
Abstract
Background:
Nutritional deficiencies are common during pregnancy and a year after childbirth. At the same time, maternal depression affects many women during pregnancy up to 1 year after childbirth. The objectives of this study were to determine the associations between nutrition status, dietary intake, and maternal depression among pregnant women.
Methods:
This was a cross-sectional study that included 262 pregnant women aged 15 to 49 years attending the antenatal clinic in 2 public health facilities in urban low-income settlements in Nairobi, Kenya. Maternal depression was assessed using Edinburgh Postnatal Depression Scale (EPDS). Mid-upper arm circumference (MUAC) was used to determine nutritional status. Dietary intake was assessed using the 24-hour recall, and brain essential nutrients were assessed through a questionnaire. Odds ratio was used to test the associations. All maternal characteristics with P < .001 in the univariable analysis were considered in the multivariable logistic regression, variables with P < .05 were considered significant.
Results:
Of the 262 pregnant women, 33.6% (95% CI: 27.9-40.7) had depressive illness as indicated by EPDS >13. About 9.9% of pregnant women had MUAC < 23 cm. The study established statistically significant association between poor nutrition by MUAC and maternal depression (P < .001). Maternal depression was statistically significantly associated with inadequate intake of brain food essential (P = .002). Maternal depression was statistically significantly associated with lower income (P < .001). In multivariable regression analysis, the main predictor of maternal depression was poor nutrition (P < .004).
Conclusion:
These findings reveal an association between poor nutrition and maternal depression. These results suggest that nutritional deficiencies could be a contributing factor for maternal depression. Study recommends dietary interventions as cost-effective way to reduce deficiencies and improve mental health problems for pregnant women. Assessment of maternal depression and dietary intake be integrated as fundamental components of antenatal care.
Background
Adequate nutrition for women during pregnancy prevents nutritional deficiencies that affect women’s physical and mental health. 1,2 The health of pregnant women, whether good or poor, affects not only the mother’s quality of life but also fetal life and long-term health problems. 3 Maternal depression, defined as a mood disorder, is common during pregnancy and up to 1 year postpartum. 4 -6 The World Health Organization estimates that maternal depression among pregnant women in developing countries ranges from 15% to 57%. 7,8 At the same time, pregnancy malnutrition in Africa is still high, with an overall pooled prevalence of 23.5% with variation between countries. 9 -12 Research demonstrates high rates of mental health problems in pregnant women and mothers among the poorer sections of developing countries 13 ; besides, mental illnesses are generally more prevalent in urban than in rural areas. 8 Various prevalence rates of maternal depressions have been reported across countries; for example, the prevalence rate of 20.2% in Pakistan, 29% in Brazil, 39% in Bangladesh, 39.5% in Tanzania, 14 and 35.7% in Ethiopia. 15 In Kenya, estimated prevalence rates are 38.4% and 13% among pregnant 16 and postpartum women, 17 respectively.
In Sub-Saharan Africa, many women have chronic energy deficiencies during pregnancy due to insufficient food intake, high energy expenditure, and demands of pregnancy contributing to maternal malnutrition. 12 Nutritional deficiencies of essential vitamins and minerals have been linked to maternal depression. 18 In Kenya, nutrition situation analysis conducted among pregnant women revealed that iron deficiency, also known as anemia, was 55.1%, iodine deficiency disorders was 36.8%, and zinc deficiency among mothers was 52%. 19 It is documented that, around the world, about 800 women die from pregnancy or childbirth-related complications every day. 12,20
Epidemiological studies indicate that quality of diet has implications for malnutrition and depression. 10,21,22 Poor diet during pregnancy exposes women to increased risk of maternal depression. 3 Brain food essentials (BFEs) are important nutrients for brain function and regulation of the neurotransmitters such as serotonin, dopamine, and norepinephrine in mood stabilization. 3,23,24 Deficiencies of BFEs, mainly of ω-3 fatty acids, folate, and B12, iron, zinc, magnesium, vitamin C, and vitamin A, have been linked to increased incidences of depression. 18,24,25 One study that investigated the role of nutrition for depression reported that anemic women have significantly higher depressive symptoms compared to nonanemic women. 10 In South Africa, a study evaluated the relationship between food insufficiency and mental disorders; the results revealed that food insufficiency is associated with mood disorders. 26 A systematic review and meta-analysis study by Lai et al 27 disclosed that a healthy diet pattern was highly associated with reduced odds of depression where high intakes of fruit, vegetables, fish, and whole grains were related to reduced depression risk. Nutritional deficiencies adversely affect both maternal well-being and birth outcomes. 12 Conclusive evidence on nutritional enhancement as a treatment strategy for depression is still lacking. 13,21,22 Given this backdrop, the overall objective of this article is to identify nutritional factors associated with maternal depression among pregnant women in 2 urban low-income settlements in Nairobi, Kenya, where assessment for maternal depression, dietary intake, BFE intake, and nutritional status were the study’s specific objectives.
