
Abstract
Background:
Contaminated complementary foods are associated with diarrhea and malnutrition among children aged 6 to 24 months. However, existing complementary food safety intervention models are likely not scalable and sustainable.
Objective:
To understand current behaviors, motivations for these behaviors, and the potential barriers to behavior change and to identify one or two simple actions that can address one or few food contamination pathways and have potential to be sustainably delivered to a larger population.
Methods:
Data were collected from 2 rural sites in Bangladesh through semistructured observations (12), video observations (12), in-depth interviews (18), and focus group discussions (3).
Results:
Although mothers report preparing dedicated foods for children, observations show that these are not separate from family foods. Children are regularly fed store-bought foods that are perceived to be bad for children. Mothers explained that long storage durations, summer temperatures, flies, animals, uncovered food, and unclean utensils are threats to food safety. Covering foods, storing foods on elevated surfaces, and reheating foods before consumption are methods believed to keep food safe. Locally made cabinet-like hardware is perceived to be acceptable solution to address reported food safety threats.
Conclusion:
Conventional approaches that include teaching food safety and highlighting benefits such as reduced contamination may be a disincentive for rural mothers who need solutions for their physical environment. We propose extending existing beneficial behaviors by addressing local preferences of taste and convenience.
Introduction
An estimated 178 million children under the age of 5 in low- and middle-income countries are stunted. 1 Substantial and irreversible linear growth faltering can occur particularly among 6- to 24-month-old children who have developing immune systems and are vulnerable to enteric infection. 2 Inadequate complementary feeding, which includes contaminated foods and water, poor hygiene practices, and unsafe storage and preparation of foods can result in both short- and long-term health, developmental, and economic consequences. 3 Therefore, in addition to ensuring that an infant and young child is receiving the right amount of nutrition at the right frequency, it is important to ensure that complementary foods do not pose a risk of gastrointestinal diseases. 4 –6
Indicator organisms such as fecal coliform 7,8 and fecal Streptococci 9 and specific pathogens such as Salmonella, Campylobacter jejuni, Shigella, Vibrio cholera, and Escherichia coli have all been isolated from complementary foods in Bangladesh 7,9 –15 and complementary foods in other developing countries. 16 In the context of developing countries, contamination levels in food can be higher than the contamination levels in drinking water. 4,5,8,17 –20
The foodborne route is widely considered to be of great importance for transmission for gastrointestinal infections, however evidence linking food contamination to food hygiene practices and health outcomes is lacking. 5,21,22 Poor levels of food hygiene practices by mothers have been linked with diarrhea among children in Vietnam 23 and Indonesia. 24 A recent study in Bangladesh found that 40% of sampled complementary foods were contaminated with E. coli, and consumption of E coli-contaminated food was associated with a higher frequency of reported diarrhea incidence in the past 24h among 6 to 24 months old children. 25
Few interventions have tackled the problem of complementary food safety in developing countries. Based on a review of the literature, we classified interventions to promote complementary food safety into two groups: “deep and narrow” versus “shallow and broad.” In the “deep and narrow” approach, which dominates the literature, the multiple pathways of food contamination are addressed comprehensively but promoted to a narrow subset of the general population for a short period of time. The effectiveness of this first approach in reducing food contamination in the home has been evaluated, 20,26 –28 and several intervention models exist based on this approach. 7,10,20,29 –33 Deep and narrow interventions to promote complementary food safety, conducted in peri-urban Mali, rural Bangladesh, and rural Nepal, promoted multiple effortful behavioral steps directed at mothers: handwashing at 3 different key times, washing plates and utensils with treated water, cooking and reheating foods before consumption, and covering foods with tight-fitting lids. 7,20 A fifth instruction regarding boiling milk was added to the intervention in Nepal (note 1). All of these intervention studies reported decreased levels of food contamination over time among the households who received the intervention.
These intervention studies demonstrate that implementing multiple behavioral steps to ensure food hygiene at the individual level, with close supervision and guidance of a community health worker, can reduce food contamination. However, practicing multiple behavioral steps is inconvenient, and this limits the potential for sustained adoption of the behaviors. 34,35 Moreover, cost-intensive promotional activities are required for such intensive interventions, which further limit the potential for implementation at large scale.
The current study is the first step in an effort to identify and develop a shallow and broad approach to design a candidate intervention that can then be less intensive and possibly exhibit marginal gains but to a much larger target population. Adopting the shallow and broad approach from the outset, we conducted a qualitative study with the aims (1) to understand current behaviors, motivations for these behaviors, and the potential barriers to behavior change and (2) to identify one or 2 simple actions that can address one or few food contamination pathways and have potential to be delivered to a larger population.
Methods
Data Collection
From October 2013 to March 2014, the field team conducted semistructured observations, video observations, in-depth interviews, and focus group discussions (Table 1). The research team divided the study participants into different groups—mothers of 6 to 12 months old children, mothers of 13 to 18 months old children, and mothers of 19 to 24 months old children. The rationale for this division was that children of different ages are fed different complementary foods, and so we wanted to address this variation in our data collection. 36 The research team attempted to interview equal numbers of mothers of children from each category. All data collection, except video observations, were collected by native Bengali speakers with extensive qualitative research experience (including MJR, MN, and FA). Video observations were collected by local recruits.
