
Abstract
Background:
Assessment of high-dose vitamin A supplementation (VAS) coverage often relies on postevent coverage (PEC) surveys, but the validity of these methods has rarely been evaluated.
Objectives:
To assess reported VAS coverage and factors associated with missed coverage and to investigate the reliability of the results.
Methods:
During a cross-sectional survey, 10 454 caregivers of children <27 months old were asked whether their child had received VAS in the past 6 months. During a 48-week longitudinal study of 6232 children 6 to 30 months old, caregivers were asked every 4 weeks if their child had received VAS in the past 4 weeks.
Results:
The cross-sectional study showed that 94.4% (95% confidence interval [CI]: 93.8%, 94.9%) of eligible children 6 to 26 months of age reportedly received VAS in the previous 6 months, as did 85.8% (CI: 84.5%, 87.2%) of ineligible, 0 to 5 months old children. The longitudinal study showed that 81.6% of children surveyed within 4 weeks following a VAS campaign reportedly received VAS during the campaign and 13.4% of caregivers incorrectly reported receiving VAS when no campaign had actually occurred. False-positive reporting was more likely when oral polio vaccine (OPV) was distributed during the reporting period (20.6% vs 5.4%; P < .001). Showing a photo of OPV during the interview reduced the odds ratio (OR) of false-positive reports (OR = 0.7 [0.6-0.8]).
Conclusions:
The PEC surveys should include children outside the target age to assess targeting efficiency, and pictures of both VAS and oral vaccines distributed during the same period should be shown during interviews to enhance reporting accuracy.
Introduction
Vitamin A deficiency is a major public health problem affecting an estimated 190 million preschool-aged children, mostly in Africa and Southeast Asia, 1 and may result in xerophthalmia and excess morbidity and mortality. Several studies have shown that high-dose vitamin A supplementation (VAS) of preschool children reduces childhood mortality caused by measles 2 and severe diarrhea and dysentery, 2,3 and a recent meta-analysis concluded that VAS is effective in reducing all-cause mortality in children 6 to 59 months of age by 24%. 4 Vitamin A supplementation has been described as one of the most cost-effective interventions for increasing child survival. 3,5
Based on the health impact and low cost of VAS, the World Health Organization (WHO) recommends VAS for children 6 to 59 months of age in settings where vitamin A deficiency is a public health problem. 6 The suggested annual dosing schedule is 100 000 IU vitamin A (provided as oil-based retinyl palmitate or retinyl acetate) on 1 occasion for children 6 to 11 months of age and 200 000 IU vitamin A every 4 to 6 months for children 12 to 59 months of age. Vitamin A supplementation is not currently recommended by WHO for neonates and infants <6 months of age because of its uncertain benefit for morbidity and mortality reduction in this age range. 7,8
To achieve a measurable impact on child survival at the population level, WHO and the United Nations Children’s Fund (UNICEF) recommend that at least 80% of children 6 to 59 months old should receive 2 high-dose vitamin A capsules every year about 6 months apart in countries where the under-5 mortality rate is greater than 50 child deaths per 1000 live births. 9 According to UNICEF, in 2010, an estimated 66% of children 6 to 59 months of age worldwide received 2 doses of VAS. 10
In Burkina Faso, VAS was introduced in the 1990s and linked to national immunization days against poliomyelitis. More recently, National Micronutrient Days (NMDs) were introduced as a strategy to provide VAS to children 6 to 59 months old twice yearly. 9 These NMDs provide periodic opportunities for active distribution of VAS based on 2 scenarios: (1) fixed-post campaigns, in which caregivers take their children to the distribution site in the community and (2) door-to-door campaigns, in which the distribution teams visit all households. The UNICEF reported in 2010 that 100% of 6 to 59 months old Burkinabe children were reached with 2 VAS doses based on administrative data. 10 Data from the Orodara health district, in the southwestern region of the country, showed that VAS coverage reached 107% of children in this age range in 2009, indicating that overreporting had occurred, the true population denominator was underestimated, children outside the target age range received VAS, or some children received more than 1 capsule. Despite the reportedly high coverage, based on administrative data, it is possible that with overreporting some targeted children remained untreated. Therefore, we used information from a separate cross-sectional survey to assess the VAS coverage of young children in this health district and determine factors associated with missed coverage. We also examined longitudinal data to investigate the accuracy of reported coverage during a postevent survey and factors associated with erroneous reports.
Methods
Study Design and Population
The study was conducted in the context of a larger community-based intervention trial to assess different strategies for delivering supplemental zinc. An initial cross-sectional survey was completed to identify children eligible for the trial and to collect information on current health-related conditions, including receipt of VAS. Children who were enrolled in the longitudinal study were also reassessed monthly with regard to these issues.
Cross-Sectional Survey
From April to September 2010, we carried out a cross-sectional, community-based household survey in 106 communities in the catchment areas of 24 health centers in the southern half of the Orodara Health District in southwestern Burkina Faso (Supplement file 1). We used a 2-stage sampling procedure to identify households with children <27 months of age. In the first stage, we selected 24 health centers in the district, based on their accessibility within 90 minutes (1-way) by vehicle from the district health office. In the second stage, we selected specific communities, based on their accessibility by vehicle from the respective health centers. The participating communities represented 73% of all communities in the selected health centers’ catchment areas. According to the most recent district census data, the total population of the 106 selected communities was approximately 150 000 people, representing approximately 88% of the total population in the southern half of the Orodara Health District. 11
For the initial survey, a local guide was hired in each community to lead the survey teams to all households, with the objective of visiting 100% of the eligible concessions (extended family compounds comprised 1 or more households). Child age was calculated as the survey date minus the date of birth, which was determined from the child’s birth certificate or health card or through a local events calendar if the child’s birth certificate or health card was unavailable (12.8% of children). The survey teams revisited households when no respondents were available, and a household was dropped only after 3 failed attempts. A total of 10 454 caregivers of all children <27 months of age present in these communities were interviewed.
The survey questionnaire was developed in French and revised after pretesting. Twenty-seven locally hired interviewers were trained on the overall census questionnaire during a 2-week period using didactic sessions and supervised, simulated, and actual interviews with child caregivers. The interviewer’s standard operating procedure manual was used during the training process, and the importance of showing a picture of VAS capsules during each interview was emphasized. The interviewers were divided into 7 teams to collect information in French or Dioula (the predominant local language) on sociodemographic characteristics of the concessions, households, and mothers, as well as the child’s illness history during the preceding 24 hours. Caregivers were also asked whether their child had received a high-dose vitamin A capsule during the previous 6 months. To assist the caregiver’s recognition of VAS, a picture of the 2 different types of vitamin A capsules used during the NMD was displayed at the time of the interview. Interviewers were regularly supervised by a field supervisor and participated during refresher training sessions. The rounds of VAS distribution prior to and during the survey took place in May and December 2009 and May 2010. An average of 2.9 ± 1.4 standard deviation (SD) months had elapsed between the most recent VAS campaign and the time of the interview.