Methods
This cross-sectional study assessed nutritional status, dietary intake, BFE intake, and maternal depression among pregnant women who attended antenatal care clinics in 2 urban low-income settlements in Nairobi, Kenya. Ethical approval was obtained from The Kenyatta National Hospital/University of Nairobi Ethical and Research Committee (KNH/UoN-ERC Ref: P56/02/2018). The study took place in 2 public health facilities in 2 urban low-income settlements: Kangemi and Kawangware. The 2 sites are both growing informal settlements located on the outskirts of the Nairobi city center. These sites were chosen purposively because the antenatal clinics (ANC) at these health facilities receive a high volume of pregnant women. Pregnant women of aged 15 to 49 years who visited ANCs for antenatal checkup during the study period February to March 2019 composed the study population. This cross-sectional study was part of the baseline assessment of a longitudinal cohort study that targeted depressed pregnant women for intervention. The intervention was a nutritional enhanced mental health intervention for depression care among pregnant women. The sample size was calculated using sample size estimation for longitudinal designs with attrition. We needed approximately 100 pregnant women with depressive symptoms. The target was 50 pregnant women from each site of which 1 would be the intervention group and another comparison group. Therefore, in total, 262 pregnant women were screened at baseline to obtained 100 depressed pregnant women. Recruitment took place at the ANC at the 2 selected health facilities, 1 site at a time. All pregnant women who came for antenatal services and were in the waiting room were approached to participate. The study purpose was explained to them, highlighting that the participation was voluntary, and their refusal to participate would not involve any penalty of benefits to which one was entitled at the clinic. The participants were assured about their privacy and confidentiality. After obtaining a written informed consent signed by the respondent based on willingness to participate, the baseline interview commenced. Consecutive sampling was used to obtain the sample size, where every pregnant woman with consent was screened for depression. These interviews were conducted conveniently around the clinic, as agreed by the participants, and lasted for 40 to 60 minutes. The study analyzed the data of 262 pregnant women who completed the baseline data.
Data Collection
Sociodemographic Characteristics
Using a questionnaire, pregnant women provided data on sociodemographic characteristics, age, marital status, maternal education level, employment status, partner’s occupation, monetary decision-making, and family monthly income.
Maternal Depression
Edinburgh Postnatal Depression Scale (EPDS) was used to assess maternal depression. Edinburgh Postnatal Depression Scale is a 10-item questionnaire in which women report how they have been feeling in the past 7 days. 28 Edinburgh Postnatal Depression Scale has a Kiswahili translation version and has been validated for detecting depression in both prepartum and postpartum mothers in many countries, including Kenya. 29 Edinburgh Postnatal Depression Scale is one of the most well-known and evaluated instruments for maternal depression and has demonstrated acceptable clinical utility as a screening tool. It has a sensitivity of 86%, specificity of 78%, and a positive predictive value of 73%. 30 The depression scores were categorized into 2 levels: EPDS score of <13 indicated nonexistence of depression and EPDS score above 13 indicated existence of depression. 28
Anthropometric Assessments
Nutritional status of pregnant women was determined using mid-upper arm circumference (MUAC). Mid-upper arm circumference is a nonstretch measuring tape applied on the left arm and recorded to the nearest 0.1 cm. The measurements were taken with no clothing on the arm and recorded in duplicate for each respondent to enhance accuracy. Respondents with MUAC < 23 cm were classified as undernourished, and respondents with MUAC ≥ 23 cm were classified as normal/nourished. 31 Hemoglobin (Hb) levels of pregnant women were obtained from pregnant women clinic card records. Pregnant women with Hb levels of 11 g/100 mL and above were classified as normal Hb. Pregnant women with Hb levels < 11 g/100 mL were classified as anemic. 32
Dietary Assessment
Dietary intakes were assessed using a 24-hour dietary recall method to determine food, energy, and nutrient intake. 33 Food consumed by women was entered in the NutriSurvey software. The NutriSurvey program is German software (EBISpro). It contains an extensive collection of food databases worldwide that can be easily integrated into the software. The food consumed was entered into the software, and the software generates an analysis of nutrients consumed from the food record. The analysis was done on the category of pregnant women. The software generated the consumed amount by pregnant women (analyzed value) and recommended value per day and generated percentage fulfillment of the daily recommended allowance for pregnant women. Women with a score of < 70% (percentage fulfillment) were classified as having inadequate intake, and women with a score of ≥ 70% were classified as having adequate intake. 34
Moreover, the BFE intake was assessed using a questionnaire checklist. Brain food essential nutrients are foods good for brain function and help balance the neurotransmitters. The food targeted as brain essentials was healthy food available in Kenya’s local environment, such as high-protein foods and ω-3 fatty acids, which are brain-building blocks, ω-3 food includes (fish, groundnuts, pumpkin seeds, Sunflower seeds, lean meats, organ meats, margarine, and eggs); B vitamins (whole grains, legumes, meat, eggs, fish, green leafy vegetables); minerals such as zinc food (pumpkin seeds); iron (kidney beans, lentils, organ meat); magnesium (black beans, avocado, pumpkin seeds); and antioxidant vitamins. 35 The BFEs questionnaire has 13 food items. Pregnant women who consumed BFEs with a total correct response score of ≥ 70%, which is about 9 of 13 food groups, indicated adequate intake of BFE. Consumption with a score < 70 indicated inadequate intake. 36
Statistical Analysis
The filled questionnaires were checked for completeness, followed by data entry and cleaning. The data were analyzed using SPSS for windows version 22. A descriptive analysis of variables, sociodemographic characteristics, anthropometric data, and hematological characteristics was undertaken. Descriptive statistics such as percentage means and standard deviation (SD) were used to summarize the sociodemographic data. Pregnant women with EPDS score > 13 were identified as with maternal depression, and pregnant women with EPDS score < 13 were identified as without maternal depression. The independent variables were categorized to analyze the association between independent and outcome variables; univariable analysis of odds ratio (OR) with 95% CI was calculated. The 24-hour dietary recall data were analyzed using NutriSurvey software (EBISpro), which contains various national and international food tables. All maternal characteristics at a P < .001 in the univariable analysis were considered multivariable logistic regression. The variables that were associated at a P < .05 were considered to be significant.
