
Abstract
Background:
Vitamin A supplementation (VAS) is currently implemented in over 80 countries worldwide, but little attention has been paid to gender equity in the design or implementation of these programs.
Objective:
This article describes the ways in which gender equity can impact or be impacted by VAS programs and suggests ways to ensure these programs better support gender equity in the future.
Methods:
We undertook a desk review of research on gender equity in health services and extrapolated findings to VAS, highlighting gender equity issues throughout the VAS implementation process and across delivery platform types. We also amassed secondary data on VAS coverage from 45 surveys in 13 countries and analyzed it to examine differences in VAS coverage between boys and girls.
Results:
Despite few significant differences in coverage between boys and girls, we identify numerous ways in which gender equity can impact or be impacted by VAS programs, including through the choice of VAS distributors and the communication materials used to promote VAS campaigns. Examining these different entry points reveals that there are several missed opportunities for better integration of gender within VAS.
Conclusions:
VAS program implementers and policymakers should revisit VAS approaches to identify opportunities for advancing gender equity through this wide-reaching platform.
Introduction
Vitamin A supplementation (VAS) for children younger than 5 years has been a cornerstone of global child survival programs for decades, 1 and VAS has been shown to have positive impacts on reducing child mortality. 2 The World Health Organization (WHO) recommends all children aged 6 to 59 months receive high-dose VAS every 4 to 6 months in areas where the prevalence of vitamin A deficiency (VAD) is ≥20% in young children, 3 and more than 80 countries currently have universal VAS programs in place. 4 This makes VAS one of the broadest-reaching child nutrition interventions in the world.
Vitamin A supplementation is a nutrition-specific intervention that seeks to improve vitamin A status in the short term (1-2 months) through the periodic delivery of high doses, thereby reducing child mortality in areas of high disease prevalence. Despite the benefits, such interventions have limits: even if the 10 core nutrition-specific interventions identified in the 2013 Lancet Maternal and Child Nutrition Series were scaled up to 90% coverage, they would only address about 20% of global stunting, 5 making it essential to also consider nutrition-sensitive interventions (those addressing underlying determinants, such as food security and resource access). 6 One key area for nutrition-sensitive intervention is supporting gender equity and women’s empowerment.
Gender equity impacts nutrition through multiple channels, including resource access, time use, and decision-making power. When women have less control over household resources and the use of their time, lower self-esteem, and limited access to information and health services, this can adversely impact their child’s nutrition through care and feeding practices; it can also indirectly impact children’s nutrition via women’s own nutritional status. 7
Given this connection, it is essential for all nutrition interventions to view their work through a gender lens: understanding how the intervention might impact, as well as be impacted by, gender equity. Vitamin A supplementation programs have historically been gender-blind: aiming to cover all children, regardless of sex, at coverage rates 80% or higher and without explicit focus on the gender dynamics that could impact their processes or outcomes. Equity in coverage is an appropriate goal: while few studies on VAD disaggregate results by sex, 4,8,9 where such results are reported, there has tended to be no significant difference between males and females. 10 This suggests that the burden of VAD is approximately equal between boys and girls. Equity in coverage, however, is only one dimension of gender equity within VAS. As attention to the importance of gender equity across all areas of health and nutrition grows, 11 it is important to explicitly examine the question of gender equity within VAS and consider how programming could become more gender sensitive (or even gender transformative) 12 in the future.
Such an examination is particularly appropriate at present, as many VAS programs are facing a major transition that could have equity implications. Historically, VAS has mainly been provided through National Immunization Days (NID) and polio Supplemental Immunization Activities. 13,14 As these involve providing essential childhood vaccines through door-to-door delivery, coverage has generally been high (>80%) for both immunizations and VAS, 15 compared to the much lower coverage typically achieved through health facility-based delivery. 16 More recently, semiannual Child Health Days or Child Health Weeks (CHDs/CHWks), which offer a package of maternal and child services through a combined facility and community-based model, have become a common delivery platform for VAS. 17 However, funding constraints and successful polio eradication efforts (and hence the disappearance of polio vaccination campaigns) are shifting the policy and program focus away from NIDs and CHDs/CHWks to the integration of VAS into routine services. 18 Two examples of this are the 6-month and 6-monthly contact points, which enable year-round supplementation and allow for bundling health services (e.g., family planning counseling) when a parent brings their child to a health facility. 19 Additional models are also being tested, such as the use of community health workers (CHWs) to facilitate campaigns. Coverage for these routine services tends to be lower and much more variable than for door-to-door campaigns, and the burdens placed on caregivers and health workers may be different.
