
Abstract
Background:
Independence gained during adolescence may be associated with unhealthy eating behaviors. Although malnutrition among adolescents is evident, studies on eating behaviors among adolescents are scarce.
Objective:
To determine the effectiveness of a teacher-led Healthy Lifestyle Program on eating behaviors among adolescents in Malaysia.
Methods:
This was a cluster randomized controlled trial (conducted in 2012 to 2014), with 100 schools randomly selected from 721 schools, then assigned to 50 intervention schools and 50 control schools. A Healthy Eating and Be Active among Teens (HEBAT) module was developed for pretrained teachers to deliver a Healthy Lifestyle Program on eating behaviors among adolescents. Eating behaviors of the respondents was determined using Eating Behaviors Questionnaire. Linear Mixed Model analysis and χ2 test were used to determine within- and between-group effects of studied variables.
Results:
A total of 4277 respondents participated in this study, with 2635 samples involved in the final analysis, comprised of 921 intervention and 1714 control respondents. There were 32.4% (36.4%) males and 67.6% (63.6%) females in the intervention (control) group. Mean age was comparable between the groups (intervention = 12.98 years; control = 12.97 years). Majority of the respondents skipped meals at baseline (intervention = 74.7%; control = 79.5%). After the program, intervention respondents had higher consumption frequency of lunch, dinner, and mid-morning snack but a lower consumption frequency of late-evening snack and meal skipping behaviors than their control counterparts.
Conclusion:
The teacher-led Healthy Lifestyle Program was effective in reducing meal-skipping behaviors among Malaysian adolescents.
Introduction
Adolescence, which is often attained between the ages of 10 to 19 years old, is a period of human growth and development that occurs after childhood and before adulthood. 1 It is characterized by dramatic changes in physical, emotional, and cognitive functions, and it is the second opportunity for adolescents to catch up with growth and development before adulthood. 2 Adolescents often struggle to gain independence over many aspects of their life, including food control. 3 Unhealthy eating behaviors (eg, meal skipping and unconventional eating patterns that do not meet dietary recommendations, such as snacking for meals) have become prevalent among adolescents in the recent years. Meal skipping is often defined as the omission or lack of consumption of 1 or more of the traditional main meals (breakfast, lunch, or dinner), while snacking can be defined as consuming foods and beverages at least once between main meals per day. 4
High prevalence of meal skipping and snacking behaviors among adolescents has been reported in recent years. 4 -9 A study in Minnesota showed that among 80 354 secondary school adolescents, the prevalence of meal skipping was 28.5%. 5 In Malaysia, more than half (72.3%) of the adolescents skipped at least one meal per day, and the most frequently missed meal was breakfast, followed by lunch, and dinner. 6 In another local study, about 1 in 7 (14.1%) adolescents skipped all 3 meals in a day. 7 Looking at the prevalence of snacking among 1774 adolescents in China, more than half (55.0%) snacked at least once per day, with the highest frequency for afternoon snack. 8 A similar scenario was reported among Malaysian adolescents. 9
Unhealthy eating behaviors may lead to increased risk of malnutrition. Larger waist circumference, higher fasting insulin, total cholesterol and low-density lipoprotein cholesterol concentrations, and a detrimental effect on cardio metabolic health were found when the problem remained for a long time among adolescents. 4,10 -12 In a recent national surveillance study in Malaysia, the prevalence of thinness and obesity among adolescents aged 10 to 14 years old was 6.9% and 14.4%, respectively. For the older age-group (adolescents aged 15 to 17 years old), prevalence of thinness and obesity was 7.0% and 9.6%, respectively. Although dual burden of malnutrition coexist among both the younger and older adolescents, prevalence of malnutrition among secondary school adolescents (37.9%) was higher compared to preschool children (15.7%) and primary school children (23.8%), 12 placing them at a higher risk of nutrition-related health issues.
Healthy eating behaviors during adolescence are crucial for both growth and development and the prevention of diet-related chronic diseases in adulthood. 13 Evidence is mounting that eating behaviors among adolescents can be improved through nutritional intervention. Numerous evidence has indicated that school-based interventions might be effective in promoting healthy eating among adolescents, since schools provide a natural learning environment, reach out to a large population of adolescents, and offer opportunities for peer interactions. 14 -16 However, such intervention is lacking in Malaysia. In Malaysia, teachers receive little training in nutrition. Appropriate and comprehensive modules to guide teachers in promoting healthy eating among adolescents are scarce. 17 In view of the importance of healthy eating among adolescents, a 3-year, teacher-led, school-based Healthy Lifestyle Program among Malaysian adolescents living in day school hostels was conducted using a module called Healthy Eating and Be Active Eating among Teens (HEBAT). This intervention emphasized the importance of energy balance through healthy eating and active living to achieve healthy body weight status among the adolescents. The current article aims to evaluate the effectiveness of the HEBAT module on eating behaviors among Malaysian adolescents living in day school hostels. We hypothesized that the Healthy Lifestyle Program was effective in promoting healthy eating behaviors (eg, lower meal skipping and snacking behaviors) among adolescents in Malaysia.