Results
Sociodemographic Characteristics Among Pregnant Women in Urban Low-Income Nairobi, Kenya
The mean (SD) age of the 262 women was 25.3 ± 5.0, with 18 to 44 age range. The majority of the study women (82%) were married, with 29.8% having less than high school education and 14% had tertiary level education. About 79.4% of the women had no employment but depended on their partners or parents; only 20.6% were employed. Slightly less than half of the women (43%) were first-time mothers. About 70% of the pregnant women were in the second trimester. Almost all the women (98%) owned a basic personal phone and slightly less than three-quarters owned a television (73%). The mean (SD) income level was 10 845.8 Kenyan shillings (KES) per month, and almost half of the women (49.6%) lived on an income < 15 000 KES, equivalent of 150 USD per month. About (38.9%) of women had their husbands make decisions on household finances.
Maternal Depression Among Pregnant Women in Urban Low-Income Nairobi, Kenya
Guided by EPDS scoring system, the 10-item question generated a depression score that ranges from 0 to 30 maximum. A score > 13 EPDS indicated the presence of clinical depression.
Of the 262 pregnant women, about a third, 33.6% (95% CI: 27.9-40.7) were found to have clinical depression as indicated by EPDS > 13. The mean (SD) EPDS score was 11.1, interquartile range of 10 with a minimum score of 0, and a maximum score of 26. The sociodemographic characteristics were compared between depressed women and nondepressed women, and the results revealed that pregnant women’s gestation age (second trimester) was statistically significantly associated with maternal depression (OR: 3.37; 95% CI: 1.60-7.10; P < .001). The lower-income level < 10 000 KES was also statistically significantly associated with maternal depression (OR 0.39; 95% CI: 0.23-0.66; P < .001; see Table 1).
Distribution of the Women by Sociodemographic Characteristics According to Maternal Depression Status EPDS Score of >13.a
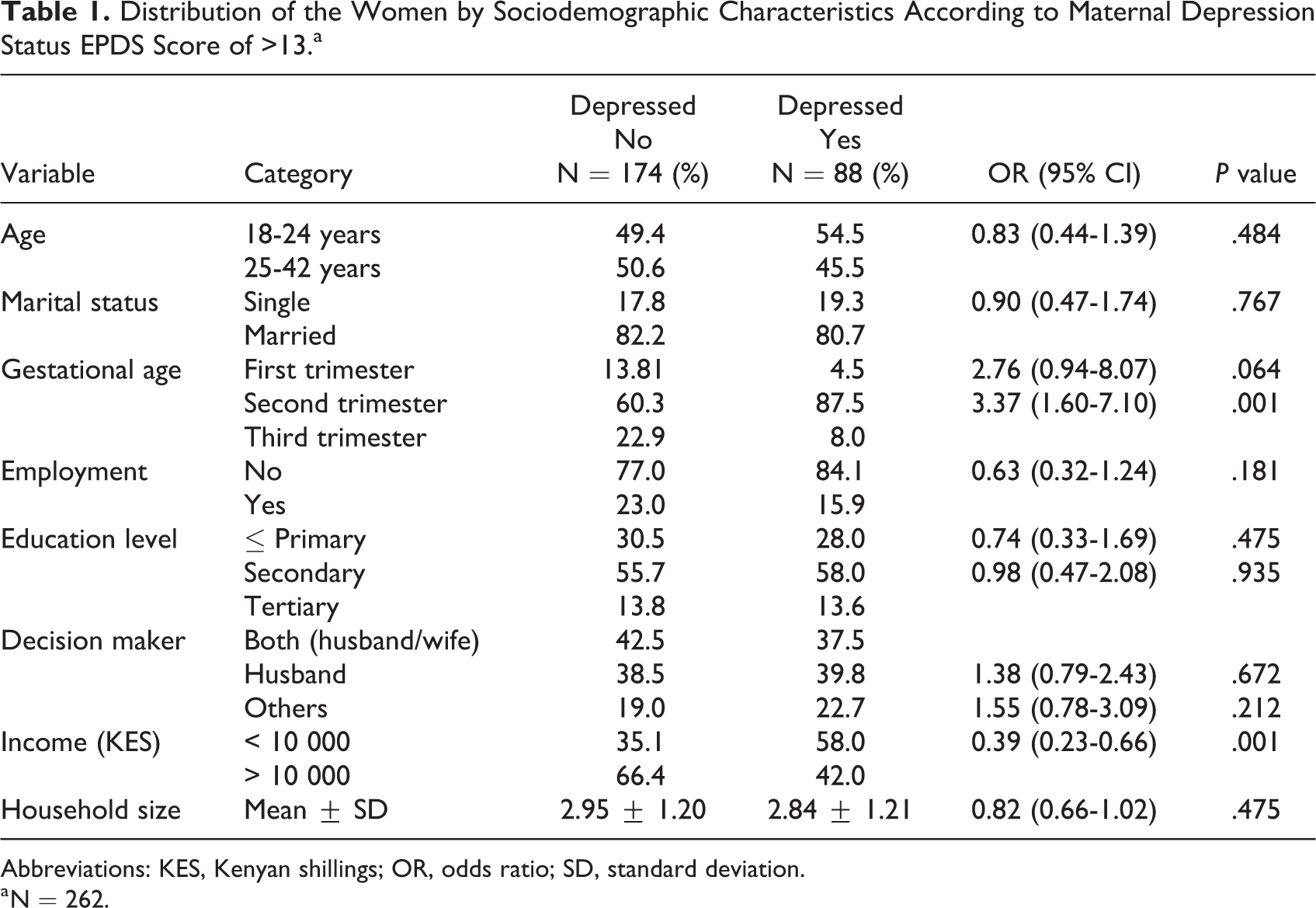
Abbreviations: KES, Kenyan shillings; OR, odds ratio; SD, standard deviation.