Summary of Data Collection Methods and Participants.
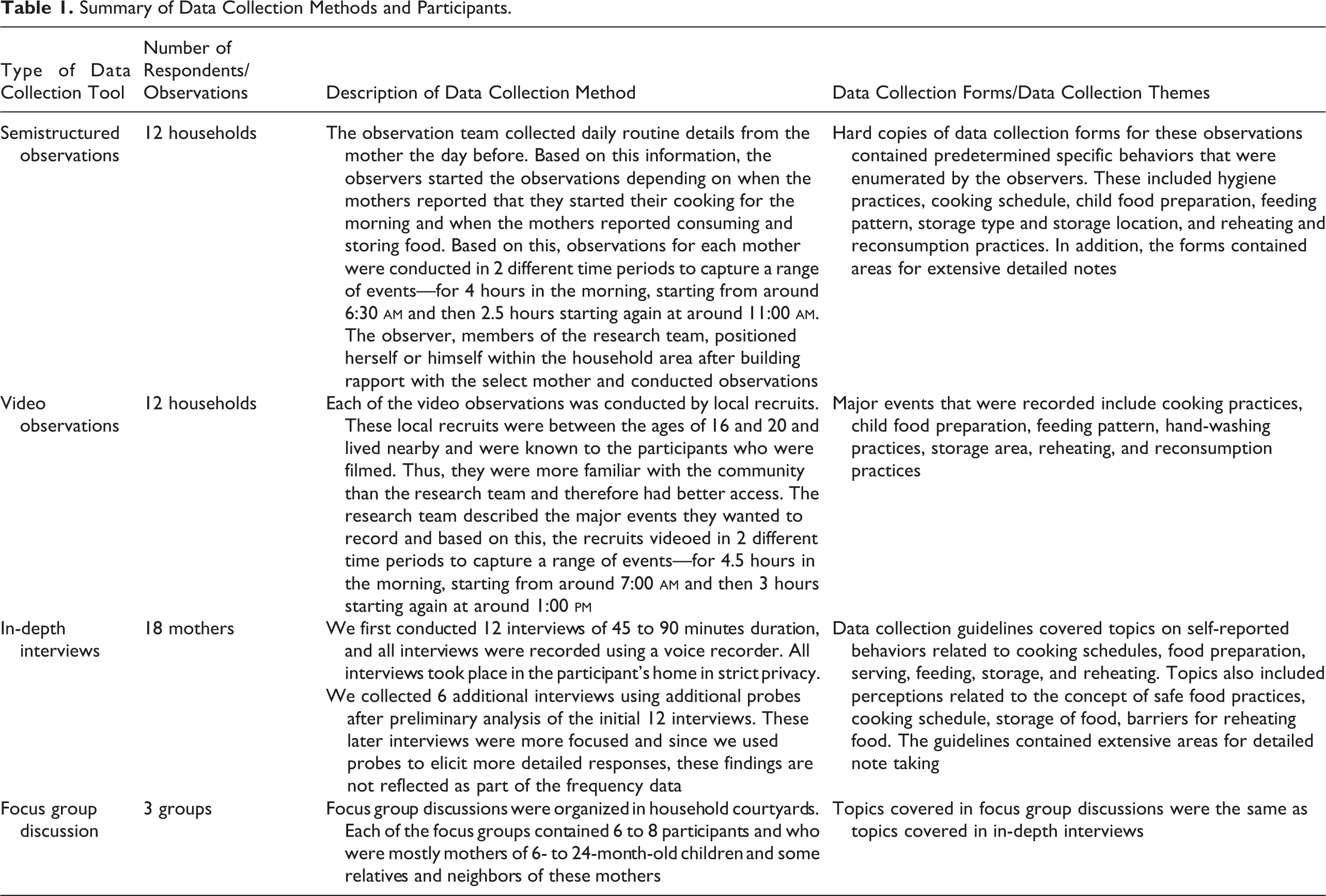
The research team asked mothers included in the video and semistructured observations (24 mothers in total) to provide details about their cooking and routine child care events prior to observation data collection so that the research team could focus on those events. For both the video and the semistructured observations, the observers visited the same mother twice within a day to capture a range of different events that were of interest for the current study. Based on these field notes, the research team generated a composite schedule representing the experience of multiple women.
Study Site and Population Selection
The study team selected rural sites, as significantly more rural households keep food at room temperatures for more than 4 hours in comparison to urban households and significantly higher number of rural households reported not reheating food before second feeding to child in comparison to urban households. 25 The research team purposively selected villages from the Basail and Delduar subdistricts, within Tangail district, because they are easily accessible from the research organization headquarters and fit the rural rather than the periurban profile. Also, records obtained by the research team’s research group (Environmental Interventions Unit, icddr,b) indicated that these subdistricts did not have any externally funded projects promoting nutrition, water, sanitation and hygiene technologies, or behavior change.
Since this study was exploratory and qualitative, we did not attempt to draw a sample representative of the entire population. The research team met with local government officers at the Basail and Delduar subdistricts explained the study purpose, and determined which villages within their subdistricts were low income and also easily accessible by road. Based on their suggestions, we identified 4 villages, 2 in each subdistrict.
