
Abstract
Introduction:
Oraon tribes of India have high levels of undernutrition. Dietary diversification is one of the food-based interventions to ameliorate malnutrition.
Objectives:
This study assessed the awareness and availability of indigenous foods and estimated dietary intakes and nutritional status with emphasis on indigenous food consumption among women in the Oraon tribal community in Jharkhand, India.
Design:
A cross-sectional study with a longitudinal component on dietary intake assessment to capture seasonality.
Setting:
Selected villages in Raidih block of Gumla district of Jharkhand.
Participants:
Reproductive-age Oraon tribal women (N =143).
Methods:
Household and dietary surveys were conducted. A 24-hour dietary recall for 2 consecutive days (repeat surveys in 2 other seasons) and food frequency questionnaire were adminsitered on 1 woman per household. Anthropometric assessments were also carried out.
Outcomes:
Socioeconomic status, awareness about indigenous foods, dietary intake pattern, and contribution of indigenous food to nutrient intake of Oraon tribal women in the reproductive age-group.
Results:
Comprehensive awareness about indigenous food resources was present. However, household food security and actual intake of indigenous foods were low. Higher intake of key micronutrients, calcium and iron, was observed among those who consumed indigenous foods. About 40% of the woman had various degrees of chronic energy deficiency.
Conclusion:
Despite rich knowledge, nutrient-rich indigenous food resources remain underutilized in the Oraon tribal community of Jharkhand, India. Identifying strategies to promote dietary diversity via optimum indigenous food intake could contribute to both food and nutrition security.
Introduction
A “triple burden” of malnutrition, that is, undernourishment, micronutrient deficiencies, and obesity, a characteristic of the epidemiological impact of nutrition transition, threatens to overwhelm developing countries of the world. 1,2 Micronutrient deficiencies, often referred to as hidden hunger, coexist with undernourishment and overnutrition. 2 Therefore, integrated and complementary actions and interventions are needed to improve nutritional status by increasing the availability of, access to, and consumption of a nutritionally adequate diet from a variety of foods (note 1).
Dietary diversity, that is, consumption of a wide variety of foods, has been identified as one of the food-based interventions to ameliorate the many-faceted burden of malnutrition. In fact, it has been included as one of the indicators apart from wasting, stunting, micronutrient deficiencies, and obesity rates for tracking the trends of this triple burden of malnutrition. 3 Indigenous and tribal people are descended from populations who inhabited a country or geographical region at the time of conquest, colonization, or establishment of present state boundaries and have their own cultures, languages, customs, and institutions. In addition to that and importantly, they retain knowledge of the land and food resources rooted in historical continuity within their region of residence. These food resources that are often referred to as indigenous foods are documented as having high nutritive value when compared to nonnative varieties. 4,5 Although the contribution of indigenous foods varies seasonally and is affected by unexpected climatic changes, 6 these foods add diversity to local food systems and are important for household (HH) food security, nutrition, and income generation (notes 2 and 3). 7 If these foods are familiar and accessible to the indigenous communities, their use can be incorporated as an effective food-based strategy to increase dietary diversity and ameliorate nutrient deficiencies in these communities. 8
Among various African and Asian indigenous communities, cultivated and wild indigenous food sources fulfill HH food requirements significantly and contribute substantially to vitamin and mineral intakes. 9,10,11 In fact, close to 90% of the most widespread and flourishing weeds in the world are edible, and many of these species have a high nutritional value and medicinal properties. 4,12 Studies from India have also documented the nutritive value of various indigenous foods, while some have recommended cultivation of wild species in backyard gardens to meet the nutritional requirements of the communities. 13,14
Despite advancements in poverty and malnutrition reduction, the indigenous communities of India, composed mainly of tribes residing in their place of origin, have a disproportionately high level of undernutrition, specifically maternal and child undernutrition and child mortality. 15 A fourth of the total population of Jharkhand, a state in the central eastern part of India, is composed of the scheduled tribes (STs). Of 30 STs notified for the state, Oraon are the second most populous tribe. 16 Studies on anthropometric and nutritional parameters of Oraon groups reveal that a significant section of the population has undernutrition, 17,18 which is present amidst a rich and diverse natural food environment. Studies have further documented various species of edible weeds and other indigenous foods from agricultural and nonagricultural fields which form a routine supplement to staple diets of this community. 13,19 However, there is a need to analyze and document the nutritive value of these foods and quantify their intakes, acceptability, and availability to create an evidence base for promoting their optimal production and consumption.
There are multiple underlying causes behind high prevalence of undernutrition in these communities, and underutilization of its rich biodiversity could be one of them. This rich biodiversity and its expression in the form of diverse indigenous food sources could be leveraged for improving their nutritional status. Further, additional information on the nutritive value of indigenous foods, estimates of their contribution to nutrient intake, and their impact on the nutritional status of community members would be instrumental in preparing strategies for improving awareness and optimizing intake.
The findings presented in this article are from a substudy of a larger project that investigated the nutrient composition of commonly consumed indigenous foods in the tribal communities of Jharkhand. The project also documented the contribution of these foods to the diet and nutritional status of women and children of the study communities. The data in the present article reflect our findings on the contribution of indigenous foods to nutrient intake and nutritional status of women in Oraon tribal community of Jharkhand.
Materials and Methods
Study Area
The study was conducted in selected villages of Gumla district of Jharkhand, which are inhabited by the Oraon tribal community.
Study Design
This was a cross-sectional study with a longitudinal component on dietary intake assessment to account for seasonal variation.
Study Period
Data were collected in 3 seasons: winter, summer, and monsoon. In January 2014 (winter season), a detailed HH and dietary survey was conducted along with qualitative enquiries. In addition to that, a 24-hour dietary recall (24-hour DR) for 2 consecutive days on 1 woman in the reproductive age-group per HH was also conducted. One-third of the same women were followed up in May 2014 (summer season), and July 2014 (monsoon season), and a 24-hour DR was conducted.