a N = 262.
Nutritional Status of Pregnant Women in Urban Low-Income Nairobi, Kenya
Maternal nutrition status was assessed using MUAC. The results revealed that, of 262 pregnant women, 9.9% (95% CI: 5.3-5.6) had MUAC < 23. The Hb levels were obtained from the clinic card records, and the results revealed that about 31.7% (95% CI: 25.2-40.3) of pregnant women were anemic as indicated by HB < 11 g/100 mL. Of the percentage of the anemic pregnant women, 29.5% were depressed pregnant women (see Figure 1).
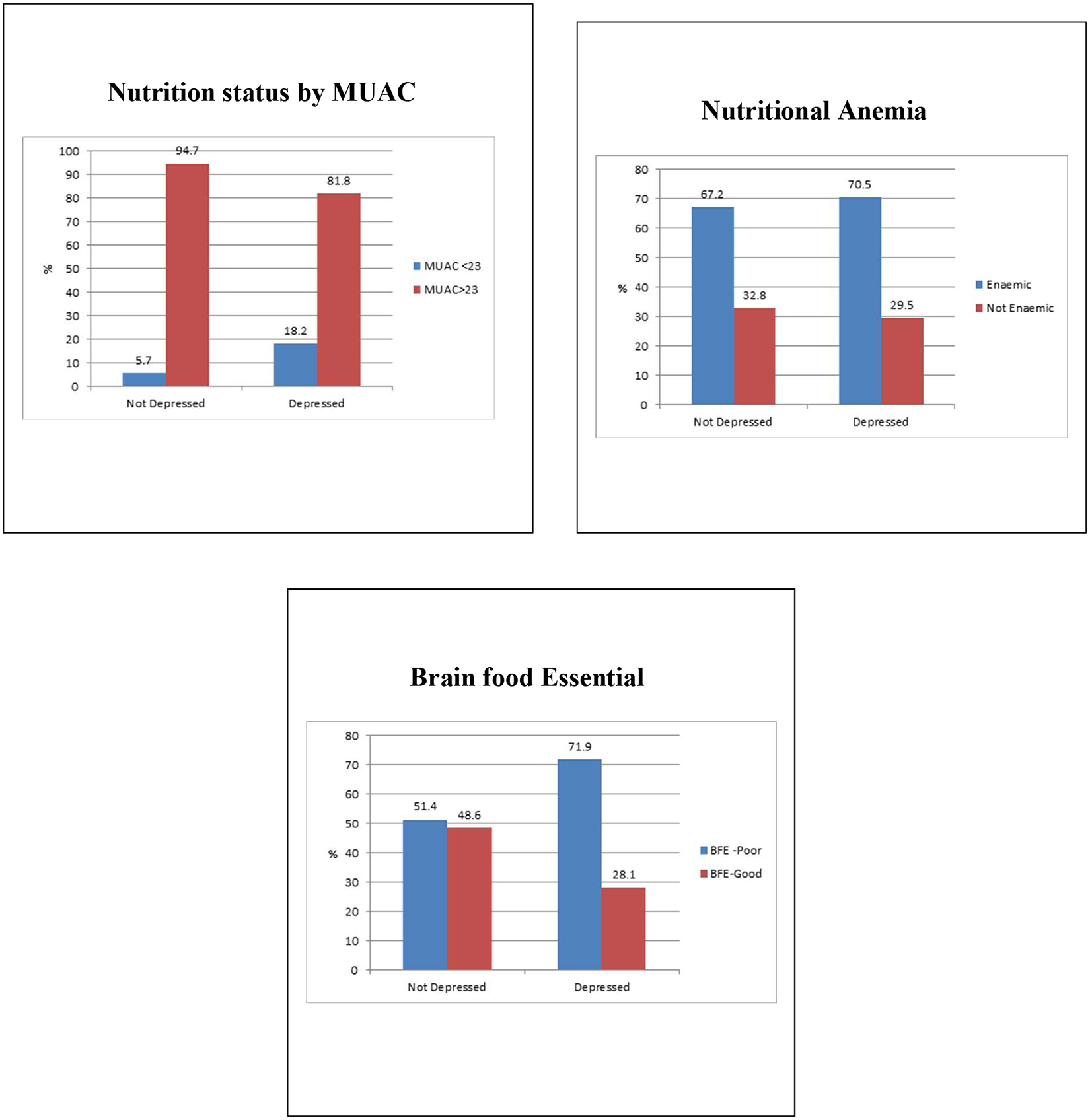
Above, Nutritional status of pregnant women according to maternal depression status with EPDS score of >13. Below, Brain food essential intake between depressed and nondepressed pregnant women in urban low-income Nairobi, Kenya. EPDS indicates Edinburgh Postnatal Depression Scale.
