
Abstract
Background:
Zinc deficiency affects multiple vital functions in the life cycle, especially growth. Limited information is available on the magnitude of zinc deficiency in Latin America and the Caribbean.
Objective:
To examine the latest available information on both the prevalence of zinc deficiency and the risk of zinc deficiency in Latin America and the Caribbean.
Methods:
The prevalence of zinc deficiency was identified through a systematic review looking for the latest available data on serum zinc concentrations from surveys or studies with national representativeness conducted in Latin America and the Caribbean. The risk of zinc deficiency in Latin America and the Caribbean was estimated based on dietary zinc inadequacy (according to the 2011 National Food Balance Sheets) and stunting in children under 5 years of age.
Results:
Only four countries had available national biochemical data. Mexican, Colombian, Ecuadorian, and Guatemalan children under 6 years of age and women 12 to 49 years of age had a high prevalence of zinc deficiency (19.1% to 56.3%). The countries with the highest risk of zinc deficiency (estimated prevalence of inadequate zinc intake >25% plus prevalence of stunting >20%) were Belize, Bolivia, El Salvador, Guatemala, Haiti, Honduras, Nicaragua, and Saint Vincent and the Grenadines. Zinc dietary inadequacy was directly correlated with stunting (r = 0.64, p < .001).
Conclusions:
Prevalence data from the four available Latin America and Caribbean national surveys indicate a high prevalence of zinc deficiency in children under 6 years of age and women 12 to 49 years of age. High rates of both estimated zinc dietary inadequacy and stunting were also reported in most Latin America and Caribbean countries.
Introduction
Zinc is an essential trace mineral that serves as a cofactor for over 300 enzymes and is important for the maintenance of biochemical functions throughout life. 1 Zinc deficiency has been associated with a variety of biochemical and physiological abnormalities, such as retarded growth and impaired immune function. 2 The development of zinc deficiency can be a result of dietary inadequacy, increased requirements during rapid growth periods, malabsorption, increased losses, and/or impaired utilization. 3 A U-shaped relationship has been suggested between zinc status and optimal health. 4,5 Serum zinc concentration is the most frequently used biochemical indicator of zinc status in populations. 6 Alternatively, the risk of zinc deficiency has been commonly estimated based on dietary intake and childhood stunting. 7,8 The objective of the present article was to estimate the magnitude of zinc deficiency in Latin America and the Caribbean based on the prevalence of low serum zinc concentrations assessed at the national level. Additionally, we examined the risk of zinc deficiency using both the amount of absorbable zinc present in the national food supply and rates of stunting in children under 5 years of age.
Methods
Prevalence of Zinc Deficiency