This study was conducted according to guidelines laid down in Declaration of Helsinki, and all procedures involving humans were approved by the Institutional Ethics Committee of the Public Health Foundation of India. Informed consent was obtained from all the adult participants in the study by the data collection team; those who were literate gave signed consent forms. Verbal consents were documented in the presence of a third-party witness.
Sample Size Calculation
In order to capture chronic energy deficiency (CED; body mass index [BMI] <18.5) among women in the study community, the objective of the sampling was set to expect at least 40% prevalence of CED. With an α level of 5%, design effect of 1.5, and an error range of ±10% with 95% confidence, a sample size of 140 was arrived at. Details on sample size calculation can be accessed elsewhere. 20
Sampling Framework
A block (subdivision of a district in a state) with high concentration of Oraon community was chosen in Gumla district of Jharkhand, and 143 HHs were selected. A total of 4 villages were identified using Probability Proportional to Size 21 sampling, and at least 35 HHs were selected from each village. The HHs surveyed were those with at least 1 child under the age of 5 years (U5), as the main study aimed to assess both maternal and child undernutrition. The detailed methodology is explained elsewhere. 20 For conducting 24-hour DR and anthropometric assessment in each HH, 1 woman in the reproductive age-group per HH was selected using the Kish selection table (a method for randomly selecting members within a HH to be interviewed). 22
Data Collection
In order to elicit information on HH socioeconomic and demographic profile and food consumption patterns with emphasis on procurement and intake of indigenous food, an interviewer-administered questionnaire pretested in 2 Oraon villages was used. The HH food security was also assessed using a validated HH food security assessment tool. 23,24 A 24-hour DR was taken for 1 woman in the reproductive age-group per HH for 2 consecutive days and in 3 seasons as described previously. The frequency of consumption of different food items under various groups was assessed using a food frequency questionnaire (FFQ). Presurvey visits and qualitative enquiries through key informant interviews and focus group discussions (FGDs) were conducted to capture the variety of foods consumed by the Oraon community and their knowledge of the nutritional and medicinal properties of these items. 19 Food items identified during the FGDs were extensively used to develop the FFQ. The FFQ list included both commonly consumed Indian food items and indigenous tribal foods. We developed and pretested a 244-item Oraon FFQ. This FFQ was administered during the survey conducted in the winter season with a reference period of 1 month. Anthropometric assessments were carried out using standard protocols and equipment (weighing scale and anthropometer rod) to measure BMI on the same woman from whom DRs were taken. The details of the data collection process are available elsewhere. 20
All the study tools were translated by a native speaker into the local language (Sahadri) and back-translated into English to check for fidelity, accuracy, and consistency. The tools were in the native language and were administered by the local field workers who were well versed in the local language/dialect. The study team accompanied and supported them in eliciting accurate information from the study participants.
Data Analysis
Dietary intake data from the 24-hour DR were entered into a validated software “DietCal” (version 3.0; Profound Tech Solution, web site: http://dietcal.in/; note 4) which is based on values from Nutritive Value of Indian Foods. 25 Samples of the indigenous foods for which nutritive values were not available were analyzed in the laboratory to estimate their nutrient content. 19 Nutrient intake data (as represented by mean) were then compared with Recommended Dietary Allowance (RDA) for Indians for a moderately active adult woman. 26 The adequacy of nutrient intake by each participant was computed in terms of Nutrient Adequacy Ratio (NAR). 27
For the HH food security scores, the sum of affirmative responses to the 6 questions in the HH food security form provided the HH’s raw score on the scale. BMI was calculated as weight (kg) divided by height (in m2). The women were classified as being underweight and as having CED or not using the standard BMI cutoffs. 28
STATA 13 (StataCorp, College Station, Texas) was used for statistical analysis. Continuous variables were summarized using parametric or nonparametric measures of central tendency, for example, mean ± standard deviation or as median and interquartile range. The categorical variables were summarized as number of participants and percentages.
Women were categorized into 2 groups: indigenous food consumer versus nonconsumer. This was based on consumption of at least 1 indigenous food during the 24-hour DR period. This was used to compare nutrient intake in the 2 groups. Similarly, the nutritional status of women was compared between the consumer and nonconsumer groups. The t test or Wilcoxon rank sum test and chi-square test were used to compare the differences in distribution of continuous and categorical variables, respectively. Difference in indigenous food consumption between the 3 seasons (winter, rainy, and summer) was assessed using Cochran’s Q test. The level of statistical significance was set at P < .05 for 2-sided tests.
Results
For the HH and dietary survey, 34 to 38 HHs each, belonging to Oraon tribal community, in 4 villages of Nawagarh, Birkera, Katkaya, and Raghunathpur in the Raidih block of Gumla district of Jharkhand, were covered. Table 1 provides the socioeconomic and demographic profile of the HHs interviewed. Adult women comprised 27% of the population (n = 887). The mean age of women in the reproductive age-group (15-49 years) was 29.1 ± 6.5. Households with very low food security constituted 24.5%. Around 52% of the study community possessed a ration card which is needed to avail benefits of the Public Distribution System, a government program addressing food security for socioeconomically disadvantaged HHs or those belonging to various grades of poverty; the card is thus an indicator of access to food security programs.
