
Abstract
Objective:
A healthy diet during pregnancy is essential to ensure optimal fetal growth and development. Women’s awareness of dietary guidelines may assist them in following a healthy diet for themselves and their unborn babies. The Institute of Medicine and the American College of Obstetrics and Gynecology have published recommendations concerning the nutrition of pregnant/nursing women. The Israeli Ministry of Health has adopted these recommendations in revised guidelines published in 2015. The aim of this study was to describe the dietary habits among pregnant/nursing women in Israel and to assess the correlation between socioeconomic parameters and adherence to those guidelines.
Methods:
We performed a cross-sectional survey by interviewing pregnant/lactating women attending family health centers (FHC) in different areas of Tel Aviv, Israel.
Results:
One-half of the 239 recruited women reported having been informed of the guidelines for dietary changes during and after pregnancy, 30% by a professional source. Women in a lower socioeconomic status (SES) consumed more undercooked (rare) beef, raw fish, and caffeine compared to women in a higher SES (P = 0.03 and P = 0.003, respectively). The former was less compliant with the recommendation for folic acid supplementation (155 [(88.1]) vs 47 [(77]), P = 0.05) and less likely to use other dietary supplements during pregnancy, e.g., multivitamins and omega 3, than the latter (P = 0.01 and P < 0.001, respectively).
Conclusion:
This survey revealed deficiencies in adherence to the implementation of medical guidelines to nutrition during and after pregnancy, as well as gaps between women of different SESs, mostly in the use of dietary supplements.
Introduction
A healthy diet and lifestyle during pregnancy are essential to ensure optimization of fetal growth and development. 1 Inappropriate nutrition and poor perinatal growth are associated with increased risk of respiratory disease, atopy, adiposity, and osteoporosis in later life. 2 -5 Women’s accurate knowledge of dietary guidelines during pregnancy may assist them in making appropriate food choices and in achieving a balanced diet for themselves and their unborn babies. The Institute of Medicine and American College of Obstetrics and Gynecology have published recommendations concerning the nutrition of pregnant and lactating women. 6,7 The Israeli Ministry of Health has adopted these recommendations in a revised guideline that was published in 2015. 8 Nutritional advice during pregnancy includes a balanced daily diet, avoidance of raw fish and undercooked (rare) steak and hamburger meat, limitation of caffeine and alcohol intake, and greater consumption of foods rich in calcium, omega 3, and iron. The main supplementation recommendation includes supplements of folic acid and iron. Iron is recommended to maintain body stores and minimize the occurrence of iron deficiency anemia. 9,10 Folic acid is recommended starting from 1 month before conception for the prevention of neural tube defects. 11 A recently published meta-analysis showed that fortified food products were effective in increasing birth weight and reducing the incidence of low birth weight. 12 Another report noted that while lifestyle habits are essentially under maternal control, they can be influenced by the health-care provider. 13 The aim of this study was to describe maternal dietary and lifestyle habits among pregnant and lactating mothers in Israel and to compare them to the national recommendations. Our second aim was to assess the correlation between socioeconomic parameters and adherence to these guidelines.