Methods
Ethical Approval
Ethical approval was obtained from the Ethics Committee for Research Involving Human Subjects, Universiti Putra Malaysia. Permissions to conduct this study were obtained from the Ministry of Education Malaysia and respective school principals from the selected day schools prior to data collection. Study information was distributed to all eligible respondents, and written consents were obtained from the respondents or their caretakers prior to data collection.
Participants and Study Design
Our respondents were recruited from day schools. There are 2 types of boarding school systems in Malaysia, namely, full boarding schools and day schools. Unlike students attending full boarding schools, students of day schools reside in the hostels during weekdays and are allowed to go home during weekends. A multistage stratified cluster sampling method was used in this study. In 2012, a total of 100 schools were randomly selected from 721 day schools and were randomly assigned to 50 intervention schools and 50 control schools based on 6 main regions in Malaysia, namely, Northern region, Southern region, Central region, East-Coast region, Sabah, and Sarawak. Stratification was done based on the geographical regions and locations (urban and rural areas) in Malaysia.
All adolescents from form 1 (grade 1 of the lower secondary school) of the selected day schools (mean age: intervention group: 12.98 years; control group: 12.97 years) were invited to participate in the study (n = 5186), with 4277 adolescents consented to participate (response rate was = 82.5%). Of the 4277 respondents recruited, 1885 (44.1%) were in the intervention group, and 2392 (55.9%) were in the control group. The study followed the cohort of students from form 1 to form 3. The intervention group received intervention based on the HEBAT modules, while the control group continued their standard practices. The control group received HEBAT modules after completion of this study. This design allowed the researchers to determine the causal effect of the intervention on eating behaviors among intervention respondents.
Intervention Program
The 3-year Healthy Lifestyle Program was conducted using 2 phases of the HEBAT modules, with the general objectives to introduce the concept and basic knowledge on healthy lifestyle to the adolescents as well as to empower the adolescents with healthy eating and physical activity skills to be applied in their daily life. The concept of the HEBAT modules is based on an emphasis in achieving healthy body weight status among the adolescents, whereby ways to maintain energy balance through healthy eating and active living were conveyed to the respondents through various interactive educational activities. Four topics of the HEBAT module phase I which comprised of the basic knowledge on healthy lifestyle were introduced to the adolescents. This was followed by another 6 topics of HEBAT module phase II which aimed to enhance skills on practicing healthy lifestyle among the adolescents. Details of HEBAT module are depicted in Table 1.
Topics and Objectives of HEBAT Modules (Phase 1 and 2).
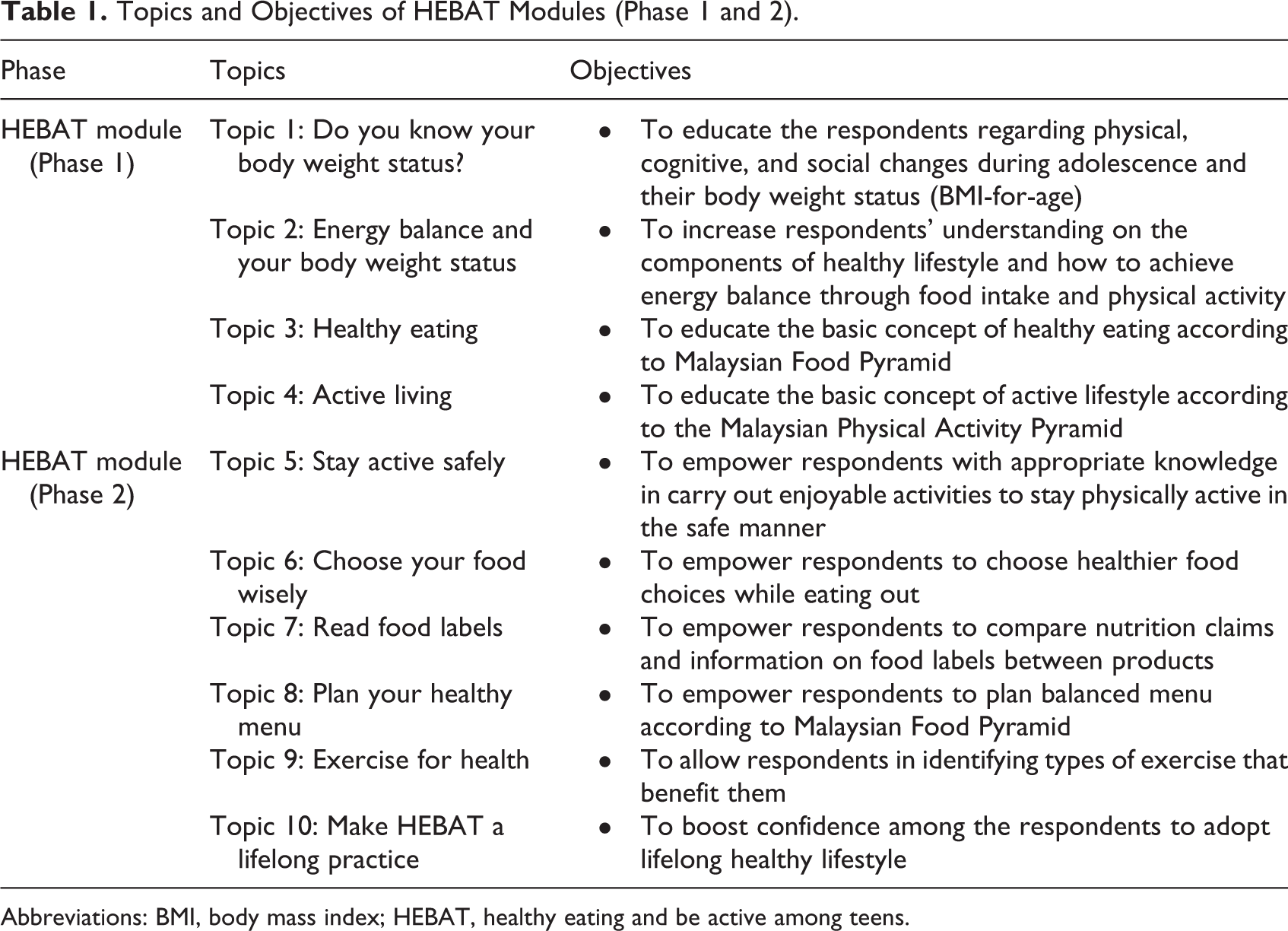
Abbreviations: BMI, body mass index; HEBAT, healthy eating and be active among teens.
