions were audio-recorded, and a note taker was also present.
Structured interviews among mothers of infants <24 months of age were also conducted, with a questionnaire focused on IYCF knowledge, attitudes, and practices. Interviewers received training on the survey questionnaire, and the interviews were approximately 60 minutes in duration. A total of 119 structured interviews were conducted across the 10 sites.
In-depth interviews (IDIs) were conducted among government health workers and lead mothers. A note taker was present to record responses, and interviews were also audio-recorded. The IDIs with health workers and lead mothers were used to understand their roles in providing health and nutrition information and their own knowledge and perceptions of practices related to nutrition and care in pregnancy and IYCF practices. A total of 43 IDIs were conducted across the 10 sites.
Data Analysis
All interviews and FGDs were conducted in Swahili and transcribed in French. The analysis was conducted in English by a bilingual French/English speaker. For FGDs, the note taker for each FGD listened to the taped discussion and completed notes for each group discussion. Direct statements of respondents were written verbatim when they were describing their perceptions and feelings about specific behaviors. Upon completion of each FGD report, responses were consolidated across all FGDs according to major headings and subheadings of the FGD guide. Responses were reviewed for patterns and trends.
For the structured interviews of mothers of infants <24 months of age, quantitative analysis methods were used and means and frequency distributions were examined. Feeding practices were stratified by infant age-group (0-5 months, 6-11 months, and 12-23 months) in the analysis.
For the IDIs, each interviewer listened to the tape of the interview and completed their interview notes. Notes were organized by each of the major themes captured by the IDI guide, and a report was completed for each IDI. Upon completion of each IDI report, responses were consolidated across all interviews, and salient themes were assessed.
Results