Methods
Participants
The study was designed as a cross-sectional survey that was conducted between February 1, 2015, and January 31, 2016. The participants were mothers of healthy infants aged 6 months or less who were born no earlier than week 35 of pregnancy. Participants who met the inclusion criteria were recruited among the mothers visiting the public well-baby clinics (“Tipat Halav”) of family health centers (FHCs) of 6 different areas of Tel Aviv, Israel. Data were collected via a questionnaire administered by 2 trained interviewers (S.B. and A.F.) during personal interviews. The questionnaire was developed by the author (R.L.), who is a specialist in nutritional science, and was based on similar surveys that assessed nutrition and the use of supplements during pregnancy. 3,14 This survey was approved by the local Institutional Ethics Committee. Socioeconomic status (SES) was estimated according to several proxy measurements for each infant. We adopted Max Weber’s view and assessed separate but linked dimensions of social class: class (economic) and status (social). 15 A basic assumption of our study was that location of the FHCs is a good proxy marker for the SES of mothers visiting it. Family health centers were chosen for the study and classified as low/intermediate/high SES in cooperation with the Tel Aviv municipality social services administration. Additional proxy measurements for SES were the number of years of education of the participant and her spouse, which had also been reported as being good markers for SES, 14,15 as was the ratio between the number of residents and the number of rooms in the family residence. 16 We chose not to relate directly to income as a marker of SES in order to avoid a low and biased response to a survey question on this subject. 16
Measurements
The questionnaire was divided into 4 parts: demographic characteristics, clinical parameters regarding pregnancy and delivery, eating habits during pregnancy, and the use of supplements before and during pregnancy. Demographic parameters for all infant–mother dyads included characteristics of the parents (age, marital status, ethnic origin, and maternal body mass index [BMI] before pregnancy and before labor). Clinical data include medical history of the pregnancy (gravidity, parity, prenatal care, gestational age at delivery, and mode of delivery) and the infant (birth weight). Nutrition data included number of food items that were consumed in a week; foods rich in calcium (diary; glass of milk, yogurts, cheese, almonds, sesame, and sardines); foods rich in iron (beef, chicken, turkey, and legumes), liver, fish and seafood dishes, and caffeinated beverages (tea, coffee, and energy drinks); and food items that were consumed during all pregnancy: alcohol, organic food, and raw fish and uncooked beef. The mothers were asked about dietary consumption of food items during pregnancy compared to before pregnancy. Dietary supplements that were studied included folic acid, iron, multivitamin, omega 3, vitamin D, calcium, and probiotics. The mothers were also instructed to add other supplements if they were used and to write when they started to use the supplements before or during pregnancy.
Data Analysis
The statistical analysis was performed using SPSS (version 21.0; SPSS Inc, Chicago, Illinois). Descriptive statistics were examined for all variables. Continuous variables were expressed as median with range when they were not normally distributed and were expressed as mean (standard deviation [SD]) for normally distributed variables. Categorical variables were presented as number and percentage. Differences in all variables between 3 SES groups were examined using 1-way analysis of variance for continuous variable and the χ2 or Fisher exact test for categorical variables. A P value ≤ .05 was considered significant.
Results
The demographic characteristics of the participants in this study are presented in Table 1. We recruited 239 mothers with a mean age of 33.2 ± 5.6 years. Only 11% of mothers reported having medical problems during pregnancy, such as gestational diabetes (n = 6), preeclampsia (n = 4), intrauterine growth retardation (n = 3), hypothyroidism (n = 2), and maternal cholestasis (n = 2). Seven mothers reported having anemia during pregnancy. None of the infants had known nutritional deficiencies or neural tube defects. As expected, both parents had significantly more years of education, and the residence index was lower in FHCs that were located in areas of higher SESs (P < .001 and P = .003, respectively). Women from a higher SES had a significantly lower BMI before pregnancy compared to woman from a lower SES. There was no significant difference in BMI before labor associated with SES.
Maternal and Neonatal Characteristics.