A systematic review was conducted between July 2011 and April 2012 and updated in August 2014 to identify surveys and representative studies that assessed zinc deficiency based on serum zinc concentrations. All available evidence conducted in apparently healthy populations regarding the prevalence of zinc deficiency in Latin America and the Caribbean since 2000 was included. PubMed, LILACS, Nutrinet, and Scielo were used to identify research articles by combining the terms “zinc,” “deficiency,” “intake,” and “prevalence” with the name of each country in Latin America and the Caribbean. Studies were not excluded on the basis of language. In addition, national surveys were identified by accessing the websites of the ministries of health for each country. The prevalence of zinc deficiency was reported by low serum zinc concentrations according to cut points used in each study or survey. A prevalence of zinc deficiency higher than 20% was considered to be a public health problem. 1,8
Estimation of the Prevalence of Inadequate Zinc Intake
The dietary intake of zinc at the national level was also explored for those countries for which there was a lack of national biochemical data but dietary intake information was available from food frequency questionnaires or 24-hour recalls. Estimated Average Requirements (EAR) were used to assess adequacy of dietary intake. 4 The sequence of calculations to estimate the prevalence of inadequate zinc intake was based on the following analytical methods and model assumptions of the standardized approach recommended by the International Zinc Nutrition Consultative Group (IZiNCG): 4,9,10 1) The country-specific average daily per capita availabilities (kcal/capita/day) of foods were obtained from food balance sheets. 11 2) The total zinc and phytate contents of the daily food supply were estimated by using the food composition database of the World Food System International Mini-list. 12 3) The physiological requirements for zinc were calculated based on the age and sex distribution of the population of each country. 4 4) The total population for each Latin American and Caribbean country was obtained from the Institute for Health Metrics and Evaluation (IHME), University of Washington. 13 5) The percentage of the mean physiological requirement for zinc that is available in the national food supply was calculated by dividing the estimated absorbable zinc content of the national food supply by the national physiological requirements. 4,9,10 6) The prevalence of inadequate zinc intake was estimated assuming a 25% interindividual coefficient of variation (CV). This CV was based on existing data for which the intake distribution variability had been determined. 14–16 The estimated prevalence rates of inadequate zinc intake were categorized as low (< 15%), moderate (15% to 25%), or high (> 25%). 8
Prevalence of Stunting
Stunting data (length- or height-for-age z-score < 2 SD) were identified using the latest World Health Organization (WHO) child growth standards. 17,18 The prevalence of stunting was categorized as low (< 20%), medium (20% to 29%), high (30% to 39%), or very high (≥ 40%) according to the WHO classification. 19,20
Risk of Zinc Deficiency per Country