The structure of the modules was developed systematically to ease the implementation of the interventions, whereby each topic consisted of teaching guidelines, topic notes or power point slides, goal card, program feedback, and tutorial forms. Various interactive and learning activities were adopted, including body weight status assessment, group discussions and presentations, role-plays, games, and sketches. Educational materials such as food physical activity cards and food labels were developed to enhance the learning process during the intervention. A comic book (Buku Komik Kembara Alam Sam) published by the Nutrition Society of Malaysia, Growth Reference Charts (body mass index [BMI]-for-age) from the Ministry of Health Malaysia as well as skipping ropes and pedometers were used together with the modules of HEBAT. The modules and education materials were pretested prior to program implementation at 2 day school hostels (1 in rural area and 1 in urban area) to ensure the appropriateness of the contents of the modules and educational materials.
The implementation of the intervention program was planned in such a way that no teaching was done during school holidays and the examination month to ensure good attendance and submission rate among the intervention respondents. One new topic from the HEBAT modules was introduced each month by the trained teachers. Delivery of each topic took about an hour, and key messages were highlighted by the teachers before and at the end of each topic. The teachers also emphasized the importance of energy balance to achieve healthy body weight status. To ensure all respondents followed the study protocols, the program implementation was monitored continuously through phone calls, e-mails, and school visits by the research team. Control respondents continued their physical education class as usual.
Assessment of Sociodemographic Background
Information such as age, sex, ethnicity, date of birth, monthly pocket money, number of siblings, parental educational level, occupation, and monthly income were ascertained using a pretested structured questionnaire.
Assessment of Eating Behaviors
The Eating Behaviors Questionnaire was adopted to determine the eating behaviors of the respondents. 4 We extracted 6 items from the original questionnaire and ascertained the frequency of meal consumption (3 items) and frequency of snacking between main meals (3 items) for a 1-week interval. The respondents were requested to indicate the number of days that they practiced such eating behaviors over the past 1 week, ranging from “0” day to “7” days/week. For example, respondent who chose “2” for breakfast consumption indicated he consumed breakfast 2 times in a week. With reference to a previous local study, 18 respondents were requested to indicate the daily consumption pattern for 3 main meals (breakfast, lunch, and dinner) and 3 snacks in between the main meals (midmorning snack, afternoon snack, and late-evening snack).
If respondents consumed a particular meal (eg, breakfast) for 7 days in a week, “1” score was given; if respondents consumed the particular meal for 0 to 6 days, “0” score was given, indicating that particular meal was skipped. In order to determine meal skipping behavior, the score for each of the main meal consumption (breakfast, lunch, and dinner) was added. A score of “3” indicated that respondents never skipped meals in a week, while a score <“3” indicated that respondents had ever skipped meals. For snacking behavior, number of days of snack consumption between meals (midmorning, afternoon, and late-evening snack) in a week was added. A score of “0” indicated respondents never snacked between meals, while a score of “1” and above indicated respondents snacked in a week.
Statistical Analysis
A modified intention-to-treat (ITT) analysis was used, and respondents who fulfilled the following criteria were included in the data analysis process:
19
Intervention respondents who completed all components of the module (10 topics) and respondents from both intervention and control groups who completed all 3 points of data collection (pre-intervention, post intervention I, and post intervention II)
The final analyzed sample comprised of 921 and 1714 respondents from the intervention and control groups, respectively, given an overall response rate of 61.6%. The attrition was attributed to respondents who were unable to complete all the intervention topics (absence for 1 topic or more, 40.2%), no longer staying in the hostels (35.1%), or transferred to other schools (24.7%). These respondents were considered dropouts from the study and were not included in the data analysis (Figure 1).