This crossroads offers an opportunity to rethink VAS approaches, including to consider previously neglected aspects such as gender equity. This article aims to inform this discussion, with a focus on sub-Saharan Africa (SSA). In the following sections, we explore two propositions and then propose a new framework for considering gender equity in VAS programming. First, we explore the proposition that gender intersects with VAS in ways that go beyond equal coverage by conducting a review of the literature on gender equity in health services. Second, we consider the proposition that VAS coverage between boys and girls is equal by analyzing secondary data in 13 SSA countries. We then use evidence from these analyses to develop a framework for examining gender at different stages of a VAS program and under different models. We next discuss these results, while the final section concludes.
Methods
To explore intersections between VAS and gender apart from coverage, a literature review was conducted on terms related to gender inequality and health services, particularly for VAS and immunization, in SSA. The objective was to identify gender-related barriers to and facilitating factors for health service access and provision, with a focus on those potentially relevant for VAS. Searches were done using PubMed and Google Scholar; citations in and of identified articles were screened to identify further articles for review. All articles deemed relevant to the topic were documented and included in the final review. The review was conducted from October 25, 2018, to April 4, 2019.
To assess gender-based differences in VAS coverage, we analyzed data from coverage surveys undertaken approximately 4 to 6 weeks after different VAS distribution rounds between 2010 and 2015, each of which included data from at least 1 of 13 SSA countries. Sampling used an adaptation of the WHO immunization coverage cluster survey approach, 20 with 30 clusters of 30 children each. Data were collected through face-to-face interviews with a primary caregiver; in 85% of cases, this was the mother. Questionnaires covered receipt of campaign-provided services, caregiver awareness, and reasons for children not being covered. Altogether, there were 45 country-round data sets, containing observations from a total of 61 929 children aged 6 to 59.9 months. Data were analyzed using Stata SE15 21 to determine VAS coverage levels for each country and round and tested for differences in coverage between boys and girls.
Literature Review: Gender and Health Services
This review found that gender inequalities can exist on both the supply and demand sides of health services. On the supply side, the evidence shows generally imbalanced gender representation in the health workforce. Women are underrepresented in higher level decision-making posts, making it difficult to improve the quality of care for women and children at a systemic level, since male decision-makers may fail to consider the unique challenges affecting women and children. 22 On the other hand, women are overrepresented in lower level health personnel positions closest to communities, contributing to the “feminization” of these health spaces, which can act as a barrier to male attendance. 23 Female health-care workers often experience negative stereotyping, sexual harassment, poor support for working mothers, and pregnancy- and caregiver-based discrimination. These working conditions contribute to both the difficulties women face in ascending the career ladder and poor-quality services from stressed or demotivated health workers. 24 Low-quality health services then negatively shape the interactions of health workers with mothers (leading to lower demand). The health facility itself can also be a barrier, particularly when considering the intersectionality of gender with socioeconomic status and ethnicity. 25 A lack of privacy in health facilities can result in increased public scrutiny and stigma for low-income mothers who have negative interactions with health workers. 26
At the community level, CHWs have played an important role in reducing micronutrient deficiencies by disseminating nutrients in preventative packages 27 and recently as VAS distributors in rural Burkina Faso. It has been demonstrated that female CHWs are better at addressing reproductive health issues because women do not want to share these issues with men, whereas male CHWs are critical for reaching men who feel it is “unmanly” to use health services. 28 Female CHWs have been shown to reduce gender inequity when working in areas where women face unique social challenges (such as required dress for health facility attendance or movement restrictions), but hiring female CHWs can be a challenge because of literacy or educational requirements. 29 Female CHWs often find themselves in the paradoxical position of lacking support and being underpaid within the broader health system, but having higher status in the community, which can result in their overlooking low-status children. 26 Relying exclusively on either female or male CHWs can thus exclude men or women and entrench negative gender norms around health.