Background and demographic characteristics of the 119 mothers of infants <24 months are described in Table 1. The mean age of mothers was 25.8 years, and the mean age of their infants was 7.9 months. Almost half of the mothers were literate (44%), however, around 28% had never attended school. Most mothers were married (86.6%), and the majority were from the Mufulero ethnic group (59%) followed by the Kibembe ethnic group (30%). Most of the mothers reported small businesses (47%) and agriculture (46%) as sources of income for their households.
Background Characteristics of 119 Mothers of Infants <24 Months.
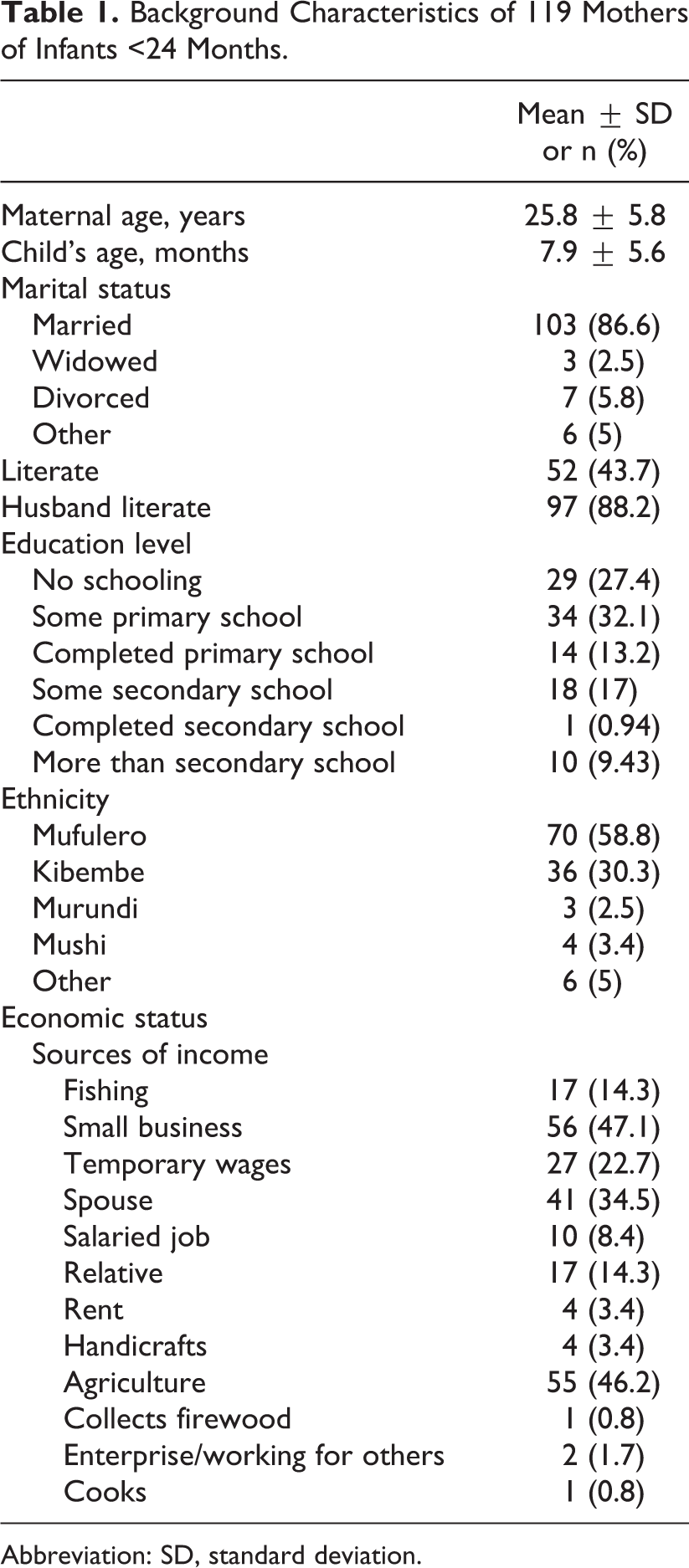
Abbreviation: SD, standard deviation.
Infant and Young Child Feeding Practices
Initiation of breastfeeding
A summary of the frequency of mothers reporting key IYCF practices is displayed in Figure 1. About half of the mothers reported initiating breastfeeding within an hour of childbirth, and 37% reported feeding their infant colostrum. Various explanations for the benefits of mohondo, or colostrum, included the following: it cleans the stomach, gives intelligence to the child, gives energy, contains vitamins and protein, protects the child from disease, and helps the “white milk” to come in. Although traditionally their grandparents would discard colostrum, many women attribute their knowledge of colostrum’s benefits to advice coming from the health center (nurses, midwives and community health workers): At the health center they tell us to give the milk right away because it helps the child to grow. Before [health center counseling] we used to throw out the first milk. (Mother of child <24 months, FGD)
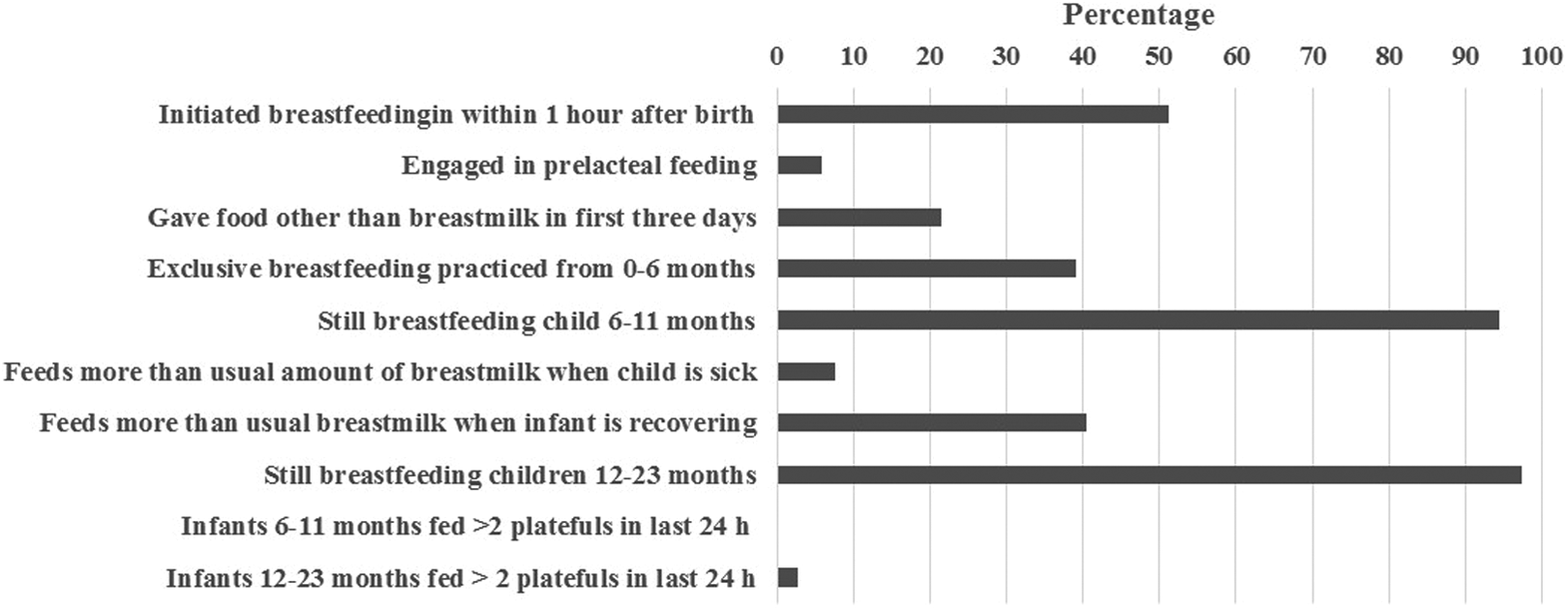
Frequency of Key IYCF Behaviors Reported by 119 Structured Interview Respondents (mothers of infants < 24 months).
Exclusive breastfeeding
Several months after birth, about 20% of women reported difficulty breastfeeding. The main reasons included feeling there was not enough breast milk, not having the time to feed the infant, pain, plugged milk duct, and mother or baby becoming ill. A few reported giving sugar water or asking another woman to breastfeed instead, because they felt as though they lacked breast milk since they were unable to see milk “running out.”