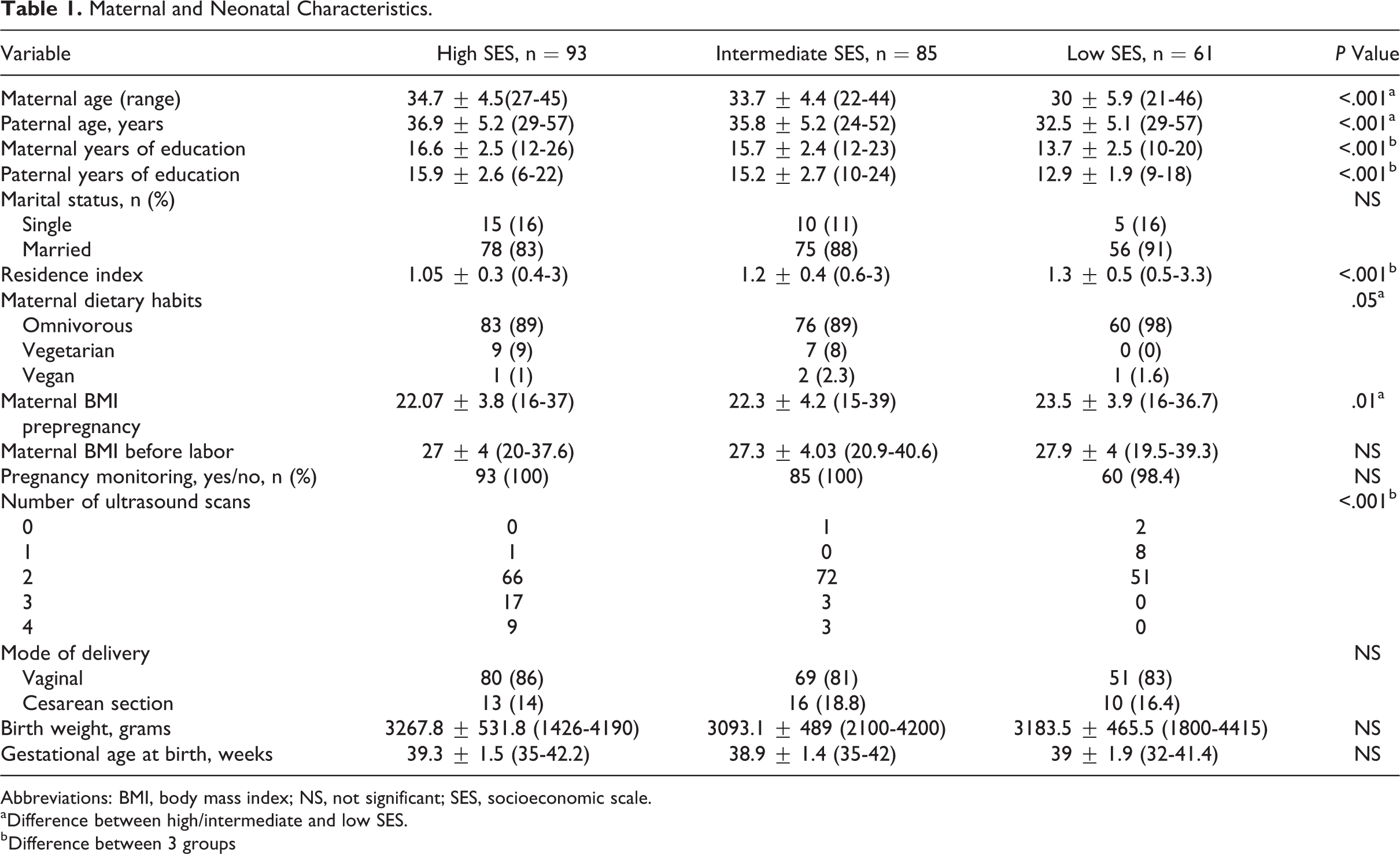
Abbreviations: BMI, body mass index; NS, not significant; SES, socioeconomic scale.
aDifference between high/intermediate and low SES.
bDifference between 3 groups
Nutrition During Pregnancy: Awareness of and Application of Ministry of Health Guidelines
Figure 1A displays the information sources nutritional guidelines. One-half (118) of the participants reported being aware of nutritional guidelines for pregnant woman. Sixty percent of the mothers relied on professional consultation (36% physician, 31% dietitian, and 33% nurses), while the other 40% obtained information from nonprofessional sources (friends, the internet, etc). Notably, there were no differences between SESs in the level of awareness of dietary guidelines or in the sources of information (P = .9 and P = .5, respectively).
