
Abstract
Background
Diet quality indexes (DQIs) consist of combinations of foods and/or nutrient components that represent adherence to dietary guidelines. A high-quality diet during pregnancy contributes to optimal birth outcomes.
Objective
We developed and validated the first DQI for pregnancy for South African women.
Methods
The South African Food Based Dietary Guidelines and pregnancy dietary guidelines were used as theoretical basis for the a priori development of the South African Diet Quality Index for Pregnancy (SA-DQI-P). To validate the SA-DQI-P, we applied it to data collected for the Nutritional status of Expectant Mothers and their newborn Infants (NuEMI) study (N = 682). We determined the associations between SA-DQI-P scores in tertiles with nutrient intakes, sociodemographic factors, household food security level, and biochemical values.
Results
A lower household density ratio, household access to a toilet, refrigerator, and microwave, a higher educational level, being employed and being food secure were significantly associated with a higher score. After correcting for energy intake, higher scores were significantly associated with higher intakes of protein, total fat, saturated fat, cholesterol, calcium, vitamin A, vitamin E, folic acid, vitamin B12, and vitamin C. Significantly more participants who were vitamin A deficient scored in the lowest tertile than those in higher tertiles.
Conclusion
The SA-DQI-P is the first DQI developed for a South African population and has proven to be valid in ranking diet quality in pregnant women in our sample. Information regarding diet quality of this vulnerable group can assist with planning nutrition intervention programs to improve nutritional status.
Development of a Diet Quality Index for Pregnant Women in South Africa
Good nutrition during pregnancy can contribute to the better health of the mother and baby. There are various nutrition-related guidelines and recommendations that pregnant women should follow to help them to ensure that they are receiving all the nutrients that are required for both mother and baby. Since the diet is so complex it is a good idea to test the entire diet as a whole to see how well the diet aligns with the recommendations. In order to do this, an index can be developed to give a score for the entire diet—the better the score, the closer the diet is to the guidelines which can promote health. We developed our own diet quality index (DQI) to test the quality of the diet of pregnant women in South Africa. The index contains the following beneficial components: wholegrains, vegetables, whole fruit, dairy, eggs, fish, legumes, iron, calcium and folate. It also includes a limit on added sugar and saturated fatty acids (SFAs) because these nutrients are not related to good nutrition. We found that the women in our study scored the lowest in the wholegrain, fish, legumes, and whole fruit components. We found that there are some sociodemographic factors that can increase the chances of not scoring high in our index, such as a lower educational level and not being food secure (having access to enough adequate food in the household). Intakes of many beneficial nutrients were related to higher scores. Many participants who did not consume enough vitamin A scored low in our index. This type of information can help with planning nutrition intervention programs to improve nutrition in pregnant women.
Introduction
Ensuring optimal diet quality during pregnancy is vital for supporting normal fetal development, and it is well-known that maternal malnutrition increases short-and long-term health risks for both mother and offspring. 1 In Africa, maternal malnutrition is prevalent and was estimated at 23.5% based on a pooled analysis of 23 studies. 2 This widespread maternal malnutrition is a reflection of broader dietary patterns observed in particular regions such as urban Soweto, South Africa, where women of reproductive age often consume poor-quality diets characterized by a heavy reliance on refined grain intake due to its affordability and availability, with a low intake of nutrient-dense foods. 3
DQIs offer a valuable tool for assessing adherence to dietary recommendations and guidelines with the goal of evaluating the overall quality of a diet. DQIs consist of different combinations of foods and/or nutrient components and enable researchers to evaluate various related aspects of the diet concurrently which may provide a good description of usual dietary intake. 4
Dietary recommendations for pregnancy differ from general recommendations, resulting in the development of specific DQIs for this population. Several DQIs specifically for pregnancy have been developed. 5 These indexes generally contain food groups such as fruit, vegetables, grains, meat, and legumes, as well as nutrients that are especially important during pregnancy (iron, folic acid, calcium, and omega-3 fatty acids).6–10 Some DQIs for pregnancy add components indicating fat and carbohydrate quality.7,8 Han et al 10 were unique in adding the use of antenatal supplements in the DQI they developed, while the DQI by Crivellenti et al 9 is the only index for pregnancy that includes the intake of ultraprocessed foods (UPF) as a moderator component (referring to a dietary component that should be limited or eaten in moderation). The published DQIs developed in different countries for use in pregnancy were based on the unique dietary guidelines and recommendations of each country. While South Africa has no pregnancy-specific dietary guidelines, pregnant females can follow the South African Food Based Dietary Guidelines (SAFBDGs), which are suitable for all individuals above the age of 5 years. 11 Furthermore, the Department of Health Guidelines for Maternity Care in South Africa 12 offer specific recommendations for the intake of iron, folic acid, and calcium during pregnancy. International maternity nutrient intake and supplementation guidelines are also available, such as those developed by the Institute of Medicine (IOM) (now known as the National Academy of Medicine) as well as the World Health Organization (WHO).13,14
Although certain DQIs for use during pregnancy are available, most were developed using dietary recommendations and dietary intake data from high-income countries such as the United States of America, Canada, Ireland and Finland, 5 while none has specifically been developed and validated for African populations. The absence of country-specific DQIs represents a significant gap, as using a contextually and culturally relevant tool to determine and monitor diet quality is vital in ensuring the accuracy and pertinence of the results.
To address this gap, we developed the South African Diet Quality Index for Pregnancy (SA-DQI-P). This tool enables the evaluation of adherence of pregnant South African women to maternal dietary recommendations which is vital for the development and refinement of nutrition interventions.
This study aimed to develop and validate the SA-DQI-P by applying it to a sample of pregnant women urban central South Africa. For validation, differences in diet quality scores by sociodemographic characteristics, household food security level, nutrient intakes, and biochemical variables were also determined.
Methods
Structure and Development Process of the DQI for Pregnant Women in South Africa (SA-DQI-P)
Aspects related to component selection and scoring practices need to be considered during the development of a DQI. 15
Component Selection of the SA-DQI-P
The SAFBDGs as well as the Guidelines for Maternity Care in South Africa underpinned the selection of components. In addition, specific international food and nutrient recommendations related to pregnancy were considered, which included recommendations from the IOM and the WHO. An a priori approach to component selection was followed, meaning that they were selected based on current knowledge of nutrition-related factors that affect health. 15
SAFBDGs as a Theoretical Basis for Component Inclusion
The SAFBDGs were used as the main theoretical basis for the inclusion of specific foods, food groups, and nutrients in the index. Table 1 summarizes the current SAFBDGs and indicates which component represents each guideline.
The SAFBDGs and Corresponding SA-DQI-P Component.