The duration of exclusive breastfeeding was short due to the common practices of giving infants water and early introduction of complementary foods. About half of the mothers interviewed felt that water should be given to infants <6 months of age when the weather is hot (54%), and 41% of the mothers reported giving their infants under 6 months of age water on the previous day. In all of the sites, children commonly receive porridge and other semisolid foods before 6 months of age. Mothers explained that a child’s cry indicated that they were not satisfied during or after breastfeeding. This, combined with mothers’ perceived inability to produce enough milk, led them to introduce foods generally within the first 2 to 3 months of life. Mothers felt encouraged in this practice when children stopped crying after being given food. “When the child cries, the child is hungry” was frequently voiced as well as the belief that giving porridge makes children “calm.” Several mothers discussed this practice: He cries, he cries, you give milk and he isn’t satisfied. (Mother of child <24 months, focus group participant) If you give the porridge his eyes follow the porridge and he takes it and is satisfied. (Mother of child <24 months, focus group participant) I take tea at 6 [AM], arrive at the field at 8. When I return home, I find that he has cried all day so I am obligated to give porridge. (Mother of child <24 months, focus group participant).
Complementary feeding
In general, porridge was introduced to children first, followed by food the family eats (cassava, fufu, and sombé) between the ages of 7 and 12 months. Women felt that the children’s crying indicated when they were ready for complementary foods. As one woman explained, she started feeding her child porridge at 6 months. At 7 months, she started giving fufu because her child cried frequently with just porridge, and she assumed he was not satisfied. Other women said the point at which the child refused to take porridge any longer was indicative of when to introduce family food.