Socioeconomic and Demographic Profile of the Households.a,c
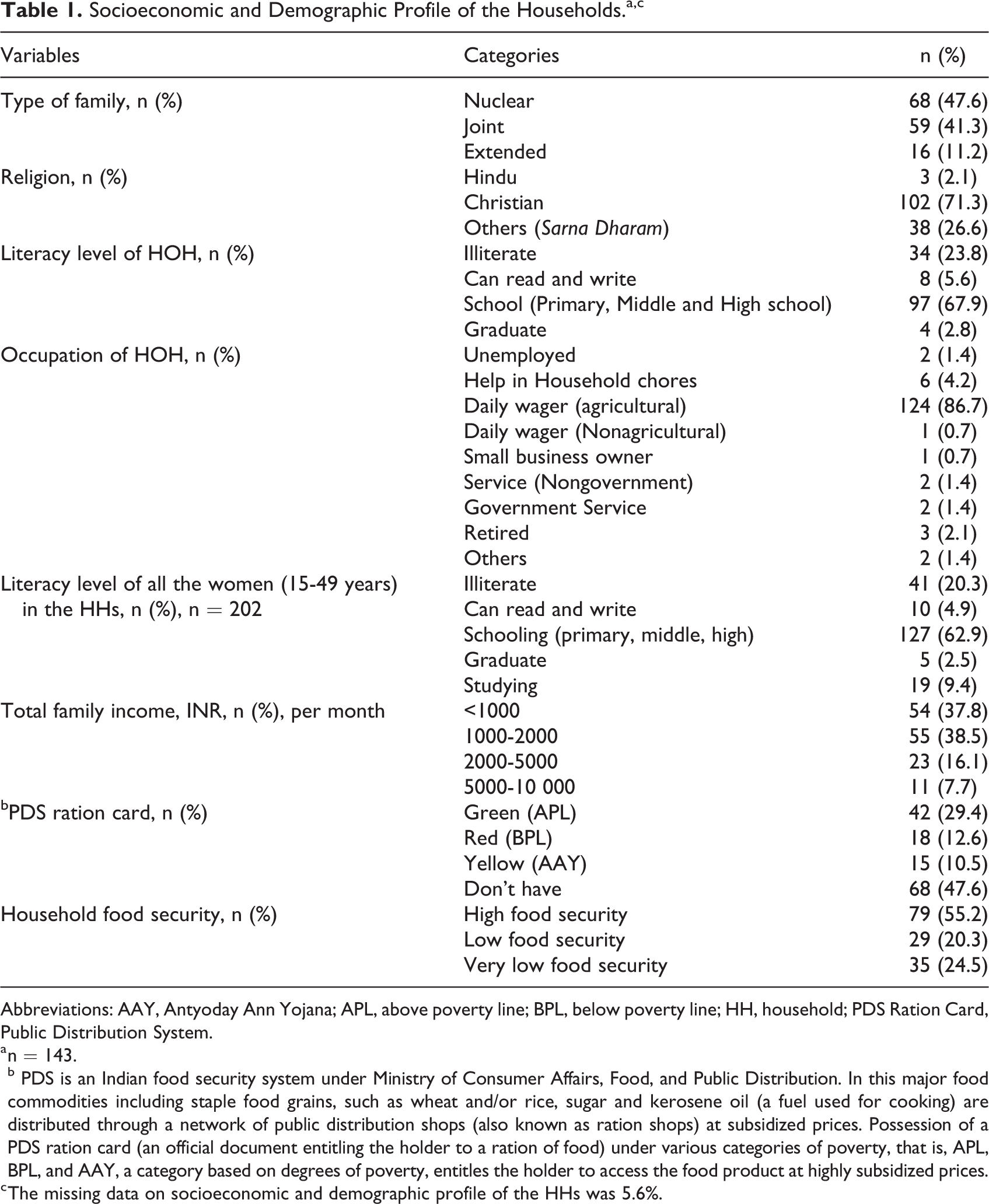
Abbreviations: AAY, Antyoday Ann Yojana; APL, above poverty line; BPL, below poverty line; HH, household; PDS Ration Card, Public Distribution System.
a n = 143. b PDS is an Indian food security system under Ministry of Consumer Affairs, Food, and Public Distribution. In this major food commodities including staple food grains, such as wheat and/or rice, sugar and kerosene oil (a fuel used for cooking) are distributed through a network of public distribution shops (also known as ration shops) at subsidized prices. Possession of a PDS ration card (an official document entitling the holder to a ration of food) under various categories of poverty, that is, APL, BPL, and AAY, a category based on degrees of poverty, entitles the holder to access the food product at highly subsidized prices.
c The missing data on socioeconomic and demographic profile of the HHs was 5.6%.
Cultivation of Food or Use of Livestock for HH Consumption
Oraon communities are agriculturist. A majority of HHs had agricultural land (95.8%) and backyard gardens (67.1%), and around half of them were using agricultural produce (52.6%) and produce from garden such as fruits and vegetables (45.8%) for HH consumption. A majority (88.1%) of HH owned livestock such as goats, sheep, cattle, poultry, and pigs, and three-fourths (76.2%) of them used these for HH consumption. A majority (79.7%) of HH reported collecting 50% of their daily requirement for food from the homegrown foods and nearby forests. Mean monthly expenditure on food items such as sugar, oil, and so on, was INR 1054.5 ± 894.2 (range: 200-6000 INR).
Awareness About Indigenous Foods Among the Oraon HHs
Since identification and consumption of indigenous foods were the key focus of the main study, detailed investigations about the indigenous foods were carried out in the study population. All the respondents (100%) reported awareness about indigenous varieties of green leafy vegetables (GLVs) and their consumption during some months or throughout the year. Other indigenous food items from different food groups such as cereals, roots and tubers, other vegetables, mushrooms, fruits, meats and fish, oil, and alcoholic drinks were also reported. Supplemental Table S1 provides a list of the indigenous foods reported.
About three-fourths of the HHs reported consumption of GLVs, meats, vegetables, pulses, and fruits by everyone in the family at any point of time in the year. Majority (95.1%) of the HHs reported storing and preserving specific indigenous foods for consumption during lean periods and throughout the year. These included GLVs such as Phutkal, Saarla, Chakod, Chench, Mustard leaves, and Lotni saag that were preserved by sun drying or boiling the GLVs followed by sun drying.