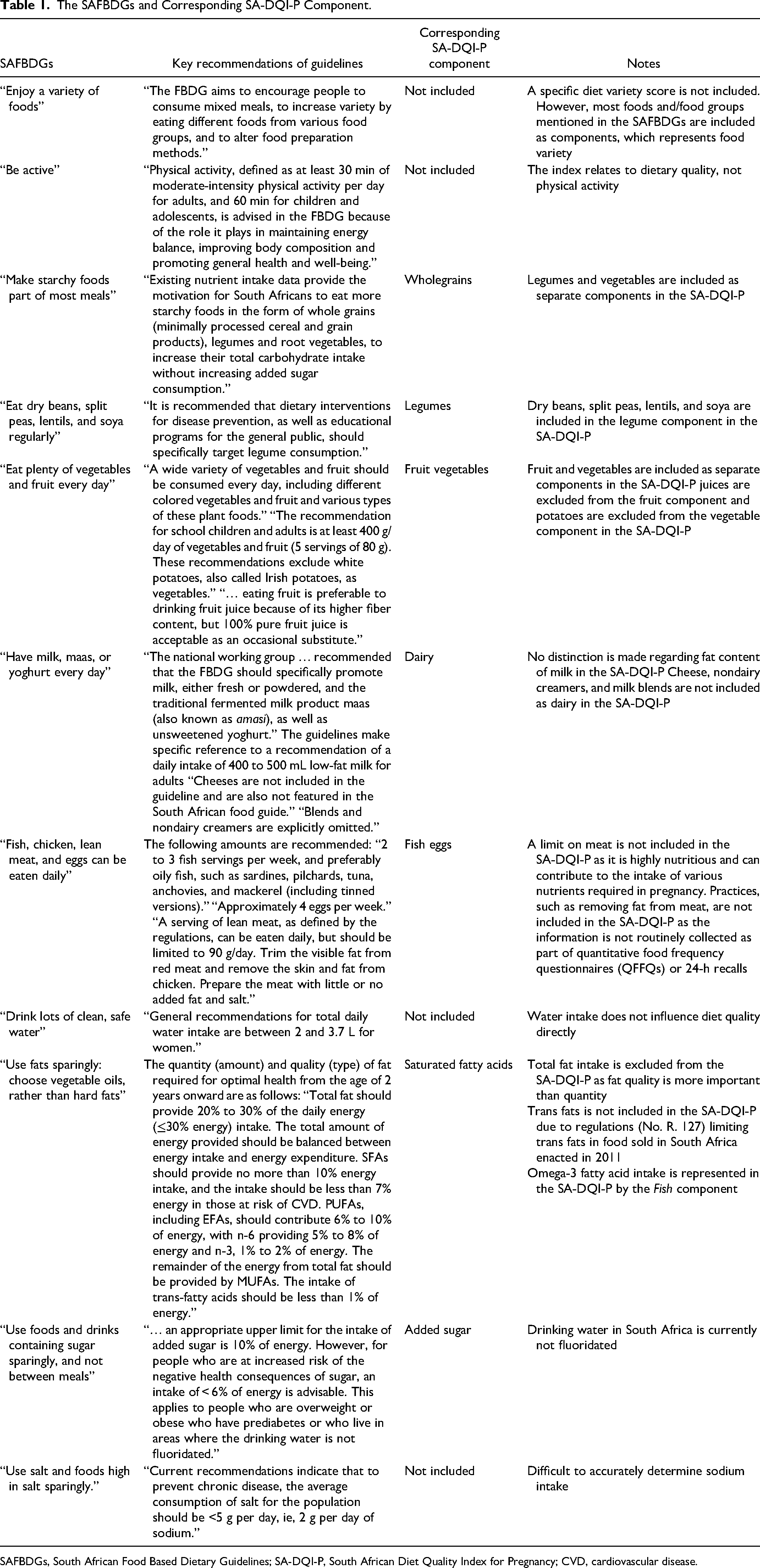
SAFBDGs, South African Food Based Dietary Guidelines; SA-DQI-P, South African Diet Quality Index for Pregnancy; CVD, cardiovascular disease.
Other Nutrition-Related Pregnancy Guidelines as a Theoretical Basis for Component Inclusion
The IOM and WHO guidelines recommend an increased intake of iron, folic acid, and calcium during pregnancy.13,14 Prenatal micronutrient supplementation with iron, folic acid, and calcium is also specifically recommended in the Guidelines for Maternity Care in South Africa and by the WHO.12,14 Therefore, intake of these nutrients is included in the SA-DQI-P.
Food Variety Dimension
The following components comprise the food variety dimension of the SA-DQI-P: wholegrains, vegetables, whole fruit, dairy, eggs, fish, and legumes.
We chose the standard for the maximum score for the wholegrain component used in the Healthy Eating Index—2015 (HEI-2015) 16 as the SAFBDGs do not indicate a specific amount of wholegrains that should be consumed. Since the SAFBDGs recommend a combined intake of 400 g of fruits and vegetables per day, we opted to use the scoring guidelines of the DQI Adapted for Pregnant Women (IQDAG) 9 as it represents fruit and vegetables as separate components and considers intake thereof relative to energy intake. Additionally, the fruit component of the IQDAG focuses on whole fruit intake only (excluding 100% juice and juice blends), which aligns with the recommendations of the SAFBDGs. Fresh, frozen, canned, and dried fruits are included in the fruit component, as recommended in the SAFBDGs. 17 We included the recommendation of the SAFBDGs regarding dairy intake (400-500 mL of low-fat dairy per day) in the scoring of the component. This intake range excludes cheese and mainly focuses on low-fat milk, maas (cultured milk drink), and yoghurt. A review of dietary surveys in South Africa (2000-2015) indicates that full cream milk is one of the top foods adults consume. 18 Recent evidence suggests that dairy fat exerts a neutral or positive effect on cardiovascular health. 19 Therefore, no distinction is made regarding the fat content of dairy products in the SA-DQI-P. For scoring purposes, a maximum score will be obtained at an intake of 400 mL daily.
Eggs were included in the SA-DQI-P in amounts recommended by the SAFBDGs (3 to 4 eggs per week). As eggs are an excellent source of numerous nutrients, including protein, choline, vitamin D, vitamin A, vitamin E, lutein, zeaxanthin, and nonheme iron, it is a cost-efficient way to provide these nutrients in the diet. Eggs are also a major source of dietary cholesterol. However, the most current Dietary Guidelines for Americans (2020-2025) do not explicitly focus on reducing dietary cholesterol. Rather, the guidelines state the following: “The National Academies recommends that trans-fat and dietary cholesterol consumption be as low as possible without compromising the nutritional adequacy of the diet.” 20 Thus, we concluded that because eggs are extremely nutritious, intake of more than 3 eggs per week, would not negatively impact scoring of the component. Egg and dairy intake were also specifically included in the SA-DQI-P because they contribute significantly to choline intake. Maternal choline intake plays a vital role in placental functioning, foetal neurodevelopment and epigenetic programming in the foetus. 21
The SAFBDGs recommend 2 to 3 servings (80 to 90 g per serving) of fish per week. However, this recommendation is not specific to pregnant women and includes tinned fish. 22 Therefore, the joint recommendation for pregnant women of the Environmental Protection Agency and Food and Drug Administration 23 was used for scoring purposes in the SA-DQI-P. These guidelines acknowledge that fish intake should be limited during pregnancy (240 to 360 g lower mercury fish per week) to prevent excessive intake of mercury.