Cassava flour was often used to make porridge and involved cutting manioc into pieces and soaking it in water for at least 24 hours to reduce the cyanide content, followed by drying it in the sun and then pounding it into flour. Most often, porridge consisted of only cassava flour and water, while access to other flours varied depending on location. In the lowlands, sorghum, maize, cassava, soybean, and rice flours were used and several were mixed to prepare porridge, but this practice was not found in the other sites. In the highlands, porridge made from green plantain flour was frequently used. The technique involved drying sliced green plantains in the sun and then grinding them into flour.
There is little variety among foods in the diets of children 6 to 12 months old. In the group discussions, mothers cited sugar as the ingredient most commonly added to porridge. A small percentage of mothers mentioned adding meat/fish (20%) or eggs (19%) to enrich the porridge. A slightly higher percentage of mothers mentioned adding colorful fruits and vegetables (24%), milk (26%), soy flour (30%), or sugar (23%) to make the porridge more nutritious. When asked what variety of foods should be in a 6- to 12-month-old child’s diet, less than half the mothers mentioned fish (20%), eggs (42%), yellow vegetables (38%), meat (41%), or green leafy vegetables (60%). Although some mothers had favorable attitudes toward adding nutrient-dense foods to their children’s diet, 87% of mothers felt that the high cost of these foods made it difficult for her to obtain them.
Children eat what the family eats, as one mother said, “we give children what we have.” A health worker explained that it is challenging to diversify children’s diets: A lot of mothers know that they must add soybean flour, peanuts, fish, sugar, sorghum to porridge, and fruits like avocado and banana, but it is not done because many households are very poor. (Health worker, IDI)
Families with livestock do not appear to be giving their children the meat and milk from the cows and goats, and this may have been because they preferred to sell animal products to supplement their incomes. The little meat they eat is generally purchased. Milk was not reported as a food frequently given to children, though it was commonly sold in plastic water bottles along the road in towns.
In the day prior to the survey, 44% of 6- to 11-month-old infants and 86% of 12- to 23-month-old infants were fed fufu (Figure 2). Cassava or maize porridge was the second most common food that was fed the previous day for infants 6 to 11 months of age, and beans and green leafy vegetables were the second most common foods fed to infants 12 to 23 months. Fish was the main animal source food fed to both age-groups in the previous day. Over half of the children 6 to 23 months of age had not yet been given eggs, yellow fruits or vegetables, or meat. More than 40% had not yet been fed legumes or fish. Among the infants who had already been introduced to the foods, 9 months was the median age when meat was introduced and 8 to 8.5 months was the median age for yellow fruits and vegetables, green vegetables, legumes, eggs, and solid food. Fish and semisolid foods were first introduced at a median age of 7 months, whereas porridge was introduced at about 6 months of age.