Longitudinal Assessment
An intervention trial to assess different zinc intervention strategies was conducted in the same communities among 6365 children 6 to 30 months of age. The 24 health center catchment areas were divided into 36 clusters. Individual clusters were stratified by selected indicators (urban/rural; distance from main hospitals) and assigned within strata to different interventions. These children and their caregivers were visited weekly from December 2010 through February 2012.
For the purpose of the present analyses, a dietary and health practices questionnaire was completed every 4 weeks, usually with the primary caregiver. The questionnaire was designed to elicit information on dietary practices, the use of mosquito nets, and the reported receipt of VAS. Similar to the initial survey, caregivers were shown a picture of the 2 different types of vitamin A capsules used during VAS campaigns and asked whether their child received a capsule during the 4 previous weeks. Six months after the beginning of the longitudinal study, we also began presenting a photo of the locally administered oral polio vaccine (OPV) because several polio vaccine campaigns were conducted in the study area. Caregivers were asked whether their child received the VAS and/or OPV over the same reference period. Throughout the longitudinal study, two 4-day VAS campaigns took place in March and October 2011. All children enrolled in the trial were within the target age range of the VAS campaigns.
Ethics
The survey and the longitudinal study were part of the initial protocol of the zinc supplementation trial, which was approved by the Institutional Review Boards of the Centre Muraz in Bobo-Dioulasso (Burkina Faso) and the University of California, Davis, USA. Oral parental consent was obtained for participation in the survey, and written consent was obtained for participation in the longitudinal trial. The trial was registered at www.clinicaltrials.gov as NCT00944359.
Statistical Analysis
Data were double-entered and compared using EpiData Entry version 3.1 (Odense, Denmark). All statistical analyses were performed using the SAS System version 9.3 (SAS Institute, Cary, North Carolina). A community was defined as urban when the locality performed the functions of the chief town of an administrative unit (region and province) or if the total population was >5000, and a school, administrative services, public water system, and electricity were available.
Household economic status was characterized using data on household assets (plow, cart/wagon, sprayer, farm animals, television, solar panel, radio, portable telephone, bicycle, and motorcycle) and housing characteristics (construction materials for walls, floors, and roofs; drinking water supply; and waste disposal facilities for the concession). 12 Factor analysis was used to assess which variables were correlated, and principal component analysis was used to construct a single, summary variable representing household assets and infrastructure as a proxy for relative economic status among households. This variable was then split into quintiles to create a categorical variable indicating households and concessions with the highest, high, medium, low, or very low economic status.
For the longitudinal study, reported receipt of VAS in the past 4 weeks was considered possibly valid when this was reported during the 4 weeks following each VAS campaign if the respondent stated that VAS was received during a VAS campaign. Positive responses reported during the remaining periods were considered false-positives, as the most recent VAS campaign had occurred more than 4 weeks before the interview.
For both studies, bivariate analyses were completed to describe the relationship between reported VAS receipt and all relevant variables. Odds ratios (OR) of positive and false-positive receipt of vitamin A were estimated by logistic regression with the GENMOD procedure for binary distribution in SAS. Only covariates significantly associated with the outcome at a level of significance of 10% were included in the final models. A P value < .05 was considered as statistically significant. Multiple comparisons of group means within covariates were performed using least square means by the Tukey–Kramer adjustment. For the cross-sectional survey, results from children ≥6 months and <6 months of age at the time of VAS were analyzed separately. For the longitudinal study, cluster and repeated monthly interviews of caregivers were considered as random effects and stratum as a fixed effect.
Results
Cross-Sectional Survey
Study site and baseline characteristics of study population
During the cross-sectional survey, interviews were completed with 10 454 caregivers of 10 571 children <27 months of age (Figure 1). The total number of households visited represented 100% of those identified by local guides in each village. Someone was present in the concession at the time of the visit for 99.9% of the concessions, and when someone was present, 99.7% of them consented to participate in the survey. The vast majority (91.6%) of the respondents were the mothers of the identified target child. The demographic and socioeconomic characteristics of the entire sample are shown in Table 1. The majority of caregivers (71.6%) had not received any formal education and most worked on household farms or as merchants.
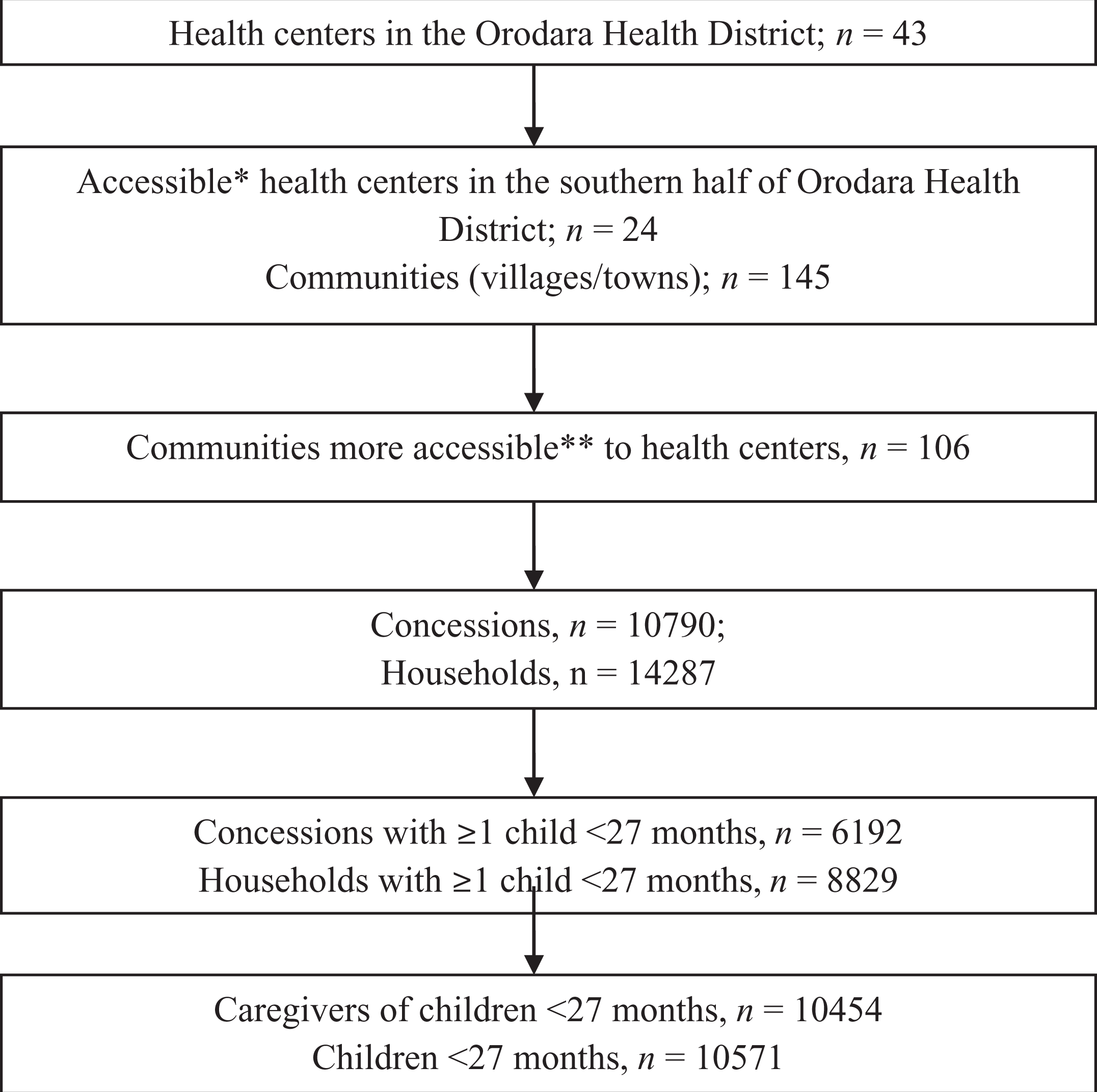
Summary of sampling framework for the cross-sectional survey of vitamin A supplementation coverage. *Accessible was defined as located less than 90 minutes by vehicle from the district health office (1-way, dry season). **More accessible was defined as accessible by vehicle.