Dietary Intake of Pregnant Women in Urban Low-Income Nairobi, Kenya
Dietary intake was assessed using one time 24-hour recall in this cross-sectional study. The NutriSurvey software category of pregnant women was used for analysis. The food consumed was entered into the software. The software generated an analysis of the food consumed, and genetared the results which include the nutrient contents, the analyzed value, the recommended values of pregnant women per day, and percentage fulfillment for the consumed food by pregnant women. Results reveal that most pregnant women did not fulfill their recommended daily requirements of food intake for pregnancy as indicated by percentage fulfillment of < 70%, regardless of their status, whether with depression or without depression. When percentage fulfillment was compared between depressed women and nondepressed women, results revealed a statistically significant association between energy fulfillment and maternal depression; there was a statistically significant association between phosphorous and maternal depression (see Table 2)
Achieved Percentage of Recommended Dietary Intake Between Depressed and Nondepressed Pregnant Women in Urban Low-Income Nairobi, Kenya.a
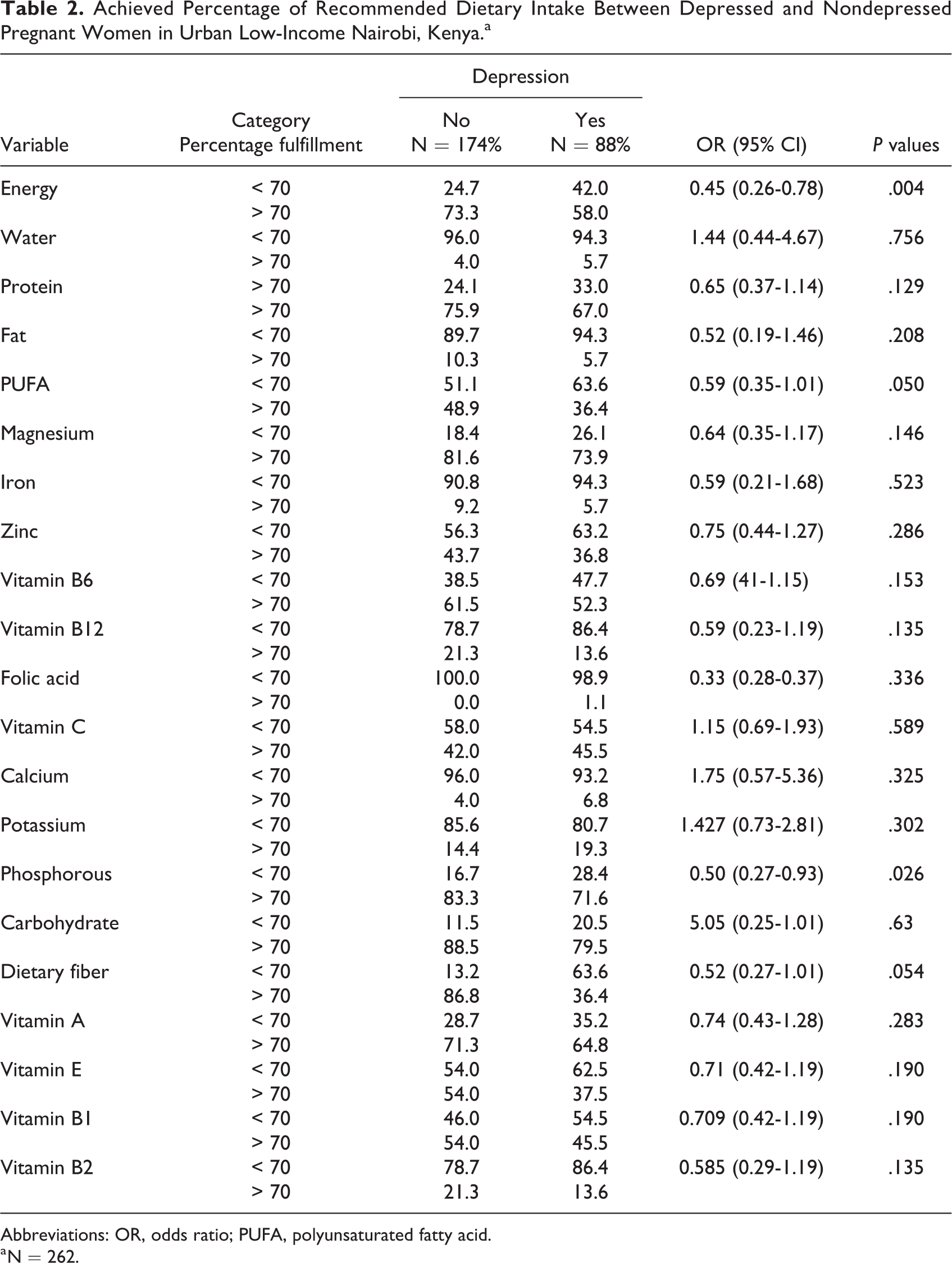
Abbreviations: OR, odds ratio; PUFA, polyunsaturated fatty acid.
a N = 262.