General Dietary Intake Pattern of Adults in the HHs
A majority (90%) of HHs were nonvegetarian. Most (52.4%) of the adults consumed 3 main meals a day. Consumption of in-between meals was not reported by majority (75%) of adults. Those who reported in-between meals consumed a variety of home-cooked and commercially available ready-to-eat foodstuffs such as papad (55.6%), biscuits (61.1%), tea (80%), puffed rice (30.6%), fruit (30.6%), rice flakes (22.2%), sattu ka pani (roasted gram powder mixed with water; 2%), and others (5.6%) such as puri (crackers made with wheat flour) and roti (chapati). A majority (97.9%) of HHs consumed packaged iodized salt. Consumption of alcohol by any member of the family was reported by 93% of the HHs.
Although the community reported awareness about a variety of indigenous foods, a detailed FFQ (244 food items) carried out during the main survey in January 2014 during the winter season revealed low levels of consumption of these foods on a regular basis. A majority (57.3%) of HHs consumed rice as a staple twice daily. The GLVs constituted the other common food item in the habitual diets of Oraon community. Over a third (37.1%) of the population consumed GLVs once a day. About 40% of the HHs also consumed other vegetables twice/day followed by 35.7% who consumed them once/day. Almost half (49.6%) reported consuming flesh foods 1 to 2 times a week in the previous month, and 48.9% reported consumption of fruits 1 to 2 days/week. About 42.7% consumed pulses/legumes 1 to 2 times a week. More than a fourth of the population did not consume milk in the past month. Consumption of mustard oil was reported by majority (65.2%) of the HHs twice a day. Consumption of the indigenous Mahua oil (Dori oil) was reported by only a few (n = 2) HHs during the month of the survey. Sugar consumption was reported by over a quarter (29.6%) of HHs once a day. Various indigenous varieties of alcoholic drinks were reported to be consumed, which included Hadiya, Khajur Taadi and Mahua. More than one-third (34.3%) of HHs reported consuming these alcoholic beverages 3 to 4 times a week.
Nutrient Intake of Women in the Reproductive Age-Group (15 to 49 Years)
During the winter season, the first survey, a 2-day 24-hour DR, was conducted with 1 randomly selected woman per HH (n = 138). One-third of these women (n = 56) were visited again in the summer season and yet again in monsoon season (n = 52) for repeat 2-day 24-hour DR in order to assess the seasonal variability in their dietary intake. Table 2 provides a detailed description of their nutrient intake in the 3 seasons. When the dietary intakes were compared to the Indian RDA of moderately active women, the adequacy of mean