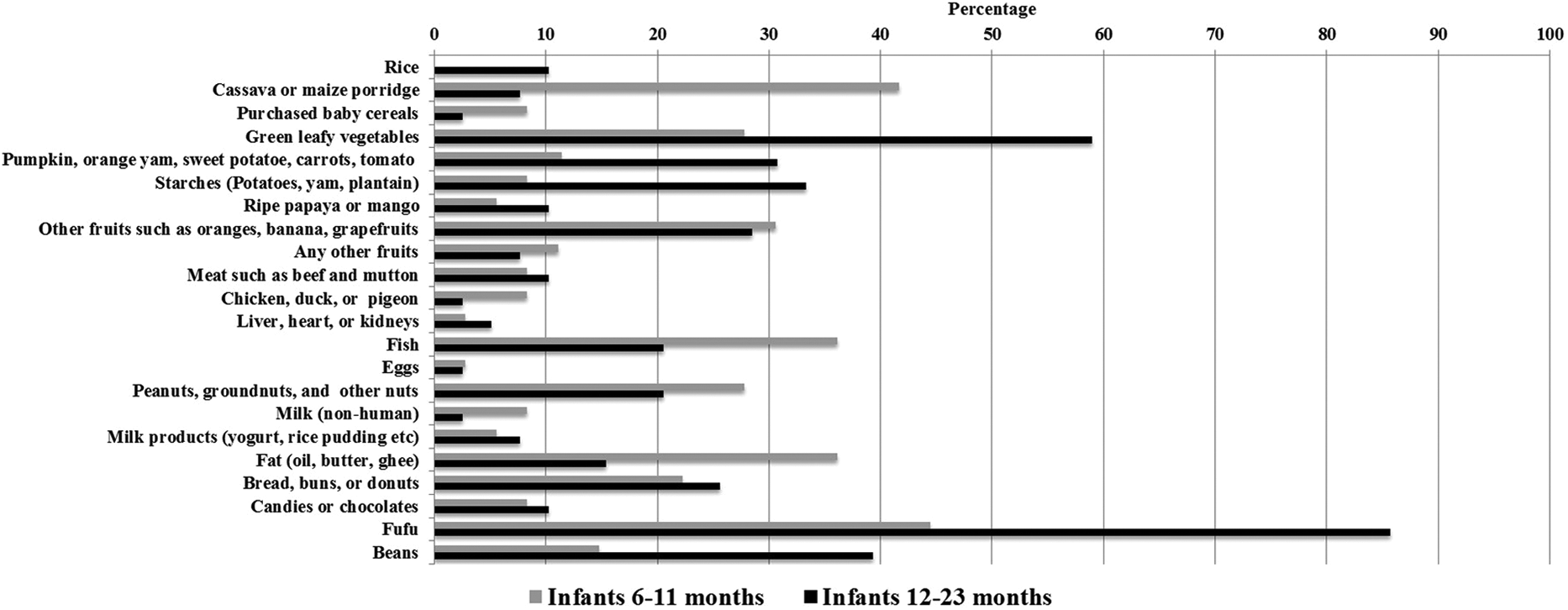
Frequency of reported consumption of selected complementary foods for infants 6–11 months and 12–23 months of age on the previous day reported by 119 structured interview respondents (mothers of infants < 24 months).
Changes in feeding behaviors as children grow older
Few changes are made to the diets of children as they grow older. Children of any age tend to eat porridge or family foods according to the family schedule, with meals occurring twice per day. Fufu is fed to the child by hand, whereas porridge is generally served using a spoon and a gobelet (cup). Once the children are capable of feeding themselves, they are given their own plastic bowl.
Although measurement of specific quantities of food is not precise, a guigoz (tin can) was used to measure flour at the market. Mothers described how they take flour by the handful and put it in the cooking pot with water. One mother estimated using about a handful of flour when preparing porridge. When describing the amount consumed, spoonfuls and tartine (oval-shaped ball of fufu) are commonly used units of measure. Several mentioned giving 2 to 3 spoonfuls of porridge when they first introduced food. When serving family food, or fufu, they talked about giving a child 1 tartine, which is created using a plastic bowl and shaping the fufu against the side of the pan. Few concrete units are used to describe the quantities of food given to children when they begin eating with the family. Children are left to eat until they are satisfied or refuse to eat anymore: We don’t have quantities of food. We put the food there in front of them and they eat until they are satisfied. (Mother of child <24 months, FGD)
Compared to children 6 to 11 months, children 12 to 23 months were given less porridge and more fufu, green leafy vegetables, vitamin-A-rich fruits and vegetables, starchy vegetables, and beans. The other food categories were consumed in similar quantities. The majority of children did not receive cow and goat milk, which highlights the importance of continued breastfeeding for children in this context. It is very common for children to be breastfed well into their second or third year of life: I have six [children]. This is my ninth born. I let my child continue until they decide they are done breastfeeding. (Mother of child <24 months, FGD)
Barriers to Optimal IYCF Practices
Women’s workload
Women’s workload required them to either tend to crops they cultivated or gather food from fields on a daily basis. Often, they left their children for hours in the care of nannies, neighbors, or family members who commonly offered porridge to soothe the child when crying, and this was a frequently cited reason for early introduction of complementary foods. Although not a widely adopted practice, there were a few women across the study sites who reported carrying their child with them to the field in order to practice exclusive breastfeeding. There were mixed responses from women as to whether they felt they could take their children with them to the field. Factors such as distance to the field, conditions in the field, and the load the women have to carry were reported as concerns. Another success strategy for exclusive breastfeeding offered by women was returning from the field every few hours to breastfeed.