Brain Food Essential Intake Among Pregnant Women in Urban Low-Income Nairobi, Kenya
Brain food essentials were assessed to determine whether women were taking enough BFEs. Women were asked if they consumed brain food items in the past 3 days. Results revealed that about 26.7% of pregnant women had inadequate intake of BFEs, as indicated by a score of < 70%. Of the pregnant women with an inadequate intake of BFE, 71.9% were depressed pregnant women (see Figure 1).
Association Between Maternal Nutrition Status, Dietary Intake, Brain Food Intake, and Maternal Depression Among Pregnant Women in Urban Low-Income Nairobi, Kenya
Nutritional status was compared between pregnant women with depression and pregnant women without depression. The results revealed that there was a statistically significant association between poor nutrition status as assessed by MUAC with maternal depression (OR 0.27; 95% CI: 0.11-0.63; P < .001). Maternal depression was statistically associated with poor intake of BFEs, with OR: 0.41; 95% CI: 0.26-0.74; P = .002. Poor nutrition status by MUAC was statistically associated with poor intake of BFEs (OR: 2.631; 95% CI: 1.15-6.00; P = .018). Maternal depression was statistically significantly associated with lower-income levels (OR: 0.39; 95% CI: 0.23-0.66; P < .001). Moreover, BFEs were also statistically associated with low-income levels (OR: 1.74; 95% CI: 1.00-3.03; P < .046; see Table 3).
Association Between Nutrition Status, Dietary Intake, and Maternal Depression Among Pregnant Women in Urban Low-Income Nairobi, Kenya.a
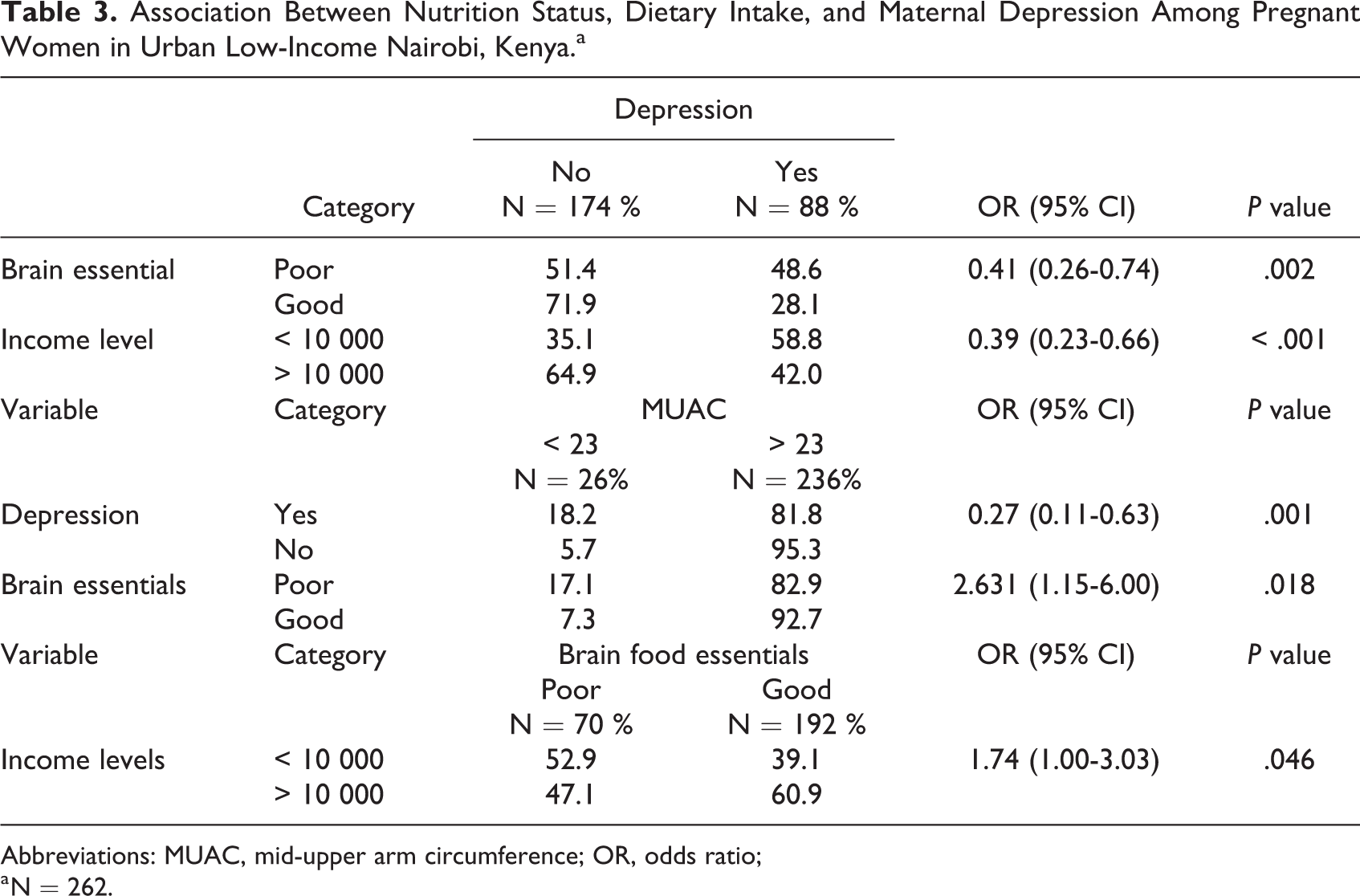
Abbreviations: MUAC, mid-upper arm circumference; OR, odds ratio;
a N = 262.