Demographic and Socioeconomic Characteristics of the Participants in the Cross-Sectional Survey.
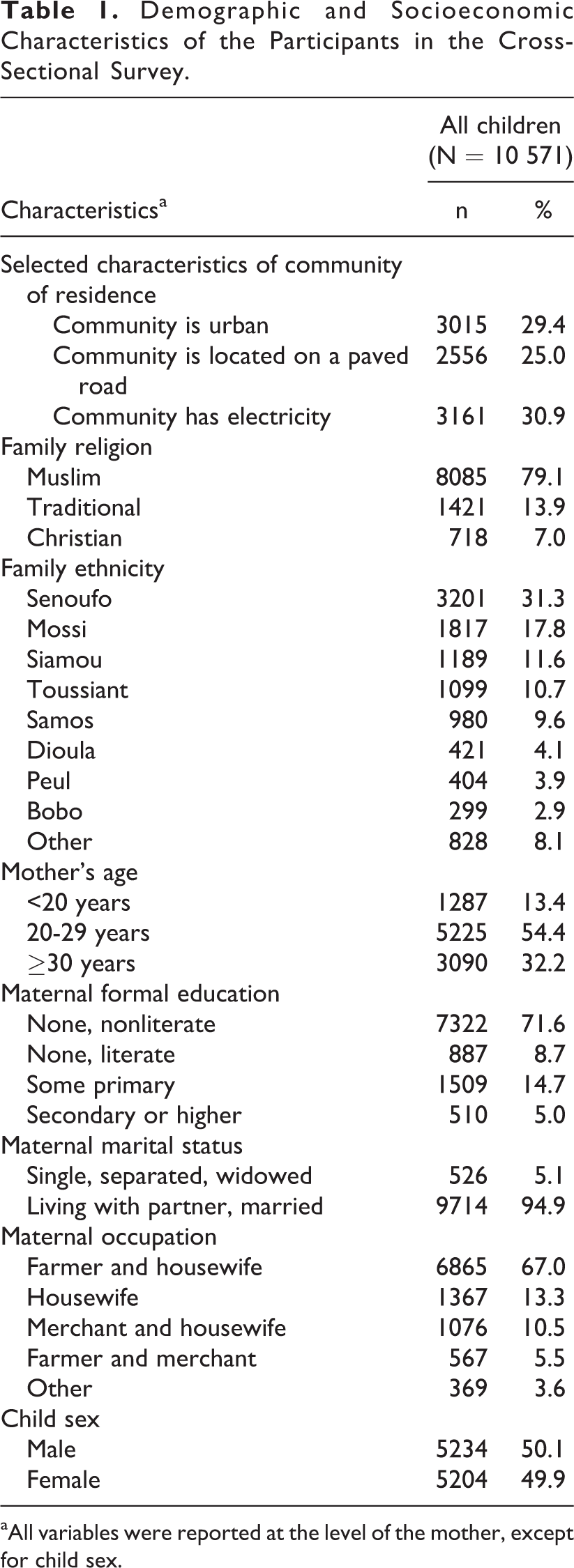
aAll variables were reported at the level of the mother, except for child sex.
Vitamin A supplementation coverage among eligible children
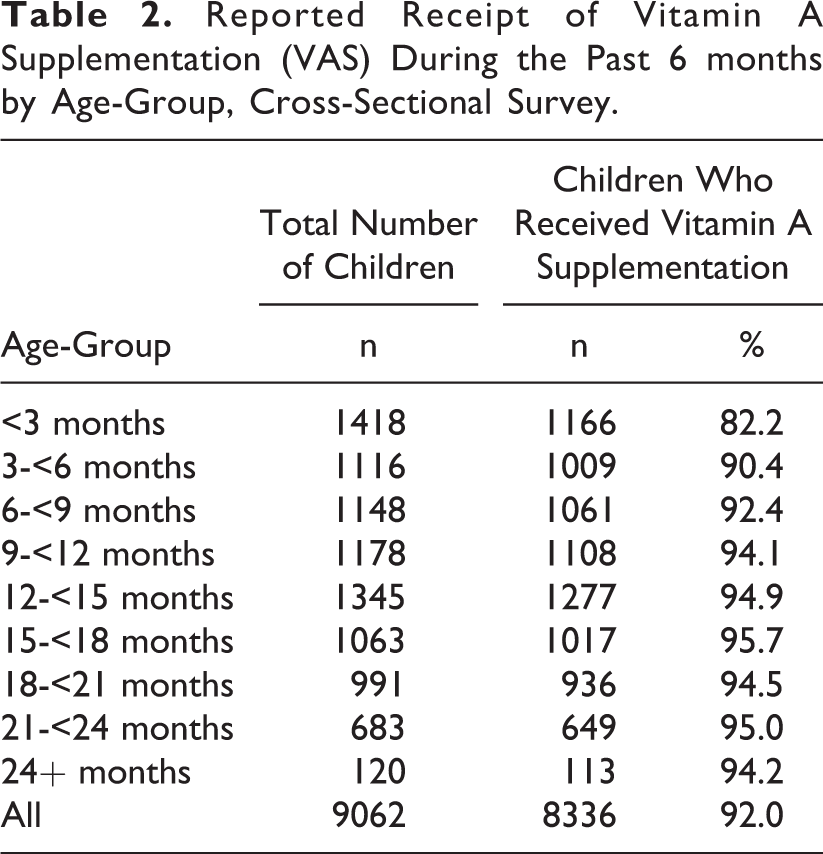
Interviews with village leaders confirmed that all communities participated in the national VAS campaign during the previous 6 months. Among all children <27 months of age with data on VAS receipt (n = 9062), 92.0% reportedly received VAS during the past 6 months (Table 2). According to national policy in Burkina Faso, children who were <6 months of age at the time of the NMDs are not eligible to receive VAS.