Poor maternal dietary intake and perceived milk insufficiency
Mothers attributed their inability to produce enough milk to not eating well in nearly every site. Some explained that with not eating all day—just consuming some water and a piece of cassava—they are unable to produce enough milk. Most women reported their child cried during or after feeding, and this lead them to think that their milk production was insufficient. Mothers often gave porridge to stop a child from crying: If they cry a lot I give porridge at two or three months [of age]. I breastfeed but he cries a lot and that makes me think it isn’t satisfying. (Mothers of children <24 months, FGD)
Poverty and lack of financial decision-making power
Power over decision-making within households influenced what foods were prepared, who eats different kinds of foods, and how money was spent. Men controlled finances and made decisions on how money should be spent, in addition to certain decisions regarding health and nutrition practices. Of those in the house, 64% of women interviewed said their husband advised them on matters related to child feeding and health. Over half (53%) of the mothers said they decided what to cook on a daily basis, whereas in 37% of households, husbands made this decision. Women described how the peanuts they cultivated were sold by the husband at the market, and, therefore, they did not consume or benefit from the income. The majority of women felt they had to consult their husbands about what to do with even a small amount of savings, and over 70% of women consulted their husbands about financial decisions.
Poverty and lack of purchasing power inhibited mothers’ ability to diversify children’s diets. As one mother explained, if she had the ability, she would add fish, peanut flour, sugar, and salt, but she rarely has the means, as “We can go one month without putting other things in porridge.” Eighty-seven percent of mothers said the cost of meat, milk, eggs, fruits, and vegetables makes it hard for them to provide these foods to children. Mothers recognized a difference in the way children eat depending on the ingredients used: When I give fufu with meat my child eats with an appetite. When I put condiments in the sauce my child eats well, my child eats more. If we give porridge we need to add sugar as that will improve the taste and the child will eat with strength. (Mothers of children <24 months, FGDs)
Lack of knowledge
A common misconception among mothers was that infants need water in addition to breast milk. Half of the women interviewed felt that water should be given to infants less than 6 months of age. Additionally, many mothers believed that breastfeeding while pregnant would negatively impact the health of the child, and pregnancy was a common reason for cessation of breastfeeding. One mother explained that she stopped breastfeeding her child upon becoming pregnant for fear of “spoiling” the skin of her child. Two women from different communities explained that they found the color of their milk changed from yellow to a clear color indicating bad milk and feared this would hurt their children. Another woman explained that her child would become “bwaki” (malnourished) if she continued to breastfeed while pregnant.
Lack of knowledge of how to enrich children’s meals was a barrier to improving complementary feeding. Many mothers reported not knowing they could add palm oil, avocados, bananas, mangos, mashed beans, and pounded peanuts to porridge. However, they expressed strong interest in learning how to prepare a variety of porridges and snack foods for the children. Availability of and access to food varied by location, affecting what could be added to porridge. In the highlands, corn, beans, and bananas were most commonly grown, and in the lakeside villages, bananas, fish, and palm oil were widely available. In the plains and lowlands, cereals, including sorghum, maize, and rice, along with tubers (cassava and sweet potato), legume (peanuts, beans), and vegetables including cabbage, eggplant, tomatoes, and onions were grown. One mother reported adding pounded dried fish to porridge made of banana flour, as fish were easily sourced in the nearby lake. In further explorations of some of the locally available options, mothers felt that on occasion, and more regularly during harvest season, they could improve complementary foods by adding some foods to the porridge or giving them as a snack. Of all the foods mentioned, palm oil, avocado, and banana came up as the most frequently foods that could be added to porridge. A few mothers said they give fruits to children because they were told it helps with defecation and/or preventing constipation.