On the demand side, the burden of maternal and child health is often placed predominately on women, who face numerous barriers to accessing health services. In one study in Burkina Faso, Mali, and Nigeria, 75% of women reported that their husbands alone made decisions concerning health care. 22 Other studies specific to VAS reported that the principal decision-maker for seeking VAS was the father in 77% of survey responses, 30 and the most common barrier to a child receiving VAS was the father’s disapproval. 31 On the other hand, immunization and child health services often target mothers as children’s primary caretakers, which may discourage fathers from sharing responsibility even though they are considered the de facto family decision-maker. 26 Closely related to decision-making power is financial power: Women who do want to access health services may not be able to afford transport to health facilities or any associated fees. 32,33 Female-headed households are more likely to have an immunized child but also to be poorer overall, indicating that even if a woman controls her income, her family is disadvantaged in other ways. 34 Women in urban areas tend to have more access to cash, but they are also employed in sectors where their pay is linked to the number of hours worked, meaning they have difficulty accessing health services during normal work hours. 35 Women also tend to be responsible for most or all unpaid work in a household, in addition to paid work. This translates both into immediate challenges in finding the time to attend a health facility or fixed-point service, as well as challenges in addressing the root causes of inequality, such as obtaining education and employment opportunities. 36 -38 The lack of educational opportunities is especially problematic because the children of more educated mothers are significantly more likely to be immunized. 26 Financial inequities are worsened in polygamous households, where women may be competing for scarce household resources with other wives, as evidenced by a study showing that women in monogamous relationships were more likely to seek health care. 39 Women’s mobility is also often more restricted in insecure areas, raising a further barrier to preventive child health care, 26 and conflict can intensify women’s burdens by increasing the number of female-headed households. 40 The links between gender and health services are thus myriad and complex.