Each individual country was classified into one of four categories of risk of zinc deficiency according to a composite index suggested by Wessells et al. 10 This indicator was based on integrating both the estimated prevalence of inadequate zinc intake and the prevalence of stunting, with a score of 1 representing the highest risk of zinc deficiency and 4 the lowest risk. A score of 1 corresponded to an estimated prevalence of inadequate zinc intake > 25% and a prevalence of stunting > 20%; a score of 2 corresponded to an estimated prevalence of inadequate zinc intake < 25% and a prevalence of stunting > 20%; a score of 3 corresponded to an estimated prevalence of inadequate zinc intake > 25% and a prevalence of stunting < 20%; a score of 4 corresponded to an estimated prevalence of inadequate zinc intake < 25% and a prevalence of stunting < 20%.
Statistical Analyses
Prevalence data were reported as percentages and confidence intervals. In those countries with two available national surveys or representative studies. A chi-squared test was used to compare discriminant data. The estimated prevalence of inadequate zinc intake was correlated with the prevalence of stunting by country using the Spearman correlation coefficient. Statistical analyses were conducted and the figures were plotted using the R programming language, version 3.1.0. 21 A p value < .05 was considered to indicate statistical significance.
Results
Prevalence of Zinc Deficiency in Latin America and the Caribbean
A total of 506 articles were initially identified, of which 47 were excluded because of duplication. After review of the titles and abstracts, 395 studies were excluded because the information was not relevant to the purpose of the review, leaving the number of selected studies at 67. After a detailed review, the final number of selected studies was 6. National data were available from five countries (Argentina, Colombia, Ecuador, Guatemala, and Mexico). 22–27 Serum zinc was assessed in all surveys by using atomic absorption spectrophotometry. The prevalence of low serum zinc was based on two cut points: < 65 μg/dL in Mexico, Colombia, and Ecuador 23,24,26,27 and < 70 μg/dL in Guatemala. 22 Four countries (Mexico, Guatemala, Colombia, and Ecuador) reported biochemical data for children under 6 years of age, and two countries (Mexico and Ecuador) also presented information on women of childbearing age. Only one country (Argentina) had information on national dietary intake. 25
Overall reported data indicate a high prevalence of zinc deficiency in children under 6 years of age (Figure 1). In Colombia, the 2010 national survey showed that the prevalence of zinc deficiency varied with ethnicity (56.3% in indigenous and 42.1% in nonindigenous people) and geographic area (47.8% in rural and 41.4% in urban areas). 23 Similarly, in Guatemala, the prevalence of zinc deficiency was higher in indigenous than in nonindigenous children (41.2% vs. 29.8%) and in children from rural areas than in children from urban areas (41.8% vs. 24.8%). 22 In Ecuador, the prevalence of zinc deficiency was slightly higher in indigenous children than in mestizos and those of other ethnicities (32.4% vs. 29%). 24 In Mexico, the prevalence of zinc deficiency varied mildly by age, with rates of 29.2%, 27.5%, and 26.4% for children 1 to 2, 3 to 4, and 5 to 6 years of age, respectively. 26 Mexican and Ecuadorian women 12 to 49 years of age also had high rates of zinc deficiency (28% and 56%, respectively). 24,27
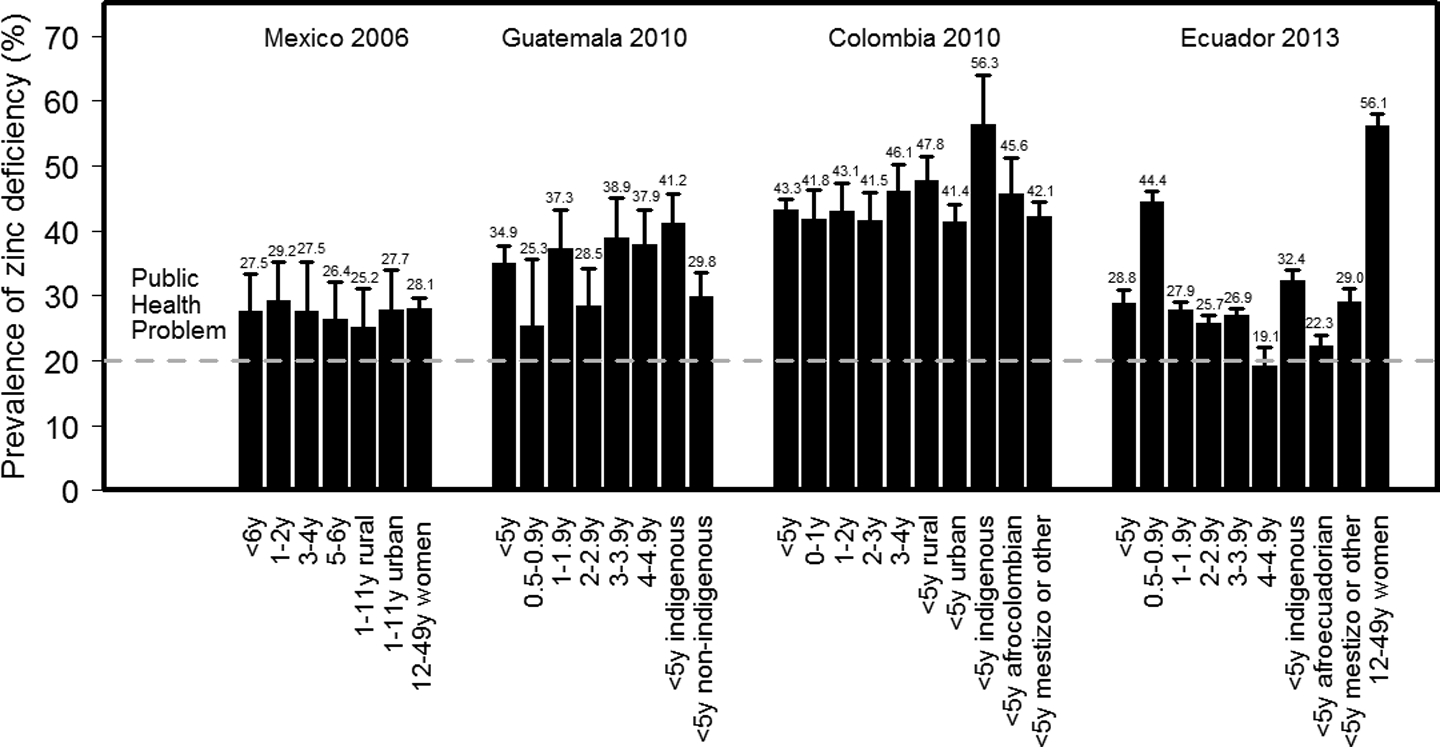
Prevalence of zinc deficiency in Latin America and the Caribbean.