For each village, the research team conducted social mapping exercises in collaboration with the local villagers. This built rapport with influential persons in the village and created a list of households that had children aged between 6 months and 2 years. For each village, the research team went door-to-door using the social mapping information, identified, and listed all the mothers of children aged 6 months to 24 months old. Using this list, the team allocated the first 3 participants in each village for semistructured observations, and then the next 3 were allocated for video observation. Three subsequent participants from the list were selected for in-depth interviews. We conducted focus group discussions with the remaining participants in each village.
Data Analysis
Audio data from in-depth interviews and focus group discussions were transcribed verbatim in Bengali and then translated into English transcripts in Microsoft Word. The translators were strictly instructed to transliterate large portions of the interviews that contained local terms and expressions. The final English transcripts therefore contained numerous transliterations so as to retain the original tone of the interviews as much as possible.
Codes were created based on themes chosen prior to data collection according to the study objectives. The research team met regularly during data transcription and translation to aid data familiarization and to generate additional inductive codes from the data. Individual and group interview transcripts were then manually coded and categorized according to these major codes. Although the interviews were coded and categorized individually, we drew inferences from the findings collectively.
The research team reviewed the video observations and made summaries of the series of steps involved in the following events—food preparation, cooking, serving, storing, reheating, and child feeding. Summaries were made in Microsoft Word and included screen shots taken from video footage to provide relevant detail and context. Data from word document summaries were then manually categorized under a priori codes first. Data from the semistructured observations were manually recorded in Bengali and then translated to English. Data from these structured observations were also manually categorized under a priori codes first. As the research team entered the data, further themes emerged from the data, and so we created new columns to incorporate these new themes under new inductive codes.
The research team also took additional open-ended field notes containing detailed accounts of their experiences, even when they were not officially observing or interviewing. These notes included informal discussions and observations. The team noted the tone and attitudes of the respondents during data collection and met regularly during data transcription and summarization to aid data familiarization process and to generate additional relevant codes and themes. Although the research team coded and categorized the observations individually, we drew inferences from the findings collectively.
Ethical Considerations
The research team stated the research study objectives clearly to the participants. The research team explained to the respondents that they have the freedom to refuse to participate and to withdraw from the study any time and that they may participate in the study but refuse to have the conversation recorded digitally. Before taking part in the study, participants provided written informed consent. The names of the respondents were recorded at the time of interview but were later replaced by numbers at the time of data transcription. The data were shared only within the coauthor team to maintain confidentiality. This study received icddr, b Ethical Review Committee clearance.
Findings
Mother’s Routine
Most of the mothers had minimal or no formal education. The primary earner of the family was typically either a farmer or lived and worked abroad (Table 2).
Demographic Information for In-Depth Interviews (12) and Observation Participants (24).
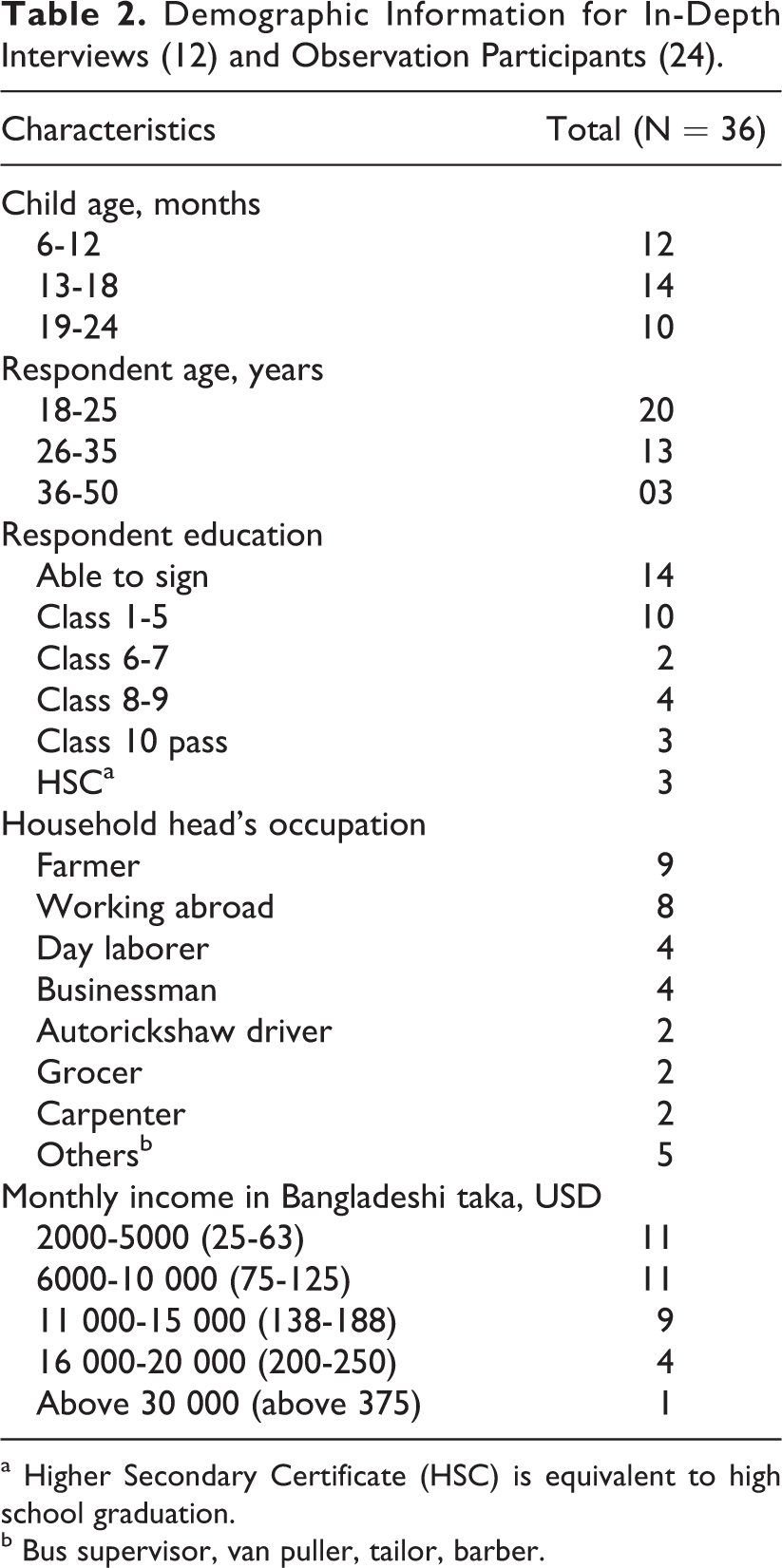
a Higher Secondary Certificate (HSC) is equivalent to high school graduation.