The following section uses these insights from the literature to develop a framework for considering gender equality within VAS. First, however, we explore the most obvious manifestation of potential inequality within VAS: unequal coverage.
Results
Gender Gaps in VAS Coverage
Results from the analysis of gendered differences in VAS coverage, shown in Table 1, demonstrate essentially no differences in coverage according to the child’s gender: for 43 of 45 surveys, there is no statistically significant difference (P > .05). This is true in both high- and low-coverage settings. For the remaining 2 surveys, both from Burkina Faso, one shows a slight gap favoring boys; the other shows a slight gap favoring girls.
Coverage by Child Gender Across 45 VAS Rounds.a
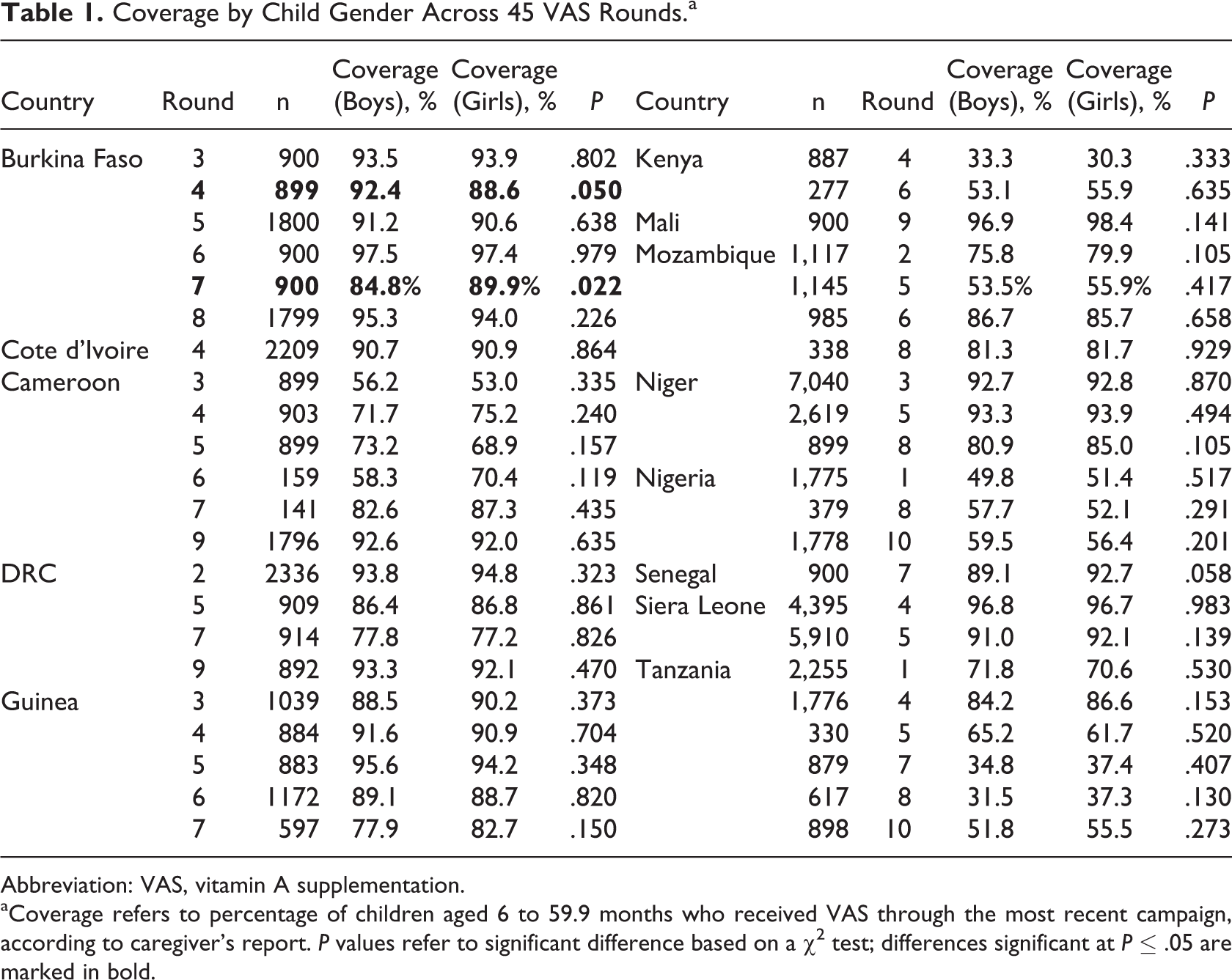
Abbreviation: VAS, vitamin A supplementation.
aCoverage refers to percentage of children aged 6 to 59.9 months who received VAS through the most recent campaign, according to caregiver’s report. P values refer to significant difference based on a χ2 test; differences significant at P ≤ .05 are marked in bold.
Gender Equity in VAS: A Framework
Although the above statistical analysis reveals gender-equitable VAS coverage in SSA, the literature summarized above suggests that gender equity issues within VAS may extend beyond coverage. Viewing that literature through the lens of gender mainstreaming within global health 41 allows us to develop a set of guiding questions for how gender could affect and be affected by VAS programs at various implementation stages. In so doing, we also draw on the framework developed in Theobald et al, 42 a recent analysis of gender within the structurally similar topic of mass-drug administration for neglected tropical diseases (NTDs). The result is depicted in Table 2.
Guiding Questions to Identify Intersections Between VAS and Gender.