Reported Receipt of Vitamin A Supplementation (VAS) During the Past 6 months by Age-Group, Cross-Sectional Survey.
Among 6591 children ≥6 months of age at the time of each NMDs, data on receipt of VAS were available for 6528 children. Of these children, 94.3% reportedly received VAS. Multivariable analysis showed that children living in rural communities were more likely to receive VAS (96.5%) than those living in urban areas (89.9%; P < .001; Table 3). Children whose residence was located on a paved road were less likely to receive VAS (93.9%) than other children (95.5%; P = .010), but children in villages with electricity were more likely to receive VAS (97.2%) than children in villages with no electricity (93.9%; P < .001). Children of families who relocated during the rainy season to work in the family fields were less likely to receive VAS (91.3%) than those who remained at their primary residence all year (95.3%; P = .003). Children of uneducated but literate mothers had the lowest reported receipt of VAS compared with children of nonliterate or educated mothers (92.9% vs 94.8%-96.0%; P = .041). Also, children whose mother was not a farmer (91.5%-93.4%) were less likely to receive VAS than children whose mother was a farmer and housewife (95.9%; P < .001). Multivariable analysis showed no significant difference in reported VAS receipt by child sex, age, or maternal age.
Factors Associated With Reported Receipt of VAS During the Past 6 Months by Selected Characteristics, Cross-Sectional Survey.a
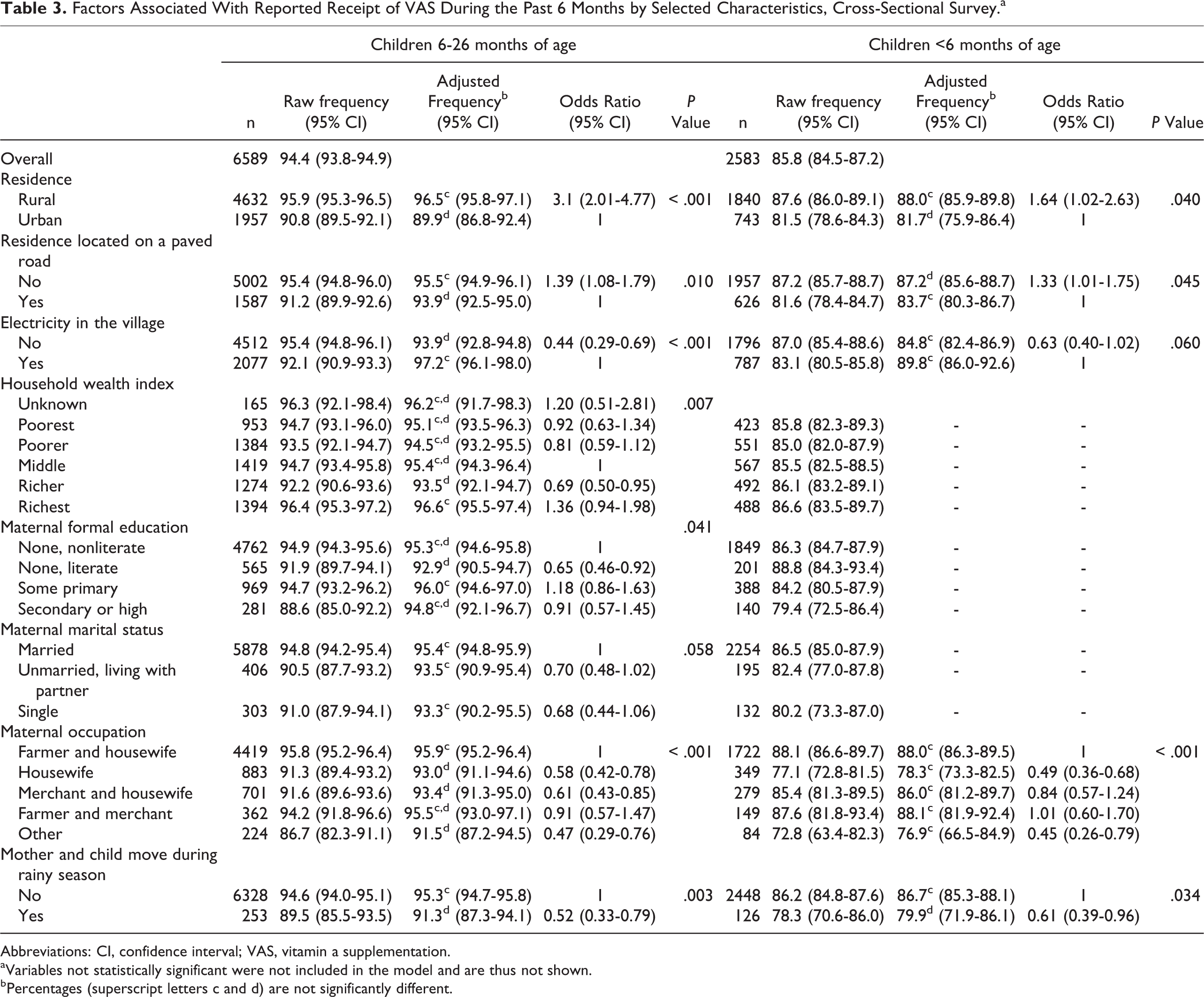
Abbreviations: CI, confidence interval; VAS, vitamin a supplementation.
aVariables not statistically significant were not included in the model and are thus not shown.
bPercentages (superscript letters c and d) are not significantly different.