Since legumes have various health and environmental benefits and are specifically promoted in the SAFBDGs, they were included as a separate component in the SA-DQI-P. The scoring categories for legumes were adopted from the IQDAG, as it includes legumes as a separate component and is not combined with other food groups such as vegetables or seafood and other plant proteins, as is used in the HEI-2015. 16
Nutrient Adequacy Dimension
Scoring of the micronutrients (iron, folate, and calcium) is based on the joint Food and Agriculture (FAO) and WHO/FAO estimated average requirements 24 for use in pregnancy (second trimester). The dietary reference intakes of the IOM were not used, as the WHO/FAO recommendations are deemed to be more suitable for use in developing countries. 25 Scoring of micronutrient intake in the SA-DQI-P does not take micronutrient supplementation into account.
Even though adequate choline intake is essential during pregnancy (similar to iron, folate, and calcium), we chose not to include it as a separate component in the SA-DQI-P. The choline content of foods is currently not included in the food composition databases of most countries. For example, choline composition is not available in the South African Food Composition Database, 26 nor the European food composition databases27,28 and therefore the National Nutrient Database of the USDA 29 is usually used to determine choline intake of populations from different countries. The matching of foods consumed in a particular study to foods in the USDA Food Composition Database in order to determine choline intake in a population is a time-intensive and, therefore expensive process. Resource-limited areas might not have the capacity to support and promote the determination of choline intake in the specific population of interest. For this reason, eggs and dairy (good food sources of choline) were specifically included in the SA-DQI-P.
Moderation Dimension
The moderation dimension is represented by limiting added sugar and SFA in the diet. The SAFBDGs specifically state that, in areas where water is not fluoridated, such as South Africa, added sugar intake must not exceed 6.0% of total energy (TE). This recommendation was made based on the association between higher sugar intake and a higher risk of dental caries. Fluoridated water has been shown to decrease the risk of caries. 30 The SAFBDGs recommend a SFA intake of <10.0% of TE, while a further recommendation of <6.0% of TE is made for individuals at risk of cardiovascular disease (CVD). A maximum value of 10.0% of TE was chosen for SFA intake for the SA-DQI-P, as the tool is designed to be able to be implemented with data collected from a quantified food frequency questionnaire (QFFQ) or multiple 24-h recalls, and medical information will not necessarily be available to be able to differentiate between individuals at risk for CVD and those not at risk. Additionally, the 2 other DQIs for pregnancy that do include SFA as a component both use a cutoff value of ≤10.0% of TE.10,31 The standard for minimum scores for these components was derived from the HEI-2015. The authors used the updated 2011 to 2012 National Health and Nutrition Examination Survey data as reference to set this standard. However, it was not used as the only criterion, as the standards may not remain appropriate for use if intakes improved substantially over time. Thus, the established criteria for added sugar and SFAs minimum standards rely on professional assessment and are linked to consumption levels deemed excessive. 16
Scoring of SA-DQI-P Components
The inclusion of certain foods, food groups and nutrients as components in the SA-DQI-P is supported by the SAFBDGs and other dietary guidelines. However, scoring of these components is based on other indexes and specific pregnancy recommendations, as the SAFBDGs do not specifically provide recommended intake amounts per unit of energy intake of the food groups (wholegrains, fruit, vegetables, and legumes). Adapting scoring to energy intake in DQIs is recommended to prevent individuals with a high energy intake from obtaining a high DQI score, while their intakes of food groups are possibly imbalanced. 15
All components have equal weighting (a maximum of 10 points per component), and scores are calculated proportionately between the minimum and maximum standards (a maximum final score of 120 points can be obtained) (Table 2).
Diet Quality Index for Pregnant Women in South Africa (SA-DQI-P).
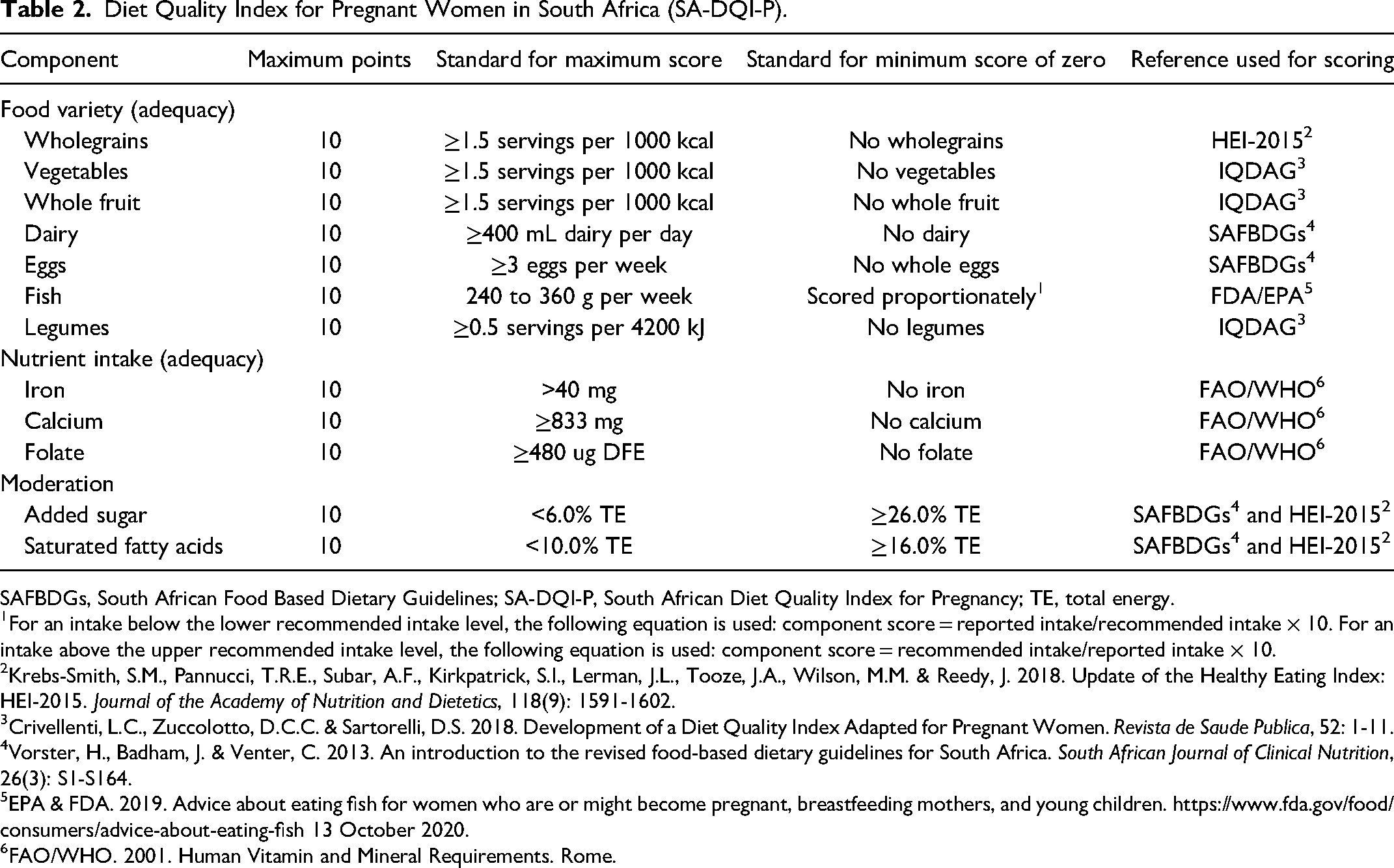
SAFBDGs, South African Food Based Dietary Guidelines; SA-DQI-P, South African Diet Quality Index for Pregnancy; TE, total energy.