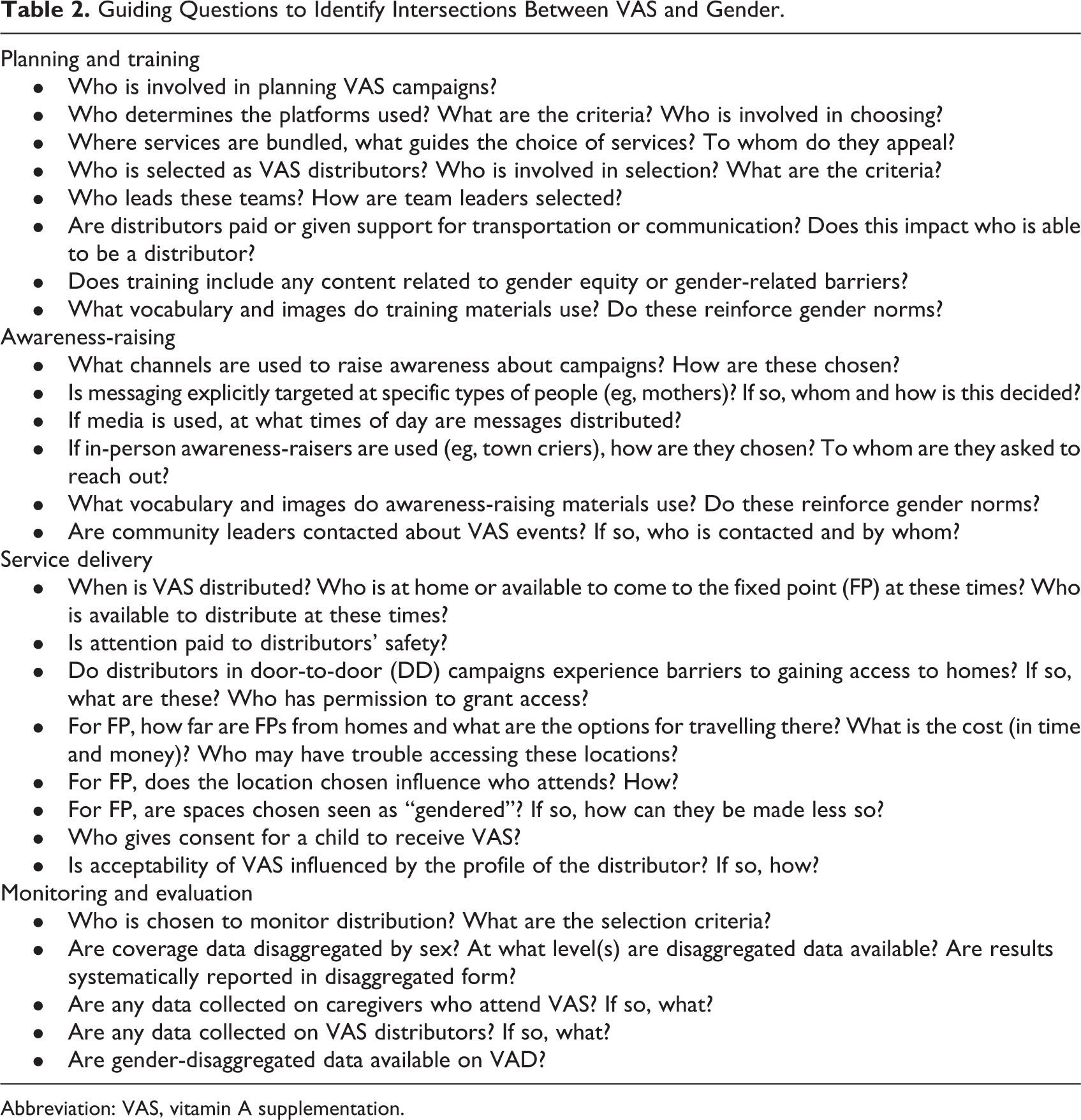
Abbreviation: VAS, vitamin A supplementation.
Table 2 identifies 4 areas of intersection between VAS and gender: planning and training, awareness-raising, service delivery, and monitoring and evaluation. Within planning and training, we recognize that VAS programs involve and employ large numbers of people at each stage; each of these offers an occasion to ensure gender equity in the workforce itself and also foster gender-equitable service delivery. For example, thought should be given to how the selection and support of distributors and team leaders, whether male or female, can reinforce or challenge gender inequities in communities. Even criteria that are not clearly related to gender, such as literacy or access to transport, can result in gender-related barriers if there are differences between men and women with regard to those characteristics. Preferred delivery platforms and bundled services may differ between male and female caregivers; the choice of platform and service package will have implications for coverage and caregiver time use. Training also offers an opportunity to either reinforce or subvert existing gender norms, especially those related to childcare.