Reported receipt of VAS among noneligible children (<6 months of age)
Among noneligible children for whom information was available, 85.8% reportedly received high-dose vitamin A capsules. Rural residence, house location on a paved road, occupational status of the mother, and non-relocation near the family field during rainy season were all associated with the reported receipt of VAS, similar to the reports for children >6 months old (Table 3). A total of 1205 caregivers were interviewed whose children were not yet born at the time of the most recent round of VAS distribution. Notably, 57.3% of caregivers of those unborn children reported that their infants had received high-dose VAS.
Longitudinal Study Assessment
In total, 6232 caregivers of 6365 children 6 to 30 months of age participated in the longitudinal study, during which 45 087 monthly interviews took place during 15 months. A total of 5927 of these interviews occurred during the 4 weeks following a VAS campaign (Figure 2).
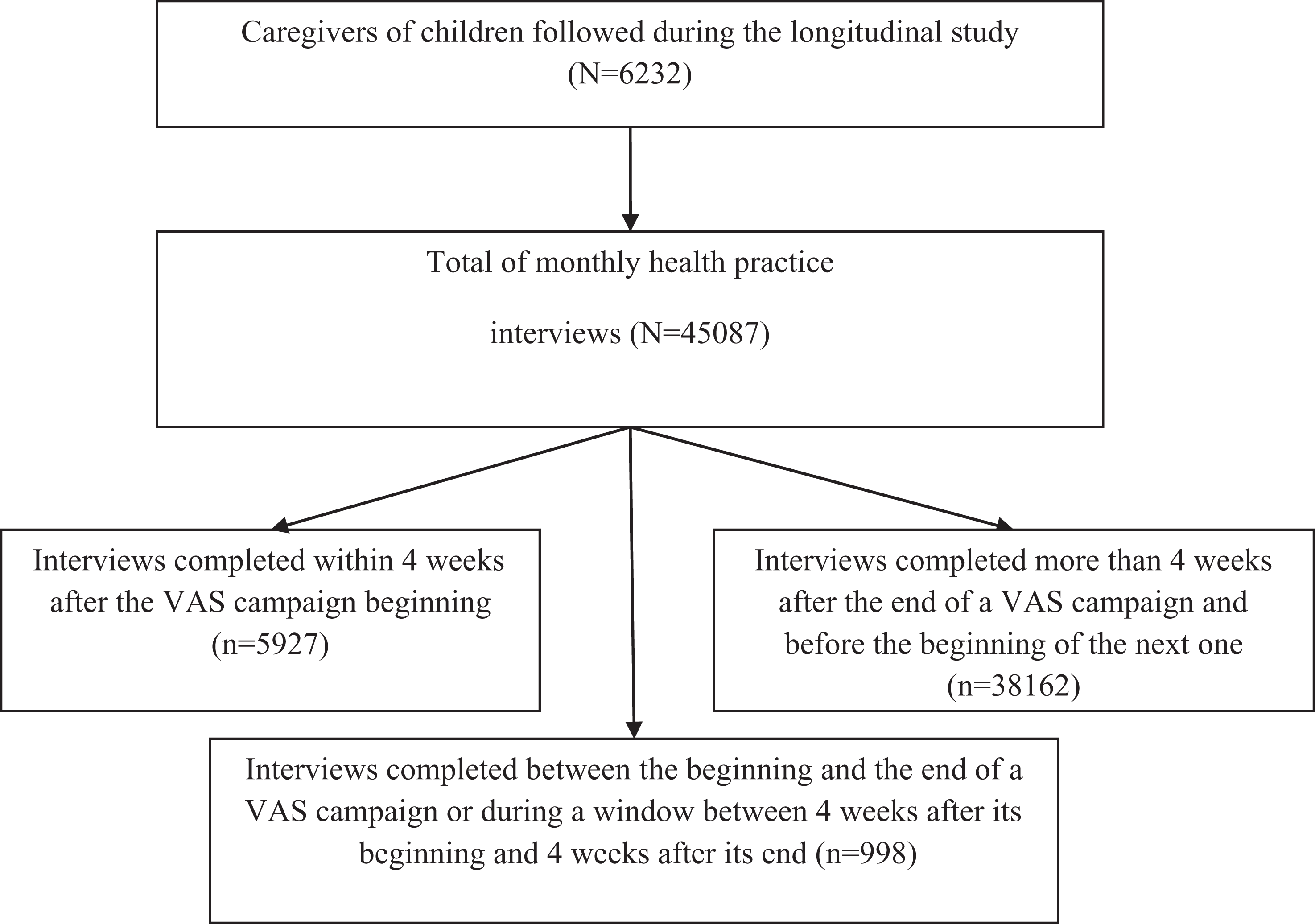
Flowchart of interviews during the longitudinal survey on vitamin A supplementation coverage.
Positive reports of VAS receipt among young children after a campaign occurred