Facilitators of Optimal IYCF Practices
Healthcare provider guidance
Healthcare providers play a large role in positively influencing women to adopt recommended practices. Clinic healthcare workers and community health workers were described as caring by 37% of mothers, well trained to counsel on child feeding by 26% of mothers, and highly intelligent by many mothers. Almost all (94%) of the mothers said they trusted the health worker’s advice about child health and feeding, and many regarded them as their most credible source of advice on matters related to pregnancy, lactation, and child care practices.
Motivation to practice optimal feeding practices
Despite the numerous barriers they are faced with, the mothers were extremely motivated to breastfeed and incorporate more diverse, nutrient-dense foods in their diets. They expressed a general feeling that breastfeeding children result in growing well and having good health. Several mothers stated that when an infant asks, “it is their right” to be breastfed. Mothers reported feeding both day and night, and some women said their children nursed so frequently at night that they have nothing left in their breasts in the morning. In fact, most mothers said they feed on demand or “each time the child asks,” often described as when the child cried. Frequent associations were made between a mother’s eating habits and her ability to breastfeed ultimately affecting the child’s health. One mother shared her perspective on this: When milk is plentiful the child will eat well [and for this] the mom needs to eat well to feel satisfied. (Mother of child <24 months, FGD) Eating fufu and sombé (cassava leaves) we are only satisfied. Adding ingredients like oil, peanuts, green onion, salt are what we wish to add to the sombé and this means we are eating well. (Mother of child <24 months, FGD)
Discussion
Breastfeeding was practiced universally in our sample of mothers in this area of South Kivu, and most mothers continued to breastfeed their infants to 24 to 36 months of age. However, many mothers believed that water was important for infants’ health, thus early introduction of liquids and semisolid foods resulted in a low prevalence of exclusive breastfeeding during the first 6 months of life. The complementary foods most commonly introduced consisted of only cassava flour and water, which is of poor nutritional quality. Fufu is introduced later but does little to improve the quality of children’s diet. Older children in the sample tended to eat what the rest of the family eats, with high-protein animal source foods often reserved for male adults. Children 12 to 23 months received more beans, vitamin-A-rich fruits and vegetables, and starchy vegetables compared to those less than 12 months of age.
The main barriers to optimal IYCF practices included lack of knowledge and misperceptions among mothers, poverty and mothers’ high work burden, and mothers’ lack of purchasing power and power over decision-making in the household. The most common misperceptions to emerge in our findings were that infants needed water on hot days as well as the inadvisability of continued breastfeeding after becoming pregnant again. A barrier to optimal breastfeeding frequently reported was poor maternal dietary intake, which was perceived to inhibit milk supply. Women’s workload emerged as the strongest barrier to achieving optimal IYCF practices. Women often had work obligations that required them to leave their children in the care of others, and many women interviewed said their housework made it hard for them to spend enough time encouraging their child to eat. Nearly half of the women interviewed felt it took too much time to reheat leftover food. Poverty was the other most frequently cited barrier to optimal IYCF practices. Women’s lack of purchasing power affected their ability to feed themselves in a way they perceived as adequate or to provide nutrient-rich foods to their children. Foods grown by the household were more often sold for additional income than consumed by the family.