For an intake below the lower recommended intake level, the following equation is used: component score = reported intake/recommended intake × 10. For an intake above the upper recommended intake level, the following equation is used: component score = recommended intake/reported intake × 10.
Krebs-Smith, S.M., Pannucci, T.R.E., Subar, A.F., Kirkpatrick, S.I., Lerman, J.L., Tooze, J.A., Wilson, M.M. & Reedy, J. 2018. Update of the Healthy Eating Index: HEI-2015. Journal of the Academy of Nutrition and Dietetics, 118(9): 1591-1602.
Crivellenti, L.C., Zuccolotto, D.C.C. & Sartorelli, D.S. 2018. Development of a Diet Quality Index Adapted for Pregnant Women. Revista de Saude Publica, 52: 1-11.
Vorster, H., Badham, J. & Venter, C. 2013. An introduction to the revised food-based dietary guidelines for South Africa. South African Journal of Clinical Nutrition, 26(3): S1-S164.
EPA & FDA. 2019. Advice about eating fish for women who are or might become pregnant, breastfeeding mothers, and young children. https://www.fda.gov/food/consumers/advice-about-eating-fish 13 October 2020.
FAO/WHO. 2001. Human Vitamin and Mineral Requirements. Rome.
The following equations are used for scoring different components, as described by Borge et al.
31
1. For components with a minimum intake recommendation (wholegrains, vegetables, whole fruit, dairy, eggs, iron, calcium, and folate), the following equation applies: 2. For components with a maximum intake recommendation (added sugar and saturated fat), the following equation applies: 3. For the fish component which has both a minimum and a maximum recommendation, the formulae in points 1 and 2 for intakes below the lower recommended intake level and above the upper recommended intake level, respectively, were used.
Intakes above the recommended minimum intake are scored a maximum score of 10.

Intakes below the recommended maximum intake are scored a maximum score of 10.

Table 2 summarizes the SA-DQI-P. Three categories of components are defined: food variety, nutrient adequacy, and moderation.
Content and Construct Validity
The concept of content validity can be defined as “how well the items developed to operationalize a construct provide an adequate and representative sample of all the items that might measure the construct of interest.” This type of validity typically depends on the judgment of the researcher/expert in the field since no statistical test is available to establish if a measure or tool sufficiently covers a content area. 32 Content validity was ensured by using the SAFBDGs as the basis for the components in the index, and by using recommended nutrient intake levels for pregnant women as described in the literature. Aligning the SA-DQI-P to the SAFBDGs ensures that the chosen components have a well-described evidence base for health promotion.
Construct validity “…assesses the extent to which a measure performs in accordance with theoretical expectations.” 33 We determined the association between SA-DQI-P scores in tertiles with nutrient intakes, sociodemographic factors, household food security level, and biochemical values.
Population and Data Collection Methods
This study used data from the Nutritional status of Expectant Mothers and their newborn Infants (NuEMI) study, a prospective cohort study investigating the nutritional status of pregnant women and determinants of birth outcomes. Data were collected between 2018 and 2019. The study recruited pregnant women in their second or third trimester attending the antenatal clinic at a regional hospital in Bloemfontein, South Africa. This clinic is considered a higher-risk clinic to which older women (>35 years), multiple pregnancies, women with previous poor pregnancy outcomes (neonatal death and preterm delivery), women with 2 or more previous cesarean sections, women with a gravida of 6 or more pregnancies, as well as those with obesity, hypertension, or diabetes mellitus are referred from surrounding areas and towns. Information regarding the study was explained to all participants by a fieldworker. Trained fieldworkers obtained information from participants during structured interviews using several questionnaires, including a sociodemographic questionnaire and a QFFQ. Household density ratio (HDR), an indication of overcrowding in a dwelling, 34 was calculated, and household food security was determined using the Household Food Insecurity Access Scale. 35 Additionally, blood samples were obtained to determine levels of hemoglobin (Hb), ferritin and retinol-binding protein (RBP). Inclusion criteria were as follows: adult (≥ 18 years) pregnant women in their second or third trimester who could speak one of the main 3 languages in the area, namely English, Afrikaans, and SeSotho. Women who were pregnant with more than 2 fetuses were excluded. A consecutive convenience sample of 682 participants was included. For the NueMI study no sample size calculation was performed since the study had numerous outcomes and analysis objectives. The sample was however, collected consecutively over a 12-month period. In the validation study the power to detect large differences (of 15% or more) between tertile groups of size 200 was more than 80%.
This study was done in accordance with the Declaration of Helsinki and ethics approval was obtained from the Health Sciences Research Ethics Committee at the University of the Free State (UFS-HSD2017/0969). All participants provided written informed consent before data collection commenced.
Dietary Intake and Analysis
A QFFQ was used to obtain dietary intake information during structured interviews with trained fieldworkers. The QFFQ was previously validated for the population in the Transition and Health during Urbanization of South Africans study 36 as well as for the Women's Health Study in the Free State, South Africa 37 and has proven reproducibility.37–39 This QFFQ was more recently used among pregnant women in the Nutrition during Pregnancy and Early Development study conducted in South Africa. 40 The QFFQ comprises information on approximately 329 commonly consumed food items; however, fieldworkers in the current study could add any food item in spaces made available on the QFFQ for items not already listed. Dietary intake was determined for the previous 28 days. Nutrient intake values were divided by 28 to calculate daily intake (See Robb et al 41 for a detailed description of dietary intake methodology).
Biochemical Values
Whole blood (50 µL) was collected during a finger prick procedure. Immediately after the finger prick, hemoglobin (Hb) concentration was measured in the blood sample using the HemoCue Hb 201+ System. On-site, the blood was processed to obtain plasma aliquots and stored at 4°C. The samples were transported daily from the study site in cooler bags with refrigerant gel ice packs to The University of the Free State for storage at −80 °C. The samples were later transported for analysis to the micronutrient laboratory of the Centre of Excellence for Nutrition (CEN) at the North-West University (NWU). The iron status indicator ferritin and the vitamin A status indicator RBP were measured in heparin plasma using the Q-Plex™ Human Micronutrient Array (Quansys Bioscience, Utah, USA) at the CEN laboratory, NWU.
The acute phase proteins alpha1-acid glycoprotein and C-reactive protein were used to identify subjects with inflammation, which confounds ferritin and vitamin A statuses. Ferritin and RBP values were adjusted according to methods described by Thurnam et al. 42 Additionally, Hb was adjusted according to the altitude as recommended by the WHO. 43 WHO cutoff values for Hb were used to define anemia (<11 g/dL). 44 Iron deficiency was defined as an adjusted ferritin value of <15 μg/L. 45 Vitamin A deficiency (VAD) was defined as the following: mild VAD (RBP ≥0.70 µmol/L and <1.05 µmol/L) and VAD (RBP <0.70 µmol/L). 46
Statistical Analysis
Numerical variables were summarized by medians and interquartile ranges (IQRs) due to skew distributions, and categorical variables by frequencies and percentages. SA-DQI-P scores were categorized in tertiles (1. 0-57, 2. 58-70, 3. 71-120) and cross-tabulated against categorical sociodemographic and nutrient intake variables with chi-squared tests. Numerical nutrient intake values were compared between SA-DQI-P tertiles using Kruskall–Wallis tests. All analyses were done using SAS Version 9.4.