Mexico and Colombia have conducted two consecutive national surveys that collected information on serum zinc concentrations. In Mexican children between 6 months and 11 years of age, the prevalence of zinc deficiency was 25.3% (95% CI, 22.8% to 27.8%) in 1999 and 26.6% (95% CI, 21.2% to 32.6%) in 2006 (p = .51). 26,28 In Colombia, children under 6 years of age had a prevalence of zinc deficiency of 26.9% (95% CI, 23.8% to 30.1%) in 2005, which increased to 43.3% (95% CI, 41.2% to 45.4%) in 2010 (p < .001). 23,29
The only country with available national data on dietary intake of zinc (by 24-hour recall) was Argentina. Argentinian children between 6 and 23 months of age had an average intake of approximately 5.7 mg/day (11.6% [95% CI, 10.4% to 12.9%] under the EAR), while in children between 2 and 5 years of age, the average intake of zinc was approximately 8.5 mg/day (4.2% [95% CI, 3.9% to 5.0%] under the EAR). 25
Estimated Inadequate Zinc Intake
Most countries in Latin America and the Caribbean had a high prevalence (> 25%) of inadequate zinc intake, including Colombia, Brazil, Venezuela, Uruguay, Belize, Haiti, Suriname, Honduras, Grenada, Nicaragua, Peru, El Salvador, Panama, Paraguay, Guatemala, Bolivia, Dominica, Saint Vincent and the Grenadines, Guyana, Bahamas, Saint Lucia, Saint Kitts and Nevis, Netherlands Antilles, Antigua and Barbuda, and Barbados (Table 1 and Figure 2A). Cuba, Mexico, Chile, Ecuador, Jamaica, and Trinidad and Tobago had a moderate estimated prevalence of inadequate zinc intake (15% to 25%), while Costa Rica, Argentina, and the Dominican Republic had a low prevalence (< 15%).
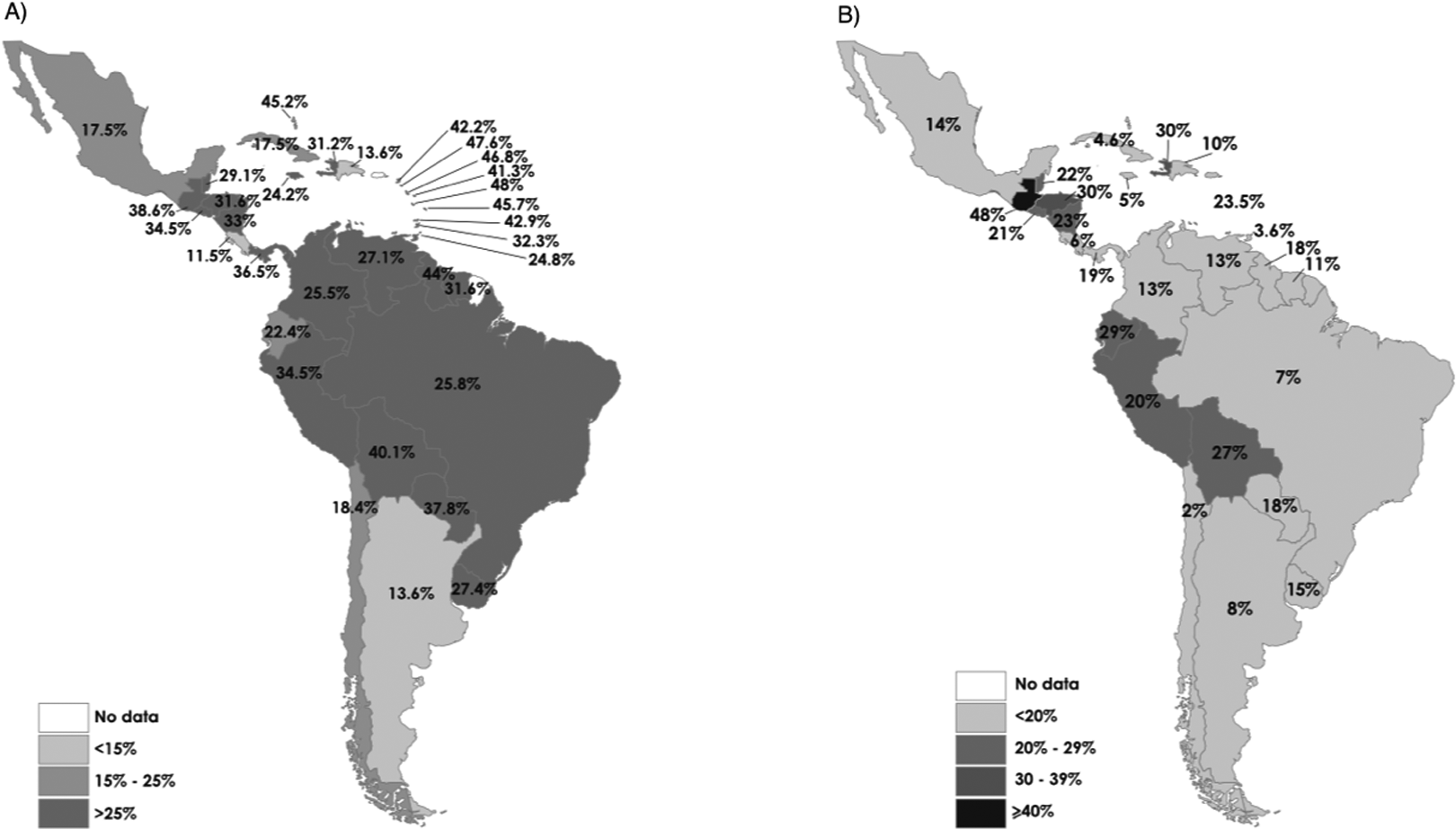
(A) Map of risk category of estimated percentage of population with inadequate zinc intake. (B) Map of prevalence of stunting in Latin America and the Caribbean.