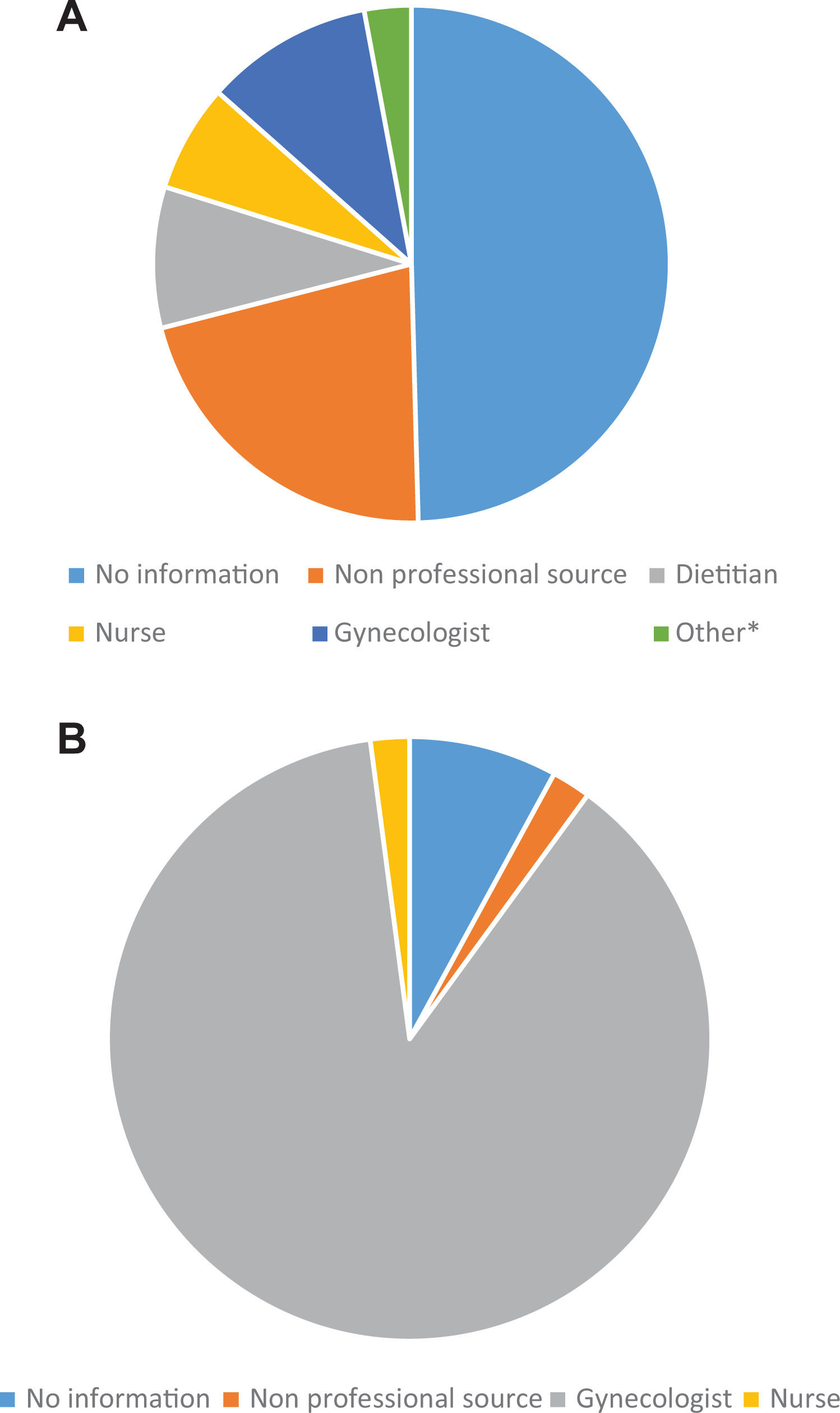
A, Information source for nutritional guideline. B, Information source for dietary supplements. *Other: naturopathic, breastfeeding consultant, midwife, and nurse.