b Bus supervisor, van puller, tailor, barber.
The rural mothers included in this sample were busy throughout the day juggling multiple tasks. The typical mother reported waking up at 5:30 When my child completed six months, mostly I prepared boiled egg and khichuri (soft food preparation of rice, lentils and vegetables). I fried fish for him without chili powder. I prepared boiled rice with fine quality rice for him. I also gave him cow’s milk twice a day. But nowadays, I cannot. Because I have given birth to another baby, I cannot manage time for preparing extra foods.
Child Feeding
All mothers cited freshly prepared khichuri, suji (semolina), shemai (sweet preparation using vermicelli), and boiled eggs as dedicated children’s foods when specifically asked. Mostly I prepare khichuri for my child, which contains seasonal vegetables, lentils and rice. This khichuri is thick in consistency. Several times I also give my child hardboiled egg. In the morning, I give my child a boiled egg first and then I prepare family foods. In the morning, I prepare suji and sometimes shemai. At 11:00 am I cook rice, and in the afternoon and in the evening again I prepare suji. I prepare baby’s food four times separately. I do not feed my child any cold food or stored food, because the child has problem of catching a cold. I do not give her special food as she enjoys family food. Moreover, my child does not like other food and eats only boiled rice. But I also fed her infant formula and suji, when she was 8 months. Now I feed my child egg, boiled rice mixed with potato and leafy vegetables. We feed her what we prepare for the family. No separate food is prepared for my child. Several times I serve her the liver if we prepare beef or chicken. For example today morning we bought ruti (locally made bread buns) and dal (lentils) from the nearby bazaar. Usually I feed my child family food such as rice, dal, beans and vegetables. I boil beans and potatoes and then mash everything with rice and then feed him. Otherwise, he does not like to eat. But sometimes I prepare dal in a different process. I just boil dal and rice together and add salt. In this season, potato is available and I feed him an egg every morning. Previously, I fed him suji. Before feeding, I mash everything with liver, rice and potato.
Types of Food Fed to Children During Semistructured Observations.
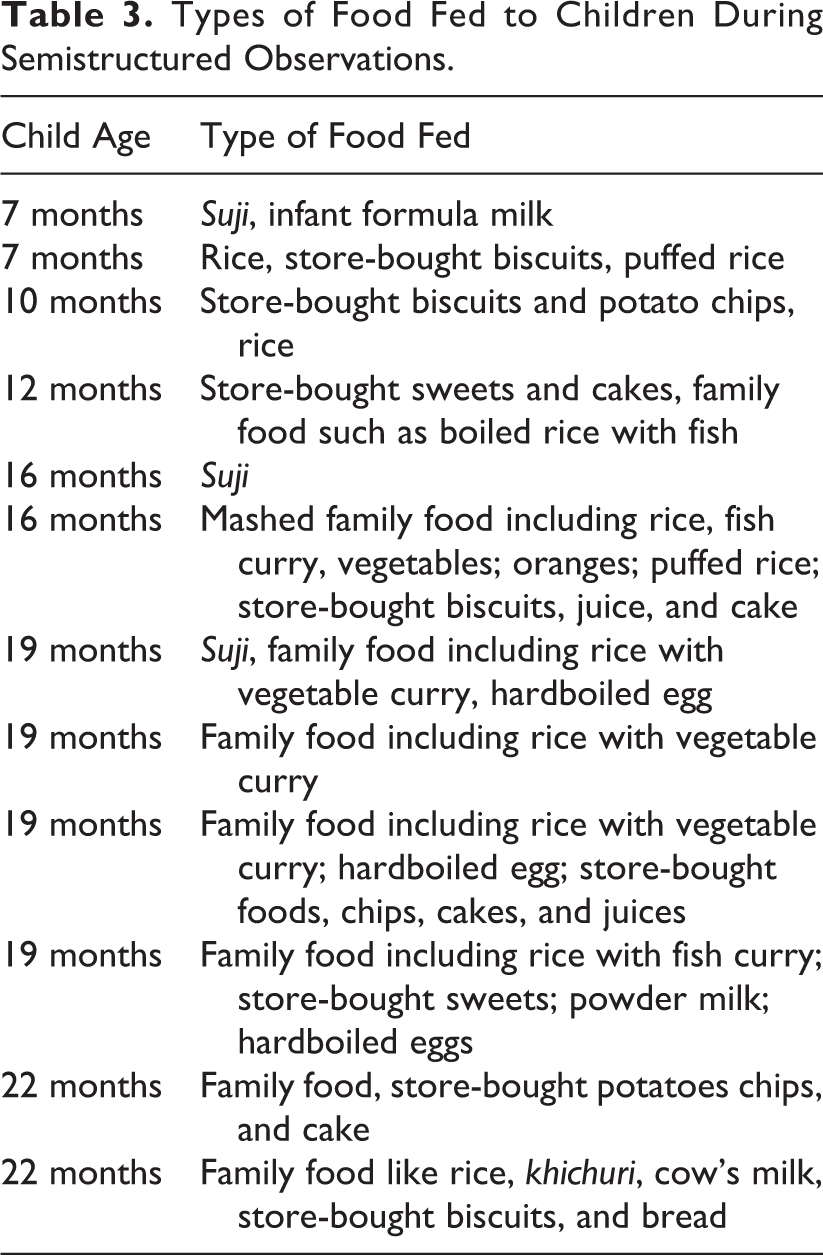
From observations and self-reports, feeding children store-bought foods such as commercially available potato chips, biscuits, and juices and locally manufactured sweets and cakes were also very common. Mothers were observed to feed children store-bought foods in 8 instances of the 12 semistructured observations (Table 3). Children of all ages are fed store-bought foods—the youngest observed child to be fed store-bought biscuits was 7 months old. Most of the mothers stated that store-bought foods are not safe and not good for their child’s health but claimed that children prefer the taste. Sometimes I serve my child biscuits … because sometimes there is no boiled rice or milk prepared that I normally feed him. During these times, I can give him this food (biscuits) to prevent him from crying or disturbing me. I know that store-bought foods are made in unhygienic conditions and they may create health hazards. However, I give store-bought foods to my child because he likes them. My child also eats biscuit, juice … his father brings these every day … I know store-bought food is not good for health but the child likes these types of food.