Results
SA-DQI-P Score
SA-DQI-P scores were calculated for 681 participants (1 participant had no dietary intake information), with a median score of 64 out of a maximum of 120 (IQR: 53-74) (Table 3). Participants scored the lowest in the wholegrain, fish, legumes, and whole fruit components, indicating that they especially struggled to meet the recommendations for intake of these components.
SA-DQI-P Component Scores and Total Score.
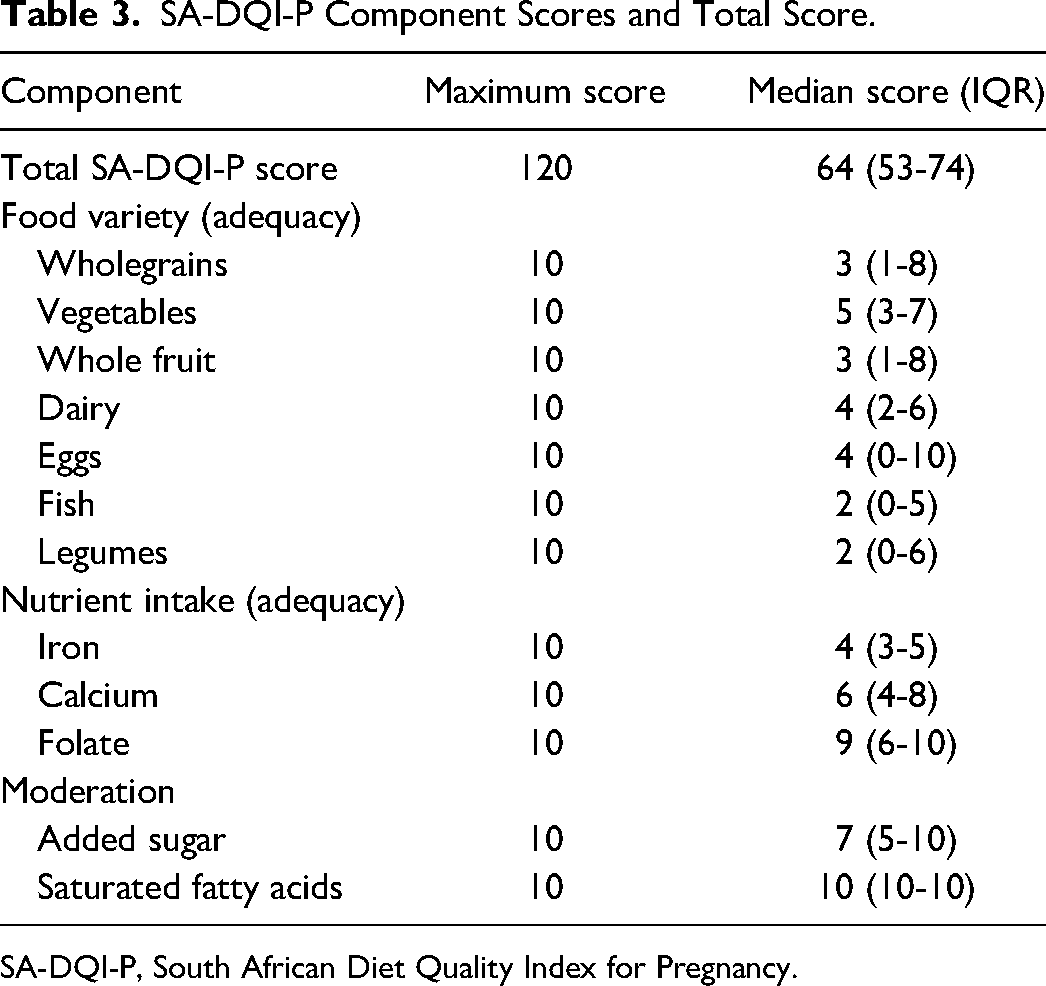
SA-DQI-P, South African Diet Quality Index for Pregnancy.
Construct Validity
The following sociodemographic factors were significantly associated with a higher SA-DQI-P score: lower HDR, household access to a toilet, refrigerator and microwave, a higher educational level, being employed, and being food secure (Table 4).
SA-DQI-P Tertiles According to Sociodemographic Factors and Household Food Security Level.
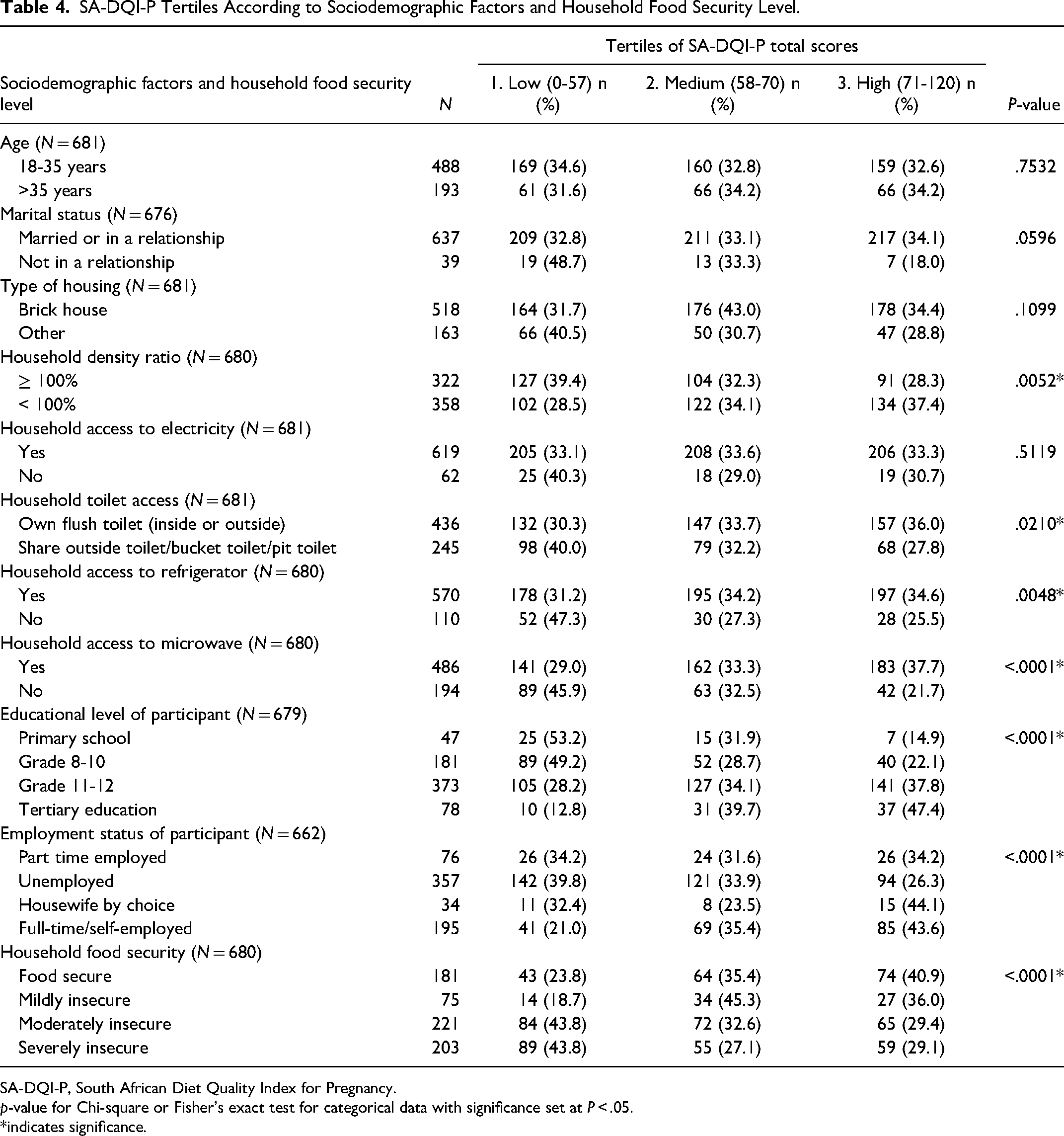
SA-DQI-P, South African Diet Quality Index for Pregnancy.