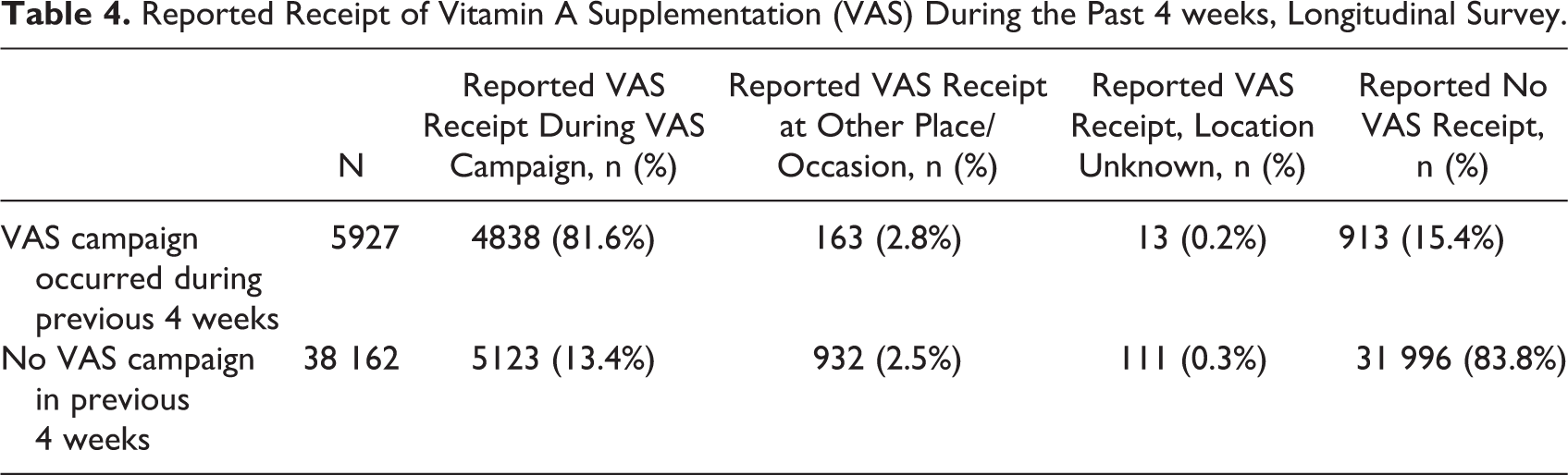
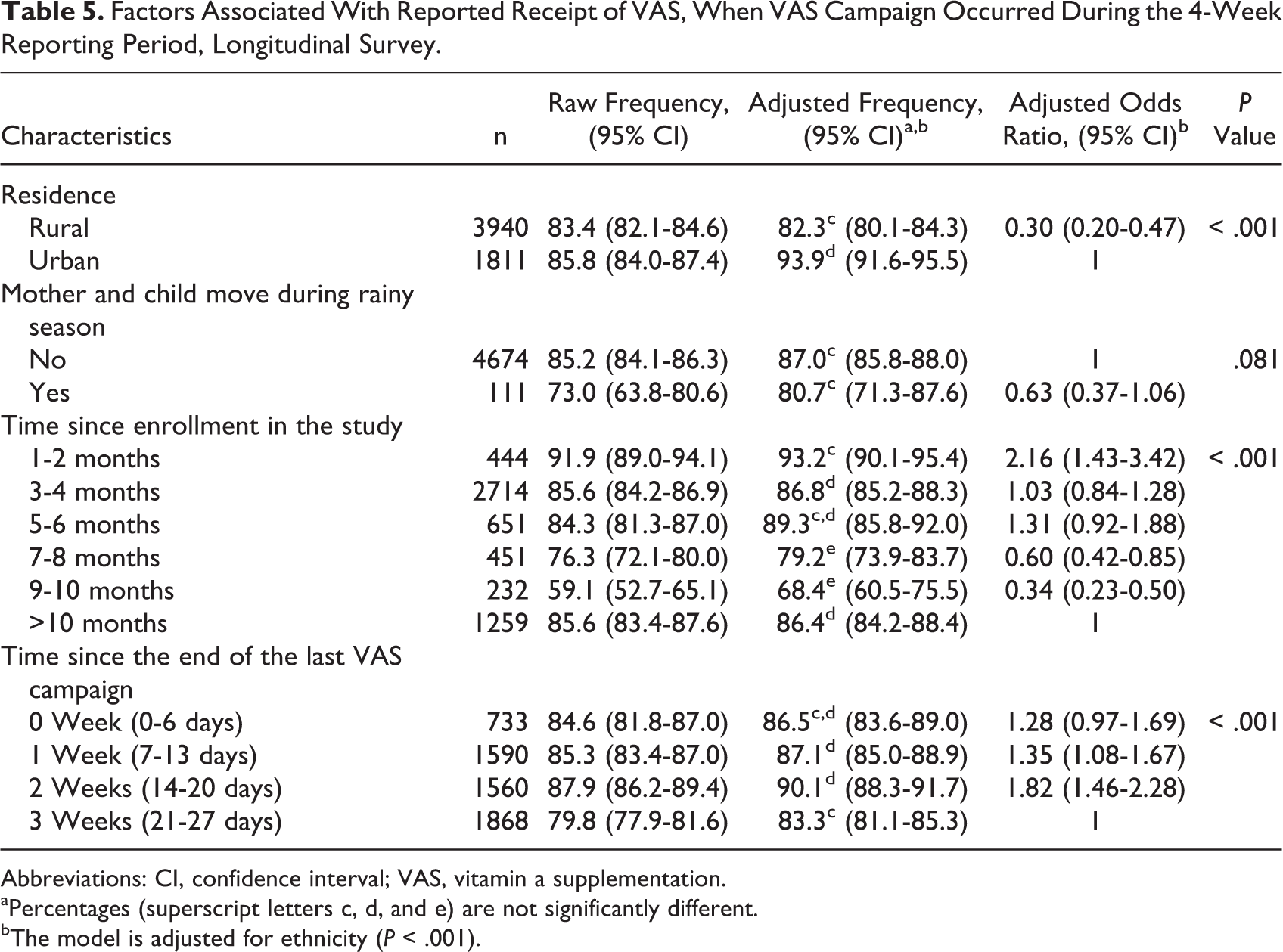
During the 4 weeks following a VAS campaign, 84.6% of children reportedly received VAS and 81.6% of the children reportedly received it during an NMD (Table 4). Multivariable analysis showed that positive reports were less likely in rural villages (82.3%) than in urban areas (93.9%; P < .001; Table 5). Caregivers were more likely to report that their child received VAS during the earlier months of the longitudinal study than during the later months (93.2% if enrolled in the study in the previous 9 months vs to 68.4%-86.4% if enrolled >9; P < .001). Reported receipt of VAS was also greater when the interview occurred 1 (87.1%) or 2 (90.1%) weeks after the campaign, as compared to 3 weeks after the campaign (83.3%; P < .001).
Reported Receipt of Vitamin A Supplementation (VAS) During the Past 4 weeks, Longitudinal Survey.
Factors Associated With Reported Receipt of VAS, When VAS Campaign Occurred During the 4-Week Reporting Period, Longitudinal Survey.
Abbreviations: CI, confidence interval; VAS, vitamin a supplementation.
aPercentages (superscript letters c, d, and e) are not significantly different.
bThe model is adjusted for ethnicity (P < .001).