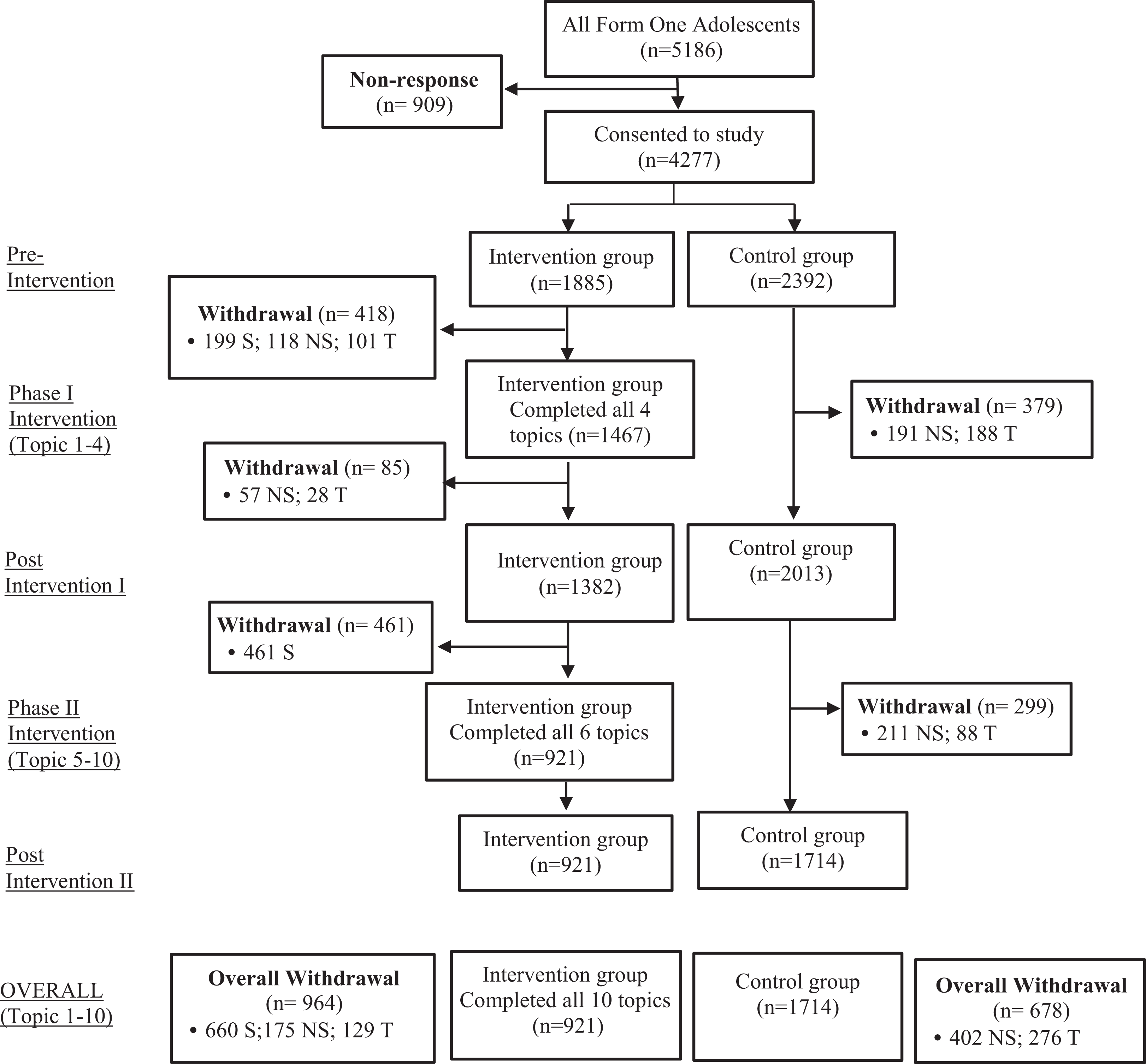
Consort diagram of study. S indicates that respondents stayed in hostel, but unable to complete all topics; NS, respondents no longer staying in hostel; T, respondents transferred to other school; Form 1 adolescents: adolescents in grade 1 of the lower secondary.
Data for a total of 921 intervention respondents and 1714 control respondents were analyzed using IBM SPSS Statistics version 21 software. Missing data (13%) were treated using Last Observation Carried Forward method. Linear Mixed Model analysis was performed to determine the within- and between-group effects of the studied variables. The time and interaction effects over 3 time points were assessed to evaluate the effectiveness of the intervention program. Chi-square test was used to determine the changes in categorical data between the groups over time. Statistical significance was set at P < .05.
Results
Table 2 shows a majority of the intervention and control respondents were female, Malay, and from rural areas. A majority of the parents had attained upper secondary school education. There were comparable characteristics between the respondents in terms of mean age, sex, ethnicities, number of siblings, monthly pocket money, parental monthly income, and parental education level.