p-value for Chi-square or Fisher's exact test for categorical data with significance set at P < .05.
*indicates significance.
Consumption of protein, added sugar, and fiber in recommended amounts were significantly associated with better SA-DQI-P scores (Table 5). Similarly, significantly more participants consumed the recommended intakes of micronutrients (calcium, zinc, vitamin A, vitamin E, folic acid, vitamin B12, and vitamin C) as scores increased per tertile. Statistically significant differences were found between tertiles 1 and 2, tertiles 1 and 3 as well as tertiles 2 and 3 for all nutrients, except between tertiles 2 and 3 for saturated fat and cholesterol.
Percentage of Participants Meeting Recommended Nutrient Intakes According to SA-DQI-P Tertiles.
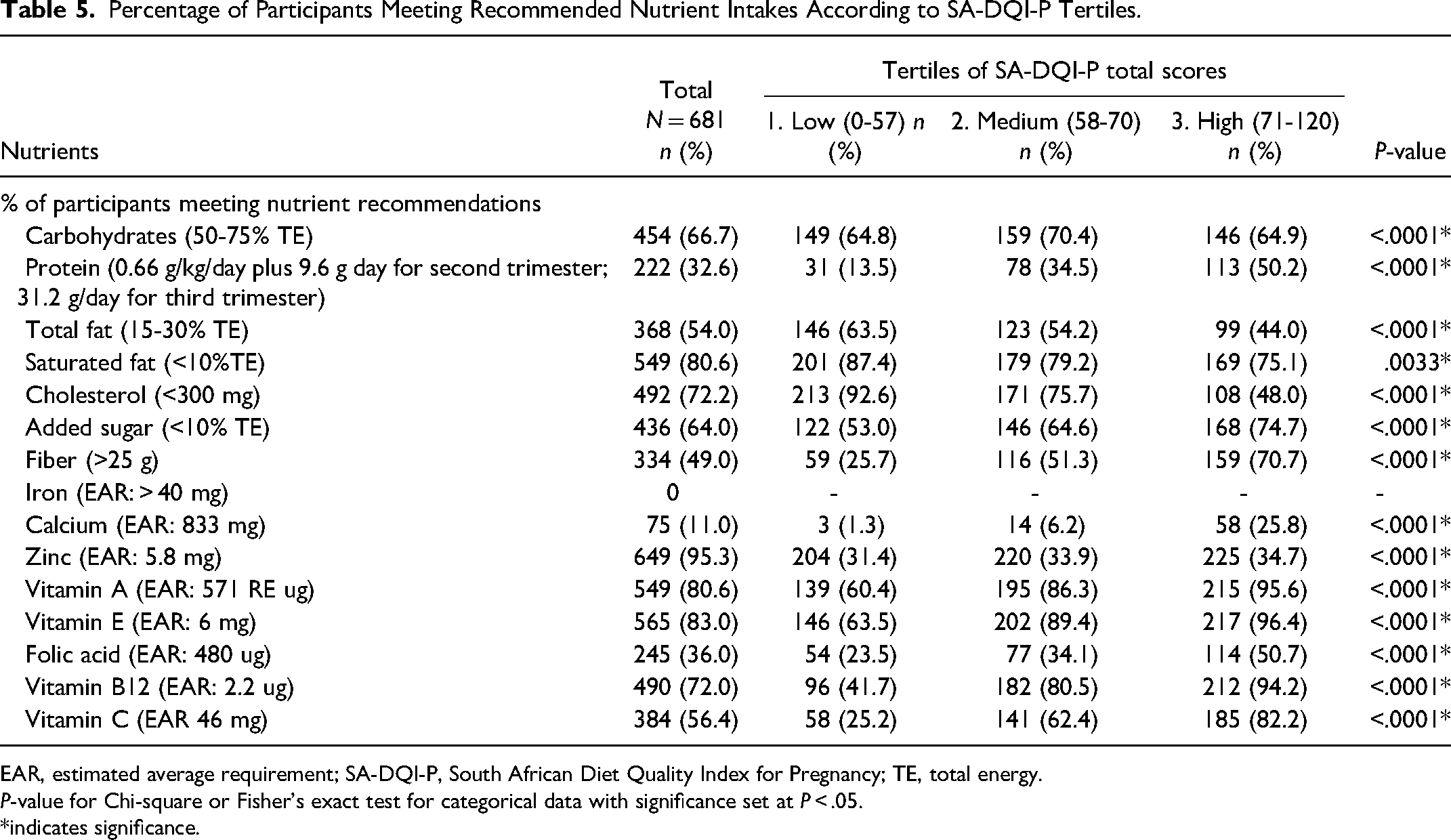
EAR, estimated average requirement; SA-DQI-P, South African Diet Quality Index for Pregnancy; TE, total energy.
P-value for Chi-square or Fisher's exact test for categorical data with significance set at P < .05.
*indicates significance.
When nutrient intakes were expressed as continuous variables, and energy intake was also accounted for, carbohydrate and added sugar intakes decreased as SA-DQI-P score increased (Table 6), while protein, total fat, saturated fat, and cholesterol intakes increased as the score increased. Calcium, vitamin A, vitamin E, folic acid, vitamin B12, and vitamin C intakes increased as the score increased. Fiber, iron, and zinc intakes did not differ statistically between SA-DQI-P tertiles. Statistically significant differences were found between tertiles 1 and 2, tertiles 1 and 3, as well as tertiles 2 and 3 for all nutrients, except between tertiles 1 and 2 for fiber, added sugar, iron, and zinc, tertiles 2 and 3 for fiber, added sugar, iron, folic acid, and vitamin E, and tertiles 1 and 3 for fiber and zinc.
Nutrient Intakes as Continuous Variables According to SA-DQI-P Tertiles.