The main facilitators to optimal IYCF practices that emerged were the healthcare providers. According to mothers, healthcare providers were accessible and played an important role in influencing them to adopt positive practices. Women’s desire for their children to be in good health was also a facilitator for optimal practices, however, their intentions to feed their children better quality diets were often impeded by the barriers described. Good maternal nutritional status was perceived as a facilitator to breastfeeding, as mothers believed their poor diets contributed to milk sufficiency. Geographical location also served as a facilitator for the inclusion of certain complementary foods in children’s diets, with nutrient-rich vegetables most widely available in the lowlands/plains villages where they are grown and fish more commonly consumed in the lakeside villages.
To our knowledge, this is the first study to explore IYCF practices in eastern DRC and to identify barriers and enablers to optimal practices. One study in the Katana and Walungu health districts in South Kivu showed that community health promoters can improve rates of exclusive breastfeeding; however, at 6 months, only 58% of infants in the intervention group were exclusively breastfed, indicating that other barriers to exclusive breastfeeding should be addressed by interventions. 8 A randomized controlled trial of ready-to-use complementary food in South Kivu found no difference in nutritional status between the intervention and control group infants, and the authors hypothesized that nutrient absorption may be impeded by environmental enteropathy and the presence of antinutrients such as phytates commonly found in complementary foods in this population. 13 The same study showed that breast milk intake of infants was not affected by complementary food intake. 14 One study on child feeding practices in Kinshasa, the capital of the DRC, found that mothers also believed that children should be given water in hot weather and believed that water was needed to digest breast milk. 12 Among mothers in Kinshasa, formula was frequently used to supplement infants’ intakes due to the belief that children were not getting enough breast milk. 12 No mothers in our study reported formula use, and in the rural areas, it was not even available for purchase.
The main limitation of the study is that the sites chosen were relatively close to health clinics, and therefore, the sample was not necessarily representative of the population served by the program. Women living farther away from healthcare services may have had poorer knowledge of optimal IYCF practices, as healthcare providers were a main source of women’s knowledge in this population.
Conclusions
This study adds contextual understanding to the high rate of chronic undernutrition in the DRC, which may be influenced by the low prevalence of exclusive breastfeeding in the first 6 months and poor complementary feeding practices characterized by lack of dietary diversity and meal frequency. The results show that structural factors, mainly poverty and women’s high work burden, have a strong influence over IYCF practices. Mothers were highly motivated to breastfeed and improve their own diet and that of their children. Poverty, lack of decision-making power among mothers and female caretakers, and the need for women to spend their entire days engaged in agriculture or other income-generating activities impeded their ability to adequately feed their children. Increasing income-generating opportunities for women and introducing labor-saving technology could reduce the time mothers spend working in the fields, allowing them to spend more time caring for their children. It would also reduce the need to sell all crops and livestock rather than consume them in the household, which would increase access to greater quantities of diverse foods. The Jenga Jamaa II programs addressed these factors through the inclusion of rations for mothers, children, and households that were provided as part of the PM2A approach, which may have resulted in some improvements in nutritional status among beneficiaries of PM2A programs. Women’s empowerment groups, focused on financial empowerment, as well as agricultural programs, which introduced labor-saving techniques, were also implemented under Jenga Jamaa II, with the objective of addressing some of the structural factors contributing to poor nutritional status of the population and reducing women’s high work burden.
Footnotes
Acknowledgments
The authors wish to thank both the Adventist Development and Relief Agency (ADRA) and World Vision (WV) headquarters and South Kivu field staff for their administrative and logistical support throughout the research. Special thanks to the interviewers, focus group facilitators, and note takers for their diligent efforts to collect the data. They would also like to acknowledge the donor, USAID’s Office of Food for Peace for the funding of this research as part of the Development Food Assistance Program, Jenga Jamaa II.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors would like to thank ADRA for their financial support to Johns Hopkins University in carrying out the research and publication of this article. This funding was made available through a USAID Office of Food for Peace Cooperative Agreement (AID-FFP-A-11-00006).