Child self-feeding was observed in 8 of 12 semistructured observations of child-feeding instances. The mother would give the child some dry foods, such as muri (puffed rice) or ruti (toasted flatbread), and then the child would self-feed unsupervised, while the mother concentrated on other tasks. During unsupervised self-feeding, 4 of 8 children dropped food on the ground multiple times and picked up the food and consumed it.
In 4 of 12 in-depth interview, mothers claimed that, in comparison to adults, children are more vulnerable to falling sick from unsafe food. In 9 of 12 in-depth interviews, mothers also asserted that feeding children cold foods would cause diseases. Five of 12 interviewed mothers mentioned that children’s foods should be special and they tried to store the children’s foods for a shorter time and reported that they frequently tried to feed children reheated foods.
Perceptions on How Food Becomes Contaminated
During the in-depth interviews, mothers mentioned a range of factors when asked what makes foods unsafe. Mothers used the local word “noshto” to describe foods that “go bad.” The use of the local term noshto is used to describe contaminated foods, stale and spoiled foods—basically any foods that are perceived to be inedible. They did not use separated terms for these. The term baashi was used to describe leftover foods that are consumed later on and likely refers to foods that have gone bad and cannot be consumed anymore, but it is also used to refer to leftover food that is consumed later. When probed about what is considered safe food in the in-depth interviews, mothers mentioned those that they do not hesitate to eat (“khete shondeho hoy na”). The leftover food from the night becomes baashi. For example, after eating at night if the leftover does not become sour or there is no bad smell, then that can be eaten. But if that food becomes sour or there is bad smell, then that cannot be eaten. Then the food becomes noshto. When I see that the color of the curry is a little different and I get bad smell from the curry then I think it is noshto. In summer food becomes noshto quickly. If I cook fish curry or black lentils, these become noshto quickly. In summer season, if I cook boiled rice in the morning, it becomes noshto by lunch. But in winter boiled rice cooked in the morning can be eaten at night. Any food can be unsafe if flies land on the food, because flies land on various places. There is a chance of food being noshto by cats, dogs, mice or other insects including flies. The food may be contaminated if not covered well … animals can make the food dirty. We cannot guess what type of disease we will get when. It is also disgusting to eat that food. Normally, if any food is stirred several times then the food becomes noshto quickly. We don’t touch the food that would be stored. We transfer a portion of food from the cooking pot to a bowl with spoon and keep covered.
Methods Employed to Keep Food Safe in the Postcooking Storage Phases
In the current study, respondents did not use any special word for “storage.” They spoke about storage in terms such as “ … then we keep it (food) for later time.” Respondents mentioned that the key methods used to ensure that food is safe include covering food, storing food on an elevated surface, and reheating food.
Based on the study participants’ responses, our findings distinguish between 2 types of storage times (Table 4):
Premeal storage: Storage of cooked food after cooking till consumption during a meal or snack.