Main Predictors for Maternal Depression
In the multivariable logistic regression analysis, poor nutritional status by MUAC was statistically significantly associated with maternal depression (P = .004) and the main predictor for depression (see Table 4).
Main Predictors of Maternal Depression Among Pregnant Women in Urban Low-Income Nairobi, Kenya.a
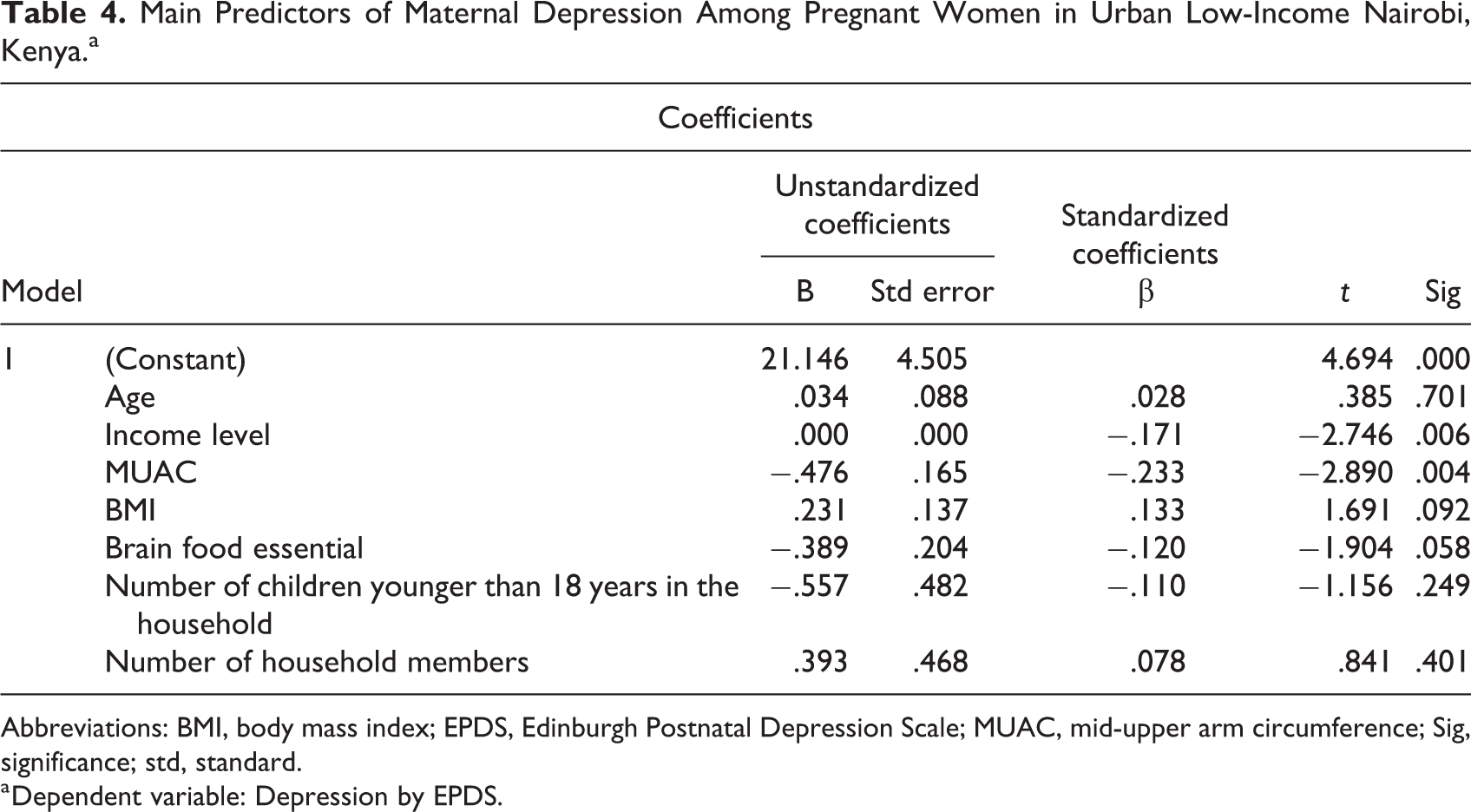
Abbreviations: BMI, body mass index; EPDS, Edinburgh Postnatal Depression Scale; MUAC, mid-upper arm circumference; Sig, significance; std, standard.
a Dependent variable: Depression by EPDS.
Discussion
Maternal Depression Prevalence Among Pregnant Women in Urban Low-Income Nairobi, Kenya
A third (33.6%) of study women had maternal depression assessed by EPDS associated with low income and gestational age, specifically in the second trimester. This prevalence rate is comparable with the available estimates for maternal depression in developing countries with a range between 15% and 57%. 7 The prevalence rates of maternal depression varies across countries in which risk factors differ from one study to another. 14,15,16 These variations could be due to methodological differences in which the studies were conducted, types of population in terms of culture, and socioeconomic status. A study by De Oliveira et al 37 in South Florida found a prevalence rate of 37.5% among Hispanic pregnant women in South Florida; education level, health status, and living with a partner were significant predictors of maternal depression. Different from our study, these factors were not significantly associated with maternal depression.