Estimated Prevalence of Inadequate Zinc Supply Based on National Food Sheet Data in Latin America and the Caribbean in 2011.
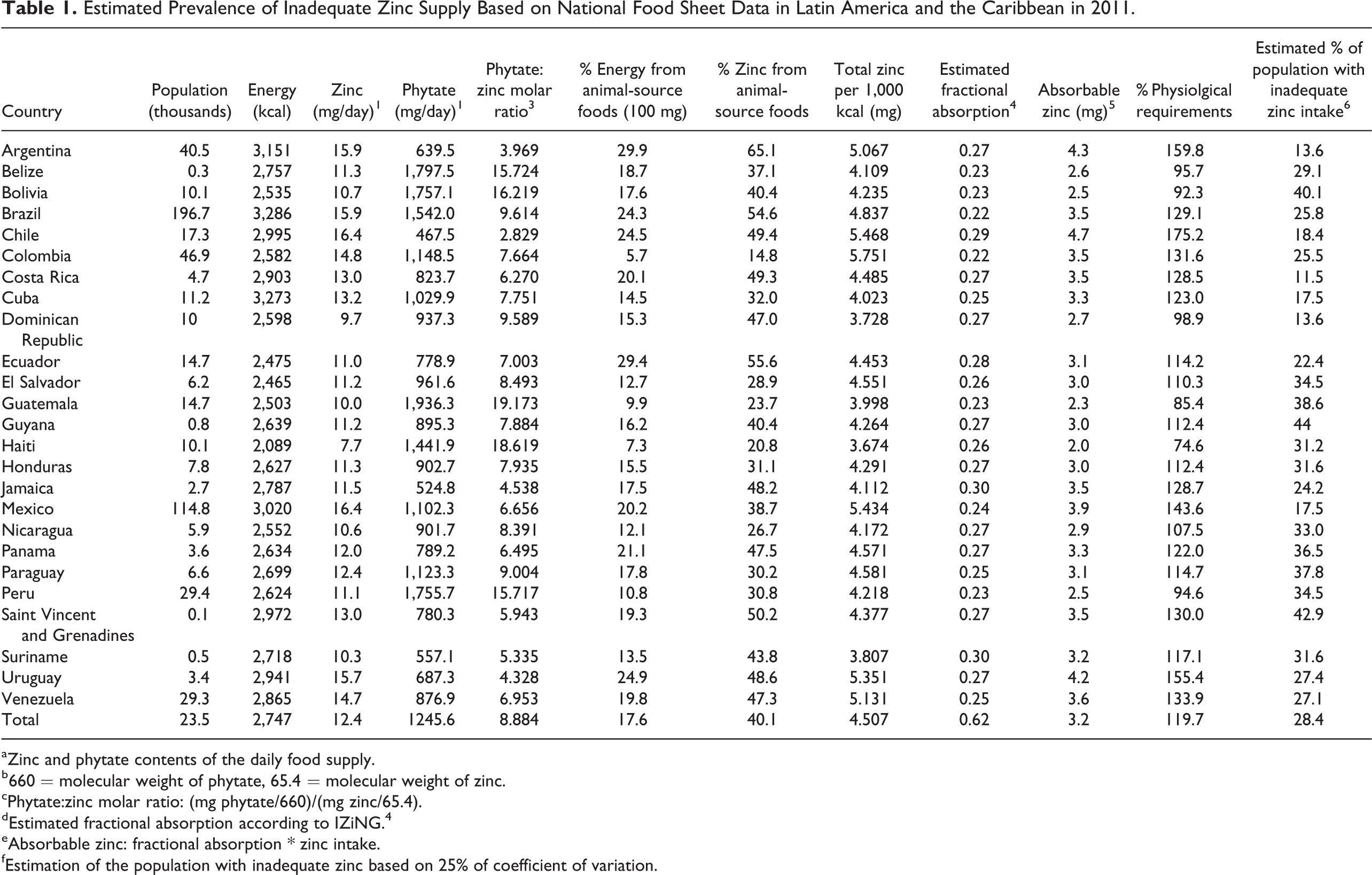
aZinc and phytate contents of the daily food supply.