Sociodemographic Background of the Respondents (Year, 2012 to 2014).a
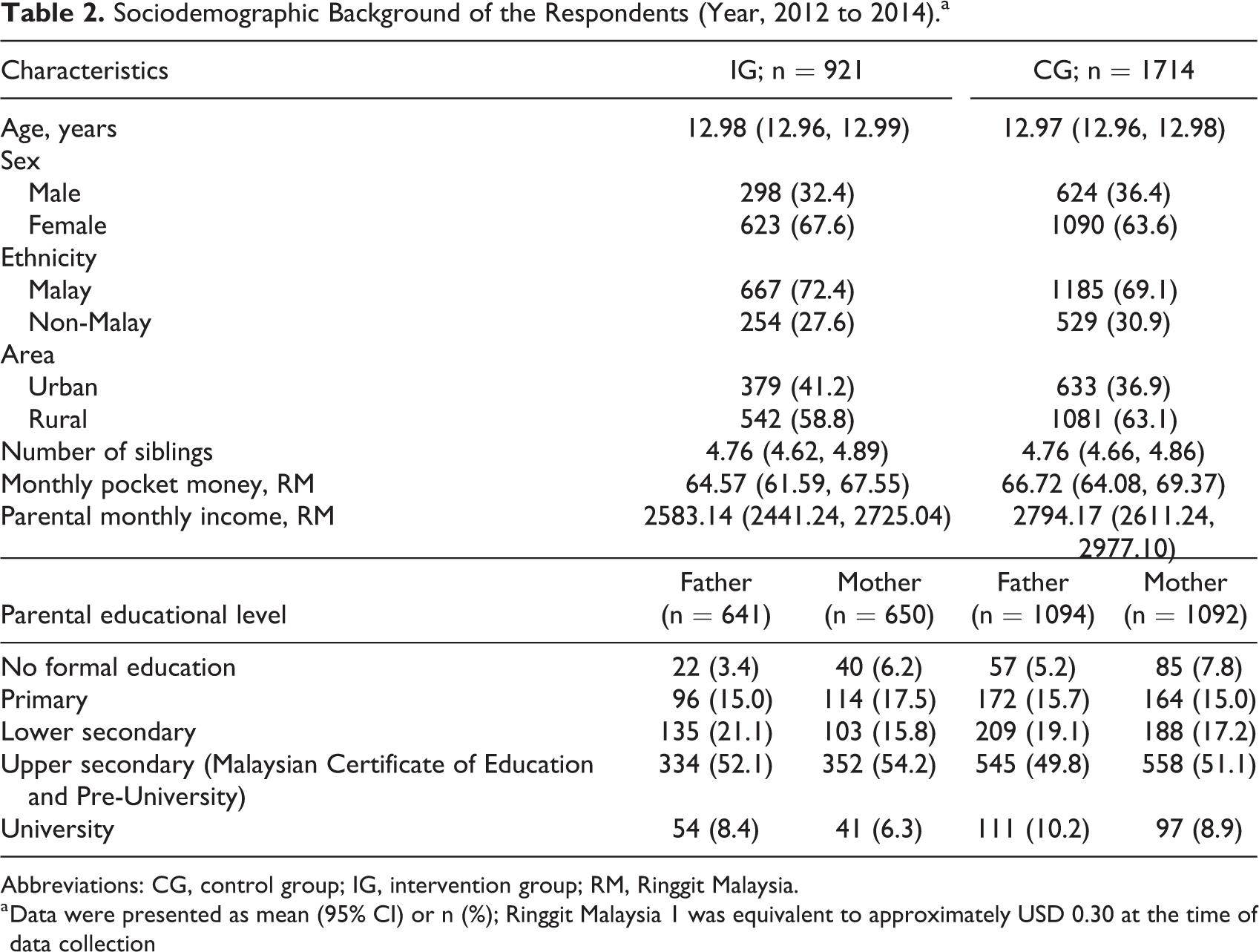
Abbreviations: CG, control group; IG, intervention group; RM, Ringgit Malaysia.
a Data were presented as mean (95% CI) or n (%); Ringgit Malaysia 1 was equivalent to approximately USD 0.30 at the time of data collection
As depicted in Table 3, the respondents consumed approximately 5 days of main meals (breakfast, lunch, and dinner) and around 3 to 4 days of snacks (mid-morning, afternoon and late-evening snack) in a week. The mean consumption frequencies of breakfast and mid-morning snack remained the same within the intervention group (Breakfast: P = .107; mid-morning snack: P = .872), while there was a significant decrease within the control group over time (breakfast: P < .001; mid-morning snack: P = .002). There was a significant increase in the mean consumption frequencies of lunch, dinner, and late evening snack among the intervention respondents over the 3 time points. Among the control respondents, there was significant decrease in the mean frequency intake of main meals (breakfast, lunch, and dinner) and mid-morning snack, while no significant change was observed on the consumption pattern for late evening snack (Table 3). The mean consumption frequency of afternoon snack significantly decreased during the post intervention I and post intervention II phases, regardless of the treatment group.
Comparison of Consumption Pattern of Main Meals and Snacks Over Time Between Intervention and Control Groups.