Table 2 lists quantitative data on the consumption of food items during pregnancy as described by the participants. They were also asked about consumption of food items during pregnancy compared to before pregnancy. We divided the participants into one group of high SESs (which was comprised of both high and intermediate SESs) and the other of low SESs. Most of the women followed the nutritional guidelines to minimize consumption of alcohol, caffeine, and undercooked (rare) red meat and raw fish, but there were significant differences between the SES groups: Women from higher SESs consumed fewer caffeinated beverages and less undercooked red meat and raw fish and decreased their alcohol intake compared to their prepregnancy levels (8.6 ± 7.6 caffeinated items per week in high SESs compared to 10.2 ± 11.6 in low SESs, P = .003; 4 women in high SESs consumed raw meat compared to 11 women in low SESs, P = .008; and 28% of women in lower SESs decreased their alcohol consumption compared to 50% in high SESs, P = .007). The average consumption of food items rich in calcium for the entire study cohort was 6.67 ± 3.7 items per day, with no significant difference between the SES groups. Thirty-three percent (n = 81) reported to have increased the consumption of foods rich in calcium, while most of the participants (n = 155, 64%) did not change their calcium consumption. Women from lower SESs were less likely to increase their calcium intake (63 vs 18, P = .04). Women from higher SESs consumed significantly less food rich in iron (2.6 ± 2.7 vs 3.5 ± 2.8 for lower SESs, P = .03). Twenty-four percent (n = 57) reported an increased consumption of food rich in iron, while the others made no changes in their iron consumption (61%, 147). Women from lower SESs were less likely to increase their iron intake during pregnancy (46 vs 11, P = .04). Twenty-five percent (n = 60) of the participants reported consuming solely organic food items in combination with other food items, with a significant difference in organic food consumption between the different SES groups (ie, higher consumption in higher SESs, 55 [29%] vs 5 [8%], P = .001).