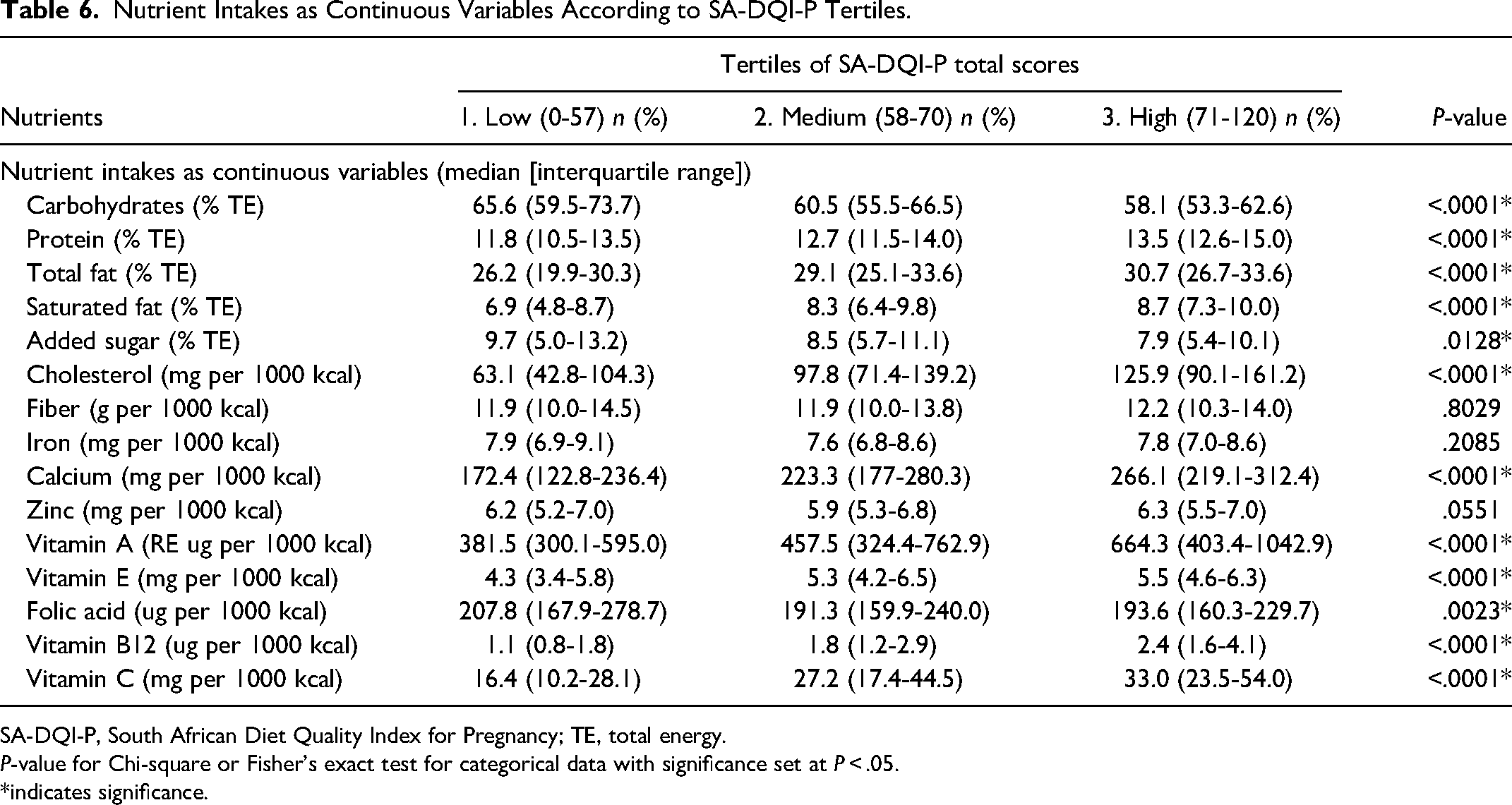
SA-DQI-P, South African Diet Quality Index for Pregnancy; TE, total energy.
P-value for Chi-square or Fisher's exact test for categorical data with significance set at P < .05.
*indicates significance.
A slightly higher percentage of VAD occurred in the lowest SA-DQI-P tertile that in the other tertiles, and the highest percentage of mild VAD occurred in the medium SA-DQI-P tertile (Table 7, P = .0398). No statistically significant associations were found between SA-DQI-P tertiles and ferritin or hemoglobin levels.
Biochemical Values According to SA-DQI-P Tertiles.
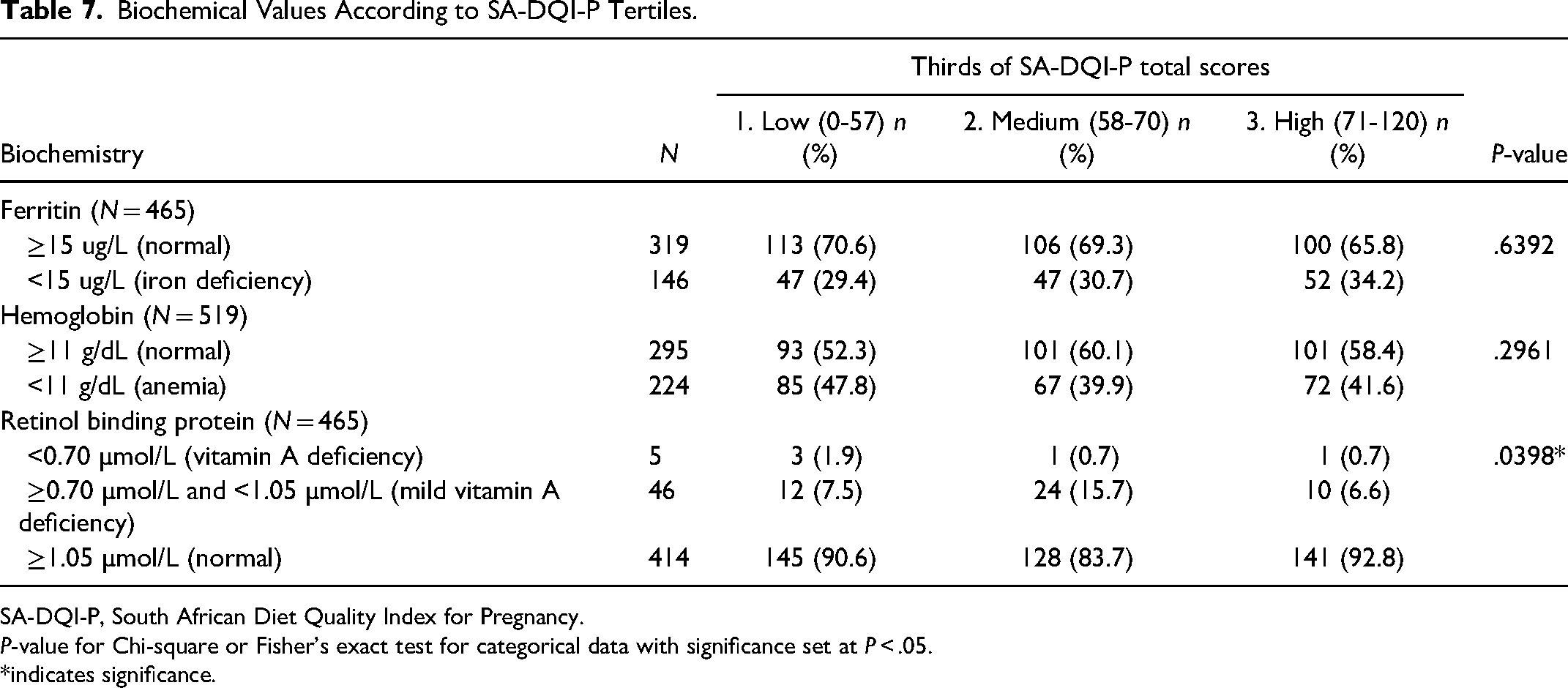
SA-DQI-P, South African Diet Quality Index for Pregnancy.