False-positive reports of VAS receipt among young children based on caregivers’ report
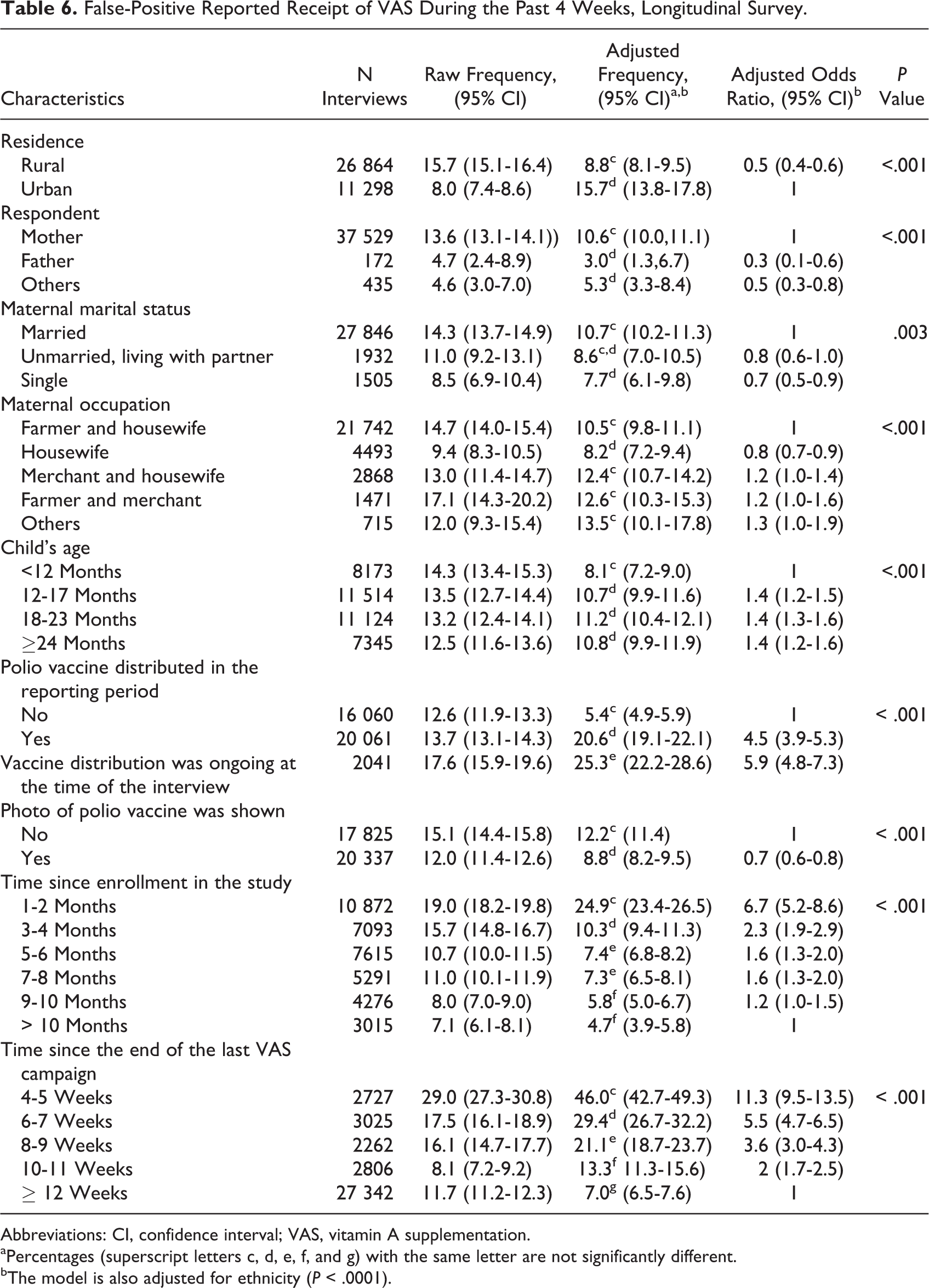
Among 38 162 interviews carried out more than 4 weeks after a VAS campaign, 13.4% of caregivers reported that their child had received VAS during a campaign in the past 4 weeks. Therefore, their responses were considered as false-positive responses (Table 6). After controlling for all significant covariables, including ethnicity (P < .0001, results not shown), false-positive responses were less likely in rural areas (8.8%) than in urban areas (15.7%; P < .001); when respondents were not the mother (3.0%-5.3% vs 10.6%; P < .001); when the mother was a housewife (8.2%) as compared to any other occupation (10.5%-13.5%; P < .001); when the mother was single (7.7%) as compared to married (10.7%; P = .003); and when children were less than 12 months old (8.1% vs 10.7%-11.2%; P < .001).
False-Positive Reported Receipt of VAS During the Past 4 Weeks, Longitudinal Survey.
Abbreviations: CI, confidence interval; VAS, vitamin A supplementation.
aPercentages (superscript letters c, d, e, f, and g) with the same letter are not significantly different.
bThe model is also adjusted for ethnicity (P < .0001).
Also, false-positive responses were more likely when OPV was distributed during the reporting period (20.6% vs 5.4%; P < .001), but showing a photo of OPV at the time of the interview reduced the OR of a false-positive report (OR = 0.7 [0.6-0.8]). Finally, false-positive reports were more common when the interview occurred shortly after the last VAS campaign (P < .001) and when the interview took place earlier in the course of the longitudinal study (P < .0001), and gradually reduced with time in both cases (from 46.0% when interview occurred 4-5 weeks after VAS to 7.0% when interview occurred 12 or more weeks after VAS and from 24.9% if enrolled in the study 1-2 months ago vs 4.7% if enrolled >10 months ago).
Discussion
Reported VAS coverage was high (94.4%) among eligible children 6 to 26 months of age in the study area. This is substantially higher than the results from the 2006 Burkina Faso Multiple Indicator Cluster Surveys (MICS), in which 67% of children 6 to 59 months of age reportedly received VAS within the previous 6 months 13 but similar to a more recent postevent coverage (PEC) survey done in 2012, in which 90.6% of 6 to 59 months old children reportedly received VAS. 14 In the health district where we implemented the survey, VAS coverage based on the disappearance of vitamin A capsules was 107% in 2009. 15 The information on health district coverage is based on administrative data from “tally sheets,” completed during VAS campaigns, whereas information from our study was based on household surveys in which the respondents were shown a photo of a child receiving a vitamin A capsule. A similar discrepancy was found in a recent survey in Sierra Leone, where 91.8% coverage was reported in the PEC survey compared to 105.1% coverage from tally sheets. 16 Analyses of our survey results showed that the reported receipt of VAS was high among noneligible children (<6 months old), although VAS is not recommended for children <6 months due to the limited evidence of its effect on morbidity and mortality reduction. 8 This practice would result in an overestimation of the proportion of eligible children who received VAS during campaign events when coverage rates are based on the disappearance of supplements and the estimated number of children 6 to 59 months of age. 17
In our study, the apparent high coverage of noneligible children below 6 months of age could be explained by the difficulty in ascertaining the children’s age. Moreover, refusing to supplement a child brought by a parent to the site of distribution may be frustrating for both the parent and the community health agent. 18 To permit appropriate targeting of eligible children, children’s parents must be sensitized to register their children’s birth, and birth certificates or health cards should be checked during the NMDs. In addition, the VAS program should develop simple tools based on the conventional calendar and dates of important local events to define the target age range for each round of NMDs, and the VAS distributors should be trained to target only eligible children 6 months to 5 years of age. The PEC surveys also should include coverage assessment among ineligible children to evaluate if supplements were correctly targeted only to eligible children.
The apparent high coverage of noneligible children could also be explained by false-positive reports of VAS receipt when no VAS distribution had actually occurred, as in the case of infants who had not been born at the time of the previous round of distribution but were nevertheless reported to have received the supplements. These were almost certainly false-positive responses because VAS was generally not available in health centers or pharmacies in the study area, so VAS was only available during campaigns. It is possible that caregivers confused VAS with other items, such as orally administered vaccines.