Meal-to-meal storage: Storage of food from the time of the first meal until later consumption during a meal or snack.
Storage Conditions of Different Foods in Semistructured Observation Households.a
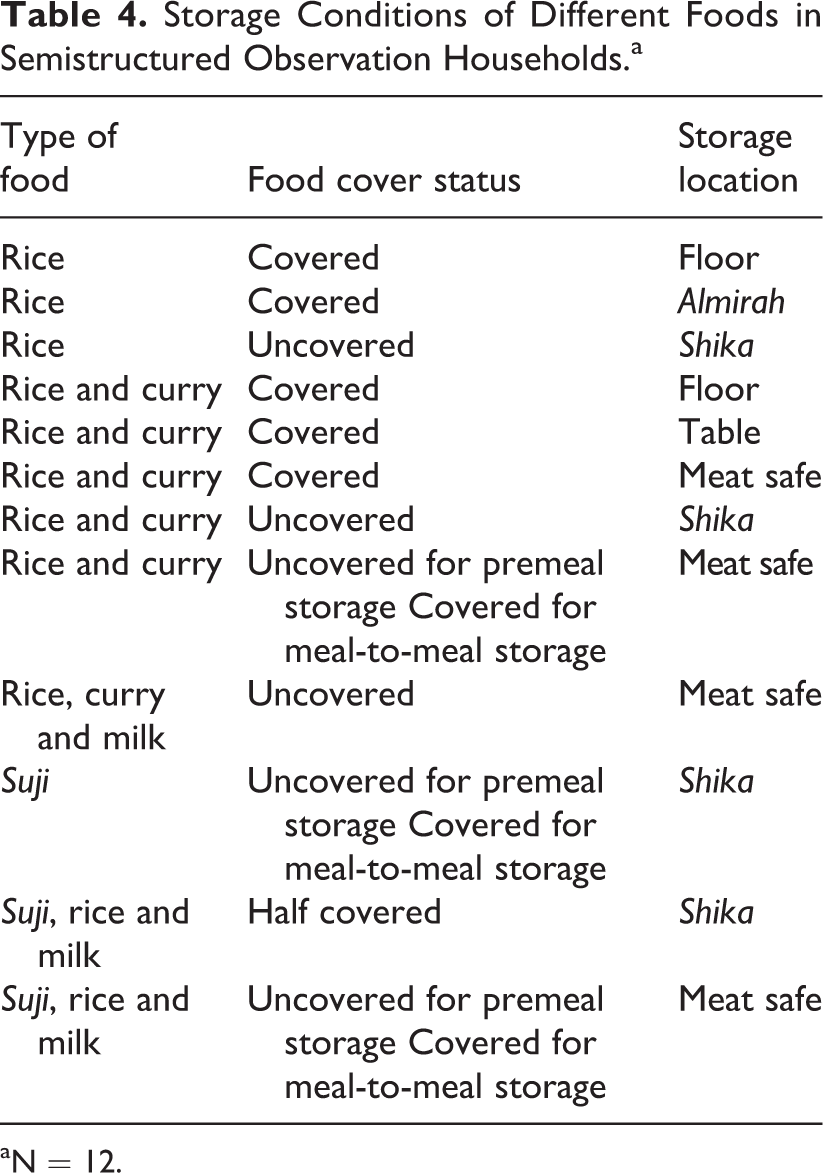
aN = 12.
Half covered food was noted when the research team observed a spoon or a wooden stick placed in the container with the lid half on, ensuring that there was an opening through which the steam can escape. Some of the local hardware used for storage included the shika (a shelf with rope attached hanging from the ceiling), almirah (a wooden cabinet used for storing clothes but also has a section for food storage), macha (a wooden shelf attached to a wall at an elevated level), and meat safes (cabinets made of wood or steel with screened or netted doors so that air can pass through as shown in Figure 1).

Typical meat safes used in rural Bangladesh.
Food covering and storage on an elevated surface
In most cases, the practice of food covering was similar for premeal and meal-to-meal storage (Table 4). Respondents in general mentioned keeping food on some sort of elevated surface out of reach of insects and animals to keep food safe. Foods stored on the floor were found to be covered even though 5 of 12 mothers reported that in general storing food on the floor made food vulnerable to animals and insect. I keep all the foods on a shelf (higher surface) so that dogs or cats can’t nibble those. I store cooked foods like boiled rice and curries in the dishes covered with lid. If the foods are too hot I keep those aside for a while so that the steam reduces, then I cover those with lids and store … if hot foods are kept covered then it may become contaminated.
In 2 of 12 semistructured observation, participants were observed to separate the food from the cooking pot into serving plates, while the rest served food directly from the cooking pot during mealtime. The duration of premeal storage (between cooking and consumption as part of the first meal of the day) ranged from 15 minutes to 1 hour. The duration of meal-to-meal storage (between the first meal and the second meal within the same day) ranged from 4 to 8 hours.
Reheating before consumption at next meal
Mothers from the focus group discussions explained that they cook and consume food in the morning and then store the leftover food for 4 to 5 hours until lunch. Mothers also reported that sometimes they reheated food in the morning that was stored overnight but leftover food from the morning is not always reheated for consumption at lunch. When the research team asked why they reheat food, the main reason for reheating that the mothers cited was that cold food tastes bad, and the men and children of the household prefer hot food. Due to work pressure we can’t reheat foods always. As we are villagers, we have lots of work to do. Moreover village women do not usually reheat foods before eating. We can eat cold foods. But we reheat foods for men in spite of having work pressure, because they are not habituated to eating cold foods. We do not reheat curries of gourd and radish, because they will not taste good if reheated.