P-value for Chi-square or Fisher's exact test for categorical data with significance set at P < .05.
*indicates significance.
Discussion
A notable gap in maternal nutrition assessment methodology and practice has been addressed with the development and validation of the SA-DQI-P. This tool enables the culturally and contextually relevant determination of maternal diet quality in South Africa.
During the development of a DQI, component selection is a vital step. Not all food groups and nutrient components with known beneficial or detrimental effects on health were included in the SA-DQI-P. For example, even though the intake of UPF is considered detrimental to health, 47 the inclusion of a UPF component was not considered, as according to the international NOVA classification system for UPFs, 47 staple foods of the South African population (eg, most breads, porridges, and cereals, including wholegrain versions), despite being fortified with micronutrients, would be considered as UPF which would impact negatively on scoring. Clear cutoff values for UPF intake have also not been developed. Despite the fact that hypertension is a health concern in the South African population, 48 sodium intake was not considered as a component since it is difficult to accurately determine sodium intake, 49 and thus, this component was excluded. However, the SA-DQI-P does include dairy and fruit and vegetables (high in calcium, magnesium, and potassium) that have proven benefit in reducing blood pressure. 50 Choline was also not included as a component (as discussed above). However, eggs and dairy were included, as these foods are important contributors of choline in the diet. Robb et al demonstrated that the odds of a choline intake below the adequate intake level in pregnant women in the Free State, South Africa, increased significantly as egg and dairy intake decreased. 41
According to Trijsburg et al, 51 DQIs should undergo validation before widespread use thereof can be recommended. In the current study we have made use of content and construct validity during the validation process.
Sociodemographic Factors and Household Food Security
Various sociodemographic variables were associated with the SA-DQI-P score. Combined, these variables suggest that a higher socioeconomic status in the setting of the current study, in general, could be related to a better diet quality. Most of the DQIs for use during pregnancy that have been developed in recent years have also determined associations between sociodemographic factors and the diet quality score as part of the validation process.6,7,9,10,31,52–54
Although none of the recently developed DQIs for pregnancy have included the association between diet quality score and food security during development and validation, other studies have investigated level of food security and diet quality using DQIs for pregnancy. In the United States of America, both Nahm et al 51 and Gamba et al 55 found no association between maternal food security status and overall diet quality among pregnant women. However, similar to the current study, Bukari et al 56 found a positive association between poorer food security status and lower overall diet quality scores among pregnant women in Ghana, suggesting that the association between food security and diet quality among pregnant women might differ between low-, middle-, and high-income countries.
Nutrient Intakes
After correcting for energy intake, higher intakes of protein, total fat, saturated fat, calcium, vitamin A, vitamin E, folic acid, vitamin B12, and vitamin C were significantly associated with higher scores. Several DQIs that have been developed for pregnancy have included associations with nutrient intakes as part of the validation, and similar results were observed.6,8–10,54 Even with an increase in diet quality, the nutrient density (amount of nutrient per 1000 kcal) for iron, fiber, and zinc does not increase significantly. Participants in the sample scored low in most fiber-rich components (whole fruit, wholegrain, and legumes), and meat (high in iron and zinc) was not included as a component in the SA-DQI-P.
The SA-DQI-P is based on food intake alone, which excludes nutrient intake from micronutrient supplementation. The main reason for this is related to the use of the SA-DQI-P to evaluate the quality of foods that are consumed. Inclusion of supplement use in scoring may substantially increase points scored which can lead to a false category outcome that can lead to women not obtaining the necessary recommendations for improving their diet. Additionally, the assessment of compliance with supplement use recommendations might prove difficult and thus not reflect true intake. However, nutrient intake from the mandatory fortification of maize-meal and bread flour in South Africa 57 was included in the current study. Mandatory fortification of foodstuffs in a country can significantly affect the intake of certain nutrients and must be considered when diet quality results are interpreted. The finding that no participant could meet iron requirements from diet alone underscores the importance of using iron supplements at appropriate dosages during pregnancy.
Biochemical Values
No statistically significant association was found between SA-DQI-P score and ferritin or hemoglobin values in the current study. This is similar to studies done in Indonesia 58 and Ghana 59 where dietary diversity was not associated with anemia or ferritin levels among pregnant women. A review of studies conducted in Ethiopia, Kenya, Nigeria, and South Africa determined a prevalence of VAD among pregnant women ranging from 21% to 48%. 60 This is higher than found in the current study (11.0%), when mild VAD and VAD is combined. In the current study, more participants who were classified as being vitamin A deficient scored in the lowest SA-DQI-P tertile than those in the higher categories, suggesting that diet quality could influence vitamin A status among pregnant women. It is recommended that future studies investigate the association between mild VAD and diet quality, as the finding that women in the second SA-DQI-P tertile had the highest percentage of mild VAD was an unexpected finding.
Conclusion
We developed the SA-DQI-P based on national and international maternal dietary guidelines. This tool can be used by nutrition researchers in large-scale studies to identify populations with a poor maternal diet quality in South-Africa, and can possibly be used as a model for other sub-Saharan African countries. Scores can be calculated and compared periodically in similar populations to determine improvement or deterioration of maternal diet quality. Implementing this tool to collect data on maternal dietary intake could inform national policies on nutrition education programs, food and nutrient supplementation programs and the distribution of resources, specifically for pregnant women residing in communities with high levels of food insecurity. Utilizing the SA-DQI-P in other areas of South Africa can provide indispensable data required for advocating for more comprehensive nutrition-focused policies. These interventions can ultimately improve pregnancy outcomes and the long-term health of both the mother and her offspring, while also potentially reducing health care costs related to poor birth outcomes.
Footnotes
Author Contributions
The authors responsibilities were as follows: Liska Robb, Corinna May Walsh, and Gina Joubert were responsible for the project conception. Liska Robb and Elizabeth Margaretha Jordaan coded dietary intake data and Jennifer Ngounda supervised data collection and collected blood samples. Louise van den Berg was involved in the analysis of certain aspects of the dietary data. Gina Joubert performed statistical analysis. Liska Robb wrote the paper and had primary responsibility for the final content. All authors have read and approved the final manuscript.
Data Availability
Data described in the article will be made available upon reasonable request pending adequate permissions.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Department of Nutrition and Dietetics, University of the Free State, Bloemfontein, South Africa, funded this research project.