calorie and protein intake of the study population was more than 80% in all the seasons. The percentage adequacy for fats and micronutrients such as iron, calcium, folic acid, vitamin A, riboflavin, and B12; fats and micronutrients such as iron, calcium, folic acid, vitamin A, riboflavin, and vitamin B12; and fats and micronutrients such as iron, calcium, folic acid, and B12 were below 60% during the winter (n = 138), summer (n = 56), and monsoon (n = 52) season, respectively. The NAR for iron, calcium, folic acid, vitamin A, thiamine, riboflavin, and vitamin B12; iron, calcium, folic acid, vitamin A, thiamine, riboflavin, and vitamin B12; iron, calcium, folic acid, riboflavin, and vitamin B12 were inadequate in more than 50% of the study population in the winter, summer, and rainy seasons, respectively. There was almost an 8- to 10-fold increase in median intake of vitamin A in rainy season (748 µg/day) as compared to the winter (78 µg/day ) and summer seasons (98 µg/day ).
Nutrient Intake of Women in the Reproductive Age-Group (Mean Nutrient Intake of 138 Women in One Season [Winter] Along With Seasonal Intake of One-Third of Women in 2 More Seasons [Summer (n = 56) Monsoon (n = 52)].a
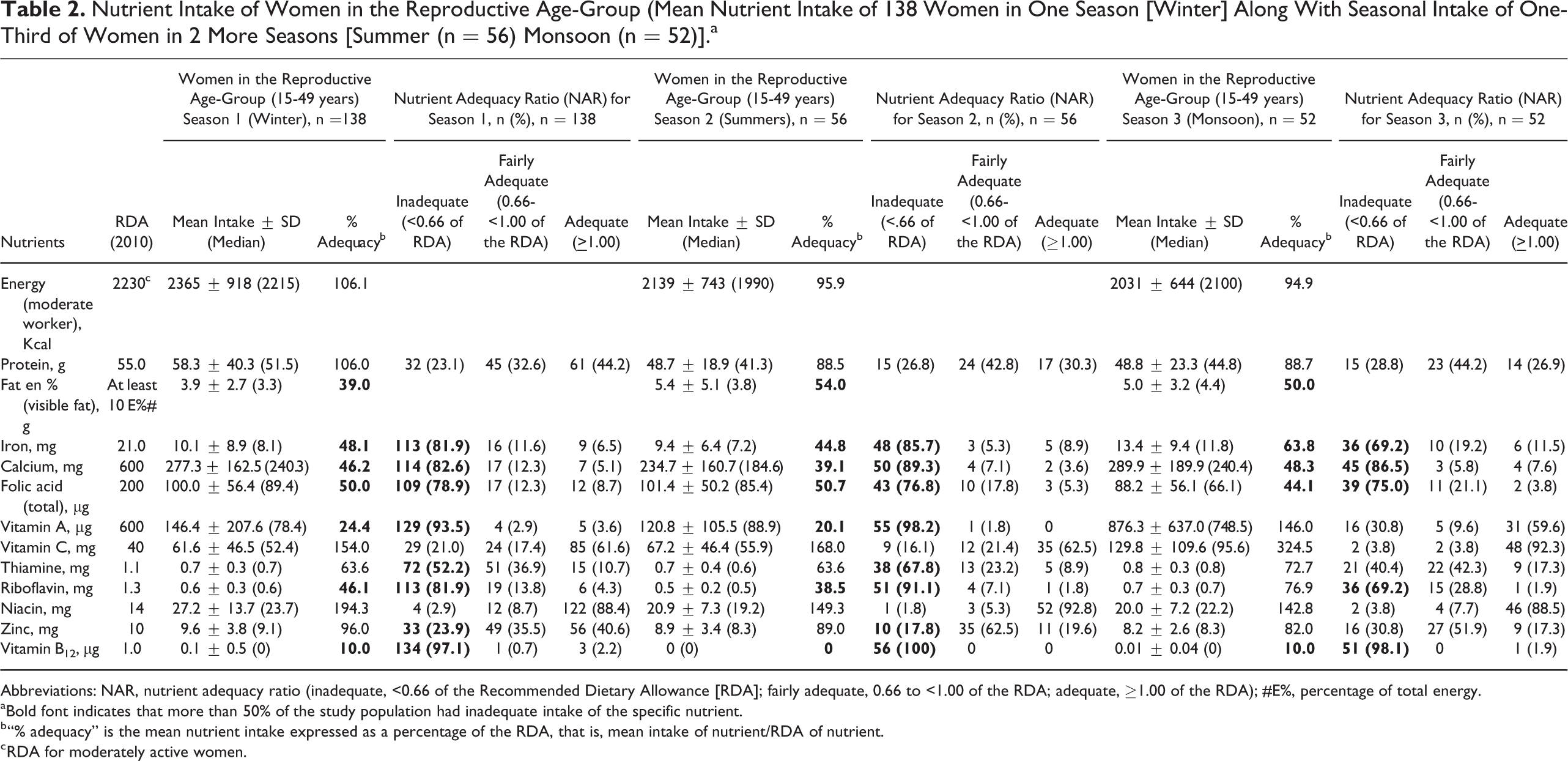
Abbreviations: NAR, nutrient adequacy ratio (inadequate, <0.66 of the Recommended Dietary Allowance [RDA]; fairly adequate, 0.66 to <1.00 of the RDA; adequate, ≥1.00 of the RDA); #E%, percentage of total energy.
a Bold font indicates that more than 50% of the study population had inadequate intake of the specific nutrient.
b “% adequacy” is the mean nutrient intake expressed as a percentage of the RDA, that is, mean intake of nutrient/RDA of nutrient.
c RDA for moderately active women.
Seasonal Variation in Indigenous Food Intake and Nutrient Intake
During the repeat 24-hour DRs, one-fourth of the study women (n = 37) could be followed in all the 3 seasons. The indigenous food consumption measured as at least 1 indigenous food consumed in the past 24 hours was significantly different across the 3 seasons (P = .036). Further, a comparison of median nutrient intake of these women in the 3 seasons (Table 3) showed that the median intake of iron (P < .000), vitamin A (P < .000), vitamin C (P < 0000), thiamine (P = .006), riboflavin (P < .000), and niacin (P = .036) was significantly different in the 3 seasons. The intake of iron, vitamin A, vitamin C, and thiamine was higher in monsoon when compared to winter and summer season.
Seasonal Trends in Nutrient Intake Among Oraon Women.a
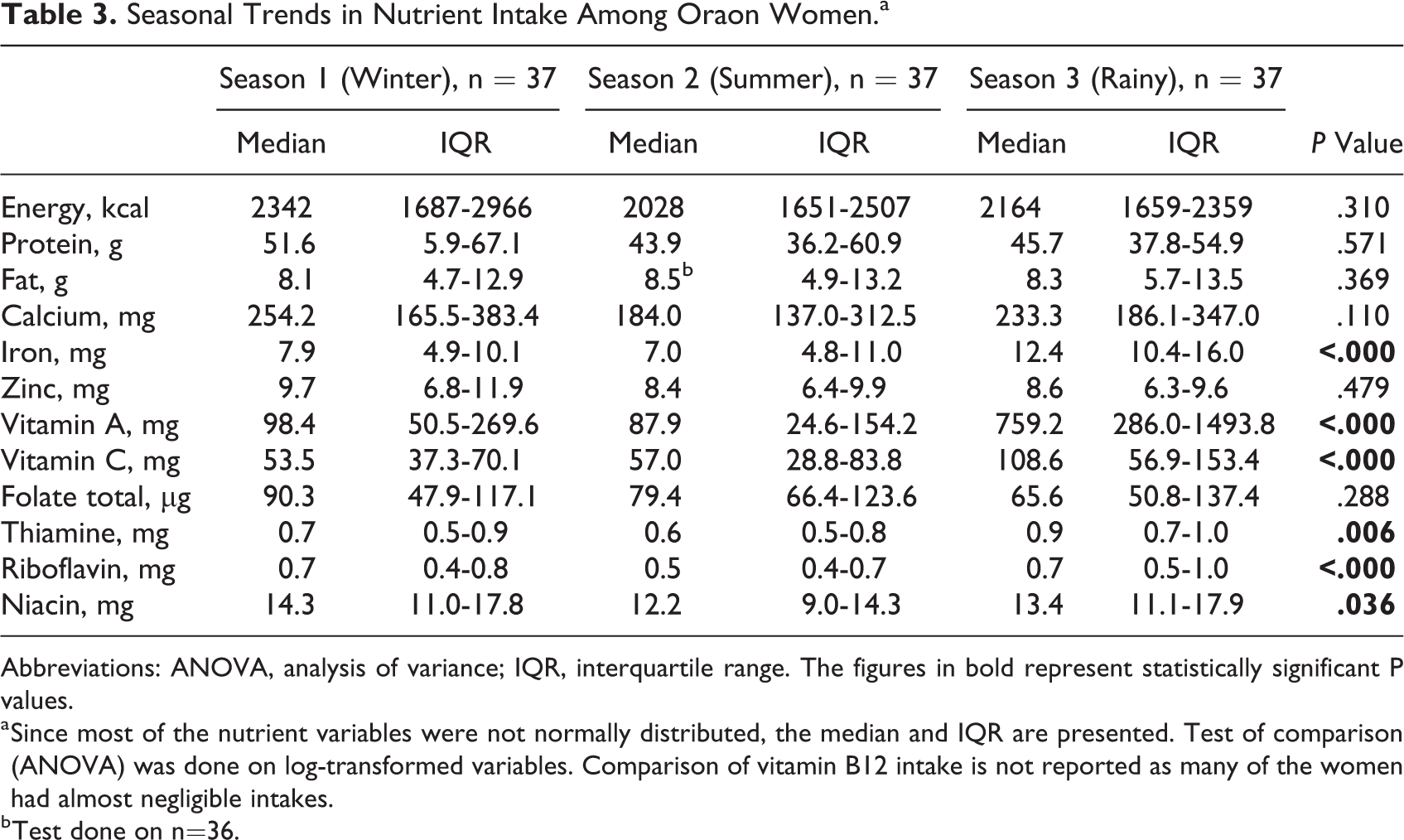
Abbreviations: ANOVA, analysis of variance; IQR, interquartile range. The figures in bold represent statistically significant P values.