According to the focus group mothers, children prefer hot foods and consuming cold food can result in children catching a cold or having stomach upset. The research team observed in one instance that hot milk was added to leftover cooked suji so that the child could consume it hot or warm. One mother explained that if food is reheated once, it can then be stored for even longer periods of time and not be spoiled.
Mothers also mentioned that they are unable to reheat foods all the time. Due to work pressure we can’t reheat foods always … feeling tired is a reason for not reheating foods It is a hardship to fire the burner for reheating using a wood and straw based burner; fuel is sometimes difficult to find and also it is very time consuming
Community Recommendations
A common recommendation from the study mothers was to use meat safes to improve food safety—10 of 12 mothers we interviewed mentioned this. Mothers who had meat safes in their households were observed to use these for both premeal and meal-to-meal storage (Table 4). I keep foods in the meat safe. I don’t cover foods with lids as those are kept in the meat safe. No insects or dust can enter into the meat safe. I don’t store food in a separate bowl because I don’t have meat safe and I have to keep foods on the floor. I don’t feel good keeping on the floor. But still I have no meat safe to store the cooked or leftover foods. There is concern that the food can be damaged by cats, dogs, mice or other insects including flies. So, I don’t store food in bowls. But we cannot easily waste foods if I keep them in the cooking pots covering with well with a lid. In summer, if I had the meat safe, I could keep food in the meat safe in a bowl without lid.
Discussion
Conventional interventions have promoted complementary food safety by recommending multiple behaviors that can eliminate all or most sources of contamination, without taking into account existing local knowledge or without necessarily making interventions convenient. Intervention messages generally stress germs and other threats to child health as reasons for adopting multiple new behaviors. Our study found that conventional approaches that include teaching food safety may be a disincentive for rural mothers who need solutions for their physical environmental constraints.
Rural mothers did not use specific biological terms to describe food safety methods and rationale but, in their own ways, described methods that are consistent with biomedical understanding. For example, rural mothers indicated that children’s foods require more care than adult foods as children are more vulnerable to falling sick. Mothers also cited important determinants of food spoilage and contamination, including storage duration, temperature (highlighting that reheating of foods is important and food goes bad faster in summer relative to winter), moisture (food remains wet due to trapped steam, moist food goes bad faster), contact with air, contact with dust, too much handling (too much stirring and contact with hands), and unclean utensils. Mothers further mentioned that covering food and keeping food on elevated surfaces can keep food safe from animals and insects. These findings are consistent with other research in Bangladesh and elsewhere 37 that existing understanding of hygiene is good, even though ideal practices are often not possible. 38 –40 Building awareness of the pathways of food contamination will be redundant in contexts where existing perceptions are already consistent with biological perspectives of food safety. Teaching community members information they already know can distract from promotion of new behaviors and can unnecessarily extend promoter visits with community members.
Although mothers explained that khichuri, suji, shemai, and boiled eggs are dedicated children’s foods, their practices reflect that children ate regular family food cooked daily. Similar findings elsewhere suggest that children’s foods are not conceptualized to be separate from adult foods, the differences being quantities, or need for modification, such as mashing or washing to remove spices. 36,41 It seems that in general rural mothers’ choices regarding food safety and child feeding are largely driven by convenience and taste preferences, not primarily by safety concerns. In rural Zimbabwe, mothers would use maize over millet and sorghum because grinding the latter took more time and energy. 42 Similarly in water treatment research studies, when given a choice, users will opt for less effective but more convenient point-of-use water treatment methods over those less convenient and more effective. 43 In our study, even when most mothers explained that raising food off the ground ensured safe storage, storing food on the ground where family members sit at meal time was also reported because it makes food easy to serve. Mothers can become very busy managing time-consuming domestic activities, 44 and preference for convenience driven by time constraints regarding complementary feeding practices has been reported by mothers in Bangladesh and elsewhere. 36,38,45,46
Linked with the theme of convenience is the importance of taste—for example, even though mothers perceived store-bought foods to be poor quality, they continued to feed them to their children because they claimed that children stopped crying because they liked the taste. Studies conducted on child feeding from Ghana and Mexico also provide evidence that a child’s preferences influenced the foods given to children. 45,47 Furthermore, reheating is a time consuming inconvenient activity, yet mothers will reheat food because men and children of the household prefer the taste of hot foods. Taste preference is an important determinant for the success of nutrition. 20,36,48 –50 Therefore, a complementary food safety intervention should emphasize child health benefits by promoting food choices and behaviors influenced by taste and convenience. 51
Based on our study findings, we propose extending the use of existing beneficial behaviors that can address local concerns and can seamlessly fit into a busy mother’s daily routine. We also propose promoting a range of benefits in line with local preferences beyond messages about food contamination and healthy growth of child.
Despite mothers reporting that covering food is important, we observed that food was frequently left uncovered. Rural mothers perceive that trapped steam causes foods to go bad, therefore food is not covered immediately after cooking. As such, this practice of leaving food uncovered for steam release should be considered when developing a complementary food safety intervention.