Consumption of Food Items During Pregnancy.
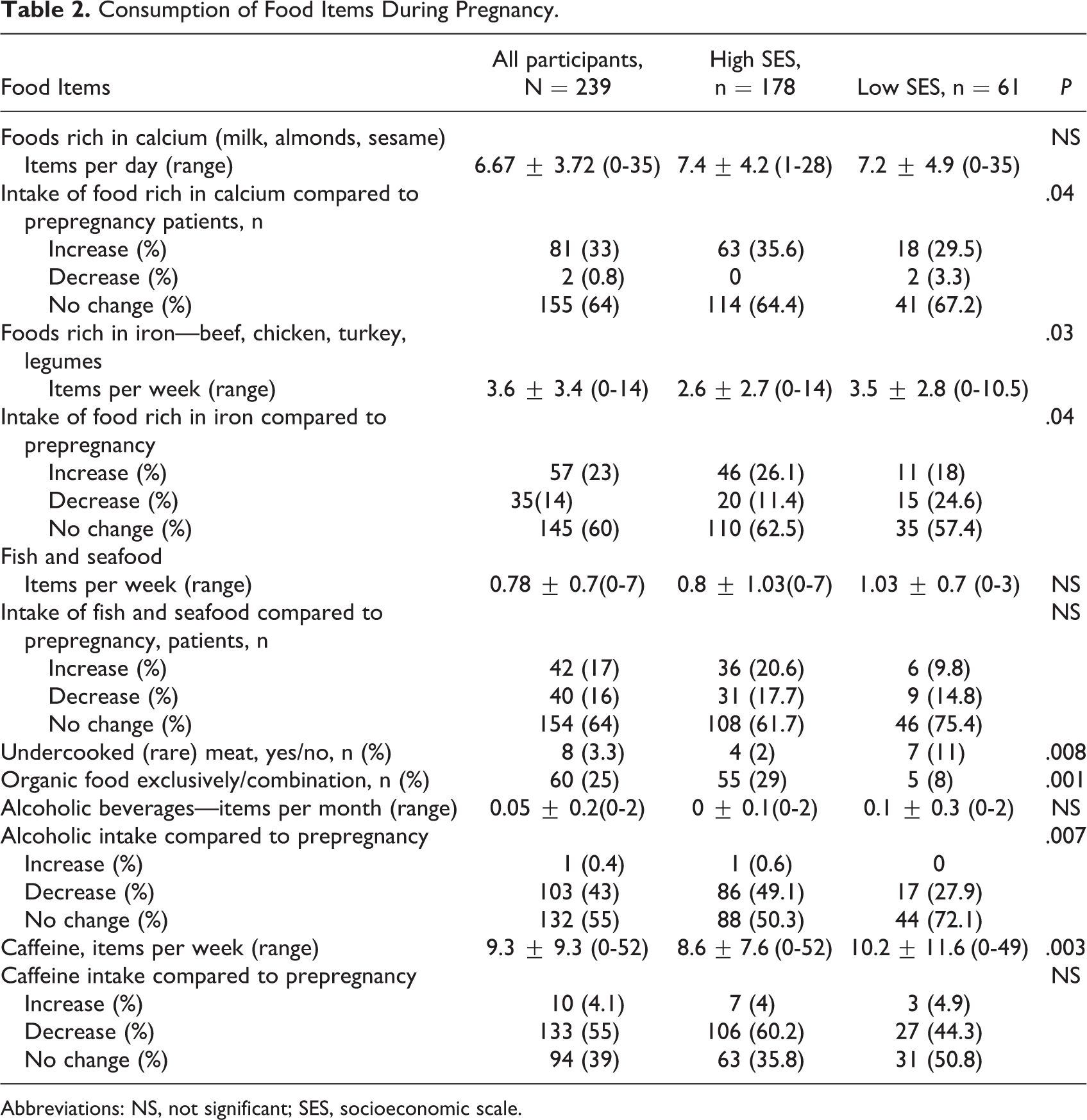
Abbreviations: NS, not significant; SES, socioeconomic scale.
Usage of Supplements Before and During Pregnancy: Awareness of Guidelines and Application
Figure 1B displays the different information sources about dietary supplements during pregnancy. Ninety-four percent reported of being aware of nutritional supplements guidelines before and during pregnancy (n = 222): 89% received the information from their gynecologist (n = 210) and the other 6% 12 from nonprofessional sources (friends, the Internet, etc), with no significant difference between the different SESs.
Table 3 depicts dietary supplements consumption during pregnancy in all participants and difference between SESs. Eighty-five percent of the participants reported to have taken or to be taking folic acid supplements in association with pregnancy (n = 202). There were significant differences between SESs in both the absolute number of women who took folic acid supplements and those who took the supplements in accordance with the guidelines 1 month before pregnancy (155 [88%] vs 47 [77%] P = .05 and 74 [41.6%] vs 13 [21.3], P = .005). Seventy-five percent (n = 181) of the participants reported having taken iron supplements before or during pregnancy, and 96% reported that their hemoglobin levels were monitored during pregnancy (n = 226). There was no significant correlation between SES and adherence to iron supplementation guidelines during pregnancy.
Dietary Supplements Consumption During Pregnancy in All Participants and Difference Between SESs.
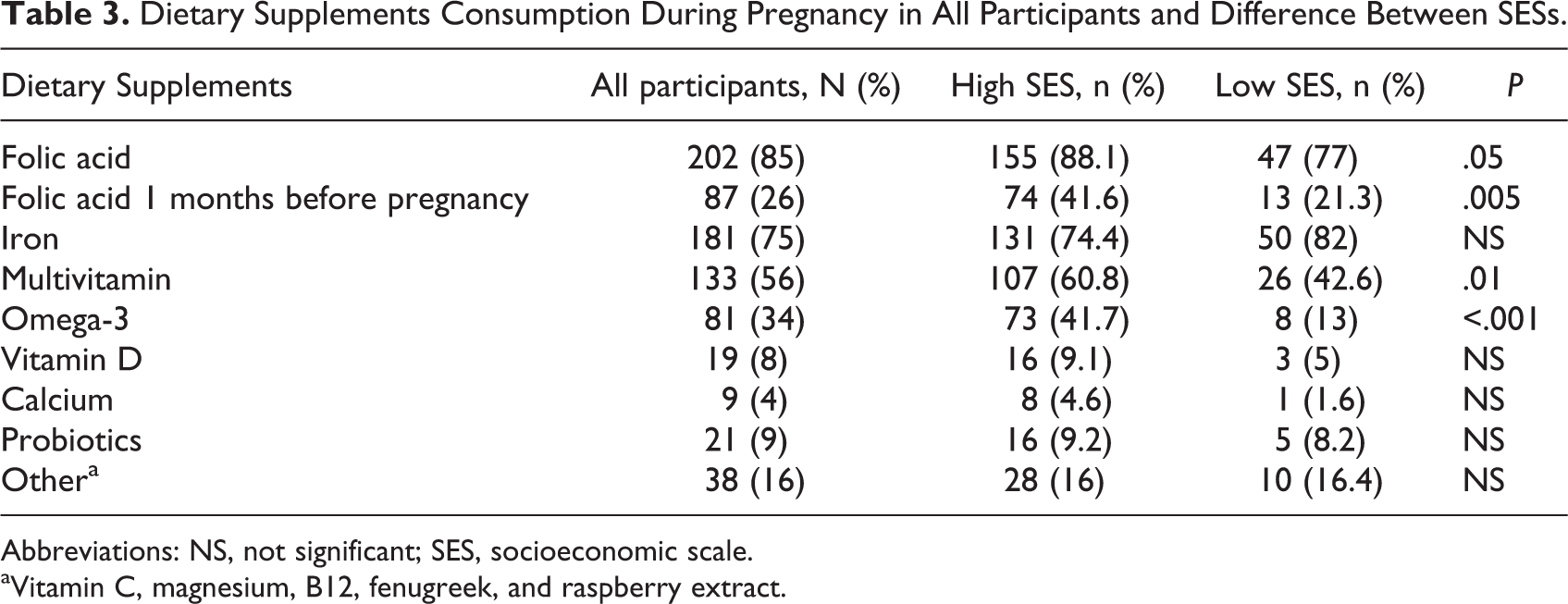
Abbreviations: NS, not significant; SES, socioeconomic scale.
aVitamin C, magnesium, B12, fenugreek, and raspberry extract.