a Since most of the nutrient variables were not normally distributed, the median and IQR are presented. Test of comparison (ANOVA) was done on log-transformed variables. Comparison of vitamin B12 intake is not reported as many of the women had almost negligible intakes.
b Test done on n=36.
Contribution of Indigenous Foods to Nutrient Intake
To explore possible contribution of indigenous foods to nutrient intake, we compared the nutrient intake in women who consumed indigenous foods in the past 2 days to the women who did not. This comparison was done on the nutrient intake of women during the winter season (n = 138). Almost 53% of the study population consumed one or more kinds of indigenous foods during the recall period. A little over a third (36%) of women reported consuming indigenous GLVs (median intake = 44 g), while consumption of other indigenous vegetables (median intake = 58 g) and meats (median intake = 74 g) was even lower (19% and 6%, respectively). Even at these low consumption levels of indigenous foods, the intake of calcium was significantly higher in women who consumed indigenous food in the past 2 days than in those who did not (P = .001). The iron intake was also higher in the group consuming indigenous foods, although it was not statistically significant (P = .055; Table 4). There were no significant differences in the median intake of other nutrients in the 2 groups. Further, the distribution of those in the high food security group in both indigenous food consumers (57.53%) and nonconsumers (53.85) was not statistically different (P = .663).
Comparison of Nutrient Intake in Oraon Women Consuming Indigenous Food Versus Those Who Did Not.a
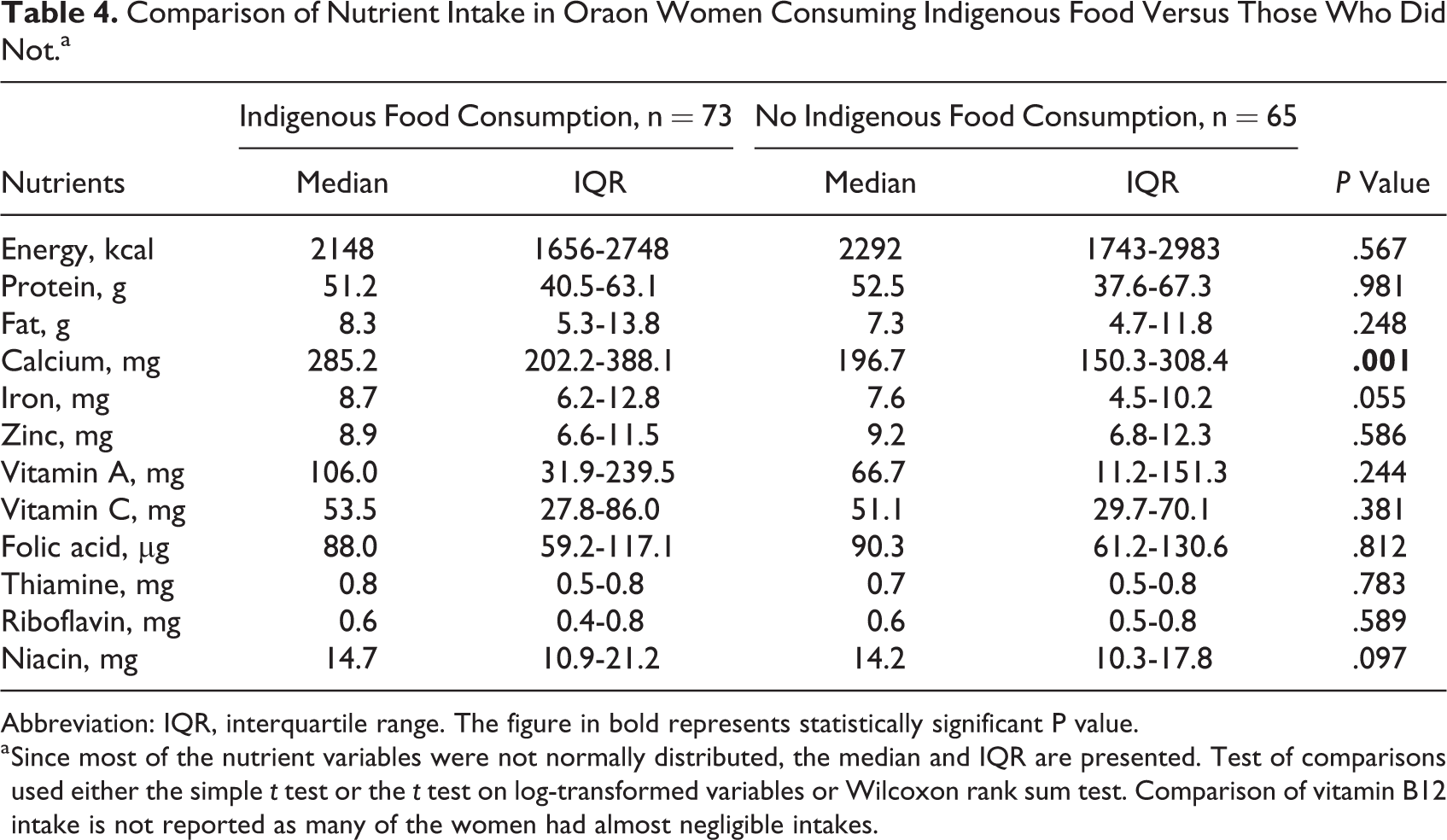
Abbreviation: IQR, interquartile range. The figure in bold represents statistically significant P value.
a Since most of the nutrient variables were not normally distributed, the median and IQR are presented. Test of comparisons used either the simple t test or the t test on log-transformed variables or Wilcoxon rank sum test. Comparison of vitamin B12 intake is not reported as many of the women had almost negligible intakes.