Within awareness-raising, it is important to consider how messaging campaigns contribute to or attempt to shift social norms that designate women as children’s primary caregivers. This includes to whom messages are directed, how they are delivered, and how they are framed—such as whether images include men as caregivers as well as women. A study in Mali linked increased VAS coverage to fathers who listened to a radio, indicating that targeted messaging can involve fathers to positively affect child health outcomes. 30 Including fathers in immunization campaigns has also been linked to increased rates of immunization. 43 Little work has been done on the gendered nature of VAS education and marketing campaigns, but evidence from vaccination suggests that messages often target women. 26 Such approaches reinforce the norm of women as being responsible for childcare and should be examined in any VAS program looking to be more gender equitable. Working with community leaders can offer an opportunity to use these trusted people to reinforce more equitable gender norms, such as by encouraging men to take their children to facilities for VAS.
Within service delivery, it is important to consider timing, location, and structure of VAS door-to-door and fixed-point programming—all of which can interact with gender issues to influence access. For example, in communities (such as northern Nigeria) where purdah (screening women from men or strangers for religious reasons) is practiced, women’s limited mobility could make it difficult for them to take their child to a health facility, and male distributors would not be allowed to access a house if the mother were home alone with a child. Distribution at fixed points can create barriers to access or place a burden on women’s time if these points are far from homes or there are limited public transportation options, as men may have better access to transportation than women. In contrast, if the spaces used for distribution are seen as gendered (such as antenatal/postnatal clinics), this may further discourage men from bringing children to VAS services.
Finally, within monitoring and evaluation, we consider both who is selected to monitor and evaluate distributions and the types of data collected. Ensuring gender-equitable VAS programs requires sex-disaggregating data on VAS caregivers, distributors, and coverage as well as on VAD. At present, limited data are available on VAD or caregiver or distributor gender. Data on coverage vary; as with NTDs programs, they may be disaggregated by sex at local levels but rarely cascaded up to the national level in their disaggregated form. 42
Discussion
Improving Gender Equity in VAS
Given the guiding questions for thinking about gender equity in VAS proposed in Table 2, we now consider ways to advance gender equity through VAS, as summarized in Table 3. Within planning and training, we see opportunities for including more women in VAS decision-making and activities and for educating men and women on gender topics. Hiring within VAS programs can be an opportunity for women to gain employment and skills, if hiring processes are sensitive to gender barriers (e.g., norms and required skills that favor men, women’s lack of work history) and provide support for overcoming barriers (e.g., transportation allowances, stipends for childcare). Trainings can be used to showcase images of gender equity and to educate men and women about gender equity and gender-related barriers, as they relate to health and nutrition. Platforms and services can be chosen to enhance equity in VAS and more broadly, such as by using gender-neutral spaces for family planning distribution as a service bundled with VAS.
Opportunities for Better Integration of Gender Equity Within VAS.