Fifty-six percent of the participants (n = 133) took multivitamin supplements during pregnancy, with the consumption being higher in higher SESs (60.8% vs 42.6% for lower SESs, P = .01). Thirty-four percent of the participants (n = 81) consumed omega-3 supplements during pregnancy, with a higher intake recorded in higher SESs compared to lower SESs (41.7% vs 13%, respectively, P < .001).
Discussion
In the present study, we observed several gaps in the awareness and implementation of professional nutritional guidelines during pregnancy and breastfeeding that were related to the SES of the mothers. Only one-half of the study women were aware of the MOH dietary guidelines, regardless of their social status. One-third of them reported that they were instructed on recommended food practices by a professional; for example, a gynecologist, a clinical dietician, or a specialist pregnancy nurse. It is important to note that national health insurance in Israel is mandatory, and so women of high and low SESs equally receive access to gynecologists or family doctor’s consultation, nursery stations, and discounted medications. Better training at the community level and strict surveillance by doctors and paramedical personnel would increase the level of application. When we examined the level of application of nutritional guidelines throughout pregnancy, we found a high level of application of the “warning” guidelines calling for avoidance or reduction in the consumption of alcoholic or caffeinated beverages and undercooked (rare) meat or raw fish (97%, 61%, and 95%, respectively). The level of application of guidelines for the adherence to certain foods, however, was lower. Thus, for example, only 34% and 24% of pregnant women increased the consumption of products enriched in calcium and iron, respectively, during pregnancy, although there was a higher level of adherence among women from higher SESs. Interestingly, there was an opposite trend for iron consumption: Women from higher SESs consumed fewer foods rich in iron, possibly due to the higher prevalence of vegetarianism among them.