b660 = molecular weight of phytate, 65.4 = molecular weight of zinc.
cPhytate:zinc molar ratio: (mg phytate/660)/(mg zinc/65.4).
dEstimated fractional absorption according to IZiNG. 4
eAbsorbable zinc: fractional absorption * zinc intake.
fEstimation of the population with inadequate zinc based on 25% of coefficient of variation.
Prevalence of Stunting
Haiti and Honduras had a high prevalence (30% to 39%) and Guatemala a very high prevalence (≥ 40%) of stunting (Figure 2B). Peru, El Salvador, Belize, Nicaragua, Saint Vincent and the Grenadines, Bolivia, and Ecuador had a medium prevalence of stunting (20% to 29%). Chile, Trinidad and Tobago, Cuba, Jamaica, Costa Rica, Brazil, Argentina, the Dominican Republic, Suriname, Venezuela, Mexico, Uruguay, Guyana, Paraguay, and Panama had a low prevalence of stunting (< 20%). A direct correlation (r = 0.64, p < .001) was found between the estimated prevalence rates of inadequate zinc intake and stunting using information across 25 countries with matching data (Figure 3).
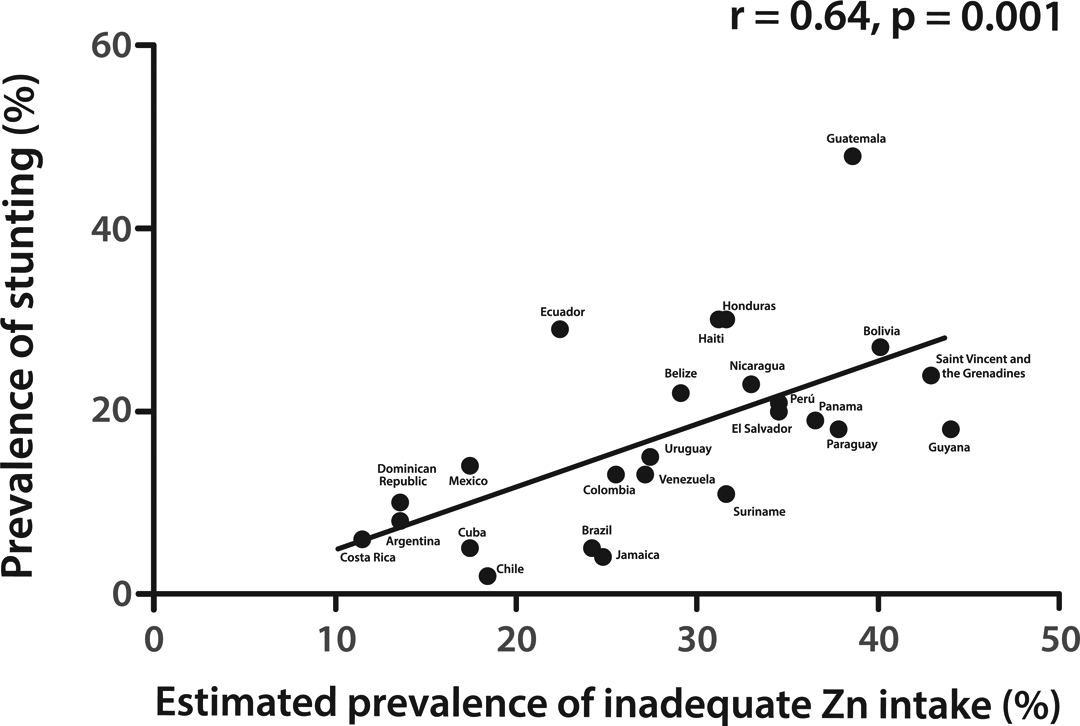
Correlation between estimated prevalence of inadequate zinc intake and prevalence of stunting in Latin America and the Caribbean.