Nutritional Status Among Pregnant Women in Urban Low-Income Nairobi, Kenya
The study results revealed that poor nutrition status was statistically significantly associated with maternal depression. Our study findings are not so different from other studies that documented poor nutritional status among pregnant women. Looking at the survey by Sheeba et al, 15 in Ethiopia, determined the magnitude of malnutrition and associated factors among pregnant women and revealed that 30.3% of pregnant women were underweight, the risk factor for undernutrition was maternal age of women that was statistically significantly associated with poor nutritional status. These results demonstrate a need to disseminate appropriate nutritional education to young mothers with a low educational background because they may be disadvantaged. A study by Barker et al 38 in England tested whether prenatal maternal depression symptoms predicted poor prenatal nutrition; results revealed that higher depressive symptoms during pregnancy were related to higher levels of unhealthy nutrition. A cohort study of pregnant women by Chatzi et al 39 in Greece investigated dietary patterns and depression during pregnancy. The results revealed that high adherence to a health-conscious diet, high in vegetables, fruit, pulses, nuts, dairy products, fish, and olive oil was associated with lower EPDS scores, β-coefficient = −1.75, P = .02. These results demonstrate that poor diet quality during pregnancy is the cause of poor nutritional status which also exposes women to maternal depression.
Dietary Intake of Pregnant Women in Urban Low-Income Nairobi, Kenya
The study findings revealed inadequate dietary intake of food among pregnant women. Most pregnant women did not meet their daily nutritional requirements for various nutrients. These findings are similar to other research findings. A study by Taleb et al 40 in South Africa, KwaZulu Natal, determined the nutritional status and food intake of pregnant women. The results indicated that except for carbohydrates and vitamin A, all the nutrients consumed by the women were lower than the recommended daily amounts; the fruits and vegetable intake was half of the recommended daily amount. Another study in Nigeria by Lindsay et al 41 revealed a high prevalence of nutrient deficiencies, including iron, folate, vitamin D, and vitamin; these nutrient deficits above are crucial brain essentials. The study by Almurshed et al, 42 in Saudi Arabia, found that the nutrient intake for pregnant women was below the recommended dietary allowances: 51.8% for energy; 93.9% for vitamin B1; 82.5% for calcium, and 98.2% for iron. These results reveal inadequate intake of nutrients among pregnant women. Some of those nutrients are essentials for brain health in which the deficiencies may lead to mood disorders among pregnant women.
Brain Food Essentials Intake Among Pregnant Women in Urban Low-Income Nairobi, Kenya
The study results revealed that pregnant women in urban low-income settings had inadequate intake of BFEs. Our results compare well with other studies conducted on a similar topic. A study by Singh et al 43 in Columbia evaluated the prevalence of nutritional deficits in pregnant teenagers and assessed the associations among micronutrient dietary intake, stress, and depression. Results revealed that more than 50% of pregnant teenagers had an inadequate folate intake, vitamin A, vitamin E, iron, zinc, calcium, magnesium, and phosphorous (excluding dietary supplements). Additionally, in the same study, > 20% of participants had an inadequate intake of thiamin, riboflavin, niacin, vitamin B6, vitamin B12, vitamin C, copper, and selenium elements which are the BFEs. 18,24,44
A limitation of this study is the cross-sectional design, which may prevent conclusive inferences about the relationship between inadequate diet and maternal depression. Longitudinal studies need to be conducted to confirm the association. Despite these challenges, we think that the article underscores the critical role of nutrition in addressing maternal mental and physical health, which needs to be enhanced in intervention development in low- and middle-income countries.
Conclusion
The study findings lead to the conclusion that there is an association between nutrition and maternal depression. Nutritional deficiencies may expose women to the risk of maternal depression. Antenatal clinic visits may provide a window of opportunity to promote good nutrition for mental health, and nutrition could be the best and cost-effective way to reduce deficiencies and improve mental health problems for mother and child. The study recommends the assessments of maternal depression and dietary assessments during prenatal clinic visits to be integrated as a fundamental components of care at primary health facilities. Development of food-based interventions and user-friendly tools for assessing maternal depression in the Kenyan context is required.
Footnotes
Authors’ Note
B.A.M. had a primary role and was involved in study design, data collection, data review, data extraction, and manuscript writing. W.K.M. helped conceptualize the study design, correct, and edit the manuscript. S.N. was involved in editing and reviewing the manuscript. M.K. was involved in editing and reviewing the manuscript for submission. All authors read and approved the final manuscript. All data generated and analyzed during this study are included in this published article. Informed consent was obtained from participants in this research for future uses of data, such as publication, preservation, and long-term use of research data. Confidentiality was assured. The information collected was kept confidential. Serial numbers were used instead of name. Ethical approval was obtained from The Kenyatta National Hospital/University of Nairobi Ethical and Research Committee (KNH/UoN-ERC) Ref. P56/02/2018. The study purposes were explained to the participants. The respondent signed informed consent based on willingness to participate in the study; verbal consent was witnessed and formally recorded.
Acknowledgments
The authors would like to thank our study participants, numerous Antenatalal Clinic nurses at Kangemi and Kawangware Health Centres, Community health workers, and personnel who supported data collections.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.