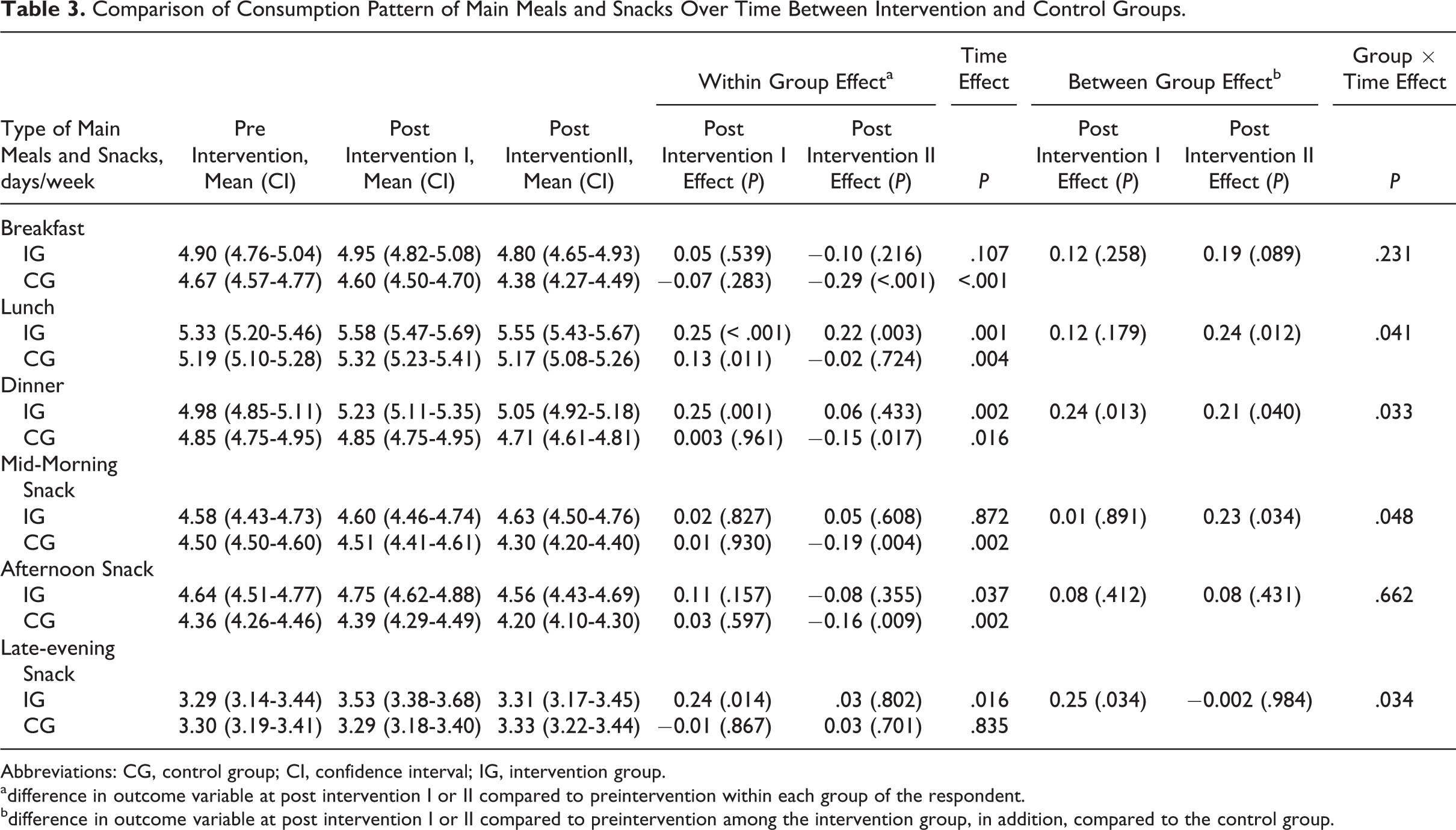
Abbreviations: CG, control group; CI, confidence interval; IG, intervention group.
adifference in outcome variable at post intervention I or II compared to preintervention within each group of the respondent.
bdifference in outcome variable at post intervention I or II compared to preintervention among the intervention group, in addition, compared to the control group.
On the other hand, while there was comparable mean consumption frequency of lunch and dinner between the groups at baseline, the intervention group had significant higher mean frequency of lunch and dinner at post intervention II. No significant difference in the consumption frequency for breakfast was observed between the 2 groups at the end of the intervention. For snacking behavior, only mean frequency intake on afternoon snack was significantly higher among the intervention respondents at baseline. Mean consumption frequency was higher for mid-morning snack but lower for late evening snack in the intervention group compared to their control group counterparts after the program, indicated by the significant group and time effects. In general, comparison between the groups showed that the intervention program was able to improve consumption frequencies of lunch, dinner, and midmorning snacking and reduce frequency of late evening snack.