Risk of Zinc Deficiency per Country
The countries with the highest risk of zinc deficiency (estimated prevalence of inadequate zinc intake > 25% plus a prevalence of stunting > 20%) were Belize, Bolivia, El Salvador, Guatemala, Haiti, Honduras, Nicaragua, and Saint Vincent and the Grenadines. Ecuador was the only country with an estimated prevalence of inadequate zinc intake ≤ 25% together with a prevalence of stunting > 20%. The countries with an estimated prevalence of inadequate zinc intake > 25% and a prevalence of stunting ≤ 20% were Brazil, Colombia, Guyana, Panama, Paraguay, Peru, Suriname, Uruguay, and Venezuela. The countries with a low risk of zinc deficiency (estimated prevalence of inadequate zinc intake ≤ 25% together with a prevalence of stunting ≤ 20%) were Mexico, Jamaica, the Dominican Republic, Cuba, Costa Rica, Chile, and Argentina.
Discussion
The objective of this review was to estimate the magnitude of zinc deficiency in Latin America and the Caribbean based on the prevalence of low serum zinc concentrations or dietary intake assessed at the national level. Stunting prevalence and the risk of zinc deficiency were also assessed. We found that since 2000 only four countries in Latin America and the Caribbean (Mexico, Guatemala, Colombia, and Ecuador) have included the assessment of zinc status in nationally representative surveys. Overall, these countries reported a high prevalence of zinc deficiency in children under 6 years of age. Mexico and Ecuador also evaluated the zinc status of girls and women 12 to 49 years of age and found a high prevalence of zinc deficiency in this population. Based on biochemical analyses, the information suggests that zinc deficiency is a public health problem in countries for which data are available.
Mexico and Colombia have been active in evaluating and implementing strategies to alleviate zinc deficiency. Both countries have conducted two consecutive national surveys and implemented interventions at the national level. Programs in Mexico, such as Liconsa and Oportunidades, which distribute milk fortified with 11.5 mg of zinc/100 g to preschoolers, have been shown to be effective in increasing serum zinc concentrations and reducing the prevalence of zinc deficiency (from approximately 1% to 10%). 30 In addition, the fortified complementary food Nutrisano has been shown to be effective in improving serum zinc in zinc-deficient children (p < .05). 31 The Ministry of Health in Mexico has distributed zinc-fortified (20 mg zinc/kg) corn and wheat flours since 1999 32 , with both flours having high stability and acceptability by the population. 33 In Colombia, a national program using the fortified complementary food Bienestarina based on cereal flour with 8.3 mg of zinc/100 mg was implemented in 1976. 34 Despite these efforts, zinc deficiency, as determined by consecutive surveys, remains high in children under 6 years of age in both countries.
A common feature in Latin America and Caribbean countries with available data on zinc status is that the prevalence of zinc deficiency is higher among disadvantaged and vulnerable groups, such as indigenous populations in Guatemala, Colombia, and Ecuador. This situation may be explained in part by the usual diet of these groups, which is characterized by a low supply of or access to zinc-rich foods (meat) and a high intake of inhibitors of zinc absorption (phytate). 35 Furthermore, these groups are usually exposed to infection, inflammation, and an elevated incidence and duration of acute and persistent diarrhea, which can result in a high loss of zinc in the feces. 36–38 The prevalence of zinc deficiency is also higher among rural than urban children. Presumably, these demographic differences overlap because the vast majority of indigenous people live in rural locations. The higher prevalence of zinc deficiency in these groups may also be partly explained by cultural differences, given that indigenous people have their own distinct languages and social and political institutions that differ from those of mainstream society, which may lead to problems of supply, distribution, and stock points in the delivery, storage, and coverage of foods or supplements containing zinc delivered by national programs implemented by governments. 39
Because of the small amount of biochemical data available, we proceeded to estimate the risk of zinc deficiency using indirect indicators (inadequate zinc intake and stunting). According to our study, the estimated average prevalence of inadequate zinc intake in Latin America and Caribbean countries was 28% (95% CI, 11.5% to 44%), and most countries were classified as being at high risk. These high figures for the risk of zinc inadequacy are consistent with data estimated by IZiNCG in 2004, which suggest that the amount of absorbable zinc currently available from the food supply in Latin American and Caribbean countries is still insufficient to reach the physiological requirements for most individuals. In 2004, the median percentage of the EAR consumed was 22.6% (IQR, 11.5% to 45%); in 2011, the median percentage of the EAR consumed was 28.2% (IQR, 22.4% to 34.5%) (p = .15). 4 A direct correlation was found between the estimated prevalence of inadequate zinc intake and the prevalence of stunting in children under 5 years of age (r = 0.64, p < .001). A similar correlation was reported by IZiNCG for 2004 (r = 0.61, p < .001) 4 and in a global analysis of zinc status for the period from 2003 to 2007 in 138 low- and middle-income countries (r = 0.48, p < .001). 10 These studies were conducted mostly in vulnerable populations that may have higher rates of dietary inadequacy and poor linear growth.