In Bangladesh, caregivers usually prepare complementary foods and continue feeding the same food to the child throughout the day until it is finished. 7 While wealthier households can refrigerate leftover food after the first feeding restricting microorganism multiplication, poorer households and those without electricity are unable to afford this luxury. Therefore, in most rural households, the bacterial population introduced during the first feeding multiplies over time, increasing the exposure dose in subsequent feeding which increases risk of illness. 7,8 This highlights that storage is an important period for food contamination.
Mothers described how meat safes protect food. As per the Oxford Dictionary definition, the term meat safe is defined as a cupboard or cover of wire gauze or a similar material, used for storing meat. However, the Bengali language over the years has adopted many English terms that used to be etic and now have become fully emic terms used in daily colloquial language. The word meat safe is one such example. For the purposes of our research findings, the term meat safe is a local term and despite of the word meat in this term, all kinds of foods are stored inside this cabinet. Meat safes allow for immediate safe storage of hot foods while addressing local concerns for steam release without the need for tight covers. They can protect food from exposure to animals and many insects, including flies, and can reduce likelihood of human-food contact. Meat safes already have a foothold in the market, are seen as durable household assets, and are locally available, acceptable, and affordable (US$25-US$30). Other simple innovations can be considered such as using netted tight-fitting lids or tight-fitting lids with vents on the top to protect food from animal, insects, and human hand contact, while still allowing steam release immediately after cooking. We recommend conducting further research using these products for further efficacy and effectiveness testing. An intervention to encourage use of convenient hardware should ensure that local values are considered to maximize uptake. Community members perceive that animals and insects are a threat to food safety and that meat safes allow steam release while protecting from these hazards and are convenient to use.
There are reasons to believe that safe storage alone can provide a significant benefit in keeping food safe. First, in another study in rural Bangladesh, we have detected significantly higher levels of E coli in uncovered stored compared to covered stored food for children less than 5 years (note 2). Second, in a randomized control trial conducted by our group, we demonstrated that water becomes contaminated on storage and that keeping water in storage vessels that limit hand contact was associated with lower microbiological contamination and reduced child diarrhea. 52 By similar logic, it is possible that safe storage alone can protect food.
Some of the data from interviews and observations have been quantified in the findings section; however, it is important to interpret these data conservatively since the number of informants is small. Furthermore, the numbers reported from the semistructured observations must also be interpreted with caution, since the physical presence of an observer can influence hygiene practice, 53,54 and as such, our data regarding “ideal” practices might be overestimates as a result of positive courtesy bias. Specifically for the video observations, we attempted to minimize reactivity by hiring and training local women from the study site to conduct the videos.
Even though we collected data from 4 rural villages within the country, these villages were typical Bangladeshi rural villages, and moreover, our conclusions are based on complementary feeding perceptions and practices that are similar among people of the demographic characteristics of respondents in villages across the country. Specifically, our study findings highlighting the importance of taste and convenience and conducting further research on existing practices is something of global relevance.
Our study focused on the postcooking phases (premeal storage and meal-to-meal storage), however, there are other contamination pathways that can be the subject of further research. We gave less importance to the food preparation phase, based on evidence suggesting that foods are cooked for long duration at high temperatures in this setting, constituting a microbiological “kill step.” 7 Previous studies of food preparation in rural Bangladesh made the key recommendation of encouraging greater handwashing. 55 We also observed mothers giving children dry foods as an example of unsupervised self-feeding, where the food would sometimes fall from the child’s hands and then the child would eat it off the ground. This has also been observed elsewhere and is estimated to expose children to human and animal feces from soil. 56 An intervention that addresses food storage only will not address the risk from unsupervised child self-feeding. A final limitation of the study is the lack of information on breastfeeding practices and infant formula use. However, infant formula use was observed in too few events to adequately evaluate this practice in this study population.
The current formative research data were analyzed to capture important considerations for devising shallow and broad interventions, hypothesizing that this approach might be more scalable and sustainable than existing interventions on complementary food safety. While the current study findings suggest that safe storage hardware might be feasible and acceptable, the contamination prevention potential of using this hardware remains a potential direction for future inquiry on food safety. For future programs and interventions on infant and young child feeding and complementary food safety, we recommend exploring 2 different types of hardware—meat safes and tight-fitting netted lids or tight-fitting lids for steam release. We know from our data that some households already have existing meat safes, and some households might not be able to afford meat safes. For these cases, we recommend research into a cheaper option of tight-fitting netted lids or tight-fitting lids with vent that can potentially allow for steam release while still protecting food from insects, animals, and hands. As such, safe storage options such as meat safes and tight-fitting lids (with steam release potential) should be tested for community acceptability, integration with food preparation steps, and the ability to reduce food contamination. Similarly safe storage interventions are likely applicable to other low income settings, especially where electricity connections and refrigerators are uncommon.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research study was funded by the Bill and Melinda Gates Foundation. International Center for Diarrheal Diseases Research, Bangladesh (icddr, b) acknowledges with gratitude the commitment of Bill and Melinda Gates Foundation to its research efforts. icddr, b is also grateful to the Governments of Bangladesh, Canada, Sweden, and the United Kingdom for providing core/unrestricted support.