Reported receipt of VAS among eligible, 6 to 27 months old children, was also high (82%) in the longitudinal study, but approximately 12% less than the coverage reported in the cross-sectional survey (94%). This may reflect a true difference in coverage across the different campaigns held in 2010 and 2011 or may be due to the methodological differences in the 2 sets of interviews. For example, the reporting periods were just 4 weeks during the longitudinal study versus 6 months in the cross-sectional survey, and the caregivers were visited repeatedly by the same enumerator during the longitudinal study, which allowed for training of the respondent and greater rapport with the interviewer. In addition, a photo of OPV was shown with the vitamin A photo during 53% of interviews in the longitudinal study but never in the cross-sectional study. Analyses of the longitudinal study results allowed us to explore how these factors could affect the validity of VAS PEC assessments. First, regarding the reporting period, the longitudinal study indicated that there was some confusion regarding the 4-week reporting period. It is possible that 3 or 4 weeks after the campaign, fewer caretakers reported receipt of vitamin A because they were under the impression that the campaign happened >4 weeks ago, and that 4 to 5 weeks after the campaign, a sizeable portion of caretakers reported receipt of vitamin A because they thought the campaign happened less than 4 weeks ago. To avoid this source of error, reporting periods that include the time of VAS should be carefully defined during routine surveys, like demographic and health surveys and MICS, using well-known local events. This observation also supports the current guidelines for PEC surveys, which suggest that PEC surveys should be implemented within 4 to 6 weeks of the VAS campaign to ensure accurate recall by the caretaker. 19 False-positive reports were also high when OPV was distributed during the reporting period and when no photo of OPV was shown during the interview. As both VAS and OPV are given orally, they may be confused by caregivers. Part of the higher coverage shown in the cross-sectional survey, during which no photo of OPV was shown, may be attributable to false-positive answers due to confusion between VAS and OPV, and also suggests a need for more education of caregivers about the nature and purpose of the different interventions.
Some sociodemographic factors also were associated with false-positive reports. For example, when the child was older than 12 months, when the respondent was the mother, when the mother was married (as compared to single), when the mother was occupied outside the home, and when the household was located in urban area, false-positive reports were more likely to occur. It is possible that these factors are related to the greater knowledge of vitamin A and/or other oral vaccines leading to overreporting.
Residing in an urban area was also related to reported VAS coverage in both the cross-sectional and longitudinal survey, but in different directions. In the cross-sectional survey, more caregivers in rural communities reported that their child had received VAS, whereas the opposite was true in the longitudinal study. Because the cross-sectional survey and the longitudinal survey assessed the coverage of different VAS campaigns, it is possible that the difference in reported coverage by site of residence was real. Cross-sectional surveys in other countries found inconsistent results for coverage in urban and rural settings. A VAS coverage survey in Guinea found that more 6 to 59 months old children living in rural areas reportedly received VAS than in urban areas. 17 In contrast, a survey in Mali reported lower VAS coverage in rural areas. 18 Thus, the practical implications of the current findings are uncertain. The other sociodemographic factors significantly associated with VAS coverage in the cross-sectional survey were not associated with VAS coverage in the longitudinal survey.
There are several limitations of the present analyses. First, the study was limited to 1 health district, and the results are not necessarily representative of the entire Orodara region or Burkina Faso as a whole. Because the primary purpose of the cross-sectional survey was to identify young children in the community for a subsequent intervention trial, only more accessible communities were selected. Although our survey included 88% of the population in the southern Orodara Health District, VAS coverage may be different in less accessible communities. Second, we cannot rule out the possibility that some of positive reports during the cross-sectional study were due to receipt of VAS during clinic visits. However, this is not likely because VAS supplies were reportedly infrequently available in health clinics and pharmacies. Thus, we assumed that any reported receipt of VAS occurred during the NMDs. Third, we did not ask about the color of VAS capsule and can therefore not assess whether the correct dosages were provided. Finally, because the administration of VAS was not directly observed, we cannot state whether some of the negative reports were false-negative reports, and we could not study factors related to false-negative reports.
Despite these limitations, the study has a number of strengths including the large sample size, the fact that majority of our respondents were the child’s primary caretaker and the mixed cross-sectional and longitudinal components of the analyses. To our knowledge, this was the first community-based study to assess the unintended VAS coverage of 0 to 6 months old children and to explore factors affecting the accuracy of VAS PEC measurement and factors related to correct reporting.
Conclusions
Vitamin A supplementation coverage was reportedly high among young children in southwestern Burkina Faso during the period of the present study. A large proportion of children below the minimum target age (<6 months) reportedly received VAS. Improved targeting to children in the recommended age range will require reinforcement of staff training and use of birth certificates and local calendars to identify the eligible children correctly. The PEC surveys should be scheduled as soon as possible following VAS campaigns, and pictures should be shown of both VAS and any oral vaccines distributed during the same period to enhance the accuracy of reported coverage. The PEC surveys should also include caregivers of children outside the target age (ie, children <6 and >59 months) to determine whether the supplements were correctly targeted.
Footnotes
Authors’ Note
Césaire T. Ouédraogo, Sonja Y. Hess, Elodie Becquey, and Kenneth H. Brown conceived and designed the study. Césaire T. Ouédraogo, Shelby E. Wilson, Elodie Becquey, Amadou Ouédraogo, Noël Rouamba, and Lea Prince contributed in study implementation and data collection in the field. Césaire T. Ouédraogo and Elodie Becquey contributed in data analysis. Césaire T. Ouédraogo, Sonja Y. Hess, Elodie Becquey, Kenneth H. Brown contributed in interpretation of results. Césaire T. Ouédraogo and Sonja Y. Hess prepared a first draft of the article. All co-authors contributed in critical review of the manuscript. All authors read and approved the final manuscript. The authors are grateful to the entire study team, including the data collection and data entry teams and other support staff. Our sincere appreciation goes to the staff at the Orodara Health District and the Helen Keller International office in Ouagadougou for their support. The authors thank Judicaël Somé, Oula Ouattara, and Honoré Konaté (Institut de Recherche en Sciences de la Santé, Bobo-Dioulasso) for assistance with the study implementation, Janet M. Peerson and Mark Dakkak (University of California, Davis) for help with statistical analyses, and Jessica Blankenship (HKI, Kenya) for valuable comments on the draft manuscript. Finally, the authors sincerely appreciate the support of the children, their parents, and local communities whose participation and support made this study possible.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Thrasher Research Fund and the Canadian International Development Agency through a grant to Helen Keller International. The funding agencies had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. No additional external funding was received for this study.