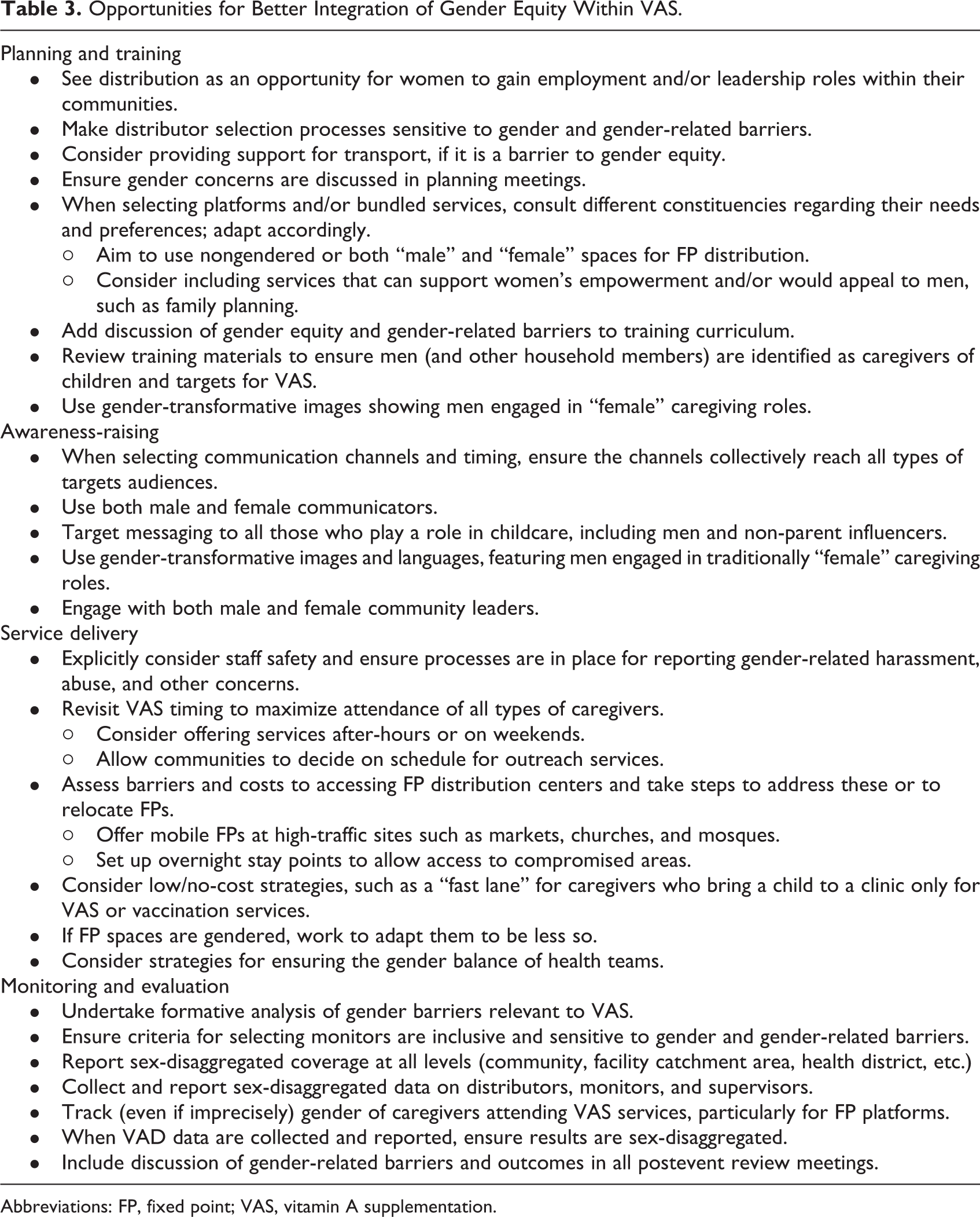
Abbreviations: FP, fixed point; VAS, vitamin A supplementation.
Within awareness-raising, we see opportunities for using channels that reach diverse audiences and for challenging gender norms through messaging. Vitamin A supplementation communication campaigns should be seen as a chance to reach a large audience not only on VAS but also on gender equity for improved nutrition. Targeted messaging can use gender-transformative images and language that encourage mothers and fathers, as well as non-parent caregivers, to be involved in childcare. Approaches may need to be tailored by sex, as there is some evidence (from the vaccination field) that men and women differ in their trust for different information sources. 44 The use of both male and female community leaders to publicize VAS campaigns could help to further solidify women’s leadership roles in communities.