On average, 17% (range, 2% to 48%) of children under 5 years of age in Latin America and the Caribbean were stunted. Based on this review, the countries with the highest risk of zinc deficiency (estimated prevalence of inadequate zinc intake > 25% and prevalence of stunting > 20%) were Belize, Bolivia, El Salvador, Guatemala, Haiti, Honduras, Nicaragua, Saint Vincent, and the Grenadines. 8,10 These countries should be prioritized for biochemical and dietary assessments of population zinc status and for implementation of intervention strategies. Costa Rica and Argentina had the lowest risk of zinc deficiency.
The magnitude of zinc deficiency is difficult to evaluate because of the lack of functional and clinical indicators as well as the limited number of biomarkers currently available to assess zinc status in populations. 40 Few studies incorporating biochemical analyses of serum zinc were available from Latin America and the Caribbean. Although serum zinc has limitations, including low sensitivity, specificity, and predictive value for individuals, it is the most commonly used biomarker for assessing zinc status in large populations. 6 Most of the available studies have been conducted in samples with low representativeness, which substantially limits comparisons across countries. Our description of zinc deficiency was based on multiple prevalence points, without assessments or predictions over time. The influence of inflammation on zinc status cannot be assessed due to a lack of inflammatory markers in the available surveys. The estimation of the risk of zinc inadequacy was based on calculations from dietary surveys not applied individually; instead we used national food balance sheets based on estimations of the supply of food per capita. Stunting is not a specific condition for zinc deficiency, and the composite index to classify the risk of zinc inadequacy in countries does not provide a true indication of the real magnitude of zinc deficiency. Although these limitations exist, this is the first review aiming to estimate the magnitude of zinc deficiency in Latin America and the Caribbean, prioritizing biochemical analyses and secondarily utilizing the estimation of the risk of zinc inadequacy. This review aims to identify the countries most afflicted by zinc deficiency in order to implement cost-effective strategies focused on improving zinc status, especially in groups at higher risk for zinc deficiency.
Conclusions
Few countries in Latin America and the Caribbean have representative data on zinc status based on biochemical assessment. Results from the four available national surveys indicate a high prevalence of zinc deficiency in children under 6 years of age and women 12 to 49 years of age. High rates of both the estimated inadequate dietary intake of zinc and stunting were also reported from most Latin America and Caribbean countries. Overall, based on available data on dietary intake and stunting, zinc deficiency appears to be a public health problem in some countries of Latin America and the Caribbean, with numerous other countries in the region being at risk for inadequacy.
Footnotes
Acknowledgments
We are grateful to Gina Bautista and Francisca Villagran for their support in data collection, and we thank Dr. Kenneth H. Brown for providing input in the design of the study.
Authors’ Contributions
Gustavo Cediel, Manuel Olivares, Alex Brito, and Daniel López de Romaña designed the study; all authors interpreted the data and helped to prepare the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Gustavo Cediel, Manuel Olivares, Alex Brito, and Daniel López de Romaña declare no potential conflicts of interest. Hétor Cori is Nutrition Science Director in Latin America for DSM Nutritional Products.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received financial support for the research and publication by DSM Nutritional Products.