Previous studies also indicated a link between SES and adherence to official dietary recommendations, healthy food intake, and the purchase of healthy foods in the Western world. 17,18 Hulshof et al examined dietary intake in adult Dutch populations with different SESs and found that dietary intake among patients in higher SESs tended to be closer to the recommendations of the Food and Nutrition Council and that this behavior was quite stable over a period of 10 years. 18 Vlismas et al reviewed dietary habits and health-related outcomes between adults from different SESs in various parts of the world and found that in most studies lower SES was related to unhealthy behaviors. 17 A multicenter, birth cohort study in 9 European countries that investigated maternal dietary habits during pregnancy and compared them to the national pregnancy recommendations found that maternal dietary habits and the use of dietary supplements during pregnancy vary significantly across Europe and that they were influenced by national recommendations. It is not known if these differences were attributed, at least in part, to differences in socioeconomic and demographic parameters. 19 The present study shows that SES itself has an effect on dietary choice during pregnancy and therefore raise the need to consider public policy intervention to regulate how pregnant women are guided about nutritional recommendations during pregnancy, especially with regard to guidelines for ensuring sufficient quantity of certain foods.
Supplements that are officially recommended during pregnancy, that is, folic acid and iron, were frequently used by our study participants (85% and 76%, respectively). There is a significant increase in the level of application of folic acid supplementation compared to data from 2002, which showed a 30.5% adherence rate among pregnant women. 20 The data from the Ministry of Health Nutrition and Health Survey (MABAT LARACH 2009-2012) and a 2017 study by Yagur et al conducted at Hillel Yaffe Hosipital in Hadera found similar higher adherence rates, with folic acid having been consumed by 86% and 71% of the studied women, respectively, reflecting an increase in awareness over the last decade. 21,22 We found that women with a low SES had lower adherence to the guideline for folic acid supplementation compared to women in a high SES as had also been observed by Oliver et al. 19
We also examined the intake of dietary supplements that are not included in the official MOH recommendations. One-half of the participants took a multivitamin (containing calcium and vitamin D) supplement, and one-third of the women took omega 3 supplements, with significant differences between low and high SESs. There is ample evidence of health benefits for the pregnant woman and the newborn in women who took dietary supplements, such as calcium, vitamin D, and omega-3, during pregnancy. Calcium intake was found to reduce the risk of hypertension and preeclampsia during pregnancy. 23 The effect of vitamin D has been investigated in various studies and remains controversial. However, it appears to be associated with a reduction in the risk of low neonatal birth weight (<2500 g) and was shown to have a beneficial effect on the maternal and fetal immune systems. 24 In a recent study by Savard et al, vitamin D was found to be one of the nutrients for which diet alone was insufficient to provide adequate intake during pregnancy, 25 and some European countries officially recommend vitamin D supplementation during pregnancy. 20 The importance of omega-3 fatty acids and, especially, docosahexaenoic acid during pregnancy and lactation, has been demonstrated in several studies. Their consumption was associated with improved cognitive development of the newborn and reduced risk of prematurity. 26 The findings of the present study raise the need to establish a clear policy on whether these supplements are essential for the pregnant woman, similar to the existing recommendations for folic acid and iron supplements and the more recent recommendation for iodine supplementation for the pregnant and lactating mothers. If these supplements are officially recommended, it will be necessary to ensure that these supplements are available to all population groups equally as opposed to the present situation as implicit in the results of this study.
The strength of this study is its relatively large sample. Although it was conducted in a single area of the country, we sampled 6 different areas of the city that was comprised of heterogeneous population with different SESs and ethnic groups and included several indicators of SES (education and income as reflected by residence index and geographical area). The limitations of the present study are the use of the survey questionnaire as a single measurement tool and the reliance on the participants’ memory of events that began 9 to 15 months prior to the interview. These limitations may impair the accuracy and reliability of the data. At the same time, these limitations do not appear to have created differential information bias among the various research groups (low, intermediate, and high SES).
In conclusion, this study presents important information regarding dietary habits and the use of nutritional supplements among pregnant and lactating women from different socioeconomic backgrounds. The results point to certain deficiencies in the awareness and implementation of existing recommendations as well as to gaps between women from different socioeconomic backgrounds. These findings can have significant health implications for pregnant women and their newborns. Further studies and public health programs aimed at ensuring optimal nutrition for women during pregnancy and lactation are warranted.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.