There are opportunities for improving service delivery through better support and training for health workers and by addressing gender-related barriers around location, distance, and perceptions of service delivery locations. Health policymakers should ensure supportive processes are in place for female health workers: female health workers may struggle to advance or remain in the workplace because of negative stereotyping, sexual harassment, and gender-related discrimination. 24 Educating health workers can be an effective strategy for promoting gender equity, as it allows workers to both pass on empowering health information to mothers and fathers in their routine interactions, such as VAS, and to work as change agents for gender equality. 23 Service locations and timing can also be adapted to be more gender equitable, for example, by offering services after-hours or on weekends to ensure working mothers and fathers can access them, or by offering mobile services for caregivers who find accessing service locations a challenge. 26
Within monitoring and evaluation, we see opportunities for improving the data available on VAS programs. Gender analyses should be done at the beginning of programs, gender-sensitive indicators should be included in monitoring, and sex-disaggregated data should be reported at multiple levels (from community to national), for multiple categories (coverage, VAD, caregivers attending services, and workforce). All of these data should be incorporated into feedback loops and regularly discussed at review meetings, to ensure that gender inequities are identified and addressed through programming.
Implications for VAS Platform Transitions
As many countries shift from campaign-based delivery mechanisms to integration of VAS into routine services, we see both challenges and opportunities related to gender. Studies in Ethiopia and Senegal have found that coverage dropped upon the shift to routine VAS services. Although neither study explicitly considered gender, both found that mothers’ preferences for delivery systems were varied (fathers were apparently not consulted). Both countries used smaller campaign-like mechanisms (e.g., “mop-up” campaigns) because of concerns about decreasing equity. 16,45 Given the challenges women face in accessing routine health services, and the norms around maternal responsibility for child health, it is likely that VAS coverage through routine platforms will place increased burdens on women’s time and result in differences in coverage across socioeconomic and geographic groups unless programming specifically considers gender-related barriers.
One promising approach to maintaining VAS coverage levels through routine services is bundling VAS with other services that are either desirable to caregivers or empowering to women. In Ethiopia, mothers did not understand the benefits of VAS but had a better understanding of deworming—combining the two could help increase VAS coverage. 45 Another review found that women-centered services were more effective when offered as part of an integrated package. 23 Sierra Leone has developed a package of services, including complementary feeding demonstrations, family planning, and VAS, 46 which has helped the country maintain high coverage levels even after switching to routine services.
Intersectionality
This article has focused primarily on gender and VAS, but gender intersects with other factors related to social inclusion, such as religion, socioeconomic status, and ethnicity. To gain a holistic picture of equity in VAS, these other factors must be taken into account. For example, in terms of service providers, research on CHWs in five African countries showed inequitable selection processes, including nepotism and literacy requirements, that may disadvantage older, poorer women. 47 Ethnic and language barriers can also hinder the dissemination of health information. 26 On the caregiver side, some women may avoid health facilities because of language barriers or perceived staff reticence to treat people from other ethnic groups. Female migrant workers may lack the social support needed to care for their children, and persons with disabilities face societal stigma and challenges accessing facilities. Although this article does not discuss these issues in detail, we recognize that these intersections are important; future research should explore these dimensions more fully.
Conclusion
In this article, we examined gender equity in VAS coverage, described how VAS programming relates to gender equity, and proposed ways to better integrate gender considerations into future VAS programming. Throughout this process, we drew on similar work undertaken in related sectors, including NTDs and vaccinations. The lessons of this article, and the guiding questions we developed for examining VAS programs, may be applied to those sectors as well as similar platforms in other health sectors. Future research can build on this approach to generate better evidence around the importance and effectiveness of considering gender in VAS programming. We hope that this work will help VAS teams move toward more gender-equitable and even gender-transformative programming.
Footnotes
Highlights
Despite few significant differences in coverage between boys and girls, there are numerous ways in which gender equity can impact or be impacted by VAS programs; viewing VAS through a gender equity lens suggests new opportunities for using this wide-reaching platform to improve gender equity.
Acknowledgments
The authors thank Amynah Janmohamed for data cleaning of the post-event coverage surveys, the staff of HKI who undertook those surveys, and Rolf Klemm and an anonymous reviewer for comments on earlier versions of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by GiveWell; Global Affairs Canada provided funding for earlier PECS. Part of this work was commissioned by UNICEF with funding provided by the Government of Canada through Global Affairs Canada, under the “Enhanced Child Health Days” grant.