Chronic Energy Deficiency in Women
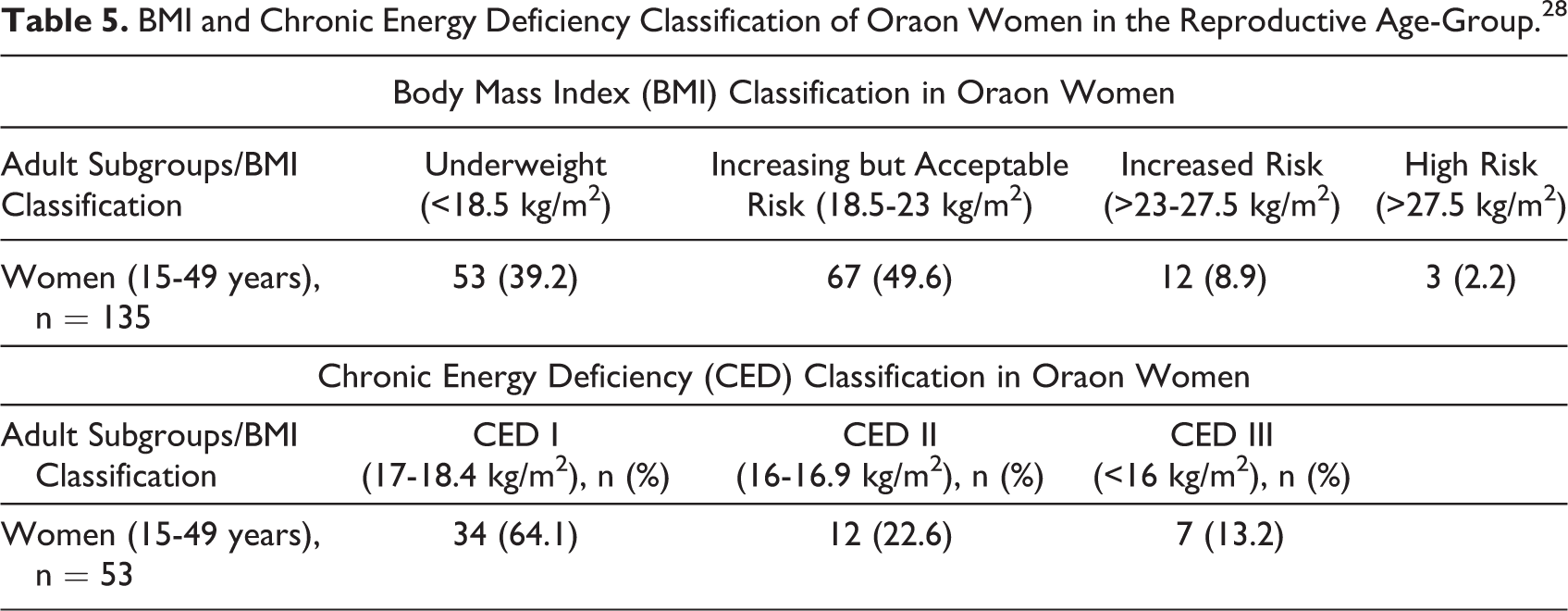
Based on anthropometric assessment, women (n= 135) were classified under various categories of underweight using CED classification (Table 5). About 40% of the women had various degrees of CED, with about 13.2% falling in the category of CED III (<16 kg/m2). There was no significant association (P = .716) between indigenous food consumption and underweight in women.
BMI and Chronic Energy Deficiency Classification of Oraon Women in the Reproductive Age-Group. 28
Discussion
Our study attempted to describe the dietary intake and nutritional status with emphasis on indigenous food consumption in a representative group of the Oraon tribal community in Jharkhand, India. The goal was to compile data on the availability and awareness about indigenous foods; estimate the actual consumption levels of these foods and their contribution to nutrient intake; and explore any association between indigenous food consumption and the nutritional status of Oraon women in the reproductive age-group.
The Oraon tribal community was aware of a wide variety of indigenous foods available in their immediate environment. Indigenous foods have been shown to be sources of essential micronutrients that are lacking in diets in many developing countries. These foods that are derived from local environmental resources including forests and other wild foods can be integrated into routine diets and have the potential to address micronutrient malnutrition. 11,29 In India, a large number of edible weeds have been shown to be used by tribals as part of their daily diets, and a systematic compilation of such edible weeds of tribals in Jharkhand and Orissa has been done. 13,30
A widespread awareness about these nutrient-dense indigenous foods 19 among the community did not translate into actual consumption of these foods, which in turn also led to poor nutrient intake. This was evident from the diets of these Oraon women. Around 47% of them did not consume any indigenous food during the DR period. Their diets were also lacking in micronutrients with NAR for iron, calcium, folic acid, thiamine, riboflavin, and vitamin B12, being inadequate in more than 50% of women in all the seasons. In addition to that, 40% of the women were underweight indicating a high prevalence of CED. The tribal population in India in general and the Oraon in particular has been seen to have high rates of malnutrition and CED. 18,31,32 Earlier studies in these communities have also documented this fact across different states and seen that both the adults and children have varying degrees of undernourishment. Globally, researchers have also explored and consolidated evidence on the potential of the biodiversity of forest and wild foods to improve dietary diversity and health outcomes. 33 -36
The paradox of high prevalence of undernutrition amidst a biodiverse food environment may be clarified by observations from our 24-hour DR and FFQ. Both the data showed that many of the indigenous foods remained underutilized in this tribal community with a comparatively low level of consumption. Only about 50% of the population reported consumption of any kind of indigenous food during the previous 2 days, and the quantity of intake was also low. Also, a seasonal variation in indigenous food consumption was observed. Other studies exploring the factors affecting low consumption of indigenous foods have also highlighted seasonality as a barrier to indigenous food consumption. 37 Other factors documented in the literature include sensory acceptability, opportunity cost for accessing and preparing these foods, suboptimal agricultural productivity, lack of formal education, lack of awareness about indigenous foods among young people, poor infrastructure, poverty, and so on. Further, there is a diminishing access and utilization of forest produce, which has the potential to support the food requirement of these vulnerable communities. 38 -40
This problem is further compounded with ongoing sociopolitical changes and imminent globalization. This phenomenon of globalization has resulted in changes that have mostly been detrimental to local biodiversity. This is due to the green revolution that often encourages mono-cropping, trade practices that promote introduction of exotic species, and transition of food preferences from traditional to processed, refined varieties, among others. 31,32
Our study also showed that that consumers of indigenous foods (although the quantity consumed was low) had higher intake of calcium when compared to the nonconsumers. It is well documented elsewhere that local food resources could be leveraged to add to food diversity and lead to improvement in micronutrient intake with positive nutritional outcomes. 41,42 A study by Powell et al in Tanzania showed that 48% of the food species consumed could be obtained in forest ecosystems, and diets with higher diversity and nutrient density were seen in children who had used forest food items. 11,43 While we have not included the data in this article, a substudy within this research project also found a number of micronutrient-rich indigenous foods in the food environment of the Oraon community. 19
Our study found a very low level of HH food security in a fourth of the HHs, and more than 50% of women had low dietary intake of micronutrients. Biodiversity is being recognized as essential for both food and nutrition security. The FAO also recommends drawing upon local biodiversity to help the world’s undernourished and economically disadvantaged to improve their dietary quantity and quality. 44 Further, nutritional programs and interventions in India and elsewhere understandably focus on providing adequate calorie consumption through energy-rich staple crops that do not, however, fulfill micronutrient requirements. This approach could benefit from a complementary strategy incorporating local indigenous foods into food programs for increasing dietary diversity and nutrition security.
A few strategic points of intervention based on our study findings could be promoting the consumption of seasonal indigenous foods through behavior change communication and preserving them for the lean season.
Conclusions
Our study has come up with some preliminary findings on diverse indigenous food systems of the Oraon tribal community, and a paradox has been observed regarding poor consumption of these resources despite awareness and seasonal availability. The data highlight the important role that indigenous foods can play in improving dietary diversity among the underprivileged tribal communities of Jharkhand specifically and the larger tribal group in general. Our findings underscore an important need for estimating intakes, assessing community knowledge about both the availability and the nutritional significance of the indigenous food items, and testing strategies such as behavior change communication for improving their intakes in the community.
Limitations
While we calculated adequacy of calorie intake based on the requirements for moderately active women, there were women who might have had higher levels of physical activity if they were routinely involved in activities such as wood chopping, working in brick kilns, cattle grazing, and so on. This may explain the higher prevalence of CED observed, despite a calorie intake close to 80% of recommended levels. For capturing seasonal intakes, 2-day 24-hours DRs were conducted only on one-third of the study sample in 2 more seasons.
Key Messages
High prevalence of undernutrition exists among women in the Oraon tribal
community of Jharkhand India amidst rich knowledge regarding the
nutrient-rich indigenous foods. The community is aware about the indigenous food resources yet the
consumption of these foods is low. Those who consumed indigenous foods had higher intake of some
micronutrients. After exploring the possible reasons for poor consumption, there is a
need to promote the incorporation of these traditional resources into
nutrition programs and interventions to improve their consumption in the
community.
Supplemental Material
supplementary_table_1_(1) - Estimates of Indigenous Food Consumption and Their Contribution to Nutrient Intake in Oraon Tribal Women of Jharkhand, India
supplementary_table_1_(1) for Estimates of Indigenous Food Consumption and Their Contribution to Nutrient Intake in Oraon Tribal Women of Jharkhand, India by Suparna Ghosh-Jerath, Archna Singh, Tanica Lyngdoh, Melina S. Magsumbol, Preeti Kamboj, and Gail Goldberg in Food and Nutrition Bulletin
Footnotes
Authors’ Note
The data can be accessed through a formal request to the authors. SGJ, AS, and MSM conceived and designed the study with overall supervision from GG. SGJ, PK, and AS developed the tools for data collection, the data analysis plan, and supervised the data collection and data entry. TL did the statistical analysis. SGJ and AS prepared the first draft of the manuscript. All authors contributed to critique and modification of the manuscript, read and approved the final version. SGJ had final responsibility for the decision to submit for publication.
Acknowledgments
The authors would like to acknowledge the invaluable contribution of all Oraon respondents in the study villages for sharing their knowledge about their rich heritage of indigenous and traditional foods. The contribution of Professor R. P. Singh “Ratan” and his team from Birsa Agricultural University for carrying out the taxonomic classification of the food samples is gratefully acknowledged. They would like to thank Ms. Keya Chatterjee, Mr. Alok Kundu, and their team at “Ekjut,” a local NGO, for providing support for their facilitation of data collection and managing an excellent team of fieldworkers. Authors would also like to thank all the field staff, ASHAs, and Anganwadi workers in the study villages for their support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Wellcome Trust Capacity Strengthening Strategic Award to the Public Health Foundation of India and consortium of UK universities (grant number is WT084754).
Supplemental Material
Supplemental material is available for this article online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.