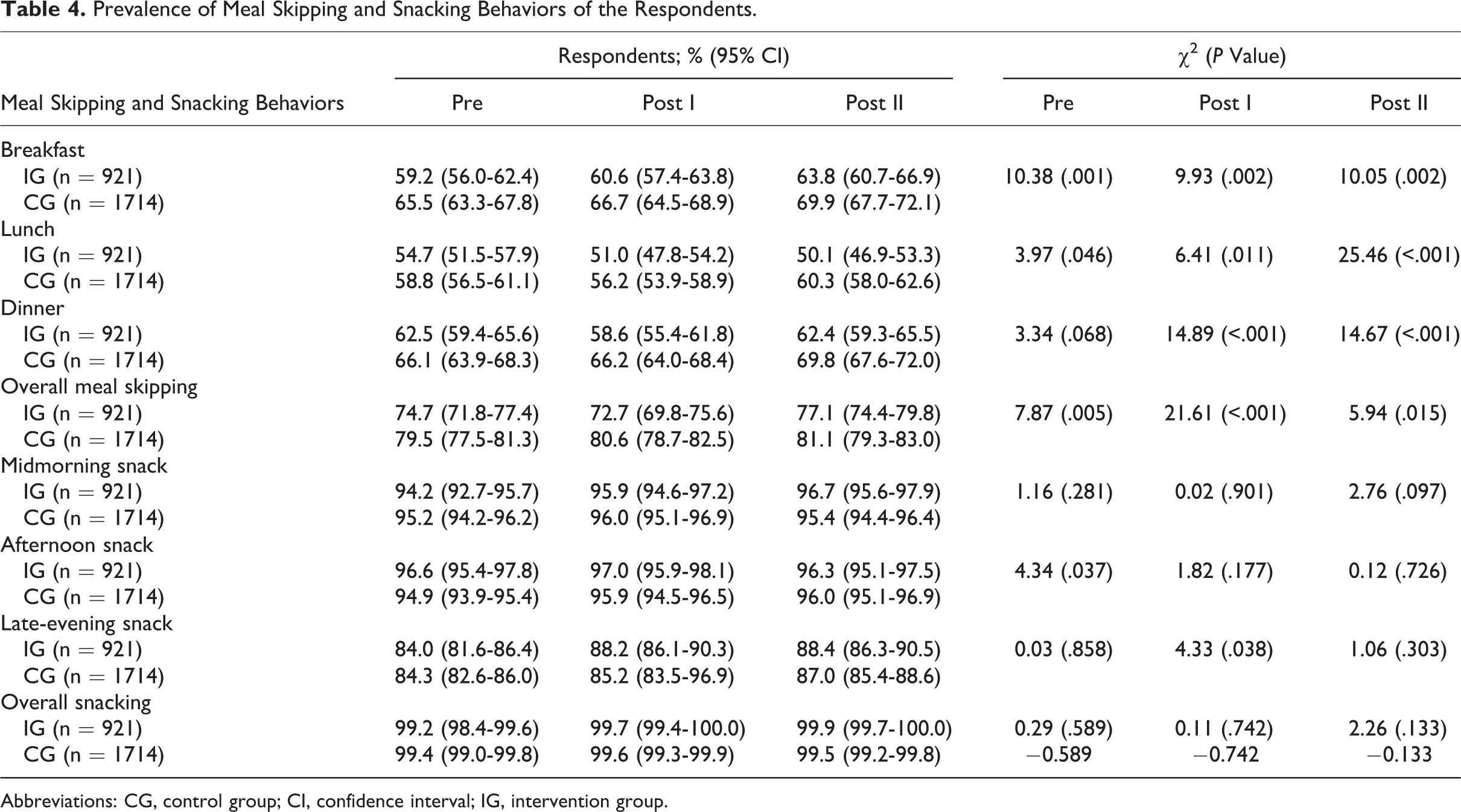
At baseline, approximately 75% and 80% of the intervention and control respondents skipped main meals. Before the intervention program, while the dinner skipping pattern was comparable between intervention and control groups, there was a significantly higher proportion of respondents from the control group who skipped breakfast and lunch. After the intervention program, approximately 1 in 4 (22.9%) of the intervention participants never skipped meals, compared to 18.9% among the control respondents. Approximately 50% to 65% and 60% to 70% respondents from the intervention and control groups skipped breakfast, lunch, and dinner after the program, respectively. A comparison between the groups revealed that the proportions of the respondents who skipped breakfast, lunch, or dinner were substantially lower among the intervention group after the Healthy Lifestyle Program, indicating that the program was able to promote healthy eating behaviors among the adolescents.
Snacking was evident among respondents, with approximately 99% having snacked, attributed to the availability of snacks prepared by the hostels. As shown in Table 4, there were subtle differences in the snacking habits of the respondents in both groups after the intervention program. At baseline, there was significant higher proportion of intervention respondents who had afternoon snacks; however, such observation could not be found at post intervention I and II, mainly attributed to increased prevalence of afternoon snacking behavior among the control group. There were comparable proportions of mid-morning and late evening snackers across the groups.
Prevalence of Meal Skipping and Snacking Behaviors of the Respondents.
Abbreviations: CG, control group; CI, confidence interval; IG, intervention group.
Discussion
Healthy eating is a cornerstone to the overall well-being of adolescents. It is important to cultivate good eating behaviors among adolescents to ensure they meet the dietary recommendations to achieve optimum growth. It is important not to skip meals, as previous studies have shown, for example, that breakfast skipping was associated with higher body weight, BMI, BMI z-scores, waist circumference, body fat mass, and percentage of body fat among adolescents compared to those who do not skip breakfast. 20-21 Respondents who skipped breakfast were found more likely to skip lunch and dinner as well, which in turn increased the risk of eating disorders, overweight, or obesity problems.
In the current study, about 75% of the respondents in both the intervention and control groups skipped at least one meal at baseline. This was consistent with a cross-sectional study by Fara Wahida et al, 6 which showed that about two-thirds of the respondents (72.3%) skipped at least one meal. There was a significantly lower percentage of breakfast skipping among the intervention group compared to the control group over the 3 time points, indicating the Healthy Lifestyle Program was effective in promoting regular meal times. This was consistent with a study by Radcliffe et al. 22 Likewise, there was a significantly lower percentage of lunch, dinner, and overall meal skipping behavior among the intervention group than the control group. The Healthy Lifestyle Program empowered the intervention respondents on ways to identify unhealthy eating behaviors such as skipping meals and enabled them to apply what they have learnt from the program into a lifelong practice. On the other hand, without appropriate healthy lifestyle intervention, adolescents in the control group might skip meals to look more muscular for males or to look slimmer for females, 11 besides other reasons such as time constraint, oversleeping, and lack of appetite. 23
At baseline, almost all respondents snacked regardless of treatment group. This was in line with a local study by Teo et al 9 , but the prevalence was somehow higher than another study in China. 8 There was no difference in the proportion of midmorning, afternoon, or late evening as well as the overall snacking behaviors between the groups over time. This might be mainly attributed to the availability of snacks prepared by the school hostels. Since all students attending day schools are provided with meals and snacks, regardless of their intervention arm, this was a big challenge to the researchers. On the other hand, it is worth noting that while there was significantly higher mean consumption frequency on mid-morning snacks among the intervention respondents, this was accompanied with lower mean frequency on late evening snacks. In light of the emerging evidence demonstrating a relationship between timing of food intake and weight regulation, whereby eating more at midday was associated with lower risk of being overweight and obese, 24– 25 the abovementioned interesting findings allowed us to presume that the intervention program was effective in reducing risk of overweight among the adolescents in the future. The results from this study provide important insights into snacking which could be used to formulate nutrition education programs and promote healthier snacking in adolescents. Despite the lack of universally agreed definition for “snack,” snacks generally comprise energy-dense food choices. It is possible that as adolescents gain more autonomy in food choices, they may choose high-energy dense foods at snack time, leading to a decrease in overall diet quality. 26-27 Although snacking can be incorporated as part of a healthy diet and can improve dietary intakes of certain vulnerable groups, such as older persons, recommendation of snacking should be accompanied with adequate knowledge and vigilance for other age-groups, including young adults. This is especially critical when a steadily increasing trend of obesity among young adults is evident, which is even more pronounced in developing countries including Malaysia, where rapid epidemiologic transition is highly expecting.
Inevitably, school policy, infrastructure, environment, curricula, and staff have the potential to positively influence the behaviors of adolescents and health. 17 Active involvement of school authorities, food providers in the school hostels, and health personnel is important as demonstrated through this study; teachers acted as role models to adolescents and teacher-led nutrition education can improve the outcome of the intervention program (eg, eating behaviors of adolescents). Besides, it is necessary to study the barriers, challenges, and obstacles while implementing an efficient and efficacious program among adolescents to overcome the unhealthy eating behaviors problem.
Limitations
Using a self-administered questionnaire might lead to underreporting or overreporting of data by the respondents. The findings might not be accurate as they depend on the honesty and the ability of respondents to understand the questions, causing the possibility of self-reported bias. In addition, there was a high dropout rate and a large number of missing data in the study variables. Statistical methods should be used to treat the missing values. This study also lacked evaluation of the teachers from the intervention schools. Hence, researchers could not know how the teachers conducted the intervention sessions to the students, causing the probability of intervention choice bias, particularly during program implementation.
This study was a cluster randomized control trial, and it recruited a large sample with a relatively high response rate of respondents. The modified ITT analysis determined changes in eating behaviors over 3 years of time between intervention and control respondents before and after the intervention program. Hence, the effectiveness of Healthy Lifestyle Program could be assessed.
Conclusions
The Healthy Lifestyle Program was effective in reducing meal skipping behaviors among Malaysian adolescents. It is important not to skip meals as adolescents who skipped breakfast were more likely to skip lunch and dinner as well, which in turn may increase the risk of eating disorders, overweight, or obesity problems. Active involvement of school authorities (eg, wardens and teachers), food providers in the school hostels, and health personnel are necessary to promote healthy eating behaviors among adolescents.
Footnotes
Acknowledgments
The authors would like to extend their appreciation to all stakeholders (Nestle Products Pte Ltd, Ministry of Education of Malaysia and Universiti Putra Malaysia).
Author Contribution
Yit Siew Chin, Mohd Taib Mohd Nasir, and Yoke Mun Chan designed the study, wrote the protocol, conducted literature searches and implemented the intervention program. Chian Yi Teng provided summaries of previous research studies, conducted statistical analysis, wrote the first draft of the manuscript, and all authors commented and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided by Nestle Products Pte Ltd Grant Protocol Number 6373700. The funder has no role in the study design, collection, analysis or interpretation of the data, writing the manuscript, or the decision to submit the paper for publication.