
Abstract
Background:
Close to half of all children younger than 5 years in the Northeast and Northwest geopolitical zones were estimated to be stunted in their growth for their age in 2013 compared to 22% of children in the rest of Nigeria.
Objectives:
We examine the drivers of chronic child undernutrition in northern Nigeria and how those drivers differ from other areas of the country.
Methods:
Both a standard child-level regression-based approach and decomposition analysis were used to address the determinants of stunting and decompose how drivers differ between northern Nigeria and other areas of the country using 2008 and 2013 Nigeria DHS data.
Results:
There are strong differences in the levels of the determinants of undernutrition in young children between the 2 parts of the country. However, equally important, the decomposition analysis shows that there are significant differences between northern Nigeria and other areas of Nigeria in the effect of the same determinant of nutritional status in accelerating or retarding the linear growth of young children.
Conclusions:
A national program to address child undernutrition must recognize this heterogeneity in its design. To impose across Nigeria, a single set of approaches to address the factors which results in stunted children is likely to fail for large numbers of children if these strong geographical differences in how these determinants operate to affect child nutritional status are not considered. Solutions need to be developed within northern Nigeria to more closely reflect the way the determinants of nutritional status operate in this area of the country.
Introduction
The burden of chronic malnutrition, in particular undernutrition, borne by the population of northern Nigeria is one of the heaviest globally. Close to half of all children younger than 5 years in the Northeast and Northwest geopolitical zones of the country were estimated to be stunted in their growth (height) for their age in 2013 (height-for-age z-score (HAZ) < −2.0) compared to 22% of children in the rest of Nigeria and 2.3% in the well-nourished population of young children globally from which the child growth standards are derived. 1,2 Stunting in young children is an indicator of chronic undernutrition that crosses generations, being a consequence of maternal undernutrition during pregnancy, which adversely affects fetal growth, coupled with poor diet and feeding practices and adverse health shocks faced by the infant during the first 2 years of life. 3 Stunted growth is the result of a range of factors, including both immediate determinants, such as the quality of nutritional care or diet that the child receives, and more basic, such as the empowerment of the child’s mother, typically the principal caregiver of the young child, in terms of the knowledge and economic resources that she can draw upon to provide the best possible care to the child. The cognitive development of the young child is impeded as this retardation in physical growth affects the child’s brain development. The impact of such stunting in physical and mental development on the well-being and economic prospects over the life span of the child as she or he grows to adulthood is uniformly adverse, resulting in generally lower educational attainment, lower economic productivity, increased morbidity, and shorter life expectancy. More broadly, chronic undernutrition is a significant barrier to Nigeria’s sustained progress in human and economic development for the benefit of all its citizens (note 1).
Efforts to sharply improve the growth trajectories of young children in northern Nigeria are being made by government agencies at federal, state, and local government levels, working with development partners and international and local nongovernmental and civil society organizations. These include ensuring that the parents of young children have better access to knowledge of good infant and young child feeding (ICYF) practices, providing antenatal clinics for pregnant women and well-child clinics for infants, addressing micronutrient deficiencies through the provision of supplements, increasing investments to treat acutely undernourished children, and advocacy efforts to increase the flow of public resources to improve the nutritional status of young children and their mothers.
However, the efforts now being made in sum are not sufficient to address the problem. Although some gains have been achieved in reducing the level of undernutrition in the country as a whole, particularly in northern Nigeria, progress is slow and not always positive. Notably, the prevalence of stunted children younger than 5 years in the Northwest geopolitical zone rose from 52.6% in 2008 to 54.8% in 2013. 1,4 A combination of efforts of much greater scope than is possible with the resources now being provided is needed to address chronic undernutrition in northern Nigeria.
To better understand the drivers of chronic child undernutrition in northern Nigeria and how those drivers differ from other areas of the country, this article presents the results of an econometric analysis of data from the 2008 and 2013 Nigeria Demographic and Health Surveys (NDHS). A standard child-level regression-based approach is used for the first part of the analysis using whether the child aged 6 to 23 months is stunted (HAZ < −2.0) as the dependent variable. Separate models of the drivers of child stunting are developed for northern Nigeria (Northwest and Northeast geopolitical zones) in 2008 and 2013 and for other areas of Nigeria in 2013. The analysis is then extended by comparing the model for northern Nigeria in 2013 to other areas of Nigeria in 2013 to decompose differences between the models. This was done to gain understanding on how the determinants of stunting in children aged 6 to 23 months differ between the 2 areas to better understand how well successful approaches used elsewhere in Nigeria to reduce child stunting might work in northern Nigeria.
The organization of this article is briefly as follows. Zonal and Demographic Focus of the Study section provides an overview of the zonal focus and the demographic focus of the study. Undernutrition in Northern Nigeria section presents an overview of undernutrition levels and trends in northern Nigeria relative to the rest of the country. This leads into a discussion of the United Nations International Children’s Emergency Fund (UNICEF) conceptual framework for understanding the drivers of child nutritional status which was used to guide the avenues of inquiry for the study. Drivers of Chronic Undernutrition in Young Children section presents in summary form the major findings of the quantitative analysis of the determinants of child stunting based on analysis of data from the 2008 and 2013 NDHS. Implications for Investment Priorities and Program Design for Improved Nutrition section provides concluding remarks and policy implications for investment priorities and program design for improved nutrition based on the results of the data analysis.
Zonal and Demographic Focus of the Study
Here several elements of the dimensions of the quantitative analysis are defined in more detail, in particular what adverse nutritional outcomes, what areas of Nigeria, and whose nutritional condition is of interest in undertaking the analysis.
Chronic Versus Acute Undernutrition
The terms of reference for the overall study specified that the focus would be chronic malnutrition in northern Nigeria, in particular chronic undernutrition, rather than acute undernutrition. This is an important programmatic distinction. Acute undernutrition generally reflects an emergency situation tied to a sharp adverse health shock or restricted dietary intake where immediate action is necessary to save the lives of those affected. Acutely undernourished individuals are at risk of death due to sharp reductions in dietary intake or due to illness that prevents the individual from making effective use of any food consumed. Acute undernutrition is characterized by wasting (low weight-for-height) or severe thinness. Addressing acute undernutrition often requires clinical or close community-based management of the diet and health of acutely undernourished individuals, actions which generally are led by health sector personnel.
In contrast, chronic undernutrition is the cumulative outcome of multiple factors, including maternal nutritional and health status, diet, patterns of infection and other illness, access to public health services, and others that impact on the growth of individuals over months and years. Effective interventions to address chronic undernutrition are designed to prevent the development of acute undernutrition, generally are done over a long-time period, and often are not nutrition-specific, but, rather are nutrition sensitive, involving inputs from multiple sectors, including health, agriculture, education, water and sanitation, and others.
Delineating Northern Nigeria
A definition of northern Nigeria was an initial step in designing this study. A review of the spatial dimensions of stunting in young children in Nigeria makes it clear that the Northwest geopolitical zone of the country has the highest prevalence, followed by the Northeast zone (Figure 1; note 2). Estimates of stunting prevalence from the 2013 NDHS and population projections for 2013 from the 2006 Census for children younger than 5 years at state level suggest that 49% of all stunted children younger than 5 years in 2013 in Nigeria were in the Northwest zone of the country and 19% in the Northeast. Based on this assessment, in undertaking the analysis, our zonal area of focus was on the Northwest and Northeast zones of the country.
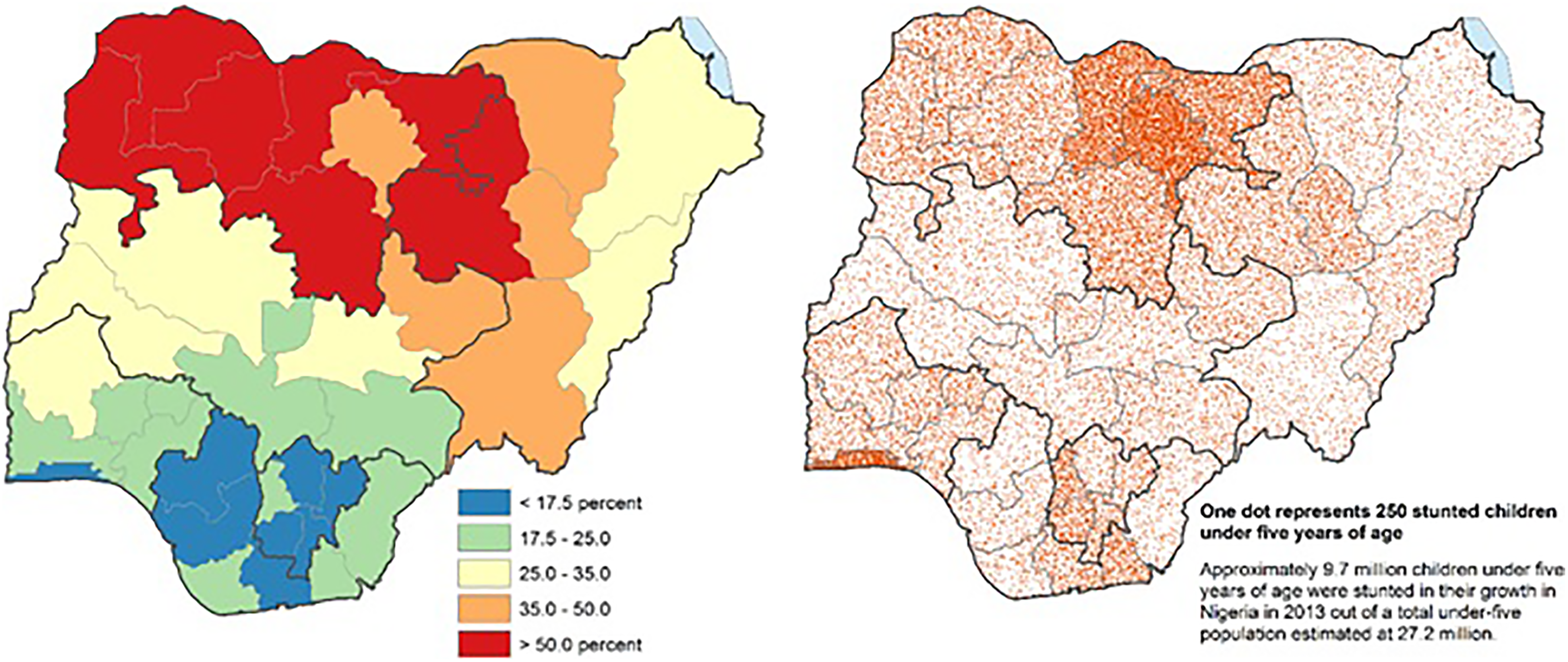
Stunting in children younger than 5 years in Nigeria in 2013, shaded area map of stunting prevalence (left) and dot map of the number of stunted children (right), by state. Source: Analysis by the authors of Nigeria Demographic and Health Surveys 2013 and National Population Commission 2006. Geopolitical zone boundaries shown.
The Nutritionally Vulnerable of Interest
All individuals are at risk of becoming malnourished to some degree. However, the developmental consequences of being malnourished for the individual and for society as a whole differ significantly between individuals. It is children younger than 2 years; their mothers; and all women of childbearing age; plus adolescent girls, for whom undernutrition is most likely to have the most adverse consequences for themselves; their households and communities; and for Nigeria. It is undernutrition in these demographic groups, particularly young children, that was the subject of our analysis.
The rationale for this is tied to the developmental window of opportunity of the 1000 days from conception through the child’s second birthday during which the greatest returns to effective action to prevent undernutrition are realized. 3 It is particularly at the start of the life cycle when it is important that young children and the mothers who bear them are properly nourished. Women of reproductive age and adolescent girls must receive proper nutrition so that when they are pregnant they can properly nourish their children in utero from the time of conception until birth. Healthy, well-nourished mothers (and future mothers) are considerably more likely to give birth to and be able to nurture and raise healthy children. After birth, proper feeding and care needs to be provided to infants so that their physical and mental growth is maintained. Interventions when children are older indeed, even after the second birthday, often cannot undo the damage done by undernutrition during the first 1000 days. By ensuring that young children and their mothers are well nourished, households and communities in Nigeria are laying an essential element of the foundation for an increasingly intelligent, creative, and healthy population from which to build a better and more prosperous future. Consequently, in conducting this study, our focus was on infants and young children, in particular, as well as their mothers, both women of reproductive age and adolescent girls who will become mothers in later years.
Undernutrition in Northern Nigeria
An overview of undernutrition in northern Nigeria relative to the rest of the country is provided in this section to describe the nutritional context for our study. This is followed by a description of the UNICEF conceptual framework of the determinants of child nutritional status which was used to guide the study.
Review of Recent Statistics on Child Nutrition
Table 1 presents recent statistics on young child and maternal nutritional status for northern Nigeria and the rest of the country, respectively. For consistency, most of the estimates in this report are drawn from the reports on the 2008 NDHS and the 2013 NDHS.
Selected Statistics on Young Child and Maternal Nutritional Status.a,b
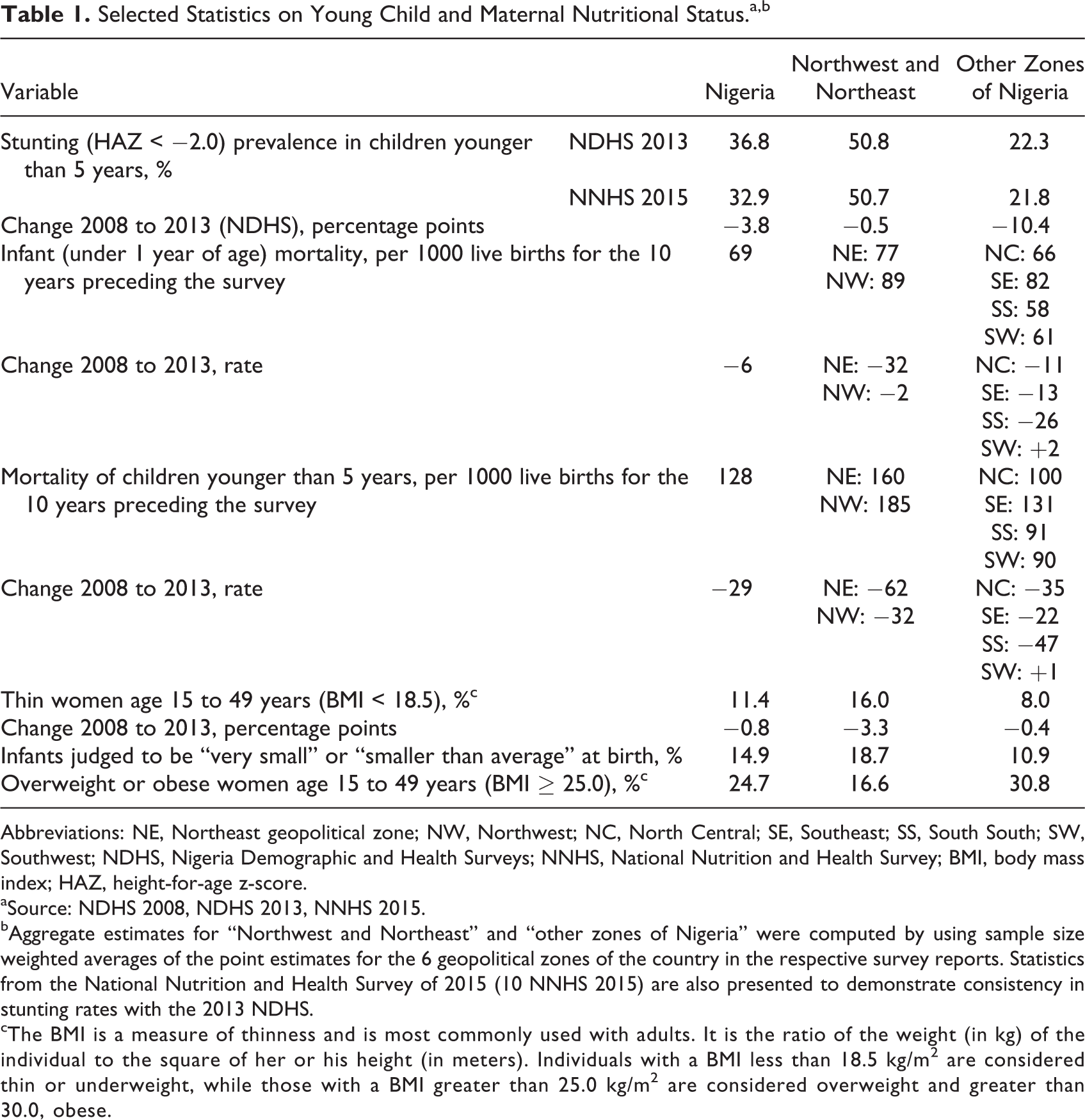
Abbreviations: NE, Northeast geopolitical zone; NW, Northwest; NC, North Central; SE, Southeast; SS, South South; SW, Southwest; NDHS, Nigeria Demographic and Health Surveys; NNHS, National Nutrition and Health Survey; BMI, body mass index; HAZ, height-for-age z-score.
aSource: NDHS 2008, NDHS 2013, NNHS 2015.
bAggregate estimates for “Northwest and Northeast” and “other zones of Nigeria” were computed by using sample size weighted averages of the point estimates for the 6 geopolitical zones of the country in the respective survey reports. Statistics from the National Nutrition and Health Survey of 2015 (10 NNHS 2015) are also presented to demonstrate consistency in stunting rates with the 2013 NDHS.
cThe BMI is a measure of thinness and is most commonly used with adults. It is the ratio of the weight (in kg) of the individual to the square of her or his height (in meters). Individuals with a BMI less than 18.5 kg/m 2 are considered thin or underweight, while those with a BMI greater than 25.0 kg/m2 are considered overweight and greater than 30.0, obese.
The results of under-five stunting in Table 1 reflect the patterns presented in the maps in Figure 1, with prevalence rates in northern Nigeria being more than twice those in the rest of the country. Stunting estimates from the 2015 National Nutrition and Health Survey are reasonably consistent with estimates from the 2013 NDHS. Trends in the prevalence of stunted young children between 2008 and 2013 show that northern Nigeria has not made any progress over this period. The lowering of stunting levels by almost 4 percentage points in the country as a whole over this period is solely due to progress in the rest of the country, where a 10-percentage point drop is estimated.
In terms of the development of chronic undernutrition after birth, Figure 2 compares the mean HAZ for children up to 5 years of age in northern Nigeria and those in other areas of Nigeria by age in months using data from the 2013 NDHS. The graph plots show that the nutritional status of newborns in northern Nigeria, on average, begins to decline immediately from birth, while in other areas of Nigeria, this decline is delayed several months. This pattern of decline a few months after birth in other areas of Nigeria is commonly seen in most populations in developing countries and generally reflects the challenges associated with safely introducing complementary foods into the diet of the young child. 6,7
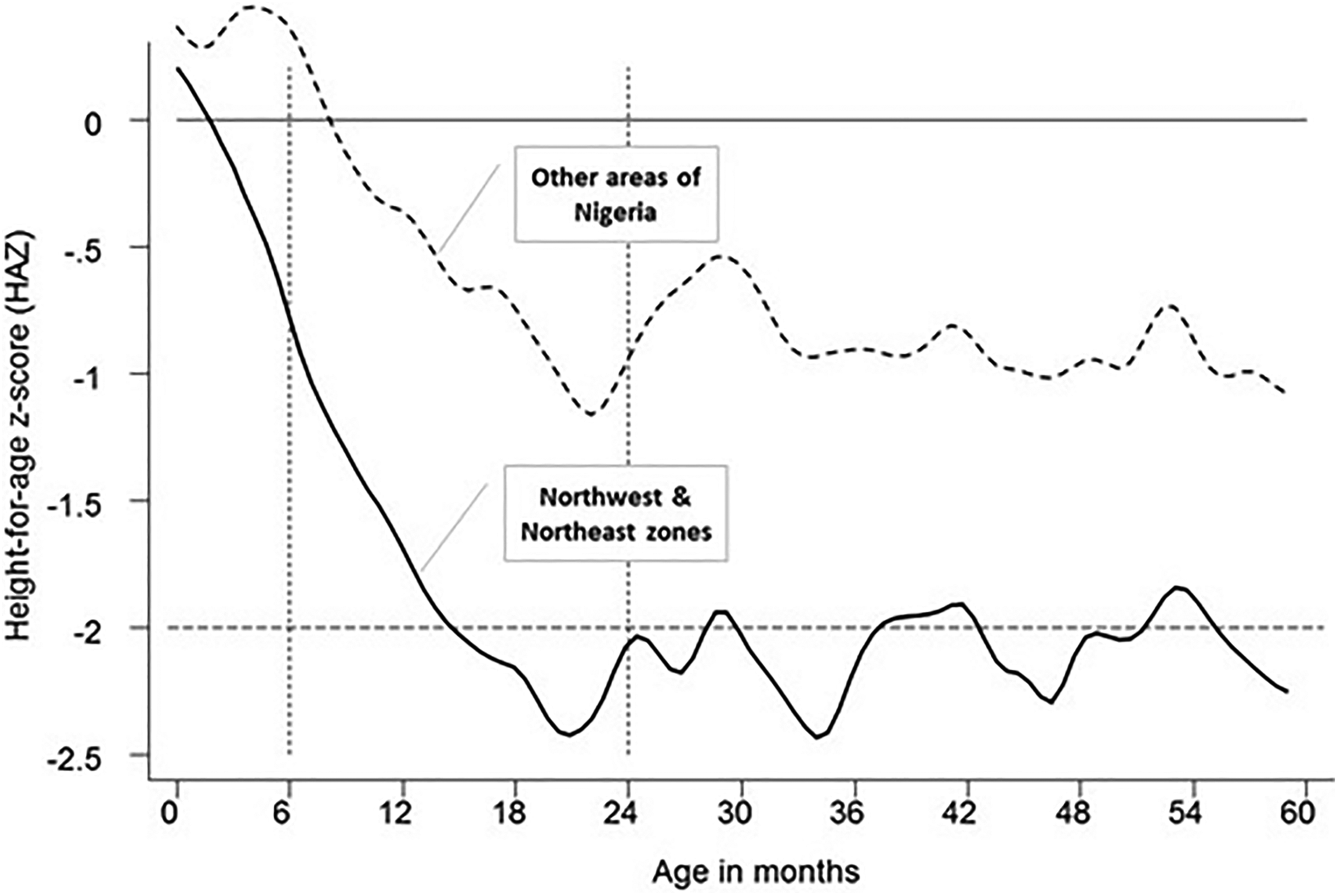
Mean height-for-age z-score (HAZ) by month of age for Nigerian children from birth to 5 years of age, 2013: Northwest and Northeast zones; rest of the country. Source: Authors’ analysis of Nigeria Demographic and Health Surveys 2013.
What is notable here is the immediate decline from birth in the average nutritional status in terms of linear growth with age of infants in northern Nigeria, indicating that many infants in northern Nigeria will have suffered from undernutrition in the womb due to their mothers being undernourished. But this undernutrition is then compounded by poor nutritional care or health challenges after birth, so no improvement in average nutritional status results is seen for infants in northern Nigeria in the months after birth, unlike in other areas of Nigeria. This decline in mean HAZ scores by month of age continues rapidly until the children are about 20 months of age, a pattern of decline in mean HAZ scores seen for both children in northern Nigeria and in other areas of Nigeria. However, for children in northern Nigeria, by 15 months of age, their mean HAZ score falls below −2.0, the clinical definition of a child being stunted in their growth. Over the next 45 months as the children age, only occasionally does the mean HAZ score for those in northern Nigeria rise above 2.0. The implication of this is that at least 1 of 2 children aged 15 to 59 months in northern Nigeria are stunted in their growth. For children in other areas of Nigeria, while significant stunting in growth occurs, mean HAZ scores are closer to −1.0 as the children age after 15 months, suggesting that either stunting is not as widespread across children in this age-group or is generally not as severe as is the case for children younger than 5 years in northern Nigeria.
Undernutrition is implicated in many of the deaths of infant and young children in developing countries like Nigeria. Although improvements are being seen in infant and mortality of children younger than 5 years levels over time, particularly in the Northeast zone of Nigeria, northern Nigerian children at birth are still significantly more likely, on the order of 60% to 70%, than children elsewhere in Nigeria to die before their fifth birthday (Table 1).
With regard to the nutritional status of women of childbearing age, women in northern Nigeria are more likely to be thin than in other parts of the country. However, reductions in the prevalence of thin women between 2008 and 2013 were considerably higher in northern Nigeria than elsewhere. Further analysis will be required to determine what drove this positive change. A potential consequence of a mother being undernourished is that her children at birth will be somewhat smaller than normal. The 2013 NDHS obtained a subjective assessment of the size of their newborn relative to other newborns from the mothers of young children. In northern Nigeria, a larger proportion of mothers considered their newborns to be smaller than normal than did mothers elsewhere in the country.
In terms of malnutrition, even if not undernutrition, overweight or obese women are not absent in northern Nigeria. Of 6 women of childbearing age, 1 women is overweight in northern Nigeria, a share that is about half of that of women elsewhere in Nigeria. At present, undernutrition is the principal nutrition challenge facing communities in northern Nigeria, rather than noncommunicable diseases associated with obesity. Nonetheless, programs to address obesity in Nigeria must ensure that those in northern Nigeria affected should also be targeted and mechanisms established to prevent this problem of malnutrition from intensifying in the north.
Conceptual Framework of the Determinants of Nutritional Status
To identify which factors might be resulting in the high levels of undernutrition observed in northern Nigeria, we employed the UNICEF conceptual framework of the determinants of nutritional status in young children (Figure 3) to guide our analysis (note 3). 8 This framework has been applied and validated in conducting many nutritional analyses globally, as it provides an efficient, succinct, and useful way to understand what set of factors might potentially be driving the nutritional condition of young children in a society or community (note 4).
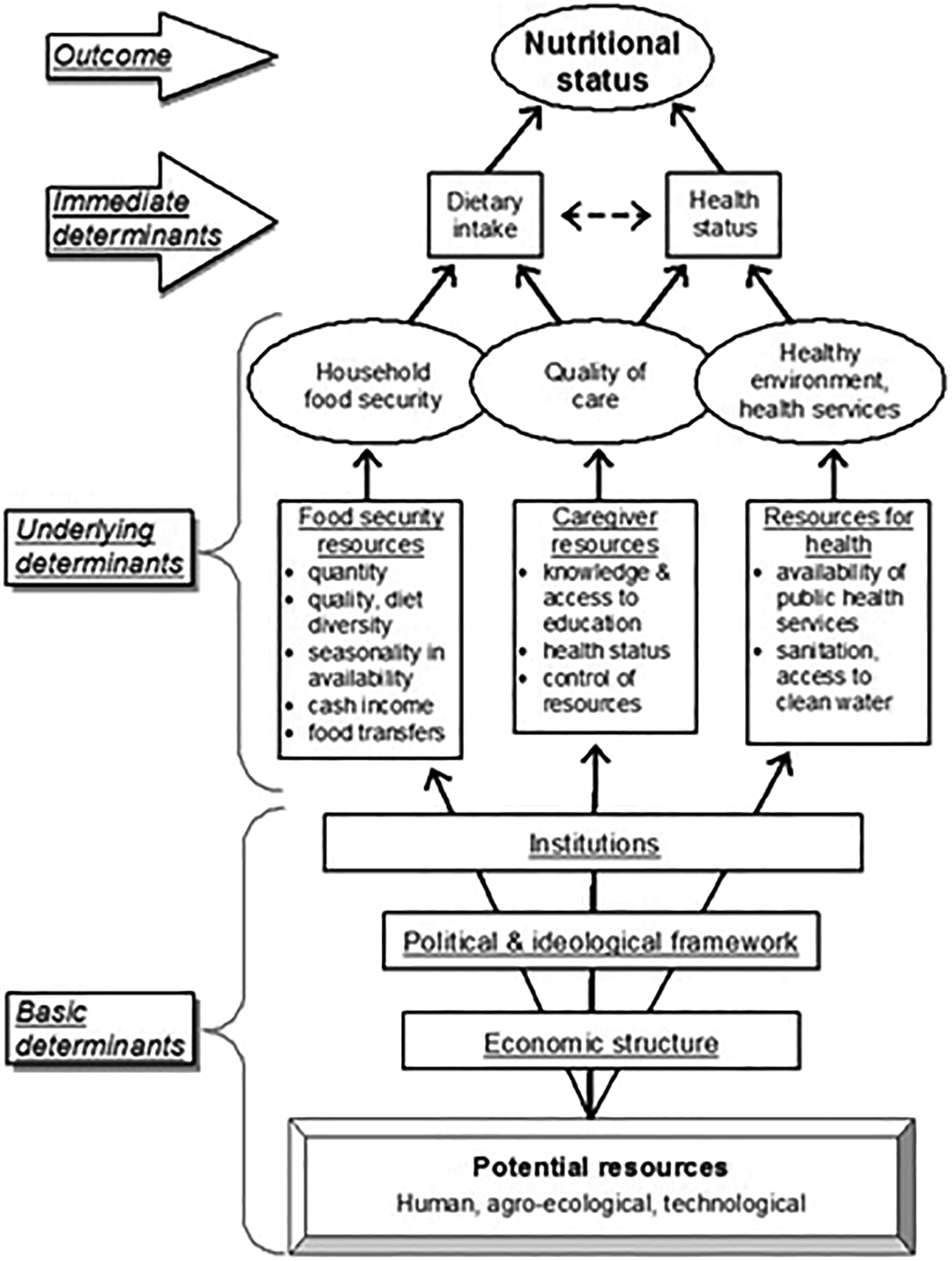
The framework presents a generalized understanding of how proper nutrition or, conversely, malnutrition is the outcome of specific development problems related directly to the level of dietary intake and the health status of the young child, the immediate determinants of nutritional status. The quality of these immediate determinants, in turn, is determined by the underlying food security status of the household in which the child resides. Of equal importance to nutrition, however, is the availability of health services and a healthy environment and the quality of care the individual receives. A sustained healthy and active life is possible only when these underlying determinants of the nutritional status of household members are of a sufficiently beneficial character.
The degree to which these 3 underlying determinants are expressed, positively or negatively, is a question of resources—primarily those available in the household and also in the community—and whether they are used effectively to address the nutritional needs of the young child. These resources include the availability of food, but extend much farther to include the physical and economic access that an individual or his or her caregiver has to that food, the caregiver’s knowledge of how to utilize available food and properly care for the individual, the caregiver’s own health status, and the control the caregiver has over resources within the household that might be used to nourish the individual. Finally, the level of access to information on and services for maintaining health; the availability of curative services; and the presence or absence of a healthy environment with clean water, adequate sanitation, and proper shelter all contribute to determining the nutritional status of an individual.
When the distribution of resources within communities and society as a whole is the central point of discussion in accounting for why some are malnourished and others are not, the framework moves from the realm of the individual and household to the political. The UNICEF framework links the availability of nutrition resources to a set of basic determinants, which are themselves a function of how society is organized in terms of economic structure, political and ideological expectations, and the institutions through which activities within society are regulated, social values are met, and potential resources are converted into actual resources. These include political, administrative, and religious institutions through which a society’s values are identified, its development vision defined, and that vision achieved. Consequently, achieving good nutritional status for all is identified in the framework as a subject for political debate and an issue of immediate concern to any national development strategy.
Finally, although not explicit in the basic form of the UNICEF framework, designing actions to reduce undernutrition requires consideration of gender-defined roles in households and communities. A key question in this regard is “Who does these nutrition-related tasks?” that result in a young child growing well or being undernourished. To a large degree, it is women who are directly involved in the processing and preparation of food and the care and feeding of young children within the household. Beyond breastfeeding, there are really few biological reasons for women alone to assume these roles and for men to shun them. However, gender bias and discrimination constrain and limit women’s rights, choices, capabilities, and opportunities. Taken together, these constraints limit women’s abilities to improve their own nutritional status and that of their children. A broad cross-country quantitative analysis 12 found that increases in the decision-making power of women relative to men were significantly associated with improved nutritional status in their children, concluding that sustainably improving nutritional status broadly requires proactive efforts to improve the status of women.
Drivers of Chronic Undernutrition in Young Children
The UNICEF conceptual framework guided the specification of the econometric models that were developed using data from the 2008 and 2013 NDHS to identify the factors most closely correlated with stunting in young children aged 6 to 23 months in Nigeria. The explanatory variables chosen for these analyses are those from the NDHS that proxy reasonably well for components of the underlying determinants of young child nutritional status according to the UNICEF framework as well as some basic determinants. Two separate analyses were conducted. The first examines how, in 2013, the determinants of stunting in young children in northern Nigeria differed from the determinants of stunting elsewhere in the country. This analysis provides insights into how reliable for guiding the design of programs to improve the nutrition of young children in northern Nigeria would be the results of a national level analysis that pools the 2 analytical regions. Essentially, is it best to treat the 2 regions separately? The second compares the determinants of child stunting in northern Nigeria in 2008 with those in 2013 to assess whether any signs of change can be seen.
The quantitative analyses focus on children aged 6 to 23 months, the period over which the diet of the child changes from primarily being based on breastfeeding to being increasingly reliant on foods eaten by the household as a whole. In terms of health and nutritional condition, this is a vulnerable period in life. Excluding from our analysis children younger than 6 months who are still predominantly breastfed allows the analysis to be more strongly focused on behaviors related to ICYF during the period it is recommended that the child be weaned, while not neglecting nutritional factors that affected the child before 6 months of age, including the nutritional status of the child’s mother, any participation in antenatal clinics by the mother, and the effects of earlier-than-recommended introduction of other liquids than breast milk or solid foods to the diet of the infant.
The upper age bound on the children included in these analyses is justified by reference to global analyses, which demonstrate that linear growth faltering in infants continues until about 24 months of age, after which only slight improvements are seen in the period to 5 years of age. 13 This pattern is seen in the growth of young children in both northern Nigeria and in other areas of Nigeria (Figure 2). While not dismissing the continuing and long-term adverse effects of poor nutritional status after a child is 2 years or older on health, cognitive development, well-being, and economic potential, it is particularly during the period when the child is in the womb before birth and in the first 2 years of life that the growth of the child “is most sensitive to environmentally modifiable factors” 14(p13) related to diet, public health and medical factors, and care. Consequently, limiting the study to children young than 2 years results in somewhat more program-relevant factors being brought into the analysis than would otherwise be the case.
It should be noted that the models are generated primarily to identify associations between specific factors and whether a young child is stunted. The analyses here do not permit one to claim any cause-and-effect relationships, whereby a factor shown to be statistically significant in the analysis can be held to be among the causes or principal drivers of the nutritional condition of the child. More sophisticated econometric techniques that focus on specific causal factors and pathways would be required to identify the particular role and intensity of a specific determinant in causing undernutrition in young children in northern Nigeria. However, for a broad assessment of what factors are likely important drivers of the nutritional status of young children in northern Nigeria and how the importance of the factors contrasts to other areas in Nigeria or may have changed over time, these models provide a useful initial set of insights.
The 2008 and 2013 NDHS data sets include detailed child, mother, and household information, including demographic and socioeconomic characteristics, anthropometry, health care and use of health facilities, feeding practices, water and sanitation, and an asset-based wealth index for each survey household (note 5), among others. As the 2 surveys are very similar in their design and content, analysis of the same determinants of nutritional status in both 2008 and 2013 can be done to assess whether the way these determinants operate to generate the outcome of the nutritional status of a young child stays constant over time.
A standard child-level regression-based approach is used for the first part of the analysis. The dependent variable is whether the child is stunted (HAZ < −2.0), a dummy variable taking a value of 1 if the child is stunted and 0 if not. Since the explanatory variable is a binary variable, a maximum-likelihood logit model is used. Similar analyses of child stunting in Nigeria have been done using various rounds of the NDHS series, including the study by Ajieroh 15 and Adekanmbi et al. 16 In developing the models, a broad range of potential explanatory variables were developed from the NDHS data sets and assessed both in terms of how well their inclusion in the model reflected conceptually informed expectations and in terms of how well they performed econometrically, particularly in terms of collinearity between explanatory variables. Three models with the same 2 dozen or so explanatory variables resulted from this assessment process.
In contrast to earlier modeling efforts, here the analysis was extended by comparing the model for northern Nigeria in 2013 to other areas of Nigeria in 2013 to decompose differences between the models. This was done to gain understanding on how the determinants of child stunting in children aged 6 to 23 months differ between the 2 areas (note 6). This decomposition analysis enables us to identify what factors might differ between northern Nigeria and the rest of the country to account for any differences in stunting prevalence observed. If some of the factors identified as differing between the 2 areas of Nigeria can be associated with specific policies or programs, insights would be provided for the design of future area-specific nutrition programming.
The Oaxaca decomposition method, 17 –19 as used here, explains the gap in child stunting prevalence between northern Nigeria and the rest of Nigeria in 2013 by decomposing that gap into 2 components based on the models for each analytical region. The first component of the gap is due to differences in the relative levels, or endowments, of the determinants of stunting between the 2 groups in each case, such as differences in levels of mother’s educational attainment, access to safe water, or to postnatal care for infants. The second is due to difference in the coefficients for the explanatory variables in the respective models for the 2 groups, that is, due to differences in the effects of those determinants on stunting in young children. Significant differences in the coefficients on the same explanatory variables for the 2 respective models would suggest that the “production functions” for the linear growth of young children differ for the 2 populations, that is, in northern Nigeria and in other areas of Nigeria (note 7).
Descriptive Statistics
The dependent variable for each of these models is whether the child has an HAZ score of less than −2.0, which is the threshold HAZ score below which a child is considered clinically to be stunted in their linear growth. In Figure 4, plots of the distribution of the HAZ scores from the 3 analytical data sets are shown. Sharp distinctions are seen in the distribution of HAZ scores for children aged 6 to 23 months between other areas of Nigeria in 2013 and northern Nigeria in 2013. However, in contrast, the curves for northern Nigeria in 2008 and 2013 closely overlap, showing little change in the distribution pattern of HAZ scores in children aged 6 to 23 months in the period between the 2 years.
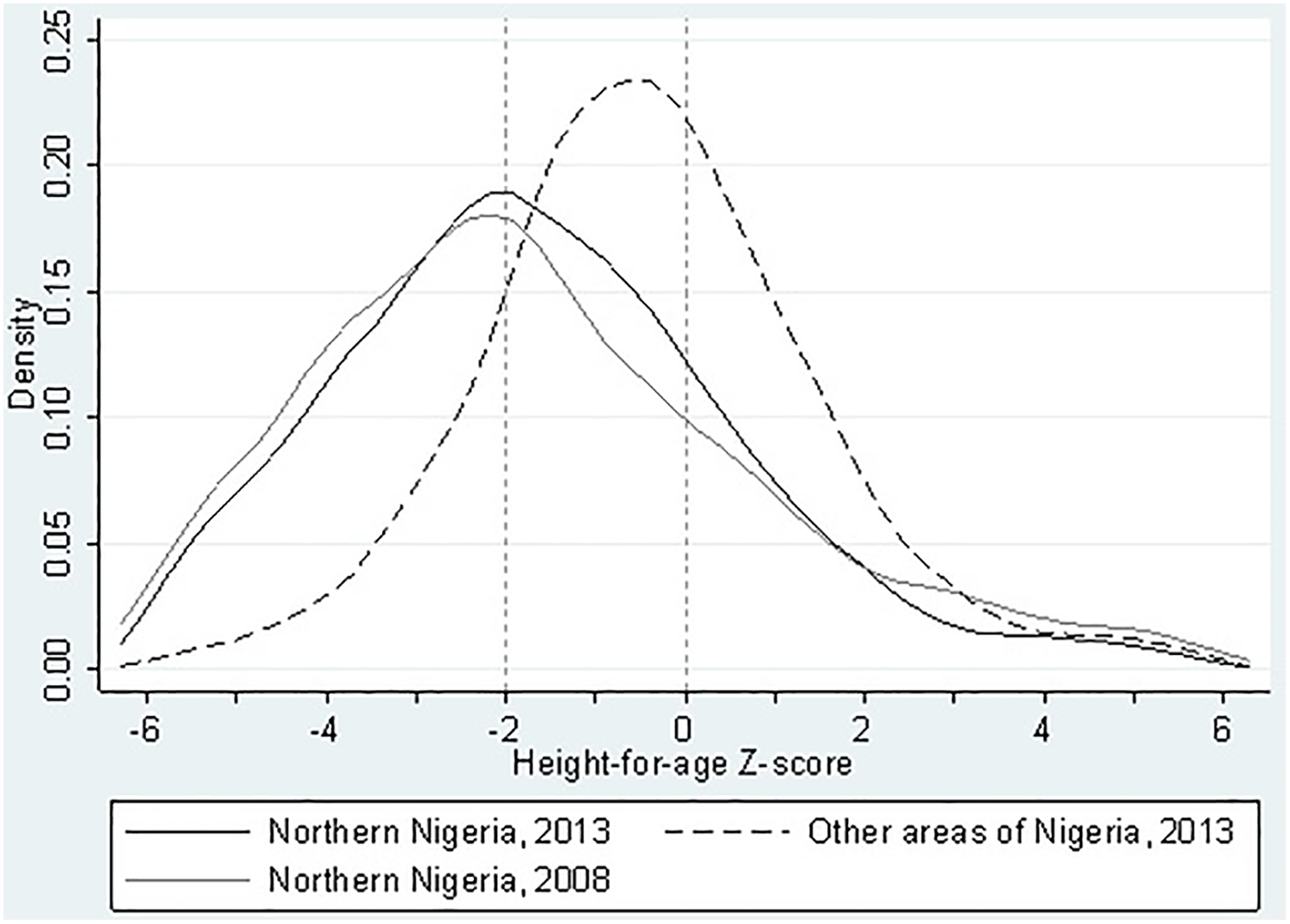
Distribution of height-for-age z-scores (HAZ) for children between 6 and 23 months of age for northern Nigeria in 2013 and 2008 and for other areas of Nigeria in 2013. Source: Analysis of Nigeria Demographic and Health Surveys 2008 and 2013. Note: HAZ = −2.0 is the threshold for clinically defining a child as stunted in their growth. HAZ = 0.0 is the median height-for-age z-score for young children in a well-nourished population.
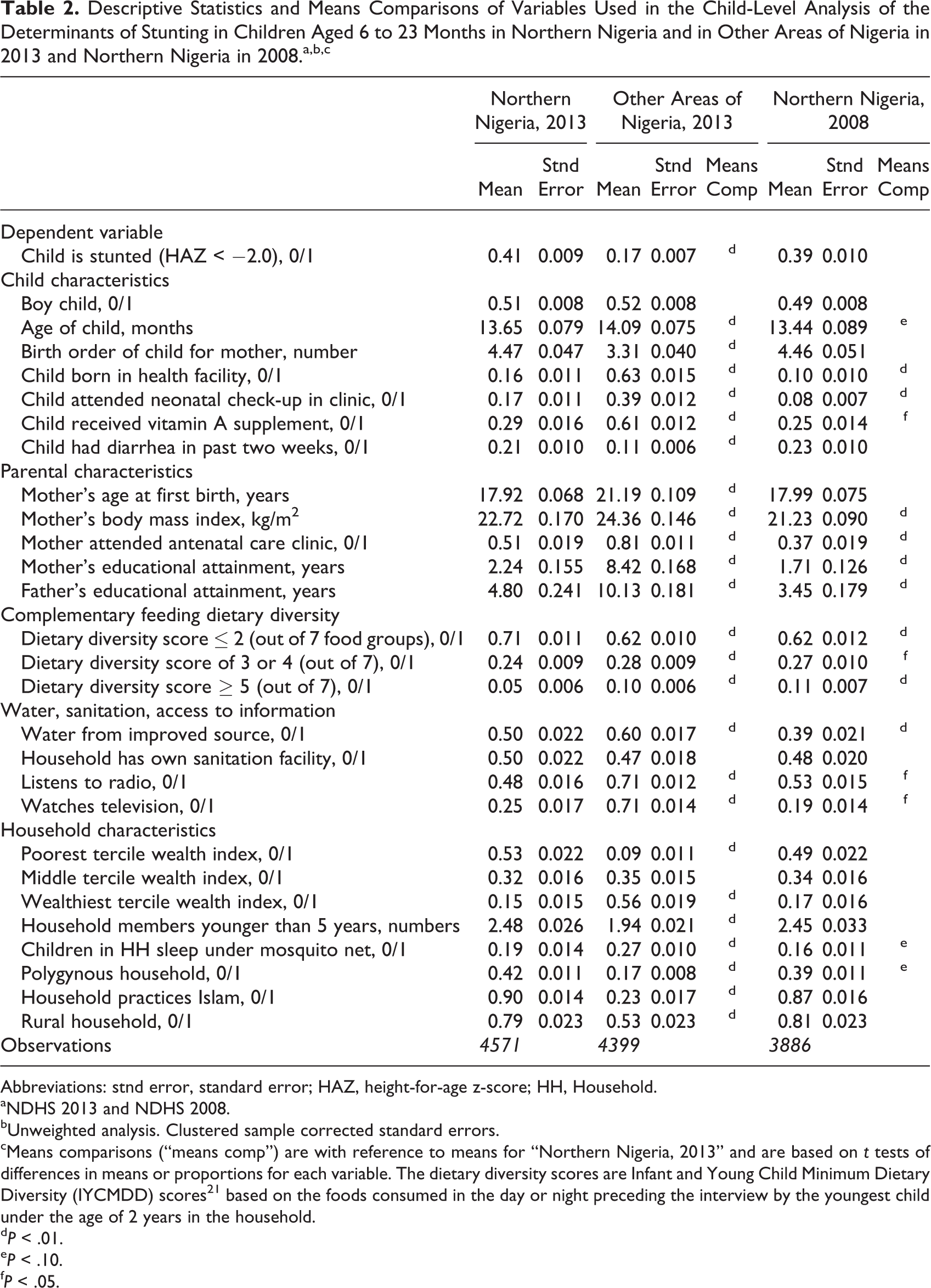
Mean values are presented in Table 2 for the dependent variable used in the quantitative analysis of whether a child is stunted and for the explanatory variables, including child and parental characteristics, the diversity of the diet fed to the youngest child in the household, and other household characteristics. These are drawn from the 3 different analytical data sets extracted from the NDHS series: Northern Nigeria, 2013; other areas of Nigeria, 2013; and Northern Nigeria, 2008. Also, the P values for comparisons of means tests for the variables used between the northern Nigeria, 2013 data set, and the 2 other analytical data sets are presented in Table 2.
Descriptive Statistics and Means Comparisons of Variables Used in the Child-Level Analysis of the Determinants of Stunting in Children Aged 6 to 23 Months in Northern Nigeria and in Other Areas of Nigeria in 2013 and Northern Nigeria in 2008.a,b,c
Abbreviations: stnd error, standard error; HAZ, height-for-age z-score; HH, Household.
aNDHS 2013 and NDHS 2008.
bUnweighted analysis. Clustered sample corrected standard errors.
cMeans comparisons (“means comp”) are with reference to means for “Northern Nigeria, 2013” and are based on t tests of differences in means or proportions for each variable. The dietary diversity scores are Infant and Young Child Minimum Dietary Diversity (IYCMDD) scores 21 based on the foods consumed in the day or night preceding the interview by the youngest child under the age of 2 years in the household.
d P < .01.
e P < .10.
f P < .05.
We observe in Table 2 that there are sharp differences in the means for virtually all variables used in the models between northern Nigeria and the other areas of Nigeria in 2013. Generally, the levels of the variables for northern Nigeria are significantly worse, in terms of how they are expected to contribute to child nutritional status than are the levels for the same variables in other areas of Nigeria, including lower use of health services, thinner mothers, poorer parental educational attainment, and generally lower household wealth status. Based on these descriptive statistics alone, it is apparent that the context within which infants grow in northern Nigeria is quite different from that found in other areas of Nigeria.
Temporally, in comparing changes in the levels of the explanatory variables in northern Nigeria between 2008 and 2013, some encouraging progress is seen. For example, more infants in 2013 were born in health facilities and were presented for check-ups, parents’ educational levels are rising, and more households are obtaining their water from protected sources. However, despite these improvements in the levels of these determinants of child nutritional status, we observe no change between 2008 and 2013 in the prevalence of stunting in children aged 6 to 23 months; indeed, we observe a small, if statistically insignificant, rise in the prevalence rate among the children in our NDHS sample. Accelerated progress on almost all the factors that conceptually we expect contribute to improved child nutritional status will be needed if young children in coming generations in northern Nigeria are to realize their physical growth potential to the same degree as young children in other areas of the country.
Models of the Determinants of Whether a Young Child in Nigeria is Stunted
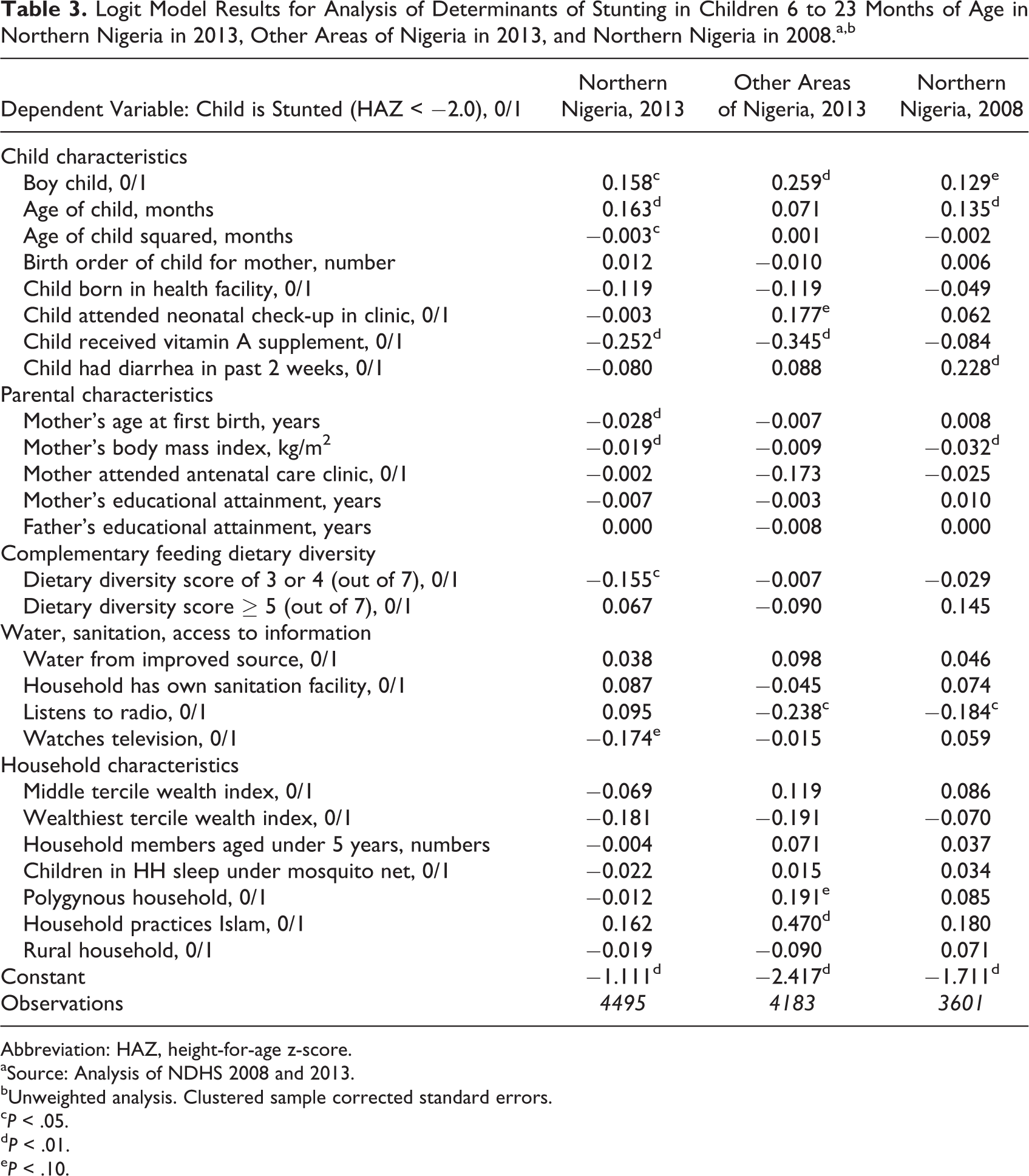
The results of the 3 logit models for this analysis are presented as coefficients in Table 3. In terms of the nature of the relationship between the explanatory variable and whether a child is stunted, although not perfect, we see general consistency across the 3 models and with our expectations based on the UNICEF conceptual framework. So, for example, in all 3 models, mothers with a higher body mass index (BMI) or households in the wealthiest tercile are more likely to have children who are not stunted, associations that are in keeping with conceptual expectations.
Logit Model Results for Analysis of Determinants of Stunting in Children 6 to 23 Months of Age in Northern Nigeria in 2013, Other Areas of Nigeria in 2013, and Northern Nigeria in 2008.a,b
Abbreviation: HAZ, height-for-age z-score.
aSource: Analysis of NDHS 2008 and 2013.
bUnweighted analysis. Clustered sample corrected standard errors.
c P < .05.
d P < .01.
e P < .10.
However, somewhat fewer statistically significant coefficients are seen in the models than were anticipated. Insufficient variability in some of the explanatory variables used is among the explanations for this. This is apparent in reviewing Table 2, particularly in northern Nigeria, for example, mother’s educational attainment or households practicing Islam. Sample size is also a factor. Earlier models run on larger NDHS samples, such as on children aged 6 to 59 months, resulted in a larger share of coefficients being significant. Finally, our current conceptual understanding of the determinants of stunting in young children is inexact and perhaps overly simplistic, which is reflected in many model coefficients having the expected signs while being statistically insignificant.
Reviewing the models, we see that boys are more likely to be stunted than girls, which is a common finding of such analyses in sub-Saharan Africa. 22 Reflecting the pattern of increased stunting with age shown in Figure 2, older children are more likely to be stunted. However, the coefficients for age and age squared are not significant for other areas of Nigeria in 2013, reflecting the moderated decline in HAZ scores for children with age in that population relative to those in northern Nigeria. Although the coefficients are insignificant, children of higher birth order for the mother are more likely to be stunted in northern Nigeria but less likely in other areas. This suggests that experience gained by the mother in raising earlier children does not bring about benefits for the growth of later children in northern Nigeria, while it does elsewhere (note 8). Children who were born in a health facility or received vitamin A supplementation are less likely to be stunted, although the relationship is not always significant. Mixed patterns that are not wholly consistent with expectations are seen in the variables on whether the child was checked in a medical clinic shortly after birth and on a recent experience of diarrhea.
With regard to parental characteristics, children of mothers who first gave birth somewhat later than other mothers are significantly less likely to be stunted only in the 2013 northern Nigeria data set. Insignificant and contrasting patterns are seen in the other data sets. The higher the BMI of a child’s mother, the less thin she is, the more likely the child is to not be stunted, reflecting the importance of the nutritional status of the mother for the nutritional status of the child. Attendance by the mother at an antenatal clinic is shown to reduce the likelihood of a child being stunted but not significantly so.
Surprisingly, educational attainment by the parents of young children is shown to have no impact on whether the child is stunted in any of the 3 models. All the coefficients are quite close to 0. This relationship is easiest to understand in northern Nigeria, where educational attainment levels are quite low. The lack of a detectable effect of parental education on whether a child is stunted in northern Nigeria may be due to a threshold effect, significant effects of education on child nutritional status only are strongly seen when parents have at least a post-primary education level. 24 The median years of education attained for both fathers and mothers in the 2013 northern Nigeria data set is 0. However, this is not the case in other areas of Nigeria, where most parents have attained significantly higher education levels. Why education in other areas of Nigeria has no significant impact on the likelihood of a child being stunted is an unexpected result and should be examined further.
Moderate diversity in the complementary foods that a child being weaned received in a household is a significant determinant of children in that household not being stunted only in northern Nigeria in 2013. In the other models, the coefficients for this variable have a similar sign but are not significant. Somewhat surprisingly, higher levels of dietary diversity do not result in a consistent or significant response across models, likely reflecting the low numbers of children with such diverse diets. The model results for safe water sources and toilet facilities for the household are contrary to expectations, suggesting that the provision of such services is not sufficient on its own to reduce stunting. Whether a mother listens to radio is associated with a child in the household being less likely to be stunted, except in 2013 in northern Nigeria. Here, the relationship goes against expectations of radio being a channel to disseminate messages on good nutritional care, possibly reflecting a change in radio programming or in patterns of radio listening since 2008. For television watchers, however, it is only in northern Nigeria in 2013 that there is a statistically significant association with the likelihood of a child not being stunted. However, only a quarter of mothers in northern Nigeria reported watching any television in 2013.
Whether a household was among the wealthiest third of households in Nigeria is shown across all models to be associated with the child likely to not be stunted but not significantly so. While the direction of this relationship is not surprising, since we would expect such households to have the resources and also are likely to have received the knowledge necessary to provide good nutritional care and good diets for their young children, that the relationship is not more strongly significant is surprising. However, we find that whether young children are members of households in the middle third of households in terms of wealth in Nigeria is not associated in a consistent or significant way with whether those children are stunted. Wealth alone appears insufficient to prevent stunting in young children.
The remaining household characteristics considered provide inconsistent and often insignificant results. Larger numbers of young children in the household are not associated with greater likelihood of a young child being stunted nor does sleeping under a mosquito net, which might be considered a proxy for a household implementing preventative health practices. Stunted children are more likely to be found in polygynous households only outside of northern Nigeria. In northern Nigeria, a closer analysis would be required to determine how co-wives in the household might improve or detract from the nutritional care a young child receives. Whether a household practices Islam is not associated with any higher chance of a young child being stunted in northern Nigeria. However, this association is seen elsewhere in Nigeria in 2013. Given that many of the determinants of child stunting that may be associated with the practice of Islam in Nigeria, such as lower female educational attainment and mothers being quite young when they first give birth, are controlled for in the model, that the coefficient on this variable is statistically significant is puzzling. Finally, stunted children aged 6 to 23 months are no more likely to be found in rural areas than in urban centers in Nigeria.
While these models confirm many of the expectations on what determines whether a young child is stunted in Nigeria, the lack of significance of many coefficients and counterintuitive results on others challenges some of these assumptions. Despite being constructed on the basis of the broadly accepted UNICEF conceptual framework of the determinants of child nutritional status, much of what drives child stunting in Nigeria is not captured by these models.
Decomposition of the 2013 Models
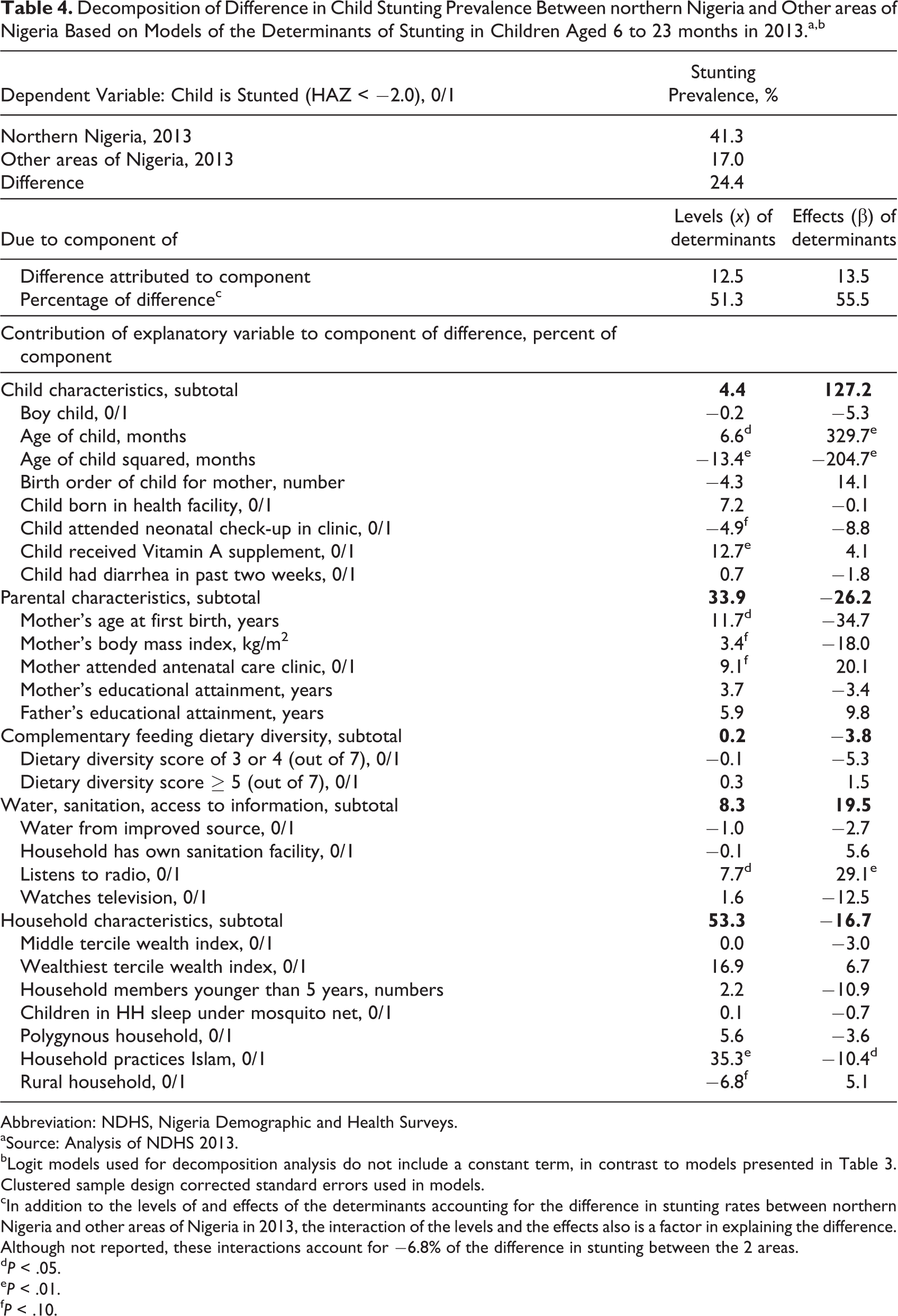
The Oaxaca decomposition approach was used to explain the gap in child stunting prevalence both between northern Nigeria and the rest of Nigeria and between 2008 and 2013 in northern Nigeria. However, for the temporal analysis, given the very small difference in stunting prevalence levels in our analytical data sets for northern Nigeria for 2008, 39%, and for 2013, 41%, no significant decomposition results were obtained. Consequently, only the decomposition results for the gap in child stunting prevalence between northern Nigeria and the rest of Nigeria in 2013 are presented (Table 4). The share of children in the analytical data set of children aged 6 to 23 months in northern Nigeria who were stunted in 2013 was 41.3%, while the share of similar children in other areas of Nigeria who were stunted was 17.0%. The difference of 24.4% in the prevalence of stunted children in the 2 parts of the country is what we wish to explain by considering differences in the levels of potential determinants (x in the regression models) of child stunting and differences in the effects of those determinants (the coefficients, β, in the regression models) between the 2 areas.
Decomposition of Difference in Child Stunting Prevalence Between northern Nigeria and Other areas of Nigeria Based on Models of the Determinants of Stunting in Children Aged 6 to 23 months in 2013.a,b
Abbreviation: NDHS, Nigeria Demographic and Health Surveys.
aSource: Analysis of NDHS 2013.
bLogit models used for decomposition analysis do not include a constant term, in contrast to models presented in Table 3. Clustered sample design corrected standard errors used in models.
cIn addition to the levels of and effects of the determinants accounting for the difference in stunting rates between northern Nigeria and other areas of Nigeria in 2013, the interaction of the levels and the effects also is a factor in explaining the difference. Although not reported, these interactions account for −6.8% of the difference in stunting between the 2 areas.
d P < .05.
e P < .01.
f P < .10.
As was evident from the means comparisons in Table 2, there are significant differences in the levels of most of the determinants included in the model between northern Nigeria and other areas of Nigeria. This is also seen here in the decomposition analysis, if not as emphatically as in Table 2. Overall, differences in levels of determinants account for 51.3% of the difference in stunting prevalence between the 2 analytical regions. These results draw attention to those determinants for which differences in their levels matter for the prevalence of child stunting in an area and can be used as evidence to guide increased public investment of various sorts to improve the local levels of these determinants. Based on the decomposition analysis, these include improving the coverage and quality of health facility–based nutritional interventions for young children, making efforts to postpone first pregnancies in women, improving maternal nutrition, increasing participation by pregnant women in antenatal clinics, and improving access of mothers to public media sources, particularly radio.
For those significant factors whose levels are not amenable to being changed, most notably religious practices, the result here reinforces arguments for greater attention to ensuring that messages on good nutrition practices are compatible with the beliefs and attitudes of religious communities. Social mobilization for improved nutrition within such religious communities should remain a central element of nutrition programs across Nigeria.
Finally, on spatial targeting of efforts to improve levels of these determinants, the results of the decomposition analysis do not suggest that specific efforts to improve the levels of these factors should be made in northern Nigeria alone. While northern Nigeria has levels for most of the significant factors significantly below other areas of Nigeria and, so, should be prioritized in making efforts to improve those levels, nationwide efforts to improve the levels of these determinants are warranted. The prevalence of stunting in children aged 6 to 23 months in other areas of Nigeria remains unacceptably high at 17%, even if this rate is significantly lower than it is in northern Nigeria. Efforts to improve the levels of these significant factors nationwide will be beneficial for young children across all of Nigeria.
As shown in the rightmost column of Table 4, there are only a few specific determinants for which significant differences in effects are observed. Most notably and reflecting the stark difference in the plots of mean HAZ score by age in month shown in Figure 2, the effects of the age of the child on the likelihood of a child being stunted differ strongly between northern Nigeria and other areas of Nigeria. That this is the case reflects the cumulative effect of a range of different factors that adversely affect the child both in the womb and in the period immediately after birth. As discussed, infants in northern Nigeria are on a declining growth performance trajectory immediately from birth, while infants in other areas of Nigeria do not experience immediate challenges to their growth performance. Moreover, as the infant ages, on average the growth of the young child in northern Nigeria is compromised far more deeply than is the case for young children in other areas of the country.
Other important factors to consider in terms of the differences in their effect on child stunting include whether the mother listens to a radio, where a much more positive impact is seen in other areas of Nigeria. Finally, whether a household practices Islam also shows a significant difference in effect between the 2 analytical regions. However, the results here show that the effect on the likelihood of child being stunted due to being a member of a Muslim household is more adverse in other areas of Nigeria than in northern Nigeria. An implication of this is that social mobilization on proper nutritional care in a manner that is compatible with their belief system is as important to undertake with Muslim households in other areas of Nigeria as it is in northern Nigeria.
Implications for Investment Priorities and Program Design for Improved Nutrition
All the analyses provide strong evidence of the need to treat the nutritional challenges of northern Nigeria quite differently than the nutritional challenges of other areas of Nigeria. There are strong differences in the levels of the determinants of undernutrition between the 2 parts of the country. These differences in levels of the determinants of child nutrition can be addressed over the long term with continued public investments to raise levels in northern Nigeria to more closely match those elsewhere in the country.
However, equally important, the results of the decomposition analysis show that there are significant differences between northern Nigeria and other areas of Nigeria in the effect of the same determinant of nutritional status in accelerating or retarding the linear growth of young children. A national program to address child undernutrition must recognize this heterogeneity in its design. To impose across Nigeria, a single set of approaches to address the factors which results in stunted children is likely to fail for large numbers of children if these strong geographical differences in how these determinants operate to affect child nutritional status are not considered. Children in northern Nigeria from birth and even earlier in the womb face greater growth challenges than do children in other areas of the country. Solutions to the problem of chronic undernutrition developed in southern Nigeria and found to be successful there, at least based on the evidence of this analysis, are unlikely to be wholly successful if replicated in northern Nigeria. Solutions need to be developed within northern Nigeria to more closely reflect the way the determinants of nutritional status operate in this area of the country. Strengthening the flow of information on optimal nutritional care practices and supporting social mobilization efforts are required to enable the information to be used effectively. Investments are also needed to enhance the numbers of experts on public health nutrition in northern Nigeria and elsewhere in the country. These investments certainly should consider reforming primary and secondary school curriculums to include more instruction on what is required to ensure that young children grow to their full potential.
Additional more detailed analysis of the NDHS data sets is required to obtain specific guidance on where financial, institutional, and human resources should be allocated to reduce chronic undernutrition in northern Nigeria. The logit analyses presented here generally confirmed expectations on what are the key determinants of child nutritional status in Nigeria. However, robust results were not obtained either in the models or in their decomposition to derive strong guidance on whether resources currently directed to specific activities to address chronic undernutrition, particularly in northern Nigeria, might be better employed in a different way. To obtain clearer guidance will require more detailed, project- and program-specific analyses. However, insofar as those activities involve consideration of the determinants shown in our northern Nigeria model for 2013 to be significantly associated with child stunting in a manner aligned with our conceptual understanding, the design of these activities is likely on the right track. This is not to say, however, that ongoing assessment and reassessment of the efficacy of those investments will not continue to be required.
Reprinted with permission of the authors and the International Food Policy Research Institute (IFPRI). Additional Working Papers and Discussion Papers of IFPRI research programs are available on the IFPRI website (www.ifpri.org/publications).
Footnotes
Authors’ Note
This article has been prepared as part of the Feed the Future Nigeria Agricultural Policy Project.
Acknowledgment
We are grateful to the Nigeria mission of the United States Agency for International Development (USAID) for providing financial assistance to conduct this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We are grateful to the Nigeria mission of the United States Agency for International Development (USAID) for providing financial